
Abstract
PROMIS effectively assesses patient health, but its use in evaluating the quality of life in acute coronary syndrome (ACS) patients on PCSK9 inhibitors (PCSK9i) remains unexplored. This study examined the impact of PCSK9i on quality of life in ACS patients, comparing PCSK9i plus statin versus statin-only therapy using PROMIS-10, and analyzed the association between PROMIS scores and major adverse cardiovascular events (MACE). The EMSIACS trial is a prospective, randomized, open-label, parallel-group, multicenter study registered at ClinicalTrials.gov (NCT04100434). This paper presents the exploratory outcomes of this trial. From September 2020 to March 2022, a total of 500 ACS patients were enrolled. Patients were randomly assigned in a 1:1 ratio to receive Evolocumab plus statin therapy or statin-only therapy. The quality of life was assessed using PROMIS 10 at baseline, week 12, and week 48. PROMIS 10 includes two summary scores: Global Physical Health (GPH, including physical health, physical function, fatigue and pain intensity) and Global Mental Health (GMH, including overall quality of life, mental health, satisfaction with social activities, and emotional problems). At week 48, MACE were evaluated in two groups. At week 12, Evolocumab significantly improved Global Physical Health (GPH) (P < 0.001) and Global Mental Health (GMH) scores (P < 0.001), particularly in pain intensity, mental health, and social activity satisfaction (P < 0.001). By week 48, both groups improved significantly from baseline, with no significant differences between them(GPH: P = 0.120; GMH: P = 0.105). Emotional problems worsened in patients with MACE (P = 0.015). Exploratory analysis suggested that PCSK9i significantly improved short-term quality of life in ACS patients outperforming statins especially in pain intensity, mental health, and social activity satisfaction. In the long term, PCSK9i sustained quality of life improvements. The occurrence of MACE in ACS patients may associate with emotional problems.
Clinical trial registration number: NCT04100434.
Similar content being viewed by others

Introduction
ACS is a rapid onset and serious cardiovascular disease with poor prognosis1, low rate of blood lipid attainment2, and often accompanied by multiple complications such as arrhythmia and acute heart failure, which pose a great threat to patients’ physical and mental health and create a heavy burden on society3. The experiences of ACS patients during the course of their illness can significantly affect their psycological state. Patients with ACS are prone to psychological issues such as anxiety and depression, which can adversely affect their prognosis in turn4,5,6.
Recent guidelines recommend that the addition of PCSK9i should be considered for patients who do not meet their low-density lipoprotein cholesterol (LDL-C) target despite using the maximum tolerated dose of statins7. Studies have shown that using PCSK9i, either alone or in combination with statins, reduces the risk of MACE in patients with ACS8,9.
Previous studies have used the EuroQol 5 dimensions questionnaire (EQ-5D) to find that PCSK9i has a positive impact on quality of life of patients with high-risk and extremely high-risk cardiovascular diseases10. Compared to EQ-5D, Patient-Reported Outcomes Measurement Information System(PROMIS) 10 Global Health, is more comprehensive, with a finer scoring system11. Studies have shown that PROMIS is effective for both the general population and patients with specific chronic diseases12,13,14. However, there are no studies to date using PROMIS 10 to investigate the impact of PCSK9i on quality of life of ACS patients. This study aims to use the PROMIS 10 scale to explore the effectiveness of PCSK9i in improving quality of life of ACS patients, compare the effects of PCSK9i combined with statin therapy versus statin monotherapy on ACS patient quality of life, and examine changes in PROMIS 10 across various dimensions. Additionally, the study will explore the correlation between PROMIS scores and the occurrence of MACE in ACS patients.
Methods
Study design and population
The EMSIACS15 is a prospective, open-label, multicenter, randomized clinical trial (ClinicalTrials.gov [NCT04100434]), a study protocol published with the first registration date of 24/09/2019. This study presents exploratory outcomes from this trial. The EMSIACS enrolled 500 ACS patients diagnosed between September 2020 and August 2022 across six top-tier hospitals in Tianjin. The included ACS patients were diagnosed with non-ST elevation myocardial infarction (NSTEMI), acute ST elevation myocardial infarction (STEMI) within 24 h, or unstable angina within 72 h. We performed stratified block randomization using the PROC PLAN procedure in SAS 9.4, with the stratification factors being the number of strata and blocks. Specifically, the number of strata (i.e., centers) was set to 7, and the number of blocks was set to 4. The patients were randomly assigned in a 1:1 ratio to two treatment groups: a group receiving Evolocumab combined with statins, and a group receiving statins alone. The patients were followed for one year. The baseline demographic features, clinical examinations, laboratory tests, questionnaires, and follow-up were carried out by the research team at Tianjin Chest Hospital. This study is an exploratory outcome of EMSIACS.
