
Abstract
To compare the postoperative outcomes of par plana vitrectomy (PPV) with subretinal recombinant tissue plasminogen activator (rt-PA) injection for submacular hemorrhage (SMH), utilizing three-dimensional (3D) heads-up or traditional microscopic (TM) visualization systems. Patients who were diagnosed with SMH and received PPV and subretinal rt-PA injection were enrolled in the retrospective cohort study. Patients were categorized to the 3D group and the TM group according to the visualization systems used in surgery. Best corrected visual acuity (BCVA), lesion parameters and the occurrence rate of postoperative adverse events were longitudinally recorded and compared. The 3D group (n = 19) and the TM group (n = 20) exhibited comparable baseline characteristics. Polypoidal choroidal vasculopathy (64.10%) was the leading cause of SMH. At the last visit, the enhancement of BCVA from baseline was 0.41 (95%CI 0.14–0.67) LogMAR in the 3D group and 0.30 (95%CI 0-0.59) LogMAR in the TM group, respectively (P = 0.555). SMH lesion parameters, including the height, greatest linear dimension and area, along with central retinal thickness, changed similarly during follow-up. Major adverse events, including photoreceptor/retinal pigment epithelial atrophy (92.31%), epiretinal membrane (41.03%), and recurrent SMH (30.77%), also occurred similarly at each follow-up in the two groups. The two visualization systems showed comparable postoperative efficacies and safety profiles in assisting PPV and subretinal rt-PA injection for SMH treatment.
Similar content being viewed by others


Introduction
Submacular hemorrhage (SMH) is a severe complication associated with vision-threatening fundus diseases, such as polypoidal choroidal vasculopathy (PCV), neovascular age-related macular degeneration (nAMD), retinal arterial microaneurysm (RAM)1,2. It refers to the accumulation of blood mainly under the neurosensory retina in the macular region, originating from the choroidal or retinal circulation. Studies in rabbit and cat models have demonstrated that SMH induced irreversible retinal damage in 7 days and severe outer retinal degeneration in 14 days3,4. In humans, the natural course of SMH is also severe and progressive. About 80% of nAMD eyes with SMH resulted in poor vision ranging from 20/100 to light perception (LP)5,6,7, highlighting the critical importance of prompt intervention for this condition.
In the last several decades, therapeutic methods for SMH have greatly expanded with the emergence of modalities such as pneumatic displacement, pars plana vitrectomy, anti-vascular endothelial growth factor (VEGF) drugs, and recombinant tissue plasminogen activator (rtPA). Combinations of these treatments are becoming mainstream options, such as pars plana vitrectomy (PPV) combined with subretinal injection of rtPA and pneumatic displacement combined with intravitreal injection of rtPA, with or without the use of anti-VEGF drugs8,9,10,11,12,13. Although recent high-quality studies have reported similar overall visual outcomes between these two combinations14,15,16, differences were noted when categorizing SMH by lesion size16. Furthermore, vitrectomy remains important for large SMH and can serve as a compensatory strategy for patients who fail to benefit from pneumatic displacement14,17. The choice between these approaches also depends on factors such as the location of the SMH, the patient’s overall health, and the surgeon’s expertise15. As a result, the combination of vitrectomy and subretinal rtPA injection is likely to remain a popular choice for managing SMH for the foreseeable future. This procedure’s pivotal step is a careful retinotomy for subretinal rt-PA administration to liquefy clots, where accuracy is crucial to prevent complications like retinal detachment or proliferative vitreoretinopathy18,19. Since studies have indicated that extensive or dense SMH predicts poorer visual prognosis, minimizing retinal trauma is vital for those with milder SMH because they are more likely to benefit from a successful surgery20,21. Complicated cases featuring concurrent subretinal and sub-RPE hemorrhages challenge the delivery of rt-PA due to limited subretinal space, which might cause potential RPE damage and trigger future neovascularization22. Advanced vitrectomy approaches, including the use of slimmer 41- and 47-gauge cannulas18,23,24,25, are essential to address these challenges.
On the other hand, improving visibility with advanced technology and special consideration on biomedical engineers may also aid in such surgery that requires high operational precision26. In recent years, three-dimensional (3D) visualization technologies have allowed surgeons to interact with detailed anatomical structures or even surgical environments during complex vitreoretinal procedures27,28,29. These systems replace traditional microscope eyepieces with high-definition cameras that capture stereoscopic images, projecting them onto a large 3D display screen to achieve improved visibility to the whole surgical team and provide other advantages such as enhanced magnification, broader visual field, and improved depth perception compared to traditional microscopes (TM)30. It also enhances surgical team communication, improves ergonomics, and reduces retinal illumine toxicities, which might potentially benefit the patients with SMH30,31,32,33,34. Though findings related to macular hole and epiretinal membrane surgeries have showed comparable three-month postoperative visual outcomes and surgical trauma between the 3D and TM systems35, few studies compared the postoperative effectiveness and safety of the two visualization systems in SMH surgery that involves subretinal operations, especially in a long term. In our recent small-scale study, 3D-assisted vitrectomies for SMH showed no iatrogenic retinal tear incidence, though there were instances of recurrent SMH, vitreous hemorrhage, and retinal detachment36, providing a preliminary impression of the 3D visualization system.
In this study, we comprehensively compared the postoperative outcomes and adverse events of patients with SMH who underwent the combination of PPV and subretinal rt-PA injection, between the two distinct visualization systems.
Methods
Study design and participants
A retrospective cohort study was conducted at the Ophthalmology Department of Peking Union Medical College Hospital (PUMCH) in Beijing, China. Institutional Review Board/Ethics Committee approval for this study (No. S-K1993) was obtained from PUMCH, adhering to the principles of the Declaration of Helsinki. Written informed consent was obtained from all participants.
