
Abstract
Students with neurodevelopmental disorders (ND) are at risk for academic impairment. However, the pervasive co-occurrence among these conditions has rarely been considered when evaluating this association. This study examined whether intellectual disabilities (ID), communication disorders, autism spectrum disorder (ASD), attention-deficit/hyperactivity disorder (ADHD), specific learning disorder (SLD), and motor disorders were related to academic outcomes. Parents and teachers completed standardized screening instruments for mental health problems and learning difficulties. Children who screened positive were interviewed for diagnostic confirmation according to the Diagnostic and Statistical Manual of Mental Disorders, while students who screened negative served as controls. Academic performance across multiple subjects was obtained from school records. The final sample comprised 9018 participants aged 5–17. Mixed-effects ordinal logistic regression models determined the independent and combined effects of ND on academic performance, adjusting for background and coexisting conditions. When examined separately, each diagnostic category was significantly associated with lower marks in all educational outcomes, even after adjusting for sociodemographic and school-related factors. However, when the influence of neurodevelopmental co-occurrence was controlled for, ID emerged as the strongest predictor of poor academic performance, followed by ADHD, SLD, and communication disorders. ASD and motor disorders were only associated with lower marks in arts and physical education. Furthermore, youth with coexisting conditions were at higher risk for academic impairment across all subjects. These findings highlight the need for early diagnosis and targeted interventions to address the specific educational needs of students with ND. Likewise, co-occurring diagnoses should be actively sought to avoid disadvantaging children with multiple disorders.
Similar content being viewed by others


Introduction
Neurodevelopmental disorders (ND) comprise a group of heterogenous conditions (i.e., intellectual disabilities (ID), communication disorders, autism spectrum disorders (ASD), attention-deficit/hyperactivity disorder (ADHD), specific learning disorder (SLD), and motor disorders) that emerge in childhood and affect typical brain development, producing delays in the expected social, emotional, language, cognitive, and/or motor milestones1. Children with ND experience functional impairments across multiple domains, which interfere with daily life activities and may have long-lasting disabling consequences. Of special relevance is the impact of ND on academic performance since educational attainment is an important determinant of future health and life opportunities2. A nationwide cohort study of over 750,000 Scottish schoolchildren identified that those treated for ADHD had higher rates of unauthorized absence and exclusion, performed worse in examinations, were at greater risk of special educational needs, and left school at an earlier age than their typically developing (TD) peers3. Students with SLD, which are characterized by persistent difficulties in learning academic skills, have also been found to achieve poorer marks, require more educational support, and have lower rates of graduation from high school and college4,5. School performance in children and adolescents with ASD tends to be more heterogeneous. While some high-functioning students perform in the average range on measures of reading and mathematical achievement6,7, others experience greater academic challenges than their TD peers due to disorder-related deficits, such as impaired social communication and interaction, attention problems, and disruptive behaviors8. Similarly, children with developmental coordination disorder (DCD) or Tourette’s syndrome frequently struggle at school9,10. In particular, DCD has a significant negative impact on handwriting performance, spelling, speed, and reading, although preliminary evidence suggests that children with DCD also exhibit learning disabilities that are not primarily motor-based9,11.
Moreover, it is well established that youth with ND are particularly at risk for multiple coexisting conditions12. For instance, those who have ADHD often meet diagnostic criteria for other mental disorders, with co-occurrence rates up to 80%13. Common codiagnosed conditions include ASD, ID, tics, and SLD2,12. Likewise, autistic children have been reported to have a mean of 3.2 coexisting disorders or problems14 and DCD usually co-occurs with other developmental traits, such as hyperactivity, social communication difficulties, and learning disabilities9,15. Lastly, overlapping between different types of SLD (i.e., with impairments in reading, written expression, and mathematics) is also frequent (30–60%)16. At an academic level, coexisting conditions have been associated with poorer educational outcomes, higher rates of grade retention, and other school problems10,17,18, pointing to an additive detrimental effect on academic achievement. Indeed, Larson et al.19 conducted a cross-sectional analysis on a nationally representative sample of 61,779 U.S. children, including 5028 with ADHD, and concluded that functioning declined in a stepwise fashion as the number of concurrent diagnoses increased.
However, there is a scarcity of research reporting academic outcomes for children with coexisting ND, since most studies have examined individual conditions such as ADHD, ASD, ID, or SLD20. In addition, those investigating co-occurring ND have mainly focused on the impact of ADHD with regard to educational attainment, school dropout, or performance on core academic subjects (e.g., reading, mathematics)10,12,18,21,22. Finally, prior investigations have often relied on parent-reported diagnoses or have been drawn from clinical samples, which may not necessarily reflect the heterogeneity in symptom severity or impairment observed within the general population10,13,17.
To address these gaps in the literature, the present study examined the associations between different ND (i.e., ID, communication disorders, ASD, ADHD, SLD, motor disorders) and academic performance across multiple domains (i.e., first language, foreign language, mathematics, physical education (PE), arts) to determine the impact of specific disorder categories and co-occurring conditions on educational outcomes. Specifically, we hypothesized that ID would negatively affect all academic domains. Students with ADHD, SLD and ASD were expected to experience difficulties in first language, foreign language, and mathematics, although we anticipated a more variable academic profile for the latter. Communication disorders would particularly impair language-based subjects, while motor disorders would be associated with lower marks in PE and arts. Last, we hypothesized that the effects of multiple co-occurring ND would be additive, resulting in poorer academic performance as the number of diagnoses increased. Thus, we expand previous research by using data from a large community sample of students aged 5–17 years, who have been accurately assessed according to the Diagnostic and Statistical Manual of Mental Disorders (DSM) criteria.
