
Abstract
Models led by trained non-professionals or incorporating peer support may serve as promising alternative approaches to address shortages of healthcare personnel and substantial economic burdens. However, no comprehensive meta-analysis has yet evaluated whether models led by non-healthcare professionals and supported by peers can achieve effectiveness comparable to those led by healthcare professionals and without peer support in improving metabolic outcomes. This meta-analysis aims to address this existing knowledge gap. Randomized controlled trials (RCTs) were systematically searched in eight Chinese and English databases from their inception to February 1, 2025. Meta-analyses, subgroup analyses, and sensitivity analyses were performed using RevMan 5.4 and Stata 18.0 software. The quality of evidence for each outcome indicator was evaluated using the online tool GRADEpro GDT. A total of 30 studies were included in the meta-analysis. The findings demonstrated that community-based interventions had a significant effect on improving HbA1c (MD = − 0.57, 95% CI = − 0.69 to − 0.45, P < 0.00001), 2-h plasma glucose (MD = − 1.68, 95% CI = − 2.24 to − 1.12, P < 0.00001), fasting glucose (MD = − 0.98, 95% CI = − 1.16 to − 0.79, P < 0.00001), total cholesterol (MD = − 0.33, 95% CI = − 0.54 to − 0.11, P = 0.003), triglycerides (MD = − 0.60, 95% CI = − 0.87 to − 0.34 P < 0.00001), and body mass index (MD = − 1.40, 95% CI = − 1.99 to − 0.80, P < 0.00001) in patients with type 2 diabetes.However, the interventions did not lead to significant changes in high-density lipoprotein (MD = 0.06, 95% CI = − 0.01 to 0.13, P = 0.09) or low-density lipoprotein (MD = − 0.33, 95% CI = − 0.94 to 0.28, P = 0.29). Subgroup analyses indicated that interventions led by healthcare professionals were more effective than those led by non-healthcare professionals in improving HbA1c (subgroup difference P < 0.05). Moreover, peer support was less effective than non-peer support in reducing HbA1c levels (subgroup difference P = 0.0003). A comprehensive assessment of the quality of evidence included in this study indicates that, despite the substantial sample size, the level of evidence for all outcome measures remains low. Despite the low certainty of evidence, the achievement of clinically meaningful reductions in HbA1c(approximately 0.30% and 0.26% in subgroup analyses) supports the use of non-professional and peer-support models as pragmatic, second-best alternatives to professional-led care in resource-limited settings.
Similar content being viewed by others

Introduction
Type 2 diabetes (T2D) is a chronic metabolic disorder characterized by persistent disturbances in glucose, protein, and lipid metabolism, resulting from a complex interplay of genetic, environmental, and lifestyle factors1.It is associated with a high risk of microvascular and macrovascular complications, as well as elevated rates of mortality and disability2.According to the 11th edition of the International Diabetes Federation’s Global Diabetes Atlas, China has the largest number of individuals with diabetes worldwide. In 2024, the estimated number of adults with diabetes in China reached approximately 148 million, with projections indicating an increase to 168.3 million by 20503.
Evidence indicates that community-based diabetes management can leverage the strengths of primary healthcare systems to promote healthy lifestyles, control key risk factors, facilitate appropriate patient triage, and manage medical costs effectively4,5. However, current models face significant challenges, including shortages of trained healthcare personnel and substantial economic burdens6, particularly in resource-limited settings. In this context, the development of cost-effective and less resource-intensive management strategies is critically important. To reduce reliance on professional healthcare providers, trained non-professionals—such as peer educators and community health workers (CHWs)—have been increasingly integrated into community diabetes care, demonstrating promising outcomes7,8. Furthermore, growing evidence suggests that such lay-led approaches are cost-effective in diabetes management, adding to their potential value9,10,11. However, the effectiveness of these models may be influenced by challenges such as ensuring the quality and standardization of training, adequate supervision, and the scope of responsibilities assigned to lay personnel. Non-healthcare professionals refer to individuals without formal clinical training who engage in health promotion activities under the supervision of qualified healthcare providers12. These personnel primarily include peer educators and CHWs. Peer educators13 are individuals from the target population who share similar sociodemographic or experiential backgrounds with patients; they deliver education and support through shared experiences and skill-building. CHWs14, also known as lay health workers or community health representatives, are frontline public health practitioners who are trusted members of their communities and possess deep contextual knowledge of local health needs.
Several previous systematic reviews and meta-analyses have confirmed the role of interventions that are not supported by healthcare professionals and peers compared with usual care for type 2 diabetes. Meta-analyses of peer support models have shown that peer support interventions significantly improve HbA1c levels compared with usual care, highlighting their value as an adjunct to standard diabetes management15,16.Similarly, for interventions led by community health workers and other lay professionals, systematic reviews consistently reported statistically significant and clinically meaningful reductions in HbA1c, affirming the absolute efficacy of the model relative to the passive control condition17,18,19. However, the evidence regarding their impact on comprehensive metabolic outcomes, particularly lipid profiles, remains inconsistent and inconclusive20,21. These conflicting findings highlight a significant gap in understanding the full scope of metabolic benefits offered by these alternative models.