Patients diagnosed with SMH who underwent PPV and subretinal injection of rt-PA from March 1, 2021, to November 1, 2023, were reviewed. Inclusion criteria: (1) a confirmed diagnosis of SMH secondary to PCV, nAMD, RAM, or traumatic retinopathy. Diagnosis of PCV was established according to the EVEREST criteria37, while the other three conditions relied on a comprehensive evaluation of medical history and imaging modalities, such as color fundus photography (CFP), ultra-wide-field scanning laser ophthalmoscope (SLO), fundus fluorescein angiography (FFA), and optical coherence tomography (OCT); (2) a disease course of less than three months from the onset of SMH to the surgery date; (3) patients who received PPV and subretinal rt-PA injection, with or without concurrent cataract surgery, intravitreal anti-VEGF drug injection, or gas/silicon oil tamponade; (4) patients with detailed medical records and comprehensive ophthalmologic examinations, including measurements of the best-corrected visual acuity (BCVA, using the Snellen Chart), intraocular pressure (IOP), CFP, SLO, FFA, and OCT; (5) patients with a follow-up period of at least 6 months. Exclusion criteria: (1) patients with only hemorrhagic pigment epithelial detachment (hPED); (2) patients with concurrent ocular diseases potentially confounding SMH results, such as central serous chorioretinopathy, subretinal scars, and Best disease; (3) patients lacking sufficient medical data or possessing medical images of inadequate quality.
Study groups and measurements
Patients were categorized into two groups based on the visualization system used in the surgery: the 3D group and the TM group. Comprehensive reviews and comparisons of medical records and image data at baseline, postoperative month 1 (PM1), postoperative month 3 (PM3), and the last follow-up visit between the two groups were performed. Parameters analyzed included age, gender, affected eye, disease type, SMH type, lesion characteristics, comorbidities, surgical details, BCVA, IOP, resolution status of SMH, and the occurrence rates of adverse events during follow-up.
The resolution status of the SMH lesion was assessed by integrating information from medical records and corresponding medical images, and it was then classified into three statuses. Complete resolution of SMH was defined as the total disappearance of hemorrhagic lesion on both CFP/SLO and OCT images. If the SMH lesion underwent a noticeable change discernible by visual inspection, it was deemed partially resolved. Otherwise, it was categorized as unchanged. Lesion characteristics were evaluated using OCT images to measure the height of the SMH lesion and central retinal thickness (CRT), while the ultra-wild-field SLO images with its built-in software to measure the greatest linear dimension (GLD) and area of the SMH lesion.
Two ophthalmologists with 3–5 years of clinical experiences (XG and QZ) were involved in measuring these parameters. If the difference between the measured values was no more than 15%, the mean values were calculated and used for analysis. Otherwise, the image was remeasured after consulting with the corresponding author (YC, with over 35 years of clinical experiences). For assessing the resolution status of SMH, controversy cases were directly resolved by consulting with the corresponding author, and Cohen’s Kappa value between the two readers was calculated.
Surgical details included the total surgical time (defined as the period from the moment of eyelid retraction using a lid speculum to the moment of completing the final stitch of scleral suturing), ILM peeling time, rt-PA injection time, type of intraocular tamponade, and combined operations. The two surgeons rated their satisfaction on a continuous scale of 1 to 10 points, representing low to excellent, for the ergonomics of both visualization systems, including overall satisfaction, visual fatigue, neck discomfort, magnification and resolution of the visual field, stereoscopic sensation and time latency between operation and visualization. The mean values of their rating were used for analysis. Postoperative adverse events included ocular hypertension (defined as over 21 mmHg), retinal detachment, vitreous hemorrhage, recurrent SMH, macular hole, epiretinal membrane, retinal pigmented epithelium (RPE)/Bruch membrane break, photoreceptor/RPE atrophy, endophthalmitis, additional PPV, and additional VEGF treatment. Specifically, photoreceptor/RPE atrophy was defined as the thinning or loss of outer retinal layers or the complete loss of the RPE layer under SMH, regardless of size, as observed on OCT images.
Surgical procedure
Two proficient surgeons, YXC and HYM, conducted the surgical procedures utilizing either the Alcon NGENU-ITY 3D Visualization System (Alcon Laboratories, Fort Worth, TX, USA) or a conventional microscope (OPMI LUMERA 700; Carl Zeiss Meditec, Germany). The former is the only available 3D visualization system in our hospital and the latter is the most frequently used conventional microscopic system by the two surgeons. All subjects underwent a standard 25-gauge three-port PPV, as illustrated in Fig. 1. Subsequently, procedures encompassing posterior vitreous detachment and vitrectomy were consistently performed. Following that, peeling of the internal limiting membrane (ILM) in the posterior pole was conducted with the aid of indocyanine green (ICG) staining, aimed at reducing physical resistance and minimizing the possibility of damaging underlying structures during subretinal injection38. The rt-PA (Actilyse, Boehringer Ingelheim Pharma GmbH & Co.KG, Germany), diluted to 0.25 mg/mL, was then injected at a volume of 0.1 mL, utilizing a 41-gauge subretinal infusion needle (MedOne, Sarasota, Florida, USA) assisted by the viscous fluid control system. The injection pressure was set at 10mmHg after testing in vitro by the experienced surgeons, which was consistent with our previously study36. The injection site was meticulously chosen to fully cover the SMH lesion while preventing excessive pressure beneath the retina. Subsequently, an air-fluid exchange was conducted, and if necessary, either 14% perfluoropropane (C3F8) or silicone oil was intravitreally injected to serve as a tamponade. Following the completion of the surgery, patients were instructed to maintain a facedown position for a period of 7 days. The key steps of the surgical procedure are shown in Fig. 2.