Methods
Procedure
The study sample was drawn from 77 general education schools in Catalonia, Spain, as part of the INSchool cohort, a larger, ongoing research. Prior to the start of data collection in 2011, the project was approved by the Ethics Committees of Vall d’Hebron University Hospital and Sant Joan de Déu Hospital, which ensured that all methods were performed in accordance with the relevant guidelines and regulations. Informed consent was obtained from all participating families, with additional permission provided by children aged 12 or older. Specifically, the current investigation analyzes data collected cross-sectionally over 11 academic years (i.e., from 2011–2012 to 2022–2023) using a two-step procedure. Figure 1 describes the study design and data collection process.

CONSORT diagram.
Screening assessment
In the first phase of the project (i.e., from September to April), parents of the participating students received a survey regarding sociodemographic data and school-related factors, along with standardized screening instruments to identify emotional or behavioral problems. The main classroom teacher also completed the corresponding teacher-reported version of the screening questionnaires, and provided information on reading and writing difficulties.
Diagnostic assessment
In the second phase (i.e., from January to June), children who screened positive for mental health problems or learning difficulties were interviewed for diagnostic confirmation based on the DSM criteria, after providing informed consent. Interviews were carried out on separate days within the school facilities so all students could complete the clinical assessment. Specifically, participants and their parents met a psychiatrist of the research team, who conducted a clinical interview. Besides, students were granted an additional appointment with an experienced neuropsychologist who evaluated their cognitive abilities, language, and learning academic skills through standardized tests.
Finally, academic performance on multiple domains (i.e., first language, foreign language, mathematics, PE, arts) was obtained from school records at the end of the academic year.
Participants
The final sample included (a) participants who screened negative in the first phase of the project, and (b) those who received a clinical diagnosis of ND. In contrast, students with a positive screening score who did not meet diagnostic criteria for any disorder were excluded from the analyses, as they may have presented with subclinical symptoms or non-specific difficulties. Children with other mental conditions were also excluded unless these co-occurred with a ND in order to reduce heterogeneity and ensure a clean comparison between affected and unaffected participants. Overall, we analyzed data from 9018 primary and secondary school students, aged between 5 and 17 years depending on their grade level at the time of participation and assessment, for whom marks in at least one of the educational outcomes of interest were available.
Measures
Screening assessment
Parents and teachers of the enrolled students completed the respective version of the Achenbach System of Empirically Based Assessment (ASEBA)23 and the Conners’ Rating Scales-Revised (CPRS-R: S/ CTRS-R: S)24. Additionally, teachers reported reading and writing difficulties through the Protocol for Detection and Management of Dyslexia. Teacher’s Version (PRODISCAT)25. Participants were identified as potential cases in accordance with the following criteria: (a) a T score ≥ 70 on any of the syndrome scales from the ASEBA, (b) a T score ≥ 70 on any of the subscales from the CPRS-R: S or CTRS-R: S, (c) five or more high-risk indicators on the PRODISCAT, or (d) a previous diagnosis of ND from a medical professional.
Diagnostic assessment
ND were determined by trained psychiatrists and neuropsychologists using DSM-IV-TR criteria for assessments conducted before 2014 and DSM-5 criteria for those conducted afterwards. Specifically, ID were diagnosed based on both the Wechsler Intelligence Scale for Children26 and a clinical evaluation of adaptive functioning, which included developmental history, parent and teacher interviews. The Clinical Evaluation of Language Fundamentals, Fifth Edition27 was applied to identify communications disorders. The presence of ASD, ADHD and motor disorders was determined using the Kiddie Schedule for Affective Disorders and Schizophrenia Present and Lifetime version28,29, along with information from school reports and direct clinical observations. Finally, SLD were evaluated based on the Battery for the Evaluation of Reading Processes, Revised30, Battery for the Evaluation of Reading Processes in Junior and Senior High-School Students, Revised31, Test for the Analysis of Reading and Writing32, Battery for the Evaluation of Writing Processes33, and NeurekaCALC34. To ensure diagnostic consistency across the study period despite changes between DSM editions, individual disorders were grouped into broader diagnostic categories (i.e., ID, communication disorders, ASD, ADHD, SLD, motor disorders). In particular, the following diagnoses were included in this report: ID, unspecified ID, global developmental delay, language disorder, speech sound disorder, childhood-onset fluency disorder (stuttering), social (pragmatic) communication disorder, ASD, ADHD, unspecified ADHD, other specified ADHD, SLD, unspecified SLD, persistent (chronic) motor or vocal tic disorder, provisional tic disorder, Tourette’s syndrome, unspecified tic disorder, other specified tic disorder, DCD, and stereotypic movement disorder.
Background characteristics
Parents completed a questionnaire on sociodemographic data, including child’s gender, age, and country of birth. The survey also collected information on their marital status, educational level, occupation, and country of birth. Students who were not native Spanish or with at least one parent born abroad were considered of foreign origin. Parents’ education and occupation were weighted to compute the Hollingshead four-factor index35, a measure of socioeconomic status (SES) ranging from 8 to 66, where higher scores reflect higher SES. Finally, parents were asked to indicate whether their child had ever repeated a grade or required some educational support.
Academic performance
Performance on six academic domains (i.e., Catalan, Spanish, English as foreign language, mathematics, PE, arts) was obtained from school records at the end of the academic year and marks were converted into a 4-point scale from D to A (D = unsatisfactory achievement, fail, 0–4.9; C = satisfactory achievement, pass, average, 5–6.9; B = good achievement, above average, 7–8.9; and A = excellent achievement, 9–10). Given the high correlation between Catalan and Spanish marks (r = .77, p < .001), we calculated the academic performance on first language as the mean of the two scores.