The existing comprehensive literature, however, has an important limitation. The prevailing, unresolved question has evolved: it is no longer merely “Is peer support effective?” but rather “How effective is it compared to the standard of professional-led care?” Similarly, for implementer selection, the key inquiry is whether non-healthcare professionals can achieve outcomes comparable to healthcare professionals. To the best of our knowledge, no previous meta-analysis has specifically undertaken this crucial comparison. This meta-analysis therefore aims to directly compare the effectiveness of community-based interventions led by non-healthcare professionals or incorporating peer support with that of those led by healthcare professionals or without peer support in improving metabolic outcomes for patients with type 2 diabetes.
Methods
Protocol and registration
This systematic review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines22(Supporting Information 1) . The study protocol was prospectively registered in PROSPERO (registration number: CRD420251084793).
Search strategy and inclusion criteria
A comprehensive literature search was performed across eight databases: PubMed, Cochrane Library, Web of Science, Embase, China National Knowledge Infrastructure (CNKI), Wanfang Data Knowledge Service Platform, VIP Database for Chinese Technical Periodicals, and the Chinese Biomedical Literature Database, covering all publications up to February 2025. The search strategy combined Medical Subject Headings (MeSH) terms and free-text keywords, which were iteratively refined through pilot testing. Key search terms included “Diabetes Mellitus, Type 2,” “Community Health Services,” and “Randomized Controlled Trial.” Detailed search strategies for the four English-language databases are provided in Supporting Information 2.
Studies were eligible for inclusion if they met the following criteria: (1) randomized controlled trial (RCT) design; (2) participants aged ≥ 18 years with a confirmed diagnosis of T2D; (3) interventions delivered in community settings by healthcare providers, CHWs, or peer educators; (4) control group receiving standard community care or routine management; and (5) intervention duration of at least six months.
Exclusion criteria comprised studies involving patients with severe acute or chronic comorbidities, those lacking detailed intervention descriptions, and publications for which full texts were unavailable.
For the subgroup analyses comparing different implementing entities or intervention methods, we adopted an “either-or” inclusion criterion. Specifically, studies were excluded from these analyses if they utilized hybrid models (e.g., involving both healthcare and non-healthcare professionals, or incorporating both peer and non-peer support). This ensured that each subgroup contained only studies with a single, clearly defined type of implementer or intervention for a direct comparison.
Literature screening and data extraction were managed using EndNote and Rayyan software. Two reviewers (Xuanning Luo and Chuanlei Zheng) independently screened titles, abstracts, and full texts. Any discrepancies were first discussed between them to reach a consensus. If an agreement could not be reached, a third senior investigator (Qingfeng Wu) was consulted to make the final decision.
Data extraction and outcome assessments
Data were independently extracted by two authors (Xuanning Luo and Chuanlei Zheng) using a standardized form. Extracted information included study characteristics such as baseline demographics, intervention components (type, duration, frequency), and outcome measures. Descriptive statistics—including sample sizes, means, and standard deviations for both intervention and control groups—were recorded. Primary outcomes were glycated hemoglobin (HbA1c), fasting plasma glucose (FPG), and 2-h postprandial glucose (2h-PPG). Secondary outcomes encompassed total cholesterol (TC), high-density lipoprotein (HDL), low-density lipoprotein (LDL), triglycerides (TG), and body mass index (BMI). For cluster-randomized trials, we preferentially extracted effect estimates (e.g., mean differences) and measures of variance (e.g., confidence intervals or standard errors) that were already adjusted for the intra-cluster correlation (ICC), as reported by the primary study authors using methods such as generalized estimating equations (GEE) or mixed-effects models.
Quality appraisal
Given that all included studies were RCTs, methodological quality was assessed using the Cochrane Collaboration’s risk of bias tool. Two reviewers (Xuanning Luo and Chuanlei Zheng) independently evaluated seven domains: random sequence generation (selection bias), allocation concealment (selection bias), blinding of participants and personnel (performance bias), blinding of outcome assessors (detection bias), incomplete outcome data (attrition bias), selective reporting (reporting bias), and other potential biases. Each domain was classified as low, unclear, or high risk of bias. A Summary of Findings table was generated using GRADEpro GDT software (Evidence Prime Inc., McMaster University, 2020) to evaluate the overall certainty of evidence. Conflicts were resolved through consultation with additional team members.