The 3D heads-up visualization system assisted PPV for SMH. The NGENUITY 3D Visualization System integrates a 3D High Dynamic Range NGENUITY Camera designed for capturing the surgical field, presenting the visuals on the sophisticated NGENUITY 3D 4 K OLED Display. Surgeons can effectively visualize stereoscopic images by utilizing 3D Passive Polarized Glasses. When paired with the CONSTELLATION Vision System, the surgeon gains the ability to monitor real-time surgical parameters and engage in seamless collaboration with surgical nurses.

Demonstration of SMH surgery process. (A) Staining of the internal limiting membrane (ILM) using indocyanine green (ICG). (B) Delicate removal of the ILM within the macular region. (C) Prior to injection, air expulsion from the infusion needle. (D) Subretinal injection of recombinant tissue plasminogen activator (rt-PA) at the submacular hemorrhage (SMH) lesion (marked with a red triangle). (E) Following the injection, the SMH lesion exhibited diffusion beneath the retina, and the boundary became indistinct. The gray dot indicated the injection site (marked with a yellow arrow). (F) Execution of a fluid-air exchange subsequent to the injection.
Statistics
Continuous data were presented as mean ± SD or median (interquartile range). Categorical data were presented as number (percentage). The BCVA measured with a Snellen chart was converted to the logarithm of the minimum angle of resolution (logMAR) for statistical analysis. Data was analyzed using Stata 18.0 software (StataCorp. 2023. Stata Statistical Software: Release 18. College Station, TX: StataCorp LLC.). The independent two-sample t test and Mann-Whitney tests were used to compare age, SMH lesion characteristics and rt-PA injection time. Fisher’s exact tests were used to compare other baseline patient characteristics, surgical details and postoperative adverse events. General estimate equation (GEE) analysis was used to fit and compare the changes of BCVA and SMH lesion in follow-ups. The exchangeable within-group correlation structure and robust standard error type with default scale factors of divisor N were selected in the GEE models. A P value < 0.05 was considered to be statistically significant.
Results
Baseline patient characteristics SMH details
Fifty-seven patients diagnosed with SMH who underwent PPV and subretinal rt-PA treatment were reviewed. Five patients were excluded due to a disease duration of more than three months before surgery. Four patients were excluded due to insufficient follow-up time (less than three months), and another nine were excluded due to the inability to measure lesion parameters (lack of OCT imaging for 2 patients, insufficient scanning width on OCT for 2 patients, and poor image quality on CFP/SLO for 5 patients). Finally, a total of 39 patients were included and categorized into the 3D group (n = 19) and the TM group (n = 20, shown in Fig. 3). Table 1 summarizes the baseline characteristics of the included patients. The mean age was 66.10 ± 12.33 years and 60.95 ± 16.67 years in the 3D and TM group, respectively (P = 0.278). 12 (63.16%) patients in the 3D group and 12 (60.00%) patients in the TM group were males, respectively (P = 1.000).

Flowchart of the patient inclusion and exclusion process. SMH submacular hemorrhage. PPV pars plana vitrectomy. OCT optical coherence tomography. CFP color fundus photography. SLO ultra-wide-field scanning laser ophthalmoscope. 3D three-dimensional heads-up visualization system. TM traditional microscopic visualization system.
In this study, PCV (64.10%) was the primary cause of SMH, followed by nAMD (15.38%), RAM (15.38%), and traumatic retinopathy (5.13%), with no statistical differences between the two groups (P = 0.386). Fifteen patients in the 3D group (75.00%) and 14 patients in the TM group (73.68%) received anti-VEGF therapy approximately 1 week before surgery (P = 1.000). SMH type including SMH and SMH with hPED was evenly distributed in the two groups (P = 0.748). On OCT images, the height of the SMH lesion was 1171.88 ± 508.23 μm in the 3D group and 1086.21 ± 551.03 μm in the TM group (P = 0.617). On CFP/SLO images, the area of the SMH lesion in the 3D and TM groups was 44.82 ± 31.31 mm² and 54.00 ± 42.14 mm², respectively (P = 0.447). Other lesion parameters, including the GLD of SMH and CRT, also revealed similarities between the two groups. Baseline BCVA was 1.87 ± 0.61 logMAR in the 3D group and 1.81 ± 0.64 logMAR in the TM group (P = 0.767).
Comparison of surgery details
As shown in Table 2, the 3D group had a longer total surgical time than the TM group (51.36 ± 9.12 min versus 45.47 ± 8.73 min, P = 0.046), while both the ILM peeling time (4.23 ± 2.14 min versus 4.98 ± 1.92 min, P = 0.256) and the rt-PA injection time (2.98 ± 1.55 min versus 3.10 ± 1.21 min, P = 0.366) were similar between the two groups. Intraocular light intensity was lower in the 3D group than in the TM group (36.32 ± 6.20% versus 41.84 ± 6.06%, P = 0.007). C3F8 gas was used as intraocular tamponades in about 90% of cases in both groups. The combinations of other steps, such as cataract surgery and intraoperative anti-VEGF drug injection, were not different between the two groups. Regarding the ergonomic appraisals by the two surgeons, overall satisfaction appeared to be similar between the two groups. The follow-up duration was 328.0 (P25-P75: 235.0–611.0) days for the 3D group and 293.5 (P25-P75: 216.5–369.5) days for the TM group, P = 0.653.
Comparison of surgical efficacy during follow-up
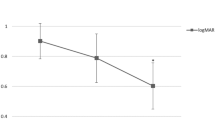
The changes of BCVA and lesion parameters during follow-up (PM1, PM3, and the last visit) were examined. As illustrated in Fig. 4, the height, GLD, and area of SMH lesions consistently decreased over time. Concurrently, BCVA also displayed a tendency to decrease throughout the follow-up period. At the last visit, the improvement in BCVA was 0.41 ± 0.59 LogMAR in the 3D group and 0.30 ± 0.60 LogMAR in the TM group, compared with baseline values (P = 0.548). Utilizing GEE analysis (Table 3), significant improvements in these lesion parameters and BCVA over time were observed. However, there were no significant differences between the 3D and TM groups. Intriguingly, post-hoc analysis (depicted by the green horizontal lines with double-sided arrows in Fig. 4, indicating a significant difference between two selected visits) revealed that, despite most lesion parameters underwent significant changes between every two consecutive visits, BCVA did not exhibit such substantial improvements, with only the BCVA of the last visit being significantly better than those of prior visits.