Statistical analyses
All analyses were performed with SPSS 29.0 (IBM Inc., Arkmonk, NY). In order to investigate the independent associations between ND and academic achievement, three mixed-effects ordinal logistic regression models were estimated for each educational outcome, with D as the highest category. In particular, we accounted for the clustering of academic marks by including school as a random effect and modeling a two-level structure with students (level 1) nested within schools (level 2). We first examined each ND (yes, no), gender (boy, girl), age (continuous variable), SES (continuous variable), ethnicity (native, foreign origin), parental divorce/separation (yes, no), educational support (yes, no), and grade retention (yes, no) individually (model 0; crude analyses). In a second set of models, each diagnostic category was adjusted for sociodemographic factors and school-related variables (model 1). Last, we considered all neurodevelopmental conditions, along with background characteristics, in the final models (model 2) to control for co-occurring disorders, which resulted in sample sizes ranging from 6590 to 7664. Additional analyses were conducted to evaluate the effects of multiple co-occurring conditions on academic performance, considering the number of ND an individual had. To control for multiple testing, a false discovery rate (FDR) threshold of 5% was applied separately within each model, based on the number of predictors included (i.e., 13 comparisons per educational outcome in the fully adjusted models).
Missing data
There were little missing values across the academic outcomes of testing (< 0.3%), except for arts (14.6%) and PE (3.88%), where missingness resulted from school-level reporting differences rather than participant non-response. With regard to background characteristics, the amount of missing data was greatest for ethnicity (9.58%), followed by grade retention (8.65%), educational support (8.55%), and parental divorce/separation (8.32%). In contrast, full data were available for gender, age, and SES. To examine the missing data mechanism, we conducted multiple analyses (i.e., Little’s MCAR test, logistic regressions on missingness indicators) and confirmed that missingness was related to observed covariates included in the model (Table S1), supporting the plausibility of a covariate-dependent missingness structure. Although full information maximum likelihood (FIML) is theoretically appropriate under this assumption, missing data were handled using case-wise deletion due to the technical limitations reported in the literature when applying FIML to complex models involving hierarchical data, ordinal outcomes with sparse categories, and large sample sizes36,37,38. Likewise, multiple imputation was not applied as most missingness occurred in binary control variables, for which reliable imputation is challenging without strong auxiliary predictors. Children with missing data had a higher prevalence of ID than the complete sample (1.65% vs. 0.47%, p = .001), and achieved a greater proportion of Ds on first language (4.49% vs. 2.28%, p = .001), foreign language (6.62% vs. 4.94, p = .037), and mathematics (8.75% vs. 5.89%, p = .001). Significant differences were also found on age (incomplete: 10.4 years, complete: 9.43 years, p < .001) and SES (incomplete: 42.1, complete = 43.8, p < .001).
Results
Sample characteristics
The sample comprised 9018 students, with a mean age of 9.48 years (SD = 2.84; range = 5–17 years). ND were present in 2707 (30%) subjects, while the remaining 6311, who screened negative in the first phase of the study, served as the control group. The most frequent conditions included SLD (n = 1525, 16.9%) and ADHD (n = 1523, 16.9%). Communication disorders were found in 269 (2.98%) students, 140 (1.55%) met criteria for ASD, 80 (0.88%) had motor disorders, and 47 (0.52%) met criteria for ID. Overall, 1522 (16.9%) participants had only one ND, 774 (8.58%) had two, 334 (3.70%) had three, and 77 (0.85%) met criteria for at least four co-occurring conditions. Compared to controls, children with ND were more likely to be male (64.2% vs. 49.2%, p < .001), older (9.75 vs. 9.37 years, p < .001), from lower SES (39.1 vs. 45.7, p < .001), and of foreign origin (28.9% vs. 16.4%, p < .001). Additionally, the percentage of participants reporting parental divorce/separation, educational support, or grade retention was higher among those who received a clinical diagnosis (p < .001). In terms of academic performance, students with ND achieved mostly a mark of C or D on all educational outcomes, while TD children had a greater proportion of As and Bs (p < .001). Table 1 shows the sociodemographic characteristics, school-related variables, and academic performance of the study sample.
Associations with academic performance
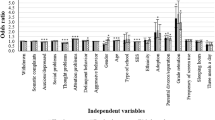
Tables 2, 3, 4 and 5 show the associations between ND and academic performance, estimated in a series of ordinal logistic regression models with school as a random effect. The unadjusted models revealed that all diagnostic categories were significantly associated with lower marks in first language, foreign language, mathematics, arts, and PE (Tables 2, 3, 4 and 5, model 0). Specifically, the strongest association was observed for ID, with odds ratios (OR) ranging from 6.91 to 14.0, partly because of the small number of participants with such disorders. Repeater students, children of foreign origin, with divorced/separated parents or who required educational support were also at risk for underperformance, while those from higher SES were found to receive better marks in all academic subjects (Tables 2, 3, 4 and 5, model 0). Gender was related to first language, foreign language, mathematics and arts, where boys performed worse than girls (Tables 2, 3 and 4, model 0). Likewise, age was associated with negative educational outcomes on language subjects and mathematics (Tables 2 and 3, model 0). Older students, in contrast, were less likely to achieve lower marks in PE (Table 5, model 0).
The effects of ND on academic performance remained even after adjustment for sociodemographic and school-related variables (Tables 2, 3, 4 and 5, model 1). However, when we additionally included all the diagnostic categories in the models to account for coexisting conditions, the associations of ASD and motor disorders with academic impairment declined to a nonsignificant level, except for arts (Table 4, model 2) and PE (Table 5, model 2). In contrast, ID were still the strongest predictor of poor performance (ORs 4.11–11.9; Tables 2, 3, 4 and 5, model 2). Similarly, children with ADHD or SLD were more likely to have lower marks than their peers in all academic domains (ADHD: ORs 2.67–4.65; SLD: ORs 1.86–5.97), although the largest group differences were found in language subjects and mathematics (Tables 2, 3, 4 and 5, model 2). Last, the relationship between communication disorders and poor educational functioning attenuated after controlling for multiple co-occurring conditions, but remained significant across the outcomes examined (Tables 2, 3, 4 and 5, model 2). Background characteristics also predicted academic achievement in the fully adjusted models (Tables 2, 3, 4 and 5, model 2). Nevertheless, once sociodemographic factors, school-related variables, and co-occurring ND were controlled for, girls attained lower marks in mathematics (OR = 1.23, 95% CI = 1.12–1.34) and gender became significant for PE, where boys performed better (OR = 0.78, 95% CI = 0.70–0.86). The effect of ethnicity declined and was no longer related to marks in foreign language and arts (Tables 2 and 4, model 2).