Operational definition of subgroup analysis
Classification of implementing entities
-
(1)
Healthcare professional-Led: Interventions primarily delivered by licensed healthcare providers—such as physicians, nurses, and other certified clinicians—who assume responsibility for clinical decision-making, patient education, and follow-up assessments.
-
(2)
Non-healthcare professional-Led12: Interventions led by CHWs, peer educators, or similar non-clinical personnel who serve as the primary point of contact and provide ongoing support to patients.
-
(3)
Hybrid intervention: Models in which leadership responsibilities are shared between healthcare and non-healthcare professionals, with neither group clearly dominant in intervention delivery.
Classification of intervention methods
-
(1)
Peer support23: Defined as emotional, appraisal, and informational support provided by individuals with lived experience of diabetes who share key characteristics with the target population. Such support aims to address psychosocial and behavioral challenges related to disease management.
-
(2)
Non-peer support: Interventions delivered by trained professionals without personal experience of the condition, excluding peer-led components.
-
(3)
Hybrid intervention: Models integrating both professional and peer support elements, with balanced contributions from both parties.
Data analysis
Meta-analyses were performed using RevMan 5.4 and Stata 18.0. All outcomes were continuous variables; mean difference (MD) was used as the effect size measure, reported with 95% confidence intervals (CIs). Statistical significance was set at P < 0.05. Heterogeneity was assessed using the I2 statistic and Cochran’s Q test. A random-effects model was applied in cases of substantial heterogeneity (I2 ≥ 50% or P ≤ 0.10); otherwise, a fixed-effects model was used (I2 < 50% and P > 0.10). For the meta-analysis of cluster-randomized trials, we utilized the adjusted effect estimates (accounting for intra-cluster correlation) as reported by the primary study authors. All included cluster-RCTs provided such adequately adjusted analyses. Should substantial heterogeneity be identified, we pre-planned to explore its sources using meta-regression analysis with key study-level covariates. Predefined subgroup analyses were conducted based on implementing entities (healthcare vs. non-healthcare professionals) and intervention methods (peer vs. non-peer support). Sensitivity analyses were performed by sequentially excluding individual studies to evaluate result robustness. Publication bias was assessed using Egger’s regression asymmetry test.
Results
Search results
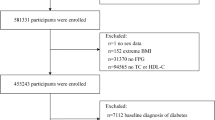
In the initial and updated literature search, a total of 9019 records were identified after duplicate removal. After screening titles and abstracts, 2385 full-text articles were reviewed for further evaluation. Ultimately, thirty studies met the inclusion criteria and were selected for data extraction and quantitative analysis24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53. The detailed article screening process is presented in Fig. 1.

PRISMA flowchart.
Characteristics of the included studies
The included articles comprised a total of 29,904 patients, with 18,535 assigned to the intervention groups and 11,369 to the control groups. Outcomes were reported as follows: thirty articles provided data on HbA1c, twelve on 2h-PPG, twenty on FPG, fifteen on TC, thirteen on HDL, sixteen on LDL and TG, and eleven on BMI. The detailed baseline characteristics are presented in Table 1.
Quality appraisal
The details of the assessment are presented in Fig. 2. Among the included studies, 26 studies reported the method used to generate random sequences, while four articles43,44,45,47 were judged to have an unclear risk of bias due to insufficient reporting on randomization procedures. Only five articles32,42,48,51,52 explicitly mentioned allocation concealment; the remaining studies did not provide specific information, resulting in an unclear risk of bias for this domain. Regarding blinding of participants and investigators, ten articles25,26,30,41,42,43,46,50,51,52, were assessed as having a high risk of bias due to the absence of blinding measures, whereas the remaining studies did not specify whether blinding was implemented, leading to an unclear risk classification. Concerning blinding of outcome assessment, only five articles45,46,49,52,53, clearly stated that outcome assessors were blinded, and were therefore rated as low risk; the rest provided no relevant information, resulting in an unclear risk of bias. With regard to incomplete outcome data, five studies31,32,34,38,39, reported participant dropout rates but failed to describe how missing data were handled, thus being classified as unclear risk of bias. In terms of selective outcome reporting, all studies were judged to be at low risk, as there was no evidence of selective reporting. Finally, the assessment of other potential biases indicated a low risk across all included studies.

Risk of bias (ROB) assessment (A) ROB summary. (B) ROB graph.
Primary outcomes
HbA1c was used as an outcome measure in all 30 studies24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53, encompassing a total of 29,904 participants. There was substantial heterogeneity among the studies (I2 = 91%), thus a random-effects model was applied for the meta-analysis. The results indicated that the intervention group achieved a significantly greater reduction in HbA1c levels compared to the control group (MD = − 0.57, 95% CI = − 0.69 to − 0.45, P < 0.00001;95% Prediction Interval: − 1.23 to 0.08)(Fig. 3).This meta-analysis demonstrates that community-based interventions are associated with a statistically significant and clinically meaningful reduction in HbA1c levels.