Comparison of changes of BCVA, IOP, and SMH lesion parameters between 3D and TM groups during follow-up using generalized estimating equation (GEE). (PM1 = postoperative month 1; PM3 = postoperative month 3; Last = last follow-up visit.) Parameters for SMH lesions encompassed the greatest linear dimension (GLD), area, and height, alongside the central retinal thickness (CRT). BCVA, CRT, GLD, area, and height of SMH lesions exhibited notable enhancements throughout the follow-up period. Statistical significances (P < 0.05), denoted by a green line segment with an asterisk at its center, were observed in the post-hoc analysis between two selected visits. However, no significant difference emerged between the two groups concerning all six parameters.
A post-hoc power analysis was conducted using the standard formula for two-sample mean comparison39, assuming a two-sided significance level of 0.05. Based on the observed within-group standard deviations and the sample sizes (3D: n = 19; TM: n = 20), the minimum detectable difference (80% power) in BCVA for each timepoint was 0.57, 0.56, and 0.58 logMAR, respectively. In contrast, the observed between-group differences at each timepoint was 0.26, 0.13, and 0.17 logMAR, corresponding to post-hoc powers of 25%, 10%, and 13%, respectively.
Postoperative SMH status and adverse events
At the last visit, 6 (31.58%), 11 (57.89%), and 2 (10.53%) patients in the 3D group achieved full resolution, partial resolution, and maintained unresolved status of SMH, respectively. In the TM group, these numbers were 5 (25.00%), 14 (70.00%), and 1 (5.00%) patient, respectively, P = 0.686. The Cohen’s Kappa value between the two readers was 0.851.
Photoreceptor/RPE atrophy (92.31%), epiretinal membrane (41.03%), and recurrent SMH (30.77%), were the most frequently observed postoperative adverse events, followed by RPE/Bruch membrane break (28.21%), retinal detachment (20.51%), vitreous hemorrhage (10.26%), high IOP (5.13%), and macular hole (2.56%). Representative adverse events are presented in Fig. 5. No cases of endophthalmitis were reported in our study. The overall occurrence rates of these adverse events did not differ between the two groups (Table 4). Moreover, their incidences were also comparable at each visit, with most of them demonstrating an increasing trend during the follow-up period (shown in Fig. 6).

Demonstrative figures of several adverse events after SMH surgery. (A) A case exhibited severe atrophy of the photoreceptors/Bruch’s membrane (indicated by a red triangle) and an epiretinal membrane (indicated by a red arrow) at 13 months postoperatively. (B) A case exhibited a distinct retinal pigment epithelium (RPE)/Bruch’s membrane break at the injection site (marked with a yellow triangle) and the presence of an epiretinal membrane (marked with a yellow arrow) at 3 months postoperatively. (C) A case presented with a large macular hole (marked with a blue triangle) at 3 months postoperatively. (E-F) The fundus images correspond to a case at baseline, 1 week postoperatively, and 3 months postoperatively, respectively. This case experienced recurrent submacular hemorrhage and retinal detachment, leading to additional pars plana vitrectomy (PPV) with silicone tamponade thereafter.

Detailed comparison of the occurrence of postoperative adverse events between 3D and TM groups at each follow-up. The incidence rates of most adverse events exhibited a similar increasing trend between the two groups during the follow-up period. The three most frequently observed adverse events at the last visit were photoreceptor/RPE atrophy (94.72% in 3D vs. 90.00% in TM, P = 1.000), epiretinal membrane (52.63% in 3D vs. 30.00% in TM, P = 0.200), and recurrent SMH (31.58% in 3D vs. 25.00% in TM, P = 0.731).
By the last visit, 13 (68.42%) patients in the 3D group and 9 (45.00%) patients in the TM group received additional anti-VEGF therapies (P = 0.200). Additionally, 3 (15.00%) patients in the 3D group and 3 (15.79%) patients in the TM group underwent additional PPVs, respectively (P = 1.000).
Stratified analysis by different fundus conditions and exploration of possible factors interacting with study groups on surgical outcomes
We further performed a stratified analysis to present baseline characteristics and surgical outcomes according to fundus conditions, as detailed in Table S1. Since PCV was the primary cause of SMH in our cohort, we additionally stratified PCV patients into the 3D (n = 11) and TM (n = 14) groups. As shown in the table, both baseline characteristics and surgical outcomes appeared comparable between the two groups. However, given the limited sample size, further comparative analysis was not performed.
To investigate whether the effect of using the 3D or TM system on surgical outcomes was influenced by other potential interacting factors, we performed interaction analyses using logistic or linear regression models, depending on the type of outcome variable. As shown in Table S2, for the five primary outcomes, including total improvement in BCVA, postoperative SMH status, number of additional anti-VEGF treatments, occurrence of RPE atrophy at PM1, and occurrence of ERM at PM3, no significant interaction effects were observed for most listed factors, except for the type and height of SMH. With increasing lesion complexity (from subretinal hemorrhage alone to both subretinal and sub-RPE hemorrhage), patients in the 3D group tended to require more additional anti-VEGF treatments (coefficient = 2.751, P = 0.014). Similarly, as SMH height increased, patients in the 3D group tended to show less BCVA improvement (coefficient = − 0.001, P = 0.025). However, after correction for multiple comparisons, these interaction effects were no longer statistically significant.
Discussion
In this retrospective cohort study, we compared the postoperative outcomes and long-term adverse events after PPV combined with subretinal rt-PA injection for SMH, mainly in patients with PCV, using the 3D and TM visualization systems. The results suggested no significant differences in overall outcomes, indicating that both systems perform comparably in assisting with this type of retinal surgery.