Sensitivity analysis examining Catalan and Spanish separately showed largely consistent results, confirming that the associations with first language were robust. Specifically, ID, ADHD, SLD, and communication disorders predicted poor academic performance on both subjects, while ASD remained significantly associated with lower marks in Spanish (Table S2).
Finally, additional analyses were conducted to examine whether a higher number of co-occurring ND was related to worse academic achievement, when adjusted for background characteristics. Each additional diagnostic category increased the likelihood of obtaining lower marks in language subjects (first language: OR = 3.07, 95% CI = 2.87–3.29, p < .001; foreign language: OR = 2.61, 95% CI = 2.45–2.78, p < .001), mathematics (OR = 2.39, 95% CI = 2.25–2.54, p < .001), arts (OR = 1.93, 95% CI = 1.81–2.06, p < .001), and PE (OR = 1.70, 95% CI = 1.60–1.81, p < .001).
Discussion
The current research examined the associations between specific ND – including ID, communication disorders, ASD, ADHD, SLD, and motor disorders – and academic performance across multiple dimensions in 9018 Spanish students, when controlling for coexisting conditions and background characteristics.
When examined separately, each diagnostic category was significantly associated with lower marks in all educational outcomes. Likewise, previous studies have consistently demonstrated that students with ADHD, ID or SLD are at higher risk for academic impairment than TD children, although the pervasive co-occurrence among ND has rarely been considered in the evaluation of this relationship3,4,5. Indeed, when we included all neurodevelopmental conditions in the models, a more restricted pattern emerged, with ID being the strongest predictor of low educational outcomes. This broad impact is unsurprising and reflects the pervasive nature of ID, which are characterized by deficits in cognitive and adaptive functioning across conceptual, social, and practical domains1. These impairments – including poor attention, working memory, information processing, and reasoning – hinder the acquisition of oral and written language skills39,40. Students with ID also show delayed mathematical development due to difficulties with basic numerical skills, planning, problem-solving, and abstract thinking41,42. Last, these deficits may affect creativity, coordination, and fine motor skills required to engage effectively in arts and PE40,43.
As hypothesized, ADHD was one of the strongest drivers behind poor academic performance in first language, foreign language, and mathematics. Indeed, a large body of literature demonstrates that youth with ADHD face significant academic challenges, even after accounting for other neurodevelopmental conditions2,4,12,13,17,21,22. These students often struggle with holding attention, following instructions, planning, and completing schoolwork44. Additionally, those with the hyperactive/impulsive presentation exhibit excessive motor activity and difficulties in staying still44. Thus, it is unsurprising that they experience problems in an academic environment, which may lead to lower levels of achievement. Unexpectedly, however, our results revealed lower marks in less academically-oriented activities such as arts and PE. In this regard, there is evidence that people with ADHD report enhanced creativity in public or mechanical abilities, but not in other artistic tasks45. Additionally, ADHD children may present motor control deficits, such as poor manual dexterity and lower performance in fundamental skills44.
Likewise, the current investigation confirmed that SLD increase the risk of poor educational outcomes in core subjects by impeding or slowing the acquisition of reading, writing, and arithmetic skills4,5,21,46. Students with SLD also struggle in several cognitive and meta-cognitive tasks, including monitoring and regulating their own performance5. In addition, we found independent, negative associations between SLD and marks in arts and PE, which was somewhat unexpected. Nevertheless, these children exhibit postural, fine and gross motor impairments, even after controlling or excluding for concurrent ADHD or DCD47, that frequently remain unrecognized in the school and sports systems. These findings highlight the need for early and continued assessments, along with adapted physical activities to optimize the motor development of children with SLD, especially given the risk of motor decline from their sedentary lifestyle behaviors47.
Another surprising finding was that participants who met criteria for communication disorders achieved lower marks than their peers across all academic domains, although differences between groups were larger in language-dependent subjects, as anticipated. In the same way, a recent systematic review demonstrated that students with developmental language disorder are at greater risk of academic failure, particularly in literacy achievement given the theoretical links between language ability and reading48. Nevertheless, they may also struggle with mathematics as many aspects are linguistic activities49. In this regard, Aguilar-Mediavilla et al.50 showed that Spanish-Catalan students with developmental language disorder had more frequent grade retention and lower marks than their peers in all academic subjects (i.e., Catalan, Spanish, English, arts), except for mathematics and PE. By contrast, larger studies reported lower scores on mathematics and there is strong evidence supporting the association of speech and language disorders with motor problems, such as slower eye-hand coordination, reduced manual dexterity, and impaired balance51,52. Thus, our results highlight the importance of integrating motor skill training into educational interventions for students with communication disorders as they may also experience significant challenges in academic subjects with lower language dependence.
Movement abnormalities often occur in ASD as well, particularly in tasks involving locomotion skills, balance and coordination53,54. Therefore, the association between ASD and poor academic performance on PE is not surprising and echoes a recent meta-analysis, which showed that children with ASD have physical activity levels that are 8–12% lower than their peers during PE and school breaks55. Students with ASD may also struggle with PE due to social and communication deficits, and the considerable stimuli existing in the gymnasium, which can trigger frustration or disruptive behaviors56. In addition, poor fine motor skills and manual dexterity, especially when manipulating writing utensils57, might explain the increased risk for underperformance in arts. Conversely, the relationship between ASD and academic impairment in language subjects and mathematics declined after controlling for other neurodevelopmental conditions. Consistent with the disorder’s heterogeneity, the literature shows a wide variability in academic performance, which presumably arises from differences in intellectual and linguistic abilities, inattention, and working memory6,58. For instance, high-functioning students with ASD have been found to perform in the average range in reading and mathematics6,7. Additional diagnoses, such as ID, communication disorders, ADHD or SLD, may also contribute to the varied academic profile of autistic children6,57, although most studies do not report the presence of coexisting disorders. Thus, further research is needed to disentangle whether the academic difficulties associated with ASD are intrinsic to the disorder or due to other co-occurring conditions.