Meta-analysis forest plot comparing HbA1c levels between the intervention group and the control group.
A total of 12 studies24,25,26,27,29,31,33,34,35,36,37,53, included 2h-PPG level as an outcome measure, involving 2908 participants. Significant heterogeneity was observed across the studies (I2 = 88%), and therefore a random-effects model was employed for the meta-analysis. The results indicated that the intervention group achieved a significantly greater improvement in 2h-PPG levels compared with the control group compared to the control group(MD = − 1.68, 95% CI = − 2.24 to − 1.12, P < 0.00001;95% Prediction Interval: − 3.65 to 0.29) (Fig. 4).These findings indicate a robust improvement in postprandial glucose control following the implementation of community management models.

Meta-analysis forest plot comparing postprandial 2 h-PPG levels between the intervention group and the control group.
There were 20 studies24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,42,44,46,52, that included FPG as an outcome measure, involving a total of 26,586 participants.Substantial heterogeneity was observed across the studies (I2 = 82%), and therefore a random-effects model was used for the meta-analysis. The results indicated that the intervention group showed significantly greater improvement in FPG levels compared to the control group (MD = − 0.98, 95% CI = − 1.16 to − 0.79, P < 0.00001;95% Prediction Interval: − 2.02 to 0.04) (Fig. 5).Community interventions therefore also confer a significant benefit on fasting glycemia. Thus, community-based management appears to have a modest but significant positive impact on total cholesterol.

Meta-analysis forest plot comparing FPG levels between the intervention group and the control group.
Secondary results
A total of 15 studies24,25,26,28,33,34,36,37,39,40,43,44,46,49,53, included TC as an outcome measure, encompassing 5228 participants in total. High heterogeneity was observed across these studies (I2 = 93%), so a random-effects model was employed for the meta-analysis. The results indicated that the improvement in TC levels in the intervention group was significantly greater than that in the control group (MD = − 0.33, 95% CI = − 0.54 to − 0.11, P = 0.003;95% Prediction Interval: − 1.44 to 0.77) (Fig. 6). Thus, community-based management appears to have a modest but significant positive impact on total cholesterol.

Meta-analysis forest plot comparing TC levels between the intervention group and the control group.
Among the 13 studies24,25,26,28,33,34,36,37,39,40,43,44,46, that included HDL as an outcome measure, a total of 3977 participants were analyzed. Significant heterogeneity was observed across the studies (I2 = 92%), thus a random-effects model was employed for the meta-analysis. The results indicated that the improvement in HDL levels in the intervention group was not statistically significant (MD = 0.06, 95% CI = − 0.01 to 0.13, P = 0.09; 95% Prediction Interval: − 0.28 to 0.40) (Fig. 7). In summary, the intervention did not lead to a statistically significant improvement in HDL cholesterol levels.

Meta-analysis forest plot comparing HDL levels between the intervention group and the control group.
A total of 16 studies24,25,26,28,33,34,36,37,39,40,42,43,44,46,50,52, included LDL as an outcome measure, involving 25,706 participants in total. High heterogeneity was observed across these studies (I2 = 100%), so a random-effects model was employed for the meta-analysis. The results indicated that the improvement in LDL levels in the intervention group was not statistically significant (MD = − 0.33, 95% CI = − 0.94 to 0.28, P = 0.29;95% Prediction Interval: − 1.08 to 1.01) (Fig. 8). Overall, no significant effect of community interventions on LDL cholesterol was observed.

Meta-analysis forest plot comparing LDL levels between the intervention group and the control group.
A total of 16 studies24,25,26,28,29,33,34,36,37,38,39,40,43,44,46,52, reported TG levels as an outcome measure, encompassing 5184 participants in total. Substantial heterogeneity was observed across these studies (I2 = 98%), thus a random-effects model was applied for the meta-analysis. The results indicated that the improvement in TG levels in the intervention group was significantly greater than that in the control group (MD = − 0.60,95% CI = − 0.87 to − 0.34, P < 0.00001; 95% Prediction Interval: − 4.23 to 2.79) (Fig. 9). This represents a significant reduction in triglyceride levels, suggesting a favorable effect on this key aspect of lipid profile.

Meta-analysis forest plot comparing TG levels between the intervention group and the control group.
Eleven studies24,25,26,33,37,39,41,44,50,51,52, included BMI as an outcome measure, involving a total of 2766 participants. Considerable heterogeneity was observed across the studies (I2 = 86%), and therefore a random-effects model was employed for the meta-analysis. The results indicated that the improvement in BMI in the intervention group was significantly greater than that in the control group (MD = − 1.40, 95% CI = − 1.99 to − 0.80, P < 0.00001;95% Prediction Interval: − 3.33 to 0.63) (Fig. 10). The findings support that community management models are effective in achieving a statistically significant reduction in body mass index.