Inclusion and exclusion criteria
Inclusion criteria: Patients aged ≥ 18 and ≤ 85 with recent hospitalization for acute phase ACS are eligible for inclusion in this study. The diagnosis for ACS in this study is defined as non-ST-segment elevation myocardial infarction (MI) within 24 h of onset, acute ST-segment elevation MI within 24 h of onset, or unstable angina within 72 h of onset. Additional inclusion criteria are based on patients with elevated LDL-C levels who meet one of the following four conditions: (1) prior to the study, patients who received intensive statins for more than 4weeks (the same dose of statin therapy has been sustained for the past 4weeks), having LDL-C levels ≥ 70 mg/dl (≥ 1.8mmol/L) or non-HDL-C ≥ 100 mg/dl (≥ 2.6mmol/L); (2) prior to the study, patients who received moderate-intensity statin therapy for more than 4weeks (the same dose of statin therapy has been sustained for the past 4weeks), having LDL-C levels ≥ 90 mg/dl (≥ 2.3mmol/L) or non-HDL-C ≥ 120 mg/dl (≥ 3.1mmol/L); (3) prior to the study, patients who do not receive any statin therapy or discontinue statin therapy, having LDL-C ≥ 125 mg/dl (≥ 3.2mmol/L) or non-HDL-C ≥ 155 mg/dl (≥ 4.0mmol/L); and (4) prior to the study, patients who do not receive any statin therapy or discontinue statin therapy, having LDL-C L125 mg/dL (≤ 3.2mmol/L).
Exclusion criteria: (1) patients unable to understand the research requirements or refuse to sign the informed consent form; (2) patients with unstable clinical status (e.g., hemodynamics or ECG instability); (3) patients with uncontrolled arrhythmia, defined as recurrent or symptomatic ventricular tachycardia and atrial fibrillation with rapid ventricular reaction that the drug cannot control within 3months prior to screening; (4) patients with severe renal insufficiency, defined as the estimated glomerular filtration rate (eGFR) < 30 ml/min/1.73m2; (5) patients with active liver diseases or liver dysfunction, either recorded in the patient’s medical record or defined as an increase in aspartate aminotransferase (AST) or alanine aminotransferase (ALT) more than 3 times above the upper limit of normal range; (6) patients with intolerance to rosuvastatin (any dose) or to other statins; (7) patients with known allergies to contrast agents, heparin, aspirin, ticagrelor, or clopidogrel; (8) patients with known allergies to supplements required for the use of the drug; (9) patients who have been treated with evolocumab or other PCSK9 inhibitors; (10) patients who have received cholesterol ester transfer protein inhibitors treatment 12months prior to screening; (11) patients who have received systemic steroid or cyclosporine treatment in the past 3months; (12) patients with known infections, hemorrhages, metabolic or endocrine disorders as determined by the researchers; (13) patients who have been included in other studies; (14) patients with active malignant tumor in need of treatment; and (15) women who are fertile (age < 50 years, menstruation in the past 12months) and have not received tubal ligation, oophorectomy, or hysterectomy.
Ethical considerations
The study was reviewed and approved by the Institutional Ethics Committee of Tianjin Chest Hospital (IEC No. 2019KY-019-01), and all enrolled patients provided informed consent. We confirm that all methods were performed in accordance with the relevant guidelines.
Drug administration and dosage
(1) Statins: Based on the 2020 edition of the Expert Consensus on Clinical Pathway of Blood Lipid Management in Patients with Acute Coronary Syndrome, all ACS patients received moderate-intensity statin therapy, either Rosuvastatin (10 mg) or Atorvastatin (20 mg) daily during the study period.
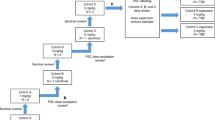
(2) Evolocumab (Repatha®): Within 72 h of ACS diagnosis, patients received a single 140 mg subcutaneous injection of Evolocumab. Subsequently, the injection was repeated every two weeks (a total of 24 injections during the 48-week follow-up period). The injection was administered using a prefilled autoinjector in areas like the abdomen, thigh, or upper arm, ensuring no tenderness, bruising, swelling, or sclerosis at the injection site.(Fig. 1).

Study flow diagram.
Data collection and follow-up
Baseline patient characteristics were assessed, including:
(1) Demographic information (gender, age); (2) Physical status (height, weight); (3) Medical history (hypertension, diabetes, hyperlipidemia, heart disease, peptic ulcers, peripheral vascular disease, stroke, surgical history); (4) Treatment history (surgical, pharmacological); (5) Lifestyle (smoking, alcohol use); (6) Current medical history (ACS type, number of affected coronary vessels, lesion locations), (7) Echocardiogram; (8) Laboratory tests (CBC, liver function, kidney function, lipid profile, myocardial injury biomarkers).