Similarly, when we included all the diagnostic categories in the models, motor disorders were only related to educational outcomes on arts and PE. This aligns with a previous investigation reporting the follow-up of children with delayed motor development, which found a lower performance in all school subjects (i.e., Finish, first foreign language, mathematics, PE, music, drawing) compared to the control group. However, differences in language and mathematics disappeared after controlling for IQ59. More recently, Harrowell et al.15 revealed that the impact of DCD on educational achievement was attenuated when the effects of co-occurring difficulties in reading, social communication, and hyperactivity/inattention were adjusted for, suggesting that other developmental conditions may account for the underperformance in academic subjects where adequate movement competence is less crucial. By contrast, subjects that have a substantial movement component, such arts and PE, may be directly impaired due to disorder-related deficits in both gross and fine motor skills60. For instance, children with DCD are less coordinated in terms of manual dexterity and face significant difficulties in writing, drawing, or using scissors60. Besides, they have trouble throwing, catching, or kicking a ball, which hinders participation in physical activities and further impacts performance60,61.
The observation that meeting criteria for multiple ND increased the odds of lower marks across all educational outcomes is an important contribution to the literature since previous studies have mainly focused on single conditions. However, those investigating the impact of ADHD in combination with ASD or SLD have reported similar results12,18,21,22.
Finally, our results corroborate the presence of a stable female advantage in school marks, especially for language subjects62. The increased risk for academic underperformance with age echoes findings from a large longitudinal study63 and may reflect the more challenging academic environment during adolescence, characterized by multiple teachers, changes in curriculum content, and different instructional and assessment methods. This association could also suggest a ‘growing into deficit’ effect, where children with ND experience a progressive decline in educational functioning as academic and cognitive demands increase, although this interpretation remains speculative given the cross-sectional nature of our study.
The main strengths of the current research include the large size and age range of the sample, and the comprehensive clinical assessment performed, although implementing such procedures in typical school settings may be difficult due to resources and personnel constraints. Moreover, we used official academic records across multiple domains and limited shared method variance by using different informants for diagnoses and academic achievement. Last, we adjusted our analyses for multiple background characteristics, co-occurring ND, and the nested structure of data within schools.
Nevertheless, alternative explanations for the observed relationships cannot be excluded since variables such as children’s intelligence quotient, executive functioning, treatment status or other coexisting psychiatric disorders were not considered. Students who screened negative did not undergo the diagnostic assessment and false negative might have occurred. However, only 0.88% of them had ever repeated a grade and 5.19% required educational support. These figures contrast with those in the positive screening group (7.43% and 21.7%, respectively), suggesting that the presence of undetected ND was likely to be low. Missing data were handled using case-wise deletion due to the methodological challenges reported in previous studies when applying FIML or multiple imputation to complex models involving ordinal outcomes, clustered data structures, binary indicators with missing values, and large sample sizes36,37,38. Therefore, it is unknown to what extent the loss of participants might have impacted the findings, but associations might have been attenuated, as children with missing data were older, from lower SES, had higher rates of ID, and achieved poorer marks in most educational outcomes than the complete sample. Moreover, although we could not compare individuals who refused to participate in the screening phase with those included in the final sample, we found that students in secondary education and those attending private schools were over-represented among non-participants. Finally, the cross-sectional design of the study prevents from drawing conclusions on causality. Caution is also warranted when interpreting the generalizability of prevalence rates since the study was not intended as an epidemiological investigation. Our primary objective was to examine the association between ND and academic performance in a large school-based sample. Thus, children with other psychiatric conditions were excluded unless these co-occurred with a ND, which may have resulted in an overrepresentation of ND diagnoses. In addition, data collection spanned the transition period from DSM-IV to DSM-5. This diagnostic shift could have influenced both prevalence and co-occurrence estimates. In particular, the broader age-of-onset criterion and the inclusion of all DSM-5 diagnostic categories (i.e., combined, predominantly inattentive, predominantly hyperactive-impulsive, other specified, and unspecified ADHD) may explain the relatively high ADHD rate. Besides, the school-based nature of our sample and the comprehensive clinical assessment performed likely facilitated the identification of less severe cases that might not have been referred for evaluation in clinical settings. Conversely, the lower prevalence of ID and ASD may reflect both the stricter DSM-5 diagnostic criteria and the characteristics of the sample. The DSM-5 places greater emphasis on adaptive functioning for the diagnosis of ID, potentially excluding children with low IQ who function adequately in daily life, and identifies fewer cases of ASD, particularly among those with milder or atypical presentations64. Furthermore, the DSM-IV did not allow the co-occurrence of ASD and ADHD, which may have led to underidentification in earlier assessments. Finally, as the sample was drawn from general education classrooms, children with more severe forms of ID or ASD – who are often placed in specialized educational settings or integrated support units within schools – were likely underrepresented. This is consistent with prior research showing that students with more profound neurodevelopmental impairments are less frequently captured in population-based studies65.
Overall, the present investigation demonstrates that ID, ADHD, SLD, and communication disorders have a strong negative influence on students’ academic performance regardless of other co-occurring conditions and background characteristics, while ASD and motor disorders are only associated with lower marks in arts and PE. Furthermore, youth with multiple ND are at higher risk of academic impairment in all educational outcomes. These findings, however, should be interpreted within the broader context of the educational system, where teachers often lack training and support to effectively address the diverse needs of students with ND. Traditional instructional and assessment methods may not align with the learning profiles of these children, and evidence-based practices are not consistently implemented in classrooms, which may further exacerbate their academic challenges. Therefore, our results underscore not only the need for early diagnosis, but the importance of developing school-based frameworks that promote inclusive pedagogical strategies, coordinated collaboration among educators, specialists, and families, and targeted academic supports to create more equitable learning environments. Indeed, evidence suggests that students with mild ID attending regular classrooms may experience greater academic progress than children in special schools66,67. Similarly, adapted teaching methods have been applied in various subjects, resulting in improved skills40. Moreover, co-occurring diagnoses should be actively sought as focusing solely on a primary condition may result in diagnostic overshadowing. This unrecognition of additional ND may delay tailored interventions for specific learning, attentional or motor difficulties, potentially exacerbating academic underperformance and widening achievements gaps over time. Further prospective studies with a broader selection of covariates (e.g., intelligence, executive functioning, treatment status) are needed to provide a more secure basis for inference and identify the combinations of disorders with the strongest impact on educational outcomes. In addition, future research should explore potential moderators of academic impairment and examine whether similar associations could be identified using screening tools specifically designed to detect potential ND, as has previously been demonstrated with other widely used standardized questionnaires such as the Child Behavior Checklist68.