Meta-analysis forest plot comparing BMI between the intervention group and the control group.
Subgroup analysis
Different implementing entities
Subgroup analyses were conducted according to the implementing entities—specifically, healthcare professionals versus non-healthcare professionals. The results indicated that FPG, TC, HDL, LDL, TG and BMI levels were not significantly influenced by the type of implementing entity (subgroup difference P-values: 0.98, 0.34, 0.47, 0.62, 0.06 and 0.18, respectively). However, the implementing entity had a differential impact on HbA1c. Compared with interventions led by non-healthcare personnel, those led by healthcare professionals demonstrated more significant improvements (P < 0.05). Interventions conducted by healthcare personnel also resulted in a significant reduction in 2h-PPG levels. However, the inclusion of only one study in the non-healthcare personnel group precluded a reliable assessment of the true difference in impact on this indicator based on the implementing entity. To maintain homogeneity within subgroups regarding implementation entities, two studies were excluded from the analysis as they reported involvement from both healthcare and non-healthcare professionals, as detailed in Table 2.(Supporting Information 9).
Different intervention methods
Subgroup analysis based on intervention type (peer support vs. non-peer support) revealed that non-peer support interventions had a significantly greater effect on HbA1c levels (subgroup difference P < 0.00001), particularly in relation to blood glucose and BMI. Only one study included postprandial 2-hPPG, HDL, and LDL as companion measures, which renders it impossible to reliably assess the true differences in the effects of the intervention methods on these indicators. For other blood glucose, lipid markers and BMI, improvements did not show significant variation according to the intervention method. To maintain subgroup homogeneity, three studies employing mixed interventions that included peer support were excluded from this analysis, as detailed in Table 3.(Supporting Information 9).
Investigation of heterogeneity and sensitivity analyses
Meta-regression
To further investigate the high heterogeneity observed in the meta-analysis, univariate random-effects meta-regression analyses were conducted on a series of covariates, including baseline levels, intervention duration, sample size, mean patient age, the study’s geographic location (specifically whether it was conducted in China), and the mode of intervention delivery. The results indicate that the sources of heterogeneity vary across outcome measures. Specifically, baseline TG levels emerged as a highly significant determinant of effect size (β = − 0.634, P < 0.001), explaining up to 87.22% of the variation between studies. For TC, the effect size was similarly significantly influenced by its baseline level (β = − 0.191, P = 0.044), while study sample size also emerged as a significant factor (β = 0.335, P = 0.045). In a subgroup analysis specific to 2 h-PPG, a significant negative correlation was observed between mean patient age and effect size (β = − 0.094, P = 0.048). However, none of the aforementioned covariates demonstrated statistically significant associations with other primary outcome measures including LDL, HDL, BMI, HbA1c, or FPG. In summary, this exploratory analysis successfully identified partial sources of heterogeneity in TG, TC, and 2 h-PPG. Nevertheless, the high heterogeneity observed in the remaining indicators remains primarily attributable to other complex factors not measured in this study. (Supporting Information 5).
Sensitivity analysis
Sensitivity analyses were conducted by sequentially excluding individual studies. Following the removal of studies contributing to heterogeneity, the intervention effects across all outcomes remained largely unchanged compared to the original analysis, suggesting the robustness and reliability of the results ( Supporting Information 4).To test the robustness of the conclusions derived from the primary subgroup analyses—comparing different implementing bodies and intervention methods—we conducted a sensitivity analysis by reclassifying and including studies with mixed intervention models that were initially excluded based on the ‘predominant lead’ rule. The results indicated that the key subgroup differences remained stable. (Supporting Information 7) To evaluate the generalizability of the study findings beyond the Chinese context, we performed a sensitivity analysis that included only ten international studies. Regarding the primary outcome measure, the analysis demonstrated that community interventions still had a significant effect on improving glycated hemoglobin (MD = − 0.49, 95% CI [− 0.78, − 0.20]), which aligns with the conclusions of the main analysis. For the secondary outcome measures, the results exhibited divergence. While the improvement in body mass index remained significant, the enhancements in total cholesterol (MD = − 0.01, 95% CI [− 0.10, 0.07]) and triglycerides (MD = − 0.11, 95% CI [− 0.23, 0.00]) were no longer statistically significant. Due to the limited number of studies reporting 2-h postprandial blood glucose (n = 0) and fasting blood glucose (n = 1) in international research, reliable conclusions could not be drawn regarding these outcomes.( Supporting Information 8).