The PROMIS 10 was used to assess patients’ quality of life at baseline, 12 weeks, and 48 weeks. At week 48, MACE events (defined as coronary heart disease death, nonfatal myocardial infarction, hospitalization for unstable angina, unplanned coronary revascularization, and stroke) were recorded.
The PROMIS 10, funded by the National Institutes of Health (NIH), consists of 10 items that generate two scores: Global Physical Health (GPH) and Global Mental Health (GMH)15. GPH includes physical health, physical function, fatigue, and pain intensity, while GMH includes overall quality of life, mental health, satisfaction with social activities, and emotional problems. Scores are calculated using a web-based tool (https://www.orthotoolkit.com/promis-10/ ), and are standardized with a mean t-score of 50 (standard deviation = 10), where higher scores indicate better health-related quality of life.
Study outcomes
The primary endpoint of this study was the change in PROMIS GPH and GMH scores between baseline, 12 weeks, and 48 weeks.
Secondary endpoints included:
(1) Changes in individual PROMIS 10 item scores and percentage change from baseline, 12 weeks, and 48 weeks,
(2) MACE occurrence at 48 weeks.
Statistical analysis
Normally distributed continuous data were expressed as mean ± standard deviation (SD), and non-normally distributed data were presented as median and interquartile range. Between-group comparisons were made using independent t-tests or rank-sum tests, while within-group comparisons were made using paired t-tests. PROMIS score changes were expressed as means with 95% confidence intervals. Statistical analyses were conducted using SPSS 26.0 and GraphPad Prism 8. A P-value of < 0.05 was considered statistically significant.
Results
Clinical characteristics
This study included a total of 500 patients (Statin treatment: 250 cases, Medium-dose statin combined with Evolocumab treatment: 250 cases). Table 1 reports the baseline characteristics of the two groups of patients. The average (25%, 75%) age of all patients was 61 (53, 67) years, with 410 patients (82%) being male (Table 1).
Addition of evolocumab outperforms statin therapy alone in lipid-lowering
As the primary endpoint of the EMSIACS trial, LDL-C levels in the evolocumab group decreased significantly from 3.45 mmol/L to 2.41 mmol/L on the 3rd day of treatment (P < 0.001), continued to decreased significantly to 1.03 mmol/L at week 4 (P < 0.001), and remained stable thereafter. At week 48, the LDL-C level in the evolocumab group was 1.07mmol/L, which was significantly lower than the 2.10mmol/L in the control group (P < 0.001) (Fig. 2). Next, the distribution of LDL-C levels was analyzed. After 4 weeks of treatment, the evolocumab group had a higher proportion of low levels of LDL-C than the control group (≤ 1.8 mmol/L: 88.96% vs. 23.42%; ≤ 1.4 mmol/L: 74.03% vs. 24.68%; ≤ 1.0 mmol/L: 52.60% vs. 1.90%; all P < 0.001). Similar results were observed after 12 weeks of treatment (≤ 1.8 mmol/L: 89.74% vs. 39.47%; ≤ 1.4 mmol/L: 74.36% vs. 10.53%; ≤ 1.0 mmol/L: 47.44% vs. 2.63%; all P < 0.001) (Fig. 3).

LDL-C level changes in PCSK9i and statin groups.

LDL-C level distribution in PCSK9i and Statin groups at baseline, week 4 and week 12.
Comparison of PROMIS GPH and PROMIS GMH scores between evolocumab group and statins group
At baseline, there was no statistically significant difference in the average (SD) PROMIS GPH scores between the Evolocumab and Statins groups [43.46 (4.96) vs. 44.20 (4.97); P = 0.141]. At 12 weeks, the PROMIS GPH score of 249 patients in the Evolocumab group was significantly different from baseline [44.21 (4.98) vs. 49.87 (7.09), P < 0.001]. At 48 weeks, the improvement in PROMIS GPH for 234 Evolocumab group patients was similar to that at 12 weeks, and was significantly different from baseline [52.87 (6.20) vs. 44.14 (4.96); P < 0.001]. However, there was no statistically significant difference between the Evolocumab and Statins groups at 48 weeks [52.87 (6.20) vs. 51.83 (6.58); P = 0.120], and the change in PROMIS GPH score between the two groups was also not statistically significant [Evolocumab group: 8.73 (7.91) vs. Statins group: 8.30 (8.38); P = 0.600] (Table 2; Fig. 4a).

Differences in PROMIS scores for PCSK9i and Statins. a and d Change of PROMIS scores at baseline, week 12, and week 48 of the two groups. (b-c) Comparison of GPH instrument items between the two groups at week 12, and week 48. (e-f) Comparison of GMH instrument items between the two groups at week 12, and week 48. PH, physical health; PF, physical function; FA, fatigue; PI, pain intensity; QoL, overall quality of life; MH, mental health; SA, satisfaction with social activities; EP, emotional problems.