Data availability
The datasets generated and/or analyzed during the current study are available from the corresponding author on reasonable request.
References
American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders 5th edn (American Psychiatric Publishing Association, 2013).
Trane, F. E. & Willcutt, E. G. Attention-deficit/hyperactivity disorder and academic functioning: reading, writing, and math abilities in a community sample of youth with and without ADHD. Res. Child. Adolesc. Psychopathol. 51, 583–596 (2023).
Fleming, M. et al. Educational and health outcomes of children treated for attention-deficit/hyperactivity disorder. JAMA Pediatr. 171, e170691 (2017).
Español-Martín, G. et al. The impact of attention-deficit/hyperactivity disorder and specific learning disorders on academic performance in Spanish children from a low-middle- and a high-income population. Front. Psychiatry. 14, 1136994 (2023).
Holopainen, L. & Hakkarainen, A. Longitudinal effects of reading and/or mathematical difficulties: the role of special education in graduation from upper secondary education. J. Learn. Disabil. 52, 456–467 (2019).
Tonizzi, I. & Usai, M. C. Math abilities in autism spectrum disorder: a meta-analysis. Res. Dev. Disabil. 139, 104559 (2023).
Troyb, E. et al. Academic abilities in children and adolescents with a history of autism spectrum disorders who achieved optimal outcomes. Autism 18, 233–243 (2014).
Milgramm, A., Christodulu, K. V. & Rinaldi, M. L. Brief report: predictors of teacher-rated academic competence in a clinic sample of children with and without autism spectrum disorder. J. Autism Dev. Disord. 51, 2132–2138 (2021).
Dionne, E., Bolduc, M. È., Majnemer, A., Beauchamp, M. H. & Brossard-Racine, M. Academic challenges in developmental coordination disorder: a systematic review and meta-analysis. Phys. Occup. Ther. Pediatr. 43, 34–57 (2023).
Ricketts, E. J. et al. Academic, interpersonal, recreational, and family impairment in children with Tourette syndrome and attention-deficit/hyperactivity disorder. Child. Psychiatry Hum. Dev. 53, 3–15 (2022).
Gomez, A., Piazza, M., Jobert, A., Dehaene-Lambertz, G. & Huron, C. Numerical abilities of school-age children with developmental coordination disorder (DCD): a behavioral and eye-tracking study. Hum. Mov. Sci. 55, 315–326 (2017).
Fleming, M. et al. Neurodevelopmental multimorbidity and educational outcomes of Scottish schoolchildren: a population-based record linkage cohort study. PLoS Med. 17, e1003290 (2020).
Lawrence, D., Houghton, S., Dawson, V., Sawyer, M. & Carroll, A. Trajectories of academic achievement for students with attention-deficit/hyperactivity disorder. Br. J. Educ. Psychol. 91, 755–774 (2021).
Carlsson, L. H. et al. Coexisting disorders and problems in preschool children with autism spectrum disorders. Sci. World J. 2013, 213979 (2013).
Harrowell, I., Hollén, L., Lingam, R. & Emond, A. The impact of developmental coordination disorder on educational achievement in secondary school. Res. Dev. Disabil. 72, 13–22 (2018).
Willcutt, E. G. et al. Understanding comorbidity between specific learning disabilities. New Dir. Child Adolesc. Dev. 2019, 91–109 (2019).
Cuffe, S. P. et al. ADHD and psychiatric comorbidity: functional outcomes in a school-based sample of children. J. Atten. Disord. 24, 1345–1354 (2020).
Smith, T. J. & Adams, G. The effect of comorbid AD/HD and learning disabilities on parent-reported behavioral and academic outcomes of children. Learn. Disabil. Q. 29, 101–112 (2006).
Larson, K., Russ, S. A., Kahn, R. S. & Halfon, N. Patterns of comorbidity, functioning, and service use for US children with ADHD, Pediatrics. 127, 462–470 (2011).
Yoro, A. J., Fourie, J. V. & van der Merwe, M. Learning support strategies for learners with neurodevelopmental disorders: perspectives of recently qualified teachers. Afr. J. Disabil. 9, 561 (2020).
Beckman, L., Janson, S. & von Kobyletzki, L. Associations between neurodevelopmental disorders and factors related to school, health, and social interaction in schoolchildren: results from a Swedish population-based survey. Disabil. Health J. 9, 663–672 (2016).
Taanila, A. et al. Association between childhood specific learning difficulties and school performance in adolescents with and without ADHD symptoms: a 16-year follow-up. J. Atten. Disord. 18, 61–72 (2014).
Achenbach, T. M. & Rescorla, L. A. Manual for the ASEBA school-age forms and profiles. In University of Vermont Research Center for Children, Youth, & Families (2001).
Conners, C. K. The Conners’ Rating scales-revised: Technical Manual (Multi-Health Systems, 1997).
Col·legi de Logopedes de Catalunya. PRODISCAT. Protocol de detecció i actuació en la dislèxia. Àmbit educatiu (Departament d’Ensenyament de la Generalitat de Catalunya, 2011).
Wechsler, D. Wechsler Intelligence Scale for children–fifth Edition (WISC-V) (NCS Pearson, 2014).