Certainty of evidence and publication bias
The certainty of the evidence was assessed using the GRADE criteria ( Supporting Information 3). All outcomes were rated as having low certainty. This downgrade was primarily due to methodological limitations and substantial heterogeneity, which affected the domains of risk of bias and inconsistency, respectively. Publication bias was assessed through visual inspection of funnel plots and Egger’s statistical test( Supporting Information 4, 6). Egger’s test indicated no statistically significant evidence of small-study effects for any outcome (P > 0.05), with the exception of TG, which showed potential publication bias (P < 0.05). To further evaluate the robustness of the triglyceride findings in light of this potential bias, we conducted a trim-and-fill analysis. The results revealed that no studies needed to be imputed, and the pooled effect estimate remained unchanged (exp(ES) = 0.486, 95% CI: 0.221–1.068). This suggests that while statistical tests indicated potential publication bias for triglycerides, the actual impact on the pooled effect size appears to be minimal.
Discussion
Summary of key findings
This study, based on a meta-analysis of 30 RCTs conducted in the community, demonstrates that the community management model significantly improves levels of HbA1c, 2h-PPG, FPG, TC, TG, and BMI in patients with T2D. However, the model did not show statistical significance in improving HDL and LDL. Key findings from subgroup analysis provide new insights for optimizing resource allocation. Interventions led by medical professionals were significantly more effective in improving HbA1c levels compared to those led by non-medical professionals (subgroup difference P = 0.0002). Similarly, the non-peer support model was found to be more effective than the peer support model in reducing HbA1c levels (subgroup difference P = 0.0003).
Comparison with prior literature
The findings of this study are consistent with the extensive body of literature that confirms the effectiveness of community management in glycemic control for patients with T2D20,54,55,56,57.Regarding lipid metabolism, the findings are consistent with those reported by White et al. 55.However, existing evidence reveals notable inconsistencies; for example, Lee et al.54 conducted a meta-analysis that identified a significant reduction in TG levels, yet no substantial improvements were observed in other lipid parameters. The Siang Joo Seah team58, reported that LDL was the only parameter that did not demonstrate significant improvement, while all other lipid parameters were notably optimized. This inconsistency may arise from differences in the baseline metabolic status of study participants or variations in the intervention protocols focusing on specific lipoproteins. Additionally, from a physiological mechanism perspective, insulin resistance enhances the activity of cholesterol ester transfer protein, leading to accelerated degradation of HDL particles, which may limit the effectiveness of lifestyle interventions on this parameter59. Therefore, from a clinical standpoint, the role of community management in comprehensively optimizing the atherogenic lipid profile is likely ancillary. Our findings underscore that to achieve comprehensive cardiovascular risk management in patients with T2D, effective community-based models must be integrated with necessary lipid-lowering pharmacotherapy. Most previous studies typically only validate the absolute efficacy of community interventions compared to routine care, or do not strictly differentiate between the implementing entities16,55. Through direct subgroup comparisons, this study provides quantitative evidence for the optimized allocation of resources regarding the relative effectiveness of “medical professionals versus non-medical professionals” and “peer support versus non-peer support” models.
Interpretation of subgroup findings: implications for resource allocation
Effectiveness of healthcare professionals and non-healthcare professionals
The advantages of interventions by healthcare professionals are closely tied to their professional qualifications and clinical decision-making abilities. For example, physicians can dynamically adjust treatment goals based on factors such as patient age, comorbidities, and functional status, while conducting structured follow-ups in line with evidence-based guidelines. This enables the implementation of multidimensional interventions addressing physiological, psychological, and behavioral aspects60. These comprehensive management capabilities, rooted in extensive medical knowledge and clinical expertise, are essential for optimizing glycemic control and preventing complications. In contrast, models involving non-healthcare professionals demonstrate notable limitations in effectiveness. Although CHWs have been involved in diabetes care for decades, their training and support systems remain insufficient61. A review by the United States Agency for International Development62 identified critical deficiencies in these training systems, including a lack of professional knowledge and skills, inadequate supervision, and the absence of standardized, mandatory certification and continuous oversight mechanisms. These deficiencies represent primary factors that hinder CHWs’ ability to provide high-quality services. This finding does not contradict but rather contextualizes the conclusions of prior literature63,64. Those studies established the absolute efficacy of peer support over passive usual care. The present analysis, by contrast, reveals its relative efficacy within a hierarchy of active strategies. The key explanatory factor is the nature of the comparator group. This clarifies that peer support’s advantage is most pronounced in resource-limited settings, while its benefit may be smaller when directly compared to professionally-led interventions.
Effectiveness of peer support and non-peer support models
The variability in the effectiveness of peer support models may stem from differences in their underlying mechanisms and the contextual conditions under which they are implemented. Peer support operates through experiential resonance and emotional connections, whereby peer educators share personal experiences, assist in problem-solving, set achievable goals, maintain regular interactions, and cultivate trust-based relationships. These strategies aim to stimulate patients’ intrinsic motivation by helping them identify their needs, develop a readiness for change, and experience a sense of emotional belonging. Consequently, this process can facilitate behavioral changes such as consistent medication adherence, healthier eating habits, and increased self-efficacy. However, the success of this mechanism in generating meaningful and sustained health improvements is heavily contingent upon the individual circumstances of the recipients.