Similarly, at baseline, there was no statistically significant difference in the average (SD) PROMIS GMH scores between the Evolocumab and Statin groups [46.51 (6.38) vs. 45.99 (5.90); P = 0.401]. At 12 weeks, the PROMIS GMH score of 249 Evolocumab patients was significantly higher than baseline [52.09 (7.75) vs. 46.54 (6.38); P < 0.001]. At 48 weeks, the improvement in PROMIS GMH for 234 Evolocumab group patients was similar to that at 12 weeks, with a significant difference from baseline [46.40 (6.33) vs. 54.77 (7.64); P < 0.001]. However, the difference compared to the Statins group was not statistically significant [54.77 (7.64) vs. 53.49 (8.54); P = 0.105], and the change between the two groups was also not statistically significant [Evolocumab group: 8.37 (10.31) vs. Statins group: 7.43 (11.11); P = 0.593] (Table 2; Fig. 4d).
Comparison of PROMIS 10 scale improvements in evolocumab and statin groups
At baseline, the fatigue score [4.16 (0.66) vs. 4.00 (0.72); P = 0.010] and social activity satisfaction score [3.18 (0.86) vs. 3.02 (0.87); P = 0.049] in the Evolocumab group were significantly different from the Statins group, while the other scores showed no statistically significant differences at baseline (P > 0.05) (Table 3).
At 12 weeks, the changes in pain intensity score in the GPH scale (43.20% vs. 13.40%, P < 0.001), mental health score in the GMH scale (31.15% vs. 20.50%, P = 0.016), and social activity satisfaction score (26.84% vs. 20.04%, P = 0.033) were significantly different between the Evolocumab and Statins groups (Table 3; Fig. 4b, e).
At 48 weeks, there were no statistically significant differences in the improvement of the individual items between the two groups compared to baseline (P > 0.05), but there were significant differences between the Evolocumab and Statins groups in the physical health (P = 0.007), mental health (P = 0.032), and social activity satisfaction scores (P = 0.009) (Table 3; Fig. 4c, f).
Changes in PROMIS 10 scale scores for each item in the evolocumab group
At 12 weeks, the Evolocumab group showed statistically significant improvements in the physical health score [3.39 (0.96) vs. 2.93 (0.83); P < 0.001] and pain intensity score [1.17 (1.99) vs. 4.05 (2.79); P < 0.001], while the physical function score showed a slight improvement [3.30 (1.10) vs. 3.17 (0.90); P = 0.209], and the fatigue score showed a slight decline [4.04 (0.70) vs. 4.16 (0.66); P = 0.055], but this change was not statistically significant. At 48 weeks, the improvement in physical health and pain intensity scores (P < 0.001) persisted, and the differences in physical function (P < 0.001) and fatigue scores (P = 0.003) were statistically significant compared to baseline (Table 4; Fig. 5a-d).

Change of PROMIS scores instrument items in PCSK9i at baseline, week 12, and week 48. (a) Change of physical health; (b) Change of physical function; (c) Change of fatigue; (d) Change of pain intensity; (e) Change of overall quality of life; (f) Change of mental health; (g) Change of satisfaction with social activities; (h) Change of emotional problems.
At 12 weeks, the Evolocumab group showed statistically significant improvements in the four items of the PROMIS GMH scale: overall quality of life [3.46 (0.90) vs. 3.01 (0.86); P < 0.001], mental health [3.80 (0.83) vs. 3.12 (0.83); P < 0.001], social activity satisfaction [3.80 (1.09) vs. 3.18 (0.86); P < 0.001], and emotional issues [4.21 (0.77) vs. 3.88 (0.87); P < 0.001]. At 48 weeks, the overall quality of life, mental health, and social activity satisfaction scores continued to improve (P < 0.001), while emotional issue scores decreased compared to 12 weeks, but the difference from baseline remained statistically significant (P = 0.002) (Table 4; Fig. 5e-h).
Comparison of changes in scores between MACE and Non-MACE patients at 48 weeks
At 48 weeks, 58 patients (12.37%) had experienced MACE. There was no statistically significant difference in the GPH (P = 0.648) and GMH (P = 0.294) scores at baseline and 12 weeks between the MACE and non-MACE groups. At week 48, the difference between MACE and non-MACE groups in GMH was statistically significant (P = 0.048)(Table 5). Regarding PROMIS 10 dimensions, the fatigue score of the MACE group was lower at 12 weeks compared to baseline, but this change was not statistically significant [3.82 (0.62) vs. 4.00 (0.65); P = 0.053]. At 48 weeks, the difference between MACE and non-MACE groups in emotional problems score was statistically significant [3.85 (1.10) vs. 4.20 (0.96); P = 0.015]. For other items, there were no significant differences between the MACE and non-MACE groups at baseline, 12 weeks, and 48 weeks (P > 0.05) (Fig. 6).