Wiig, E., Semel, E. & Secord, W. Evaluación Clínica De Los Fundamentos Del Lenguaje, Quinta Edición (CELF-5) (Pearson Clinical & Talent Assessment, 2018).
de la Peña, F. R. et al. Validity and reliability of the kiddie schedule for affective disorders and schizophrenia present and lifetime version DSM-5 (K-SADS-PL-5) Spanish version. BMC Psychiatry. 18, 193 (2018).
Kaufman, J. et al. Schedule for affective disorders and schizophrenia for school-age children-present and lifetime version (K-SADS-PL): initial reliability and validity data. J. Am. Acad. Child. Adolesc. Psychiatry. 36, 980–988 (1997).
Cuetos, F., Rodríguez, B., Ruano, E. & Arribas, D. PROLEC-R: Batería de evaluación de los procesos lectores. Revisada (TEA Ediciones, 2007).
Cuetos, F., Arribas, D. & Ramos, J. L. PROLEC-SE-R. Batería de evaluación de los procesos lectores en secundaria y bachillerato – revisada (TEA Ediciones, 2016).
Toro, J. & Cervera, M. Test de análisis de la lecto-escritura (Aprendizaje-Visor, 1991).
Cuetos, F., Ramos, J. L. & Ruano, E. PROESC. Evaluación de los procesos de escritura (TEA Ediciones, 2002).
Serra-Grabulosa, J. M. Herramientas digitales de evaluación neuropsicológica del procesamiento numérico y el cálculo, la atención sostenida, la memoria de trabajo y la lectura [Conference session]. 66a Jornada de Primavera de la Societat Catalana de Neuropsicologia (SCNPS) (2015).
Hollingshead, A. B. Four factor index of social status. YJS 8, 21–52 (2011).
Grund, S., Lüdtke, O. & Robitzsch, A. Multiple imputation of missing data for multilevel models: simulations and recommendations. Organ. Res. Methods. 21, 111–149 (2018).
Jia, F. & Wu, W. Evaluating methods for handling missing ordinal data in structural equation modeling. Behav. Res. Methods. 51, 2337–2355 (2019).
Lim, A. J. M. & Cheung, M. W. L. Evaluating FIML and multiple imputation in joint ordinal-continuous measurements models with missing data. Behav. Res. Methods. 54, 1063–1077 (2022).
Karvonen, M., Clark, A., Carlson, C., Wells, S. & Burnes, J. Approaches to identification and instruction for students with significant cognitive disabilities who are English learners. Res. Pract. Pers. Sev Disabil. 46, 223–239 (2021).
Villamil Matallana, J. F. & Paredes-Velasco, M. Teaching methodology for people with intellectual disabilities: a case study in learning ballet with mobile devices. Univers Access. Inf. Soc 1–15 (2023).
Garrels, V. & Palmer, S. B. Student-directed learning: a catalyst for academic achievement and self-determination for students with intellectual disability. J. Intellect. Disabil. 24, 459–473 (2020).
Schnepel, S., Krähenmann, H., Dessemontet, S., Moser Opitz, E. & R. & The mathematical progress of students with an intellectual disability in inclusive classrooms: results of a longitudinal study. Math. Educ. Res. J. 32, 103–119 (2020).
Koutsobina, V., Zakapoulou, V., Tziaka, E. & Koutras, V. Evaluating fine perceptual-motor skills in children with mild intellectual disability. ADEP 3, 97–108 (2021).
Bicalho, L. E. et al. Knowledge of physical education professionals and students about ADHD and its motor impairments. Braz J. Mot Behav. 17, 16–24 (2023).
Boot, N., Nevicka, B. & Baas, M. Creativity in ADHD: goal-directed motivation and domain specificity. J. Atten. Disord. 24, 1857–1866 (2020).
Standford, E. & Delage, H. Complex syntax and working memory in children with specific learning difficulties. First Lang. 40, 411–436 (2020).
Blanchet, M. & Assaiante, C. Specific learning disorder in children and adolescents, a scoping review on motor impairments and their potential impacts. Child. (Basel). 9, 892 (2022).
Ziegenfusz, S., Paynter, J., Flückiger, B. & Westerveld, M. F. A systematic review of the academic achievement of primary and secondary school-aged students with developmental language disorder. Autism Dev. Lang. Impair. 7, 23969415221099397 (2022).
Young, A. R. et al. Young adult academic outcomes in a longitudinal sample of early identified language impaired and control children. J. Child. Psychol. Psychiatry. 43, 635–645 (2002).
Aguilar-Mediavilla, E., Buil-Legaz, L., López-Penadés, R., Sanchez-Azanza, V. A. & Adrover-Roig, D. Academic outcomes in bilingual children with developmental language disorder: a longitudinal study. Front. Psychol. 10, 531 (2019).
Conti-Ramsden, G., Durkin, K., Simkin, Z. & Knox, E. Specific language impairment and school outcomes. I: identifying and explaining variability at the end of compulsory education. Int. J. Lang. Commun. Disord. 44, 15–35 (2009).
Visscher, C., Houwen, S., Scherder, E. J., Moolenaar, B. & Hartman, E. Motor profile of children with developmental speech and language disorders. Pediatrics 120, e158–163 (2007).
Kaplánová, A., Šišková, N., Grznárová, T. & Vanderka, M. Physical education and development of locomotion and gross motor skills of children with autism spectrum disorder. Sustainability 15, 28 (2022).
Sortwell, A. Planning and pedagogical considerations for teaching children with autism spectrum disorder in physical education. Kinesiol. Rev. 13, 302–312 (2024).
Rostami, H. et al. Children with autism spectrum disorder spent 30 minutes less daily time in moderate-to-vigorous physical activity than typically developing peers: a meta-analysis of cross-sectional data. Rev. J. Autism Dev. Disord. 10, 144–157 (2021).
Lee, J. & Haegele, J. A. Understanding challenging behaviors of students with autism spectrum disorder in physical education. J. Phys. Educ. Recreat Dance. 87, 27–30 (2016).