The core mechanism of peer support assumes that patients possess favorable baseline conditions. For individuals facing severe economic hardship, complex health issues, or compromised physical and mental well-being, their immediate priorities often center on resolving survival crises or alleviating acute suffering. In such contexts, while peer-provided emotional support offers psychological relief, it often fails to result in significant improvements in health-related behaviors65. Enhancing the effectiveness of peer support may require incorporating ‘active ingredients’ such as structured training; closer integration with clinical teams; and the use of validated protocols. This may be a primary reason why peer support models are less effective compared to non-peer support models.
Clinical and public health significance of modest effects
After establishing the relative effectiveness of different models, interpreting the practical significance of their effect sizes, particularly in the context of the uneven distribution of medical resources, emerges as another critical issue. The subgroup analysis revealed that while the effects of non-medical professional-led models and peer support models in reducing HbA1c were limited, with reductions of only 0.3% and 0.26% respectively, these outcomes still hold significant clinical relevance in specific contexts. Firstly, the ADA guidelines indicate that the relationship between HbA1c and microvascular complications is continuous and curvilinear. This implies that any reduction in HbA1c, regardless of how small, can lead to a corresponding decrease in the risk of complications66.
According to the risk model from the UKPDS study, a 0.3% reduction in HbA1c is associated with an estimated 6% reduction in the risk of diabetes-related mortality, 4% reduction in myocardial infarction, and 11% reduction in microvascular complications67. While this effect may appear modest at the individual level, it can translate into substantial public health benefits when applied across large populations. Second, in regions with limited medical resources, access to healthcare services is often constrained, and even a small improvement in glycemic control may have a meaningful impact on population health. For instance, when a patient’s HbA1c level is nearing the 8% threshold for accelerated complications, a reduction of 0.3% can help halt the worsening trend and alleviate the strain on scarce resources caused by acute complications. Furthermore, treatment targets should be individualized based on clinical factors such as age, duration of diabetes, complication risk, and life expectancy. In elderly patients or those with advanced complications who are more vulnerable to hypoglycemia, glycemic goals may be appropriately relaxed. Hypoglycemia not only poses immediate health risks but is also linked to an increased likelihood of cardiovascular events and mortality. Interventions that achieve gradual and sustained reductions in HbA1c may therefore offer enhanced safety and long-term clinical benefit. In summary, although non-healthcare professional-led models and peer support initiatives demonstrate modest efficacy in lowering HbA1c, their clinical relevance and public health value in specific settings should not be overlooked66,68.
Heterogeneity and context dependency
A paramount consideration in interpreting our findings is the substantial heterogeneity observed across most meta-analyses (I2 often > 90%). While this degree of variability is not uncommon in meta-analyses of complex, real-world community interventions, it necessitates caution in deriving definitive conclusions. This heterogeneity likely stems from a confluence of factors inherent to the included studies. These include variations in the specific components and intensity of the interventions, differences in the training and experience of the lay personnel delivering them, diverse demographic and clinical characteristics of the participant populations across studies, and variations in the standard of ‘usual care’ provided to control groups. We conducted extensive meta-regression and sensitivity analyses to explore these sources; however, as reported, we could only explain a portion of the heterogeneity for certain outcomes like TG and TC, while for others, such as HbA1c, the sources remain largely unexplained. Consequently, the pooled effect estimates should be viewed as a summary of a wide range of potential effects rather than a single, precise truth. The wide prediction intervals, particularly for HbA1c, underscore that the true effect in a new, similar setting could vary considerably. Despite this, the consistent direction of benefit across nearly all glycemic and metabolic outcomes strengthens the inference that community-based management is generally advantageous, even if the magnitude of benefit is context-dependent.
Limitations
Absence of cost-effectiveness evidence
A key limitation of the evidence base is the absence of cost-effectiveness data. Given that a primary rationale for exploring alternative models is to alleviate substantial economic burdens, it is a critical gap that none of the included studies provided standardized economic outcome data. Consequently, our review cannot inform whether the modest clinical benefits of non-professional or peer-support models are achieved in a cost-efficient manner. This lack of economic evidence significantly hinders the practical decision-making for policymakers who must allocate limited healthcare resources.
Limited generalizability beyond the Chinese context
A paramount consideration in interpreting our findings is the predominance of studies conducted in China. This geographical concentration, while reflective of the substantial research activity in community diabetes management within China’s rapidly evolving primary healthcare system, poses a significant challenge to the generalizability of our results. Our sensitivity analysis, which excluded China-dominant studies, underscored this concern by revealing that the significant improvements in total cholesterol and triglycerides observed in the main analysis were not sustained in the international cohort (Supporting Information 8). This suggests that the lipid-lowering benefits of community management may be more context-dependent than the glycemic benefits, which remained robust for HbA1c.