PROMIS items differences between MACE and non-MACE. (a) Differences in physical health; (b) Differences in physical function; (c) Differences in fatigue; (d) Differences in pain intensity; (e) Differences in overall quality of life; (f) Differences in mental health; (g) Differences in satisfaction with social activities; (h) Differences in emotional problems.
Discussion
Existing studies have confirmed that PCSK9 inhibitors (PCSK9i) can effectively reduce the risk of recurrent ischemic cardiovascular events in patients with a history of acute coronary syndrome (ACS) who are receiving high-intensity statins therapy, showing significant clinical advantages compared to those receiving a placebo16. Koren et al. conducted the OSLER-1 trial, which lasted over 4 years, demonstrating that Evolocumab has excellent LDL-C lowering efficacy, as well as good tolerability and safety17. Another randomized trial investigating the combination of Evolocumab or placebo with statins found no increase in neurocognitive events among patients treated with Evolocumab compared to the control group18. Multicenter observational studies on dyslipidemia also suggest that PCSK9i have good safety profiles with limited side effects19. However, there is still a lack of research exploring whether PCSK9i has a different impact on the quality of life of ACS patients compared to statin monotherapy. This study is the first to systematically explore the impact of PCSK9i on the quality of life of ACS patients using the NIH PROMIS scoring system.
At 12 weeks, the PROMIS GPH score in the Evolocumab group showed a statistically significant difference compared to the statins group. Both groups showed significant differences in pain intensity scores compared to baseline, as chest pain is a typical symptom of acute-phase ACS, and patients experience noticeable pain at baseline. At follow-up, pain scores improved in both groups, with the Evolocumab group showing a statistically significant improvement in pain score percentage compared to the statins group. The study confirms that ACS onset and progression are associated with systemic inflammation20. Some studies have found that a decrease in PCSK9 function is related to a reduction in inflammatory responses21, which may explain the improvement in the GPH and pain scores in the Evolocumab group, potentially linked to a reduction in inflammation. We observed on two patient groups regarding baseline, 12-week, and 48-week changes in hs-CRP levels. The analysis revealed no significant difference in baseline hs-CRP levels between the groups [Evolocumab group: 4.01 (2.35) vs. Statins group: 4.45 (2.88); P = 0.393]. At week 12, patients in the Evolocumab group showed significantly lower hs-CRP levels compared to the statin group [Evolocumab group: 1.59 (4.48) vs. Statins group: 3.94 (4.45); P = 0.048]. By week 48, there was no significant difference in hs-CRP levels between the two groups[Evolocumab group: 1.76 (1.03) vs. Statins group: 1.80 (1.07); P = 0.948]. These changes in hs-CRP were consistent with GPH score and patients’ pain intensity. The study revealed that PCSK9 expression was positively correlated with levels of IL-6, IL-1β, and the LC3B II/I ratio. PCSK9 inhibitors suppress the TLR4/NF-κB pathway, thereby reducing the release of proinflammatory cytokines such as TNF-α and IL-6. Concurrently, they diminish platelet hyperreactivity and lower the risk of thrombotic events via inhibition of the CD36/Nox2-ROS pathway. These mechanisms suggest that PCSK9 inhibitors possess intrinsic anti-inflammatory, and antioxidant properties22. Furthermore, some studie show that PCSK9i have an effective anti-inflammatory effect, particularly at the local level of atherosclerotic plaques23,24.
At 12 weeks, the Evolocumab group also showed a statistically significant difference in the PROMIS GMH score compared to the statins group. Furthermore, the four dimensions of the GMH score in the Evolocumab group continued to improve at both 12 and 48 weeks. Previous studies have shown that high-risk cardiovascular disease patients treated with PCSK9i experience significant improvements in anxiety, depression, and other emotional issues after 1 year of follow-up, which is consistent with the results of this study10. Our results demonstrate that PCSK9 inhibitors facilitate a rapid reduction in LDL-C. Furthermore, they may represent an effective strategy to address non-adherence in high cardiovascular risk patients25. The alleviation of patient anxiety regarding cardiovascular risk, achieved through effective risk reduction, may directly lead to improved GMH scores.
By the 48-week follow-up, the difference in quality of life between the two groups was no longer significant. We propose that this is because patients in both groups eventually achieved a more stable clinical condition, with plaque stabilization and reduced inflammation, leading to a convergence in their overall well-being. Statins may “catch up” in QOL due to cumulative LDL-lowering and plaque stabilization. Additionally, the natural recovery trajectory post-ACS could diminish differences over time.