SMH is closely related to nAMD. Poliner’s study revealed that 17% of AMD patients with PED ultimately developed SMH40. Recognizing the significant occurrence of PCV and its high incidence of SMH in Asians41, our study differentiated PCV from nAMD for clarity. According to Stanescu-Segall et al.‘s comprehensive review on SMH in 201622, SMH impairs retinal function mainly by blocking retinal nutrient and waste exchange with the RPE and causing photoreceptor damage through traction from fibrin clots and iron-driven free radical generation in the Fenton reaction. They also indicated that combined treatment modalities, including PPV, subretinal rt-PA, intravitreal gas, and anti-VEGF therapy, can significantly enhance visual acuity from 20/1000 to 20/400. However, it is imperative to acknowledge potential post-operative adverse events associated with this multi-step procedure42,43,44. Meticulous consideration of these safety issues is of great importance to avoid iatrogenic harm. Considering the advantages of the 3D head-up system over the TM system mentioned earlier, it is worth exploring whether the two systems differ in terms of visual outcomes and postoperative safety for such patients undergoing PPV and subretinal injection of rt-PA.
Our study revealed no significant differences between the 3D and TM groups in terms of baseline patient characteristics, type of SMH, lesion parameters, BCVA, surgical details, and follow-up period. Though the total surgical time was longer in the 3D group, it was interesting to notice that key steps, including the ILM peeling time and submacular injection time, were similar between the two systems, since previous studies have reported a longer macular peeling time or total surgical time with the 3D visualization system for other diseases35,45. However, more recent studies generally showed no difference in surgical time using the 3D and TM systems46. This phenomenon might be understandable because a new technique always accompanies with an initial learning curve. The intraocular light intensity tended to be lower in the 3D group, which is consistent with other reports31,46. Although ergonomic appraisals of the two systems appears similar, the two surgeons suggested that the 3D system could reduce the strong light reflection from gas bubble when performing the air-fluid exchange47. Of note, these results need to be interpreted with caution, as only two surgeons provided subjective feedback and subsequent statistical analysis was limited. More surgeons are needed to verify these differences between the two visualization systems.
GEE analysis revealed no statistically significant differences between the 3D and TM groups in the improvement of SMH lesion parameters—including GLD, area, height, and CRT—during follow-up. Similarly, there was no difference in BCVA change between the groups, indicating comparable efficacy in facilitating PPV with subretinal rt-PA injection for SMH treatment. However, since the confidence intervals for BCVA improvement in both groups are wide (0.41 ± 0.59 LogMAR in the 3D group and 0.30 ± 0.60 LogMAR in the TM group), there might be a clinically meaningful but undetected difference between the two groups. Future studies with larger sample size could help shrink the confidence intervals and obtain a more robust comparison.
We also comprehensively assessed the postoperative adverse events, revealing that photoreceptor/RPE atrophy (92.31%), epiretinal membrane (41.03%), and recurrent SMH (30.77%) were most frequently seen. The occurrence rates in each follow-up were similar between the two groups among all the adverse events. This was consistent with other studies that also reported no difference in short-term postoperative complications for various retinal diseases, like macular hole, epiretinal membrane, and retinal detachment34,35,48. The incidence rates of photoreceptor/RPE damage and epiretinal membrane seem to be higher than previous publications. Considering our medical center, PUMCH, functions as a tertiary referral institution in China, typically receiving patients with SMH diagnosed from lower-level hospitals, contributing to significant treatment delays compared to other studies with a disease duration of two days to two weeks49,50. This delay may, in part, account for the high prevalence of postoperative photoreceptor/RPE atrophy. In addition, our study extended follow-up time to a median of approximately 300 days, which is longer than those recorded in other studies (6 ~ 8 weeks)49,51. This might also partially explain the high rate of photoreceptor/RPE and ERM occurrence. Thus, our study further documented the long-term safety of the 3D visualization system involving subretinal operations.
To further identify potential factors that might influence the relationship between study groups and surgical outcomes, we conducted interaction analyses involving several patient and lesion characteristics, such as ocular conditions and key lesion parameters. The results suggested that the 3D system might perform less favorably than the TM system in certain subgroups, particularly in patients with more complex lesions (subretinal and sub-RPE hemorrhage versus subretinal hemorrhage alone) and those with greater SMH height (Table S2). Although these interaction effects were no longer significant after correction for multiple comparisons, the findings raise the concern that the 3D system may be less capable than direct visualization through the microscope in optimally displaying highly complex SMH lesions. Further studies with larger sample sizes are warranted to verify this hypothesis.
We also noticed some other interesting results. The postoperative BCVA did not exhibit as marked improvements as the lesion parameters, reaching statistical significance only at the final assessment. As mentioned earlier, the substantial occurrence of photoreceptor/RPE atrophy and other adverse events may explain the incongruence between changes in BCVA and SMH lesion parameters. Thus, the impact of earlier surgical intervention on visual outcomes necessitates further investigation.
Several issues with the current 3D system need to be addressed. One issue is the lack of an auto-focus function47, which requires surgeons to frequently refocus the image on the display. Another problem is the screen’s viewing angle. While the digital display provides the surgical team with clear visualization of the surgical field, optimal viewing is achieved only from the middle front of the screen. Deviation from this position results in reduced brightness and diminished stereoscopic effects. Additionally, since surgeons need to wear specially designed 3D glasses, it is important to design the glasses to accommodate individuals who wear prescription glasses simultaneously. Failure to address this could lead to discomfort and an increased risk of accidental dislodgment of the 3D glasses, potentially raising the risk of perioperative infections.