Fleury, V. P. et al. Addressing the academic needs of adolescents with autism spectrum disorder in secondary education. Remedial Spec. Educ. 35, 68–79 (2014).
Estes, A., Rivera, V., Bryan, M., Cali, P. & Dawson, G. Discrepancies between academic achievement and intellectual ability in higher functioning school-aged children with autism spectrum disorder. J. Autism Dev. Disord. 41, 1044–1052 (2011).
Cantell, M. C., Smyth, M. M. & Ahonen, T. P. Clumsiness in adolescence: educational, motor, and social outcomes of motor delay detected at 5 years. Adapt. Phys. Act. Q. 11, 115–129 (1994).
Zwicker, J. G., Missiuna, C., Harris, S. R. & Boyd, L. A. Developmental coordination disorder: a review and update. Eur. J. Paediatr. Neurol. 16, 573–581 (2012).
Van der Linde, B. W. et al. Activities of daily living in children with developmental coordination disorder: performance, learning, and participation. Phys. Ther. 95, 1496–1506 (2015).
Voyer, D. & Voyer, S. D. Gender differences in scholastic achievement: a meta-analysis. Psychol. Bull. 140, 1174–1204 (2014).
Sijtsema, J. J., Verboom, C. E., Penninx, B. W., Verhulst, F. C. & Ormel, J. Psychopathology and academic performance, social well-being, and social preference at school: the TRAILS study. Child. Psychiatry Hum. Dev. 45, 273–284 (2014).
Kulage, K. M., Smaldone, A. M. & Cohn, E. G. How will DSM-5 affect autism diagnosis? A systematic literature review and meta-analysis. J. Autism Dev. Disord. 44, 1918–1932 (2014).
Brock, M. E. Trends in the educational placement of students with intellectual disability in the united States over the past 40 years. Am. J. Intellect. Dev. Disabil. 123, 305–314 (2018).
Peetsma, T., Vergeer, M., Roeleveld, J. & Karsten, S. Inclusion in education: comparing pupils’ developmental in special and regular education. Educ. Rev. 53, 125–135 (2001).
Sernier Dessemontet, R., Bless, G. & Morin, D. Effects of inclusion on the academic achievement and adaptive behaviour of children with intellectual disabilities. J. Intell. Disabil. Res. 56, 579–587 (2012).
Pagerols, M. et al. The impact of psychopathology on academic performance in school-age children and adolescents. Sci. Rep. 12, 4291 (2022).
Acknowledgements
We are grateful to the students, families, and staff of the public primary schools (i.e., Ciutat d’Alba, IE Catalunya, Jaume Ferran i Clua, Joan Maragall, La Floresta, La Mirada, L’Olivera, Maria Borés, Marquès de la Pobla, Martinet, Pi d’en Xandri, Pins del Vallès, Puiggraciós, Ramon Llull, Rivo Rubeo, Sant Jordi, Tagamanent, Teresa Bergadà, Turó de Can Mates, Víctor Català), public secondary schools (i.e., Angeleta Ferrer i Sensat, Antoni Pous i Argila, Cal Gravat, Duc de Montblanc, Flos i Calcat, Guillem Catà, Institut de Vic, Institut del Ter, Jaume Callís, Lacetània, La Plana, Lluís de Peguera, Manuel de Montsuar, Molí de la Vila, Pius Font i Quer, Vallbona d’Anoia, Vil·la Romana) and private schools (i.e., Airina, Ave Maria, Bon Pastor, Casals-Gràcia, Episcopal de Lleida, Escolàpies Llúria, Escolàpies Sant Martí, Escorial Vic, FEDAC Manresa, FEDAC Vic, Garbí Pere Vergés Esplugues, Institució Igualada, Institució Tarragona, Joviat, La Farga, La Salle Manlleu, La Salle Manresa, La Salle Sant Celoni, L’Esperança, Oms i de Prat, Padre Damián Sagrados Corazones, Pia Santa Anna – Mataró, Pia Sarrià-Calassanç, Pureza de María Sant Cugat, Regina Carmeli – Rubí, Sagrat Cor Vic, Sagrats Cors Centelles, Sant Josep Oriol, Sant Miquel dels Sants, Santa Teresa de Lisieux, Santíssima Trinitat, Thau Barcelona, Viaró), who kindly participated in this study, as well as to the Department of Education of Generalitat de Catalunya.
Funding
This work was funded by Fundació “la Caixa” (LCR/PR/PR20/51150021), Diputació de Barcelona (PR(AG)72-2012 (2016/011627)), Pla Estratègic de Recerca i Innovació en Salut (SLT006/17/00285), Fundació La Marató de TV3 (202228-30-31), Fondo de Investigaciones Sanitarias (PI23/00026, PI23/00040), Agència de Gestió d’Ajuts Universitaris i de Recerca (DI-2024-00034), Fundació d’Investigació Salut i Progrés (FISP), and the Department of Health (Generalitat de Catalunya).
Author information
Authors and Affiliations
Contributions
M.P. conceived the study, performed the data curation and statistical analysis, interpreted the results, and drafted the manuscript; A.A., R.P., E.P., M.A., G.E.M., L.M., J.P. and G.P. participated in the data collection; M.C. conceived and supervised the study, participated in the funding acquisition, and review the manuscript; R.B. conceived the study, participated in its coordination, and review the manuscript. All authors read and approved the final version of the manuscript.
Corresponding author
Ethics declarations
Competing interests
G.E.M. has received travel grants from Angelini Pharma, Laboratorios Rubió, Lundbeck, and Takeda for participating in psychiatric meetings. M.C. has received fees from Takeda and Laboratorios Rubió for participating in psychiatric meetings. The remaining authors declare no conflict of interest.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Pagerols, M., Autet, A., Prat, R. et al. The negative impact of neurodevelopmental disorders and multiple co-occurring conditions on academic performance of school-age children and adolescents. Sci Rep 16, 2406 (2026). https://doi.org/10.1038/s41598-025-27769-1
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-27769-1