At 48 weeks, ACS patients who experienced MACE were more likely to have negative emotional problems. However, it must be emphasized that the nature of this association is observational and does not necessarily imply a direct causal relationship. We speculate that MACE, such as myocardial infarction and blood revascularization, are themselves a strong psychological stressor that may directly trigger or exacerbate depressive and anxiety symptoms through physiological and psychological mechanisms (such as post-traumatic stress, future concerns, and physical decline). Equally important is the possibility of reverse causation, in which emotional problems that exist at baseline but are not fully identified may be risk factors for MACE. Previous studies have confirmed that anxiety and depression play a role in the onset and progression of cardiovascular diseases26, and these psychological issues have a negative impact on the overall health of ACS patients. Anxiety and depression are also associated with an increased incidence of MACE27. Moreover, the inflammatory mechanisms involved in emotional disorders and cardiovascular diseases may be linked to lipid metabolism disturbances28. Low levels of HDL-C have also been associated with depression29. Our study demonstrates a significant association between MACE events and emotional disorders. While the causal direction remains unclear and residual confounding factors may exist, these findings underscore the importance of integrating cardiac health and mental health assessments in long-term management of ACS patients. Our results provide critical hypotheses for designing prospective studies to elucidate both the causal relationship and underlying mechanisms.
As a new type of lipid-lowering drug, PCSK9i’s mechanism of action and clinical efficacy have been the focus of clinical research. In recent years, numerous studies have demonstrated the potential of PCSK9 inhibitors to reduce the incidence of cardiovascular events and improve patient outcomes. These trials provided the evidence that, in addition to intensive statin therapy, PCSK9 inhibitors significantly lower the risk of major adverse cardiovascular events (MACE)16,30,31,32.With the progress of diagnosis and treatment technology and the transformation of modern medical model, the quality of life of patients has been paid more and more attention. Emotional distress (depression or anxiety) is a known risk factor for MACE. ESC guidelines recommend routine mental health screening post-ACS. Otherwise Emotional distress may identify patients needing both intensive lipid-lowering and psychological support. Our data suggest also initiating antidepressants/psychotherapy early, as emotional health predicted MACE. We hope that this study can provide a new perspective for the lipid-lowering treatment and the improvement of life quality of cardiovascular patients, and bring more clinical benefits to patients with cardiovascular diseases.
Conclusion
Exploratory analysis suggested that PCSK9 inhibitors can significantly improve the quality of life in ACS patients in the short term, both in GPH and GMH with better outcomes compared to statins, especially in pain perception, mental health, and social activity satisfaction. In the long term, the improvement remains significant. The occurrence of MACE in ACS patients may associate with emotional problems.
Limitations
Although this study provides strong evidence for the improvement in quality of life (quality of life) among ACS patients treated with PCSK9 inhibitors (PCSK9i), several limitations remain. First, the study included 500 ACS patients from multiple hospitals in Tianjin, which may introduce variations in clinical practice and patient populations, thereby limiting the generalizability of the results. Future study should be conducted on a broader patient population to validate the applicability of these findings. Therefore, the generalizability of our findings to other populations with different healthcare systems, cultural backgrounds, and patient expectations should be made with caution. Specifically, factors such as variations in healthcare access, insurance coverage, patient-clinician communication styles, and cultural perceptions of symptoms like ‘pain’ and ‘emotional problems’ could influence PROMIS score responses.
Second, the follow-up period was relatively short (12 and 48 weeks), and a longer follow-up would help further illuminate the long-term effects of PCSK9 inhibitors in ACS patients.
Third, this study did not conduct an in-depth analysis of patients’ emotional problems and thus could not establish a causal relationship between emotional problems and the occurrence of MACE.
While this study focused on quality of life assessment, it did not explore other potential influencing factors in depth, such as the combined use of PCSK9i with other medications, particularly ACEIs and ARBs, to determine whether combination therapy would result in a more significant improvement in quality of life. Additionally, factors such as social support, economic status, patients’ pre-existing conditions, and mental health may all play crucial roles in affecting quality of life in ACS patients.
Notably, the association between MACE and emotional issues may be influenced by residual confounding factors. For instance: Social support: Patients ‘social support levels, marital quality, and family relationships could both influence cardiac event recovery and profoundly affect emotional states, yet these data were not systematically collected. Medication use: While we adjusted for cardiovascular medications, tracking of psychiatric drug usage might be incomplete, as these drugs could concurrently affect both emotional and cardiac endpoints.
The long-term positive impact of PCSK9 inhibitors on quality of life in patients with acute coronary syndrome, as well as the association between MACE and emotional problems, requires confirmation in larger studies with longer follow-up. In particular, further studies should focus on the effects of PCSK9i in managing chronic complications and patients with multiple comorbidities. Additionally, studies should explore how optimizing treatment strategies, including the combination of PCSK9 inhibitors with other medications, can further enhance the overall health and quality of life of ACS patients.
Data availability
The datasets generated and/or analysed during the current study are not publicly available due to patient privacy concerns but are available from the corresponding author on reasonable request.