Our study has some limitations. First, the retrospective study design has inherent limitations, such as selection bias, which may compromise the reliability of data analysis. For example, for safety consideration, patients with small or shallow SMH may be less likely to undergo 3D surgeries by the two surgeons in our study. In addition, the limited sample size may have reduced the ability to detect statistically significant differences between groups. Future prospective cohort studies or randomized controlled trials with larger sample sizes are warranted to validate and strengthen our findings. Second, only two surgeons conducted 3D surgeries in our institution. This limitation might cause inter-surgeon variations, such as surgical experience and preference, to confound study results. Future research with more participating surgeons could help resolve these variations. Third, 3D visualization systems are currently costly and typically only available at higher-level hospitals, which might lead to patient selection bias and treatment delays, potentially confounding the outcomes of SMH. Wider application of these systems and future research based on their use might help address this limitation. Fourth, in our study, the definition of photoreceptor/RPE atrophy could be overly sensitive to reflect clinical significance, as small areas of atrophy may not substantially impair visual function. Therefore, future studies should consider a proper definition of clinically meaningful photoreceptor/RPE atrophy. Fifth, the imbalanced distribution of patients among the diseases leading to SMH limit the potential for further sub-analysis. Thus, our results may have limited applicability to diseases such as RAM and traumatic retinopathy.
Conclusions
In conclusion, our study found no significant difference in long-term outcomes or adverse events between the 3D and TM visualization systems for assisting PPV with subretinal rt-PA injection in patients with SMH, particularly those with PCV. As the cost of 3D systems decreases in the future, both systems may become feasible for use in vitrectomies, including those involving subretinal operations. Further investigation with a prospective study design and a larger sample size of patients and surgeons is needed to validate the benefits of this type of systems for more complex SMH lesions.
Data availability
After approval by the Institutional Review Board/Ethics Committee of PUMCH, the datasets generated and analyzed during the current study are available from the corresponding author (YC) on reasonable request.
Abbreviations
- SMH:
-
Submacular hemorrhage
- PPV:
-
Pars plana vitrectomy
- PCV:
-
Polypoidal choroidal vasculopathy
- nAMD:
-
Neovascular age-related macular degeneration
- RAM:
-
Retinal arterial microaneurysm
- rt-PA:
-
Recombinant tissue plasminogen activator
- 3D:
-
Three-dimensional
- TM:
-
Traditional microscopes
- SLO:
-
Scanning laser ophthalmoscope
- FFA:
-
Fundus fluorescein angiography
- OCT:
-
Optical coherence tomography
- BCVA:
-
Best-corrected visual acuity
- IOP:
-
Intraocular pressure
- hPED:
-
Hemorrhagic pigment epithelial detachment
- PUMCH:
-
Peking Union Medical College Hospital
- PM1:
-
Postoperative month 1
- PM3:
-
Postoperative month 3
- CRT:
-
Central retinal thickness
- GLD:
-
Greatest linear dimension
- RPE:
-
Retinal pigmented epithelium
- ILM:
-
Internal limiting membrane
- ICG:
-
Indocyanine green
- C3F8:
-
Perfluoropropane
- GEE:
-
General estimate equation
References
Hochman, M. A., Seery, C. M. & Zarbin, M. A. Pathophysiology and management of subretinal hemorrhage. Surv. Ophthalmol. 42, 195–213 (1997).
Lim, J. I., Drews-Botsch, C., Sternberg, P., Capone, A. & Aaberg, T. M. Submacular hemorrhage removal. Ophthalmology 102, 1393–1399 (1995).
Glatt, H. & Machemer, R. Experimental subretinal hemorrhage in rabbits. Am. J. Ophthalmol. 94, 762–773 (1982).
Benner, J. D., Hay, A., Landers, M. B., Hjelmeland, L. M. & Morse, L. S. Fibrinolytic-assisted removal of experimental subretinal hemorrhage within seven days reduces outer retinal degeneration. Ophthalmology 101, 672–681 (1994).
Scupola, A., Coscas, G., Soubrane, G. & Balestrazzi, E. Natural history of macular subretinal hemorrhage in age-related macular degeneration. Ophthalmologica J. Int. D’ophtalmologie Int. J. Ophthalmol. Z. Fur Augenheilkunde 213 (1999).
Hattenbach, L. O., Klais, C., Koch, F. H. & Gümbel, H. O. Intravitreous injection of tissue plasminogen activator and gas in the treatment of submacular hemorrhage under various conditions. Ophthalmology 108, 1485–1492 (2001).
Avery, R. L., Fekrat, S., Hawkins, B. S. & Bressler, N. M. Natural history of subfoveal subretinal hemorrhage in age-related macular degeneration. Retina (Philadelphia Pa). 16, 183–189 (1996).
Hanscom, T. A. & Diddie, K. R. Early surgical drainage of macular subretinal hemorrhage. Arch. Ophthalmol. 105, 1722–1723. https://doi.org/10.1001/archopht.1987.01060120120037 (1987).
Tranos, P. et al. Comparison of subretinal versus intravitreal injection of Recombinant tissue plasminogen activator with gas for submacular hemorrhage secondary to wet age-related macular degeneration: treatment outcomes and brief literature review. Int. Ophthalmol. 41, 4037–4046. https://doi.org/10.1007/s10792-021-01976-x (2021).
Tal, K. et al. Retinal penetration of intravitreally injected tissue plasminogen activator: A rat model study. Ophthalmic Res. 59, 235–240. https://doi.org/10.1159/000477621 (2018).
Saito-Uchida, S., Inoue, M., Koto, T., Kato, Y. & Hirakata, A. Vitrectomy combined with subretinal injection of tissue plasminogen activator for successful treatment of massive subretinal hemorrhage. Eur. J. Ophthalmol. 31, 2588–2595. https://doi.org/10.1177/1120672120970404 (2021).
Kimura, S. et al. Outcomes of vitrectomy combined with subretinal tissue plasminogen activator injection for submacular hemorrhage associated with polypoidal choroidal vasculopathy. Jpn J. Ophthalmol. 63, 382–388. https://doi.org/10.1007/s10384-019-00679-2 (2019).
Murphy, G. S. P. et al. Tissue plasminogen activator or perfluoropropane for submacular hemorrhage in Age-Related macular degeneration: A factorial randomized clinical trial. JAMA Ophthalmol. 142, 1157–1164. https://doi.org/10.1001/jamaophthalmol.2024.4297 (2024).
Gabrielle, P. H. et al. Tissue plasminogen Activator, antiangiogenic Agents, and Age-Related macular degeneration study: A randomized controlled trial for submacular hemorrhage secondary to Age-Related macular degeneration. Ophthalmology 130, 947–957. https://doi.org/10.1016/j.ophtha.2023.04.014 (2023). Surgery.
Veritti, D., Sarao, V., Martinuzzi, D., Menzio, S. & Lanzetta, P. Submacular hemorrhage during neovascular age-related macular degeneration: a meta-analysis and meta-regression on the use of tPA and anti-VEGFs. Ophthalmologica 247, 191–202. https://doi.org/10.1159/000537939 (2024).
Barzelay, A. et al. Pneumatic displacement with intravitreal tPA injection versus vitrectomy with sub retinal tPA injection in small and medium sub macular hemorrhages- a multicenter comparative study. BMC Ophthalmol. 24, 218. https://doi.org/10.1186/s12886-024-03468-9 (2024).
Chew, G. W. M. et al. Manch. Protoc. Retina 42, 11–18 https://doi.org/10.1097/iae.0000000000003294 (2022).
Tripepi, D. et al. The role of subretinal injection in ophthalmic surgery: therapeutic agent delivery and other indications. Int. J. Mol. Sci. 24 https://doi.org/10.3390/ijms241310535 (2023).
Toth, C. A., Benner, J. D., Hjelmeland, L. M., Landers, M. B. & Morse, L. S. Ultramicrosurgical removal of subretinal hemorrhage in cats. Am. J. Ophthalmol. 113, 175–182 (1992).
Bennett, S. R., Folk, J. C., Blodi, C. F. & Klugman, M. Factors prognostic of visual outcome in patients with subretinal hemorrhage. Am. J. Ophthalmol. 109, 33–37 (1990).
Lewis, H. Intraoperative fibrinolysis of submacular hemorrhage with tissue plasminogen activator and surgical drainage. Am. J. Ophthalmol. 118, 559–568 (1994).
Stanescu-Segall, D., Balta, F. & Jackson, T. L. Submacular hemorrhage in neovascular age-related macular degeneration: A synthesis of the literature. Surv. Ophthalmol. 61, 18–32. https://doi.org/10.1016/j.survophthal.2015.04.004 (2016).
Kadonosono, K. et al. Displacement of submacular hemorrhages in age-related macular degeneration with subretinal tissue plasminogen activator and air. Ophthalmology 122, 123–128. https://doi.org/10.1016/j.ophtha.2014.07.027 (2015).
Peyman, G. A. et al. Tissue plasminogen activating factor assisted removal of subretinal hemorrhage. Ophthalmic Surg. 22, 575–582 (1991).
Johnson, M. W., Olsen, K. R. & Hernandez, E. Tissue plasminogen activator thrombolysis during surgical evacuation of experimental subretinal hemorrhage. Ophthalmology 99, 515–521. https://doi.org/10.1016/s0161-6420(92)31939-6 (1992).
Hwang, S. H., Kim, Y. J., Cho, J. B., Kim, K. G. & Nam, D. H. Digital image enhancement using deep learning algorithm in 3D heads-up vitreoretinal surgery. Sci. Rep. 15, 18429. https://doi.org/10.1038/s41598-025-98801-7 (2025).
Mastropasqua, R. et al. New mixed reality headset: first exploratory use in intraocular surgery and telementoring. Ophthalmol. Ther. 14, 1597–1609. https://doi.org/10.1007/s40123-025-01117-y (2025).
Mastropasqua, R., Quarta, A., Ruggeri, M. L. & Mastropasqua, L. Enhancing precision and clarity with new digital color assistant in 3D Heads-Up vitreoretinal surgery. Ophthalmol. Ther. 14, 805–814. https://doi.org/10.1007/s40123-025-01106-1 (2025).
Iuliano, L., Corbelli, E., Bandello, F. & Codenotti, M. Lessons from the vitreoretinal theater using the Beyeonics One™ surgical visualization system. Eur. J. Ophthalmol. 11206721251349248 https://doi.org/10.1177/11206721251349248 (2025).
Eckardt, C., Paulo, E. B. & HEADS-UP SURGERY FOR VITREORETINAL PROCEDURES: an experimental and clinical study. Retina (Philadelphia Pa). 36, 137–147. https://doi.org/10.1097/IAE.0000000000000689 (2016).
Wang, Y. et al. A systematic review and Meta-analysis. Retina (Philadelphia Pa). 42, 1151–1160. https://doi.org/10.1097/IAE.0000000000003414 (2022).
Wang, K. et al. Three-Dimensional Heads-up cataract surgery using femtosecond laser: Efficiency, Efficacy, Safety, and medical Education-A randomized clinical trial. Translational Vis. Sci. Technol. 10, 4. https://doi.org/10.1167/tvst.10.9.4 (2021).
Romano, M. R. et al. Evaluation of 3D heads-up vitrectomy: outcomes of psychometric skills testing and surgeon satisfaction. Eye (Lond). 32, 1093–1098. https://doi.org/10.1038/s41433-018-0027-1 (2018).
Coppola, M., La Spina, C., Rabiolo, A., Querques, G. & Bandello, F. Heads-up 3D vision system for retinal detachment surgery. Int. J. Retina Vitreous. 3, 46. https://doi.org/10.1186/s40942-017-0099-2 (2017).