References
Koskinas, K. C. et al. Evolocumab for early reduction of LDL cholesterol levels in patients with acute coronary syndromes (EVOPACS). J. Am. Coll. Cardiol. Vol. 74, 2452–2462. https://doi.org/10.1016/j.jacc.2019.08.010 (2019).
Damluji, A. A. et al. Management of acute coronary syndrome in the older adult population: A scientific statement from the American heart association. Circulation vol. 147,3 : e32-e62. (2023). https://doi.org/10.1161/CIR.0000000000001112
GBD 2019 Diseases and Injuries Collaborators. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: a systematic analysis for the global burden of disease study 2019. Lancet (London England) Vol. 396 (10258), 1204–1222. https://doi.org/10.1016/S0140-6736(20)30925-9 (2020).
Ganz, F. D. K. et al. Distress among hospitalized patients with acute coronary syndrome. Nurs. Crit. Care Vol. 27 (2), 165–171. https://doi.org/10.1111/nicc.12730 (2022).
Guan, Y. Y. et al. Impact of rumination on severity and persistence of anxiety and depression in cardiac patients. Heart Mind. 5 (1), 9–16. https://doi.org/10.4103/hm.hm_38_20 (2021).
Dekker, R. L. et al. Depressive symptom trajectory predicts 1-year health-related quality of life in patients with heart failure. J. Cardiac Fail. Vol. 17, 755–763. https://doi.org/10.1016/j.cardfail.2011.04.016 (2011).
Visseren, F. L. J. et al. 2021 ESC guidelines on cardiovascular disease prevention in clinical practice. Eur. Heart J. Vol. 42, 3227–3337. https://doi.org/10.1093/eurheartj/ehab484 (2021).
Diaz, R. et al. Intensity of Statin treatment after acute coronary syndrome, residual risk, and its modification by alirocumab: insights from the ODYSSEY OUTCOMES trial. Eur. J. Prev. Cardiol. Vol. 28 (1), 33–43. https://doi.org/10.1177/2047487320941987 (2021).
Yao Yao, Q. et al. Clinical significance of PCSK9 and soluble P-selectin in predicting major adverse cardiovascular events after primary percutaneous coronary intervention in patients with acute coronary syndrome. CVIA 9 (1). https://doi.org/10.15212/CVIA.2023.0087 (2024).
Cesaro, A. et al. Impact of PCSK9 inhibitors on the quality of life of patients at high cardiovascular risk. Eur. J. Prev. Cardiol. Vol. 27 (5), 556–558. https://doi.org/10.1177/2047487319839179 (2020).
Graaf, D. E. et al. Comparison between EQ-5D-5L and PROMIS-10 to evaluate health-related quality of life 3 months after stroke: a cross-sectional multicenter study. Eur. J. Phys. Rehabilitation Med. Vol. 57 (3), 337–346. https://doi.org/10.23736/S1973-9087.21.06335-8 (2021).
Schalet, B. D. et al. Clinical validity of PROMIS depression, anxiety, and anger across diverse clinical samples. J. Clin. Epidemiol. 73, 119–127. https://doi.org/10.1016/j.jclinepi.2015.08.036 (2016).
Schalet, B. D. et al. Validity of PROMIS physical function measured in diverse clinical samples. J. Clin. Epidemiol. 73, 112–118. https://doi.org/10.1016/j.jclinepi.2015.08.039 (2016).
Cella, D. et al. PROMIS fatigue item bank had clinical validity across diverse chronic conditions. J. Clin. Epidemiol. 73, 128–134. https://doi.org/10.1016/j.jclinepi.2015.08.037 (2016).
Gao, J. et al. Nov. Effects of evolocumab added to moderate-intensity statin therapy in Chinese patients with acute coronary syndrome: The EMSIACS Trial Study Protocol. Frontiers in physiology vol. 12 750872. 23 (2021). https://doi.org/10.3389/fphys.2021.750872
Schwartz, G. G. et al. Alirocumab and cardiovascular outcomes after acute coronary syndrome. New. Engl. J. Med. Vol. 379 (22), 2097–2107. https://doi.org/10.1056/NEJMoa1801174 (2018).
Koren, M. J. et al. Long-Term efficacy and safety of evolocumab in patients with hypercholesterolemia. Journal Am. Coll. Cardiology 74,17 (2019): 2132–2146. https://doi.org/10.1016/j.jacc.2019.08.1024
Giugliano, R. P. et al. Cognitive function in a randomized trial of Evolocumab. New. Engl. J. Med. Vol. 377, 633–643. https://doi.org/10.1056/NEJMoa1701131 (2017).
Gargiulo, P. et al. Efficacy, safety, adherence and persistence of PCSK9 inhibitors in clinical practice: A single country, multicenter, observational study (AT-TARGET-IT). Atherosclerosis 366, 32–39. https://doi.org/10.1016/j.atherosclerosis.2023.01.001 (2023).