Talcott, K. E. et al. Comparison of a Three-Dimensional Heads-Up display surgical platform with a standard operating microscope for macular surgery. Ophthalmol. Retina. 3, 244–251. https://doi.org/10.1016/j.oret.2018.10.016 (2019).
Zhao, X. et al. Three-dimensional heads-up system assisted Pars plana vitrectomy and subretinal Recombinant tissue plasminogen activator injection for submacular hemorrhage. Eye Vis. 10, 8. https://doi.org/10.1186/s40662-023-00326-5 (2023).
Koh, A. et al. EVEREST study: efficacy and safety of verteporfin photodynamic therapy in combination with Ranibizumab or alone versus Ranibizumab monotherapy in patients with symptomatic macular polypoidal choroidal vasculopathy. Retina 32, 1453–1464. https://doi.org/10.1097/IAE.0b013e31824f91e8 (2012).
Okanouchi, T., Toshima, S., Kimura, S., Morizane, Y. & Shiraga, F. Novel technique for subretinal injection using local removal of the internal limiting membrane. Retina 36, 1035–1038. https://doi.org/10.1097/iae.0000000000001029 (2016).
Cohen, J. Statistical Power Analysis for the Behavioral Sciences (routledge, 2013).
Poliner, L. S., Olk, R. J., Burgess, D. & Gordon, M. E. Natural history of retinal pigment epithelial detachments in age-related macular degeneration. Ophthalmology 93, 543–551. https://doi.org/10.1016/s0161-6420(86)33703-5 (1986).
Kunavisarut, P. et al. Submacular hemorrhage: visual outcomes and prognostic factors. Asia Pac. J. Ophthalmol. (Phila). 7, 109–113. https://doi.org/10.22608/apo.2017389 (2018).
Abdulaal, M. et al. Early surgical displacement of submacular hemorrhage without tissue plasminogen activator use: one-year outcomes. Can. J. Ophthalmol. https://doi.org/10.1016/j.jcjo.2023.10.005 (2023).
Handa, S., Dogra, M., Tigari, B., Katoch, D. & Singh, R. Displacement of submacular hemorrhage with vitrectomy combined with subretinal balanced salt solution and air. RETINA 43, 2194–2198. https://doi.org/10.1097/iae.0000000000003879 (2023).
Wu, J. et al. Visual Recovery and Prognosis in the Treatment of Submacular Hemorrhage due to Polypoidal Choroidal Vasculopathy and Retinal Arterial Macroaneurysm: A Retrospective Study. Int. J. Clin. Pract. 2023, 3880297. https://doi.org/10.1155/2023/3880297 (2023).
Asani, B. et al. 3D Heads-Up display vs. Standard operating microscope vitrectomy for rhegmatogenous retinal detachment. Front. Med. (Lausanne). 7, 615515. https://doi.org/10.3389/fmed.2020.615515 (2020).
Razavi, P., Cakir, B., Baldwin, G., D’Amico, D. J. & Miller, J. B. Heads-Up Three-Dimensional viewing systems in vitreoretinal surgery: an updated perspective. Clin. Ophthalmol. 17, 2539–2552. https://doi.org/10.2147/opth.S424229 (2023).
Liu, J., Wu, D., Ren, X. & Li, X. Clinical experience of using the NGENUITY three-dimensional surgery system in ophthalmic surgical procedures. Acta Ophthalmol. 99, e101–e108. https://doi.org/10.1111/aos.14518 (2021).
Del Turco, C. et al. Heads-up 3D eye surgery: safety outcomes and technological review after 2 years of day-to-day use. Eur. J. Ophthalmol. 11206721211012856 https://doi.org/10.1177/11206721211012856 (2021).
Ali Said, Y., Dewilde, E. & Stalmans, P. Visual outcome after vitrectomy with subretinal tPA injection to treat submacular hemorrhage secondary to Age-Related macular degeneration or macroaneurysm. J. Ophthalmol. 2021 (3160963). https://doi.org/10.1155/2021/3160963 (2021).
Ozer, O. et al. The effect of subretinal Recombinant tissue plasminogen activator application for submacular hemorrhage. Retina Vitreous. 33, 129 (2024).
Ogata, M. et al. Displacement of submacular hemorrhage secondary to age-related macular degeneration with subretinal injection of air and tissue plasminogen activator. Sci. Rep. 12, 22139. https://doi.org/10.1038/s41598-022-26289-6 (2022).
Funding
This research was supported by the following fundings: National Natural Science Foundation of China (82301241 [XYZ]), National Natural Science Foundation of China (82271112 [YXC]), The Fundamental Research Funds for the Central Universities, Peking Union Medical College (3332024201 [XYZ]), Peking Union Medical College Hospital Talent Cultivation Program (Category D, UHB12268 [XYZ]), National High Level Hospital Clinical Research Funding, China (2022-PUMCH-B-101 [YXC]). The funding organizations had no role in the design or conduct of this research.
Author information
Authors and Affiliations
Contributions
XG contributed to the concept of the study. XG and XZ designed the study and did the literature search. XG, QZ, and YW collected the data. XG, QZ, and XZ did the data analysis and data interpretation. XG drafted the manuscript. HM and YC critically revised the manuscript. YC provided research funding, coordinated the research, and oversaw the project. All authors had access to all the raw datasets and the corresponding author (YC) has verified the data and had final decision to submit for publication. All authors reviewed and approved the final manuscript.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval and consent to participate
Institutional Review Board/Ethics Committee approval for this study (No. S-K1993) was obtained from PUMCH, and it adhered to the principles of the Declaration of Helsinki. Written informed consent was obtained from all participants.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Gu, X., Zhao, Q., Wang, Y. et al. Comparing postoperative outcomes of three-dimensional versus traditional microscopic vitrectomy and subretinal rt-PA injection for submacular hemorrhage. Sci Rep 15, 42046 (2025). https://doi.org/10.1038/s41598-025-26031-y
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-26031-y