Ong, S. B. et al. Inflammation following acute myocardial infarction: multiple players, dynamic roles, and novel therapeutic opportunities. Pharmacol. Ther. 186, 73–87. https://doi.org/10.1016/j.pharmthera.2018.01.001 (2018).
Walley, K. R. et al. PCSK9 is a critical regulator of the innate immune response and septic shock outcome. Sci. Translational Med. Vol. 6, 258ra143. https://doi.org/10.1126/scitranslmed.3008782 (2014).
D’Onofrio, N. et al. Jan. SIRT3 mediates the effects of PCSK9 inhibitors on inflammation, autophagy, and oxidative stress in endothelial cells. Theranostics 13,2 531–542. 1 (2023). https://doi.org/10.7150/thno.80289
Giunzioni, I. et al. Local effects of human PCSK9 on the atherosclerotic lesion. J. Pathol. Vol. 238 (1), 52–62. https://doi.org/10.1002/path.4630 (2016).
Liu, A. & Frostegård, J. Apr. PCSK9 plays a novel immunological role in oxidized LDL-induced dendritic cell maturation and activation of T cells from human blood and atherosclerotic plaque. Journal of internal medicine, (2018). https://doi.org/10.1111/joim.12758. 4 doi:10.1111/joim.12758.
Gragnano, F. et al. Adherence to proprotein convertase subtilisin/kexin 9 inhibitors in high cardiovascular risk patients: an Italian single-center experience. J. Cardiovasc. Med. (Hagerstown Md) Vol. 19 (2), 75–77. https://doi.org/10.2459/JCM.0000000000000611 (2018).
Sohier, L., Dallaire-Habel, S. & Turcotte, S. Foldes-busque, guillaume. prevalence of mood and anxiety disorders in canadians with cardiovascular disease: a cross-sectional study. Heart and Mind 8(1) 40–46, (2024). https://doi.org/10.4103/hm.HM-D-23-00060
Meyer, F. A. et al. Positive affect moderates the effect of negative affect on cardiovascular disease-related hospitalizations and all-cause mortality after cardiac rehabilitation. European J. Prev. Cardiol. 22,10 (2015): 1247–1253. https://doi.org/10.1177/2047487314549745
Hamer, M. et al. Psychological distress as a risk factor for cardiovascular events: pathophysiological and behavioral mechanisms. J. Am. Coll. Cardiol. 52. 2156–2162. (2008)https://doi.org/10.1016/j.jacc.2008.08.057
Hummel, J. et al. Serum lipoproteins improve after successful Pharmacologic antidepressant treatment: a randomized open-label prospective trial. J. Clin. Psychiatry Vol. 72, 885–891. https://doi.org/10.4088/JCP.09m05853blu (2011).
Biccirè, F. G. et al. Lesion-Level effects of LDL-C-Lowering therapy in patients with acute myocardial infarction: A post hoc analysis of the PACMAN-AMI trial. JAMA Cardiol. Vol. 9 (12), 1082–1092. https://doi.org/10.1001/jamacardio.2024.3200 (2024).
Sabatine, M. S. et al. Evolocumab and clinical outcomes in patients with cardiovascular disease. New. Engl. J. Med. Vol. 376, 1713–1722. https://doi.org/10.1056/NEJMoa1615664 (2017).
Schwartz, G. G. et al. Mar. Transiently achieved very low LDL-cholesterol levels by statin and alirocumab after acute coronary syndrome are associated with cardiovascular risk reduction: the ODYSSEY OUTCOMES trial. European Heart J. 44,16 1408–1417. 5 (2023). https://doi.org/10.1093/eurheartj/ehad144
Funding
This study was funded by Key Discipline Project of Tianjin Municipal Health Commission (TJWJ2022XK032).
Author information
Authors and Affiliations
Contributions
Anran Jing:Investigation, data collection, formal analysis, visualization, writing original draftJingxian Wang: Formal Analysis, data collection, visualizationMenglong zhang: Data collectionYan Liang: Data collection, resourcesJingyu Liu: Data collection, resourcesNan Zhang: Data collection, resourcesJixiang Wang: Data collection, resourcesXiaowei Li: Data collection, resourcesChangping Li: Conceptualization, formal analysisCui Zhuang: Conceptualization, formal analysisYin Liu: Resources, supervisionJing Gao: Funding acquisition, conceptualization, resources, supervision.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics statement
The study was reviewed and approved by the Institutional Ethics Committee of Tianjin Chest Hospital (IEC No. 2019KY-019-01), and all enrolled patients provided informed consent.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Jing, A., Wang, J., Zhang, M. et al. Effect of PCSK9 inhibitors on the quality of life in patients with acute coronary syndromes — exploratory analysis of the EMSIACS trial. Sci Rep 15, 42493 (2025). https://doi.org/10.1038/s41598-025-26495-y
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-26495-y