Several features of the Chinese healthcare context may explain these differences. The strong, centralized structure of community health centers may facilitate the standardized implementation of interventions. Furthermore, the integration of Traditional Chinese Medicine principles, as seen in several included studies25,26,29, may contribute unique benefits not captured in Western models. Additionally, the baseline “usual care” in control groups within China might differ in intensity from that in other countries, potentially amplifying the relative effect of the interventions. Consequently, while our hierarchical model is likely conceptually transferable, the absolute magnitude of benefit, particularly for lipid parameters, should be extrapolated with caution to dissimilar healthcare settings.
Methodological limitations and unexplained heterogeneity
This study is subject to several methodological constraints: (1) There are significant methodological limitations; only a few studies explicitly reported allocation concealment, and most did not implement blinding, which may overestimate the intervention effects. (2) The quality of evidence for all outcome measures is low, primarily due to significant clinical heterogeneity and the aforementioned methodological limitations. (3) The sources of heterogeneity are complex. In addition to the identified factors, significant variations in training content, skill levels, and supervision intensity among non-medical professionals across different studies represent potential sources of confounding in subgroup comparisons, contributing to heterogeneity. (4) Some subgroups included only a limited number of studies, and these results should be viewed as preliminary indications that must be interpreted with caution; definitive conclusions such as ‘equivalent effect’ or ‘no effect’ should be avoided.
Future directions
To strengthen the current evidence, future research should focus on specifically evaluating the efficacy of peer support on lipid outcomes in rigorously designed RCTs with adequate allocation concealment and blinding, validating the generalizability of lay models across diverse healthcare systems, and exploring the establishment of standardized training and certification frameworks. In addition, cost-effectiveness evaluations and safety monitoring must be incorporated as core components of the research agenda to provide a holistic assessment of these alternative implementation models.
Conclusions
This meta-analysis demonstrates that community-based management can lead to improvements in key glycemic parameters, triglycerides, and BMI in patients with T2D, despite non-significant effects on HDL and LDL and low certainty of evidence (GRADE). The findings support a tiered implementation approach: healthcare professional-led interventions are superior, but in resource-limited settings, non-professional and peer-support models serve as valuable second-best alternatives, achieving clinically relevant mean HbA1c reductions of 0.30% and 0.26%, respectively.
Data availability
The data that support the findings of this study are available from the corresponding author upon reasonable request.
References
Zhou, D. et al. The effect of Sancai powder on glycemic variability of type 2 diabetes in the elderly: A randomized controlled trial. Medicine 99, e20750 (2020).
Hippisley-Cox, J. & Coupland, C. Diabetes treatments and risk of amputation, blindness, severe kidney failure, hyperglycaemia, and hypoglycaemia: Open cohort study in primary care. BMJ 352, i1450 (2016).
Duncan, B. B., Magliano, D. J. & Boyko, E. J. IDF diabetes atlas 11th edition 2025: Global prevalence and projections for 2050. Nephrol. Dial. Transplant. (2025).
World Health Organization. Prevention and Control of Noncommunicable Diseases: Guidelines for Primary Health Care in Low Resource Settings. World Health Organization, (2012).
Gomez, M., Walker, K. Z. & Buckley, A. National evidence based guideline for the primary prevention of type 2 diabetes. In National Evidence Based Guidelines for the Management of Type 2 Diabetes. Girgis, S. (ed.) 4–165. Diabetes Australia, (2009).
Yao, J. S. The factors influencing the effect of the community-based type-2 diabetes mellitus management: A cross-sectional study in Shandong province, China. Thesis, Shandong University (2020).
Tang, T. S. et al. Comparative effectiveness of peer leaders and community health workers in diabetes self-management support: Results of a randomized controlled trial. Diabetes Care 37, 1525–1534 (2014).
McGowan, P., Lynch, S. & Hensen, F. The role and effectiveness of telephone peer coaching for adult patients with type 2 diabetes. Can. J. Diabetes 43, 399–405 (2019).
van Iseghem, T. et al. The cost-effectiveness of community health workers in primary health care: A systematic review. Value Health (2025).
González, L., Elgart, J. F. & Gagliardino, J. J. Education of people with type 2 diabetes through peers with diabetes: Is it cost effective?. Medwave 15, e6348 (2015).
Wingate, L. et al. Can peer support be cost saving? An economic evaluation of RAPSID: A randomized controlled trial of peer support in diabetes compared to usual care alone in east of England communities. BMJ Open Diabetes Res. Care 5, e000328 (2017).
Lewin, S. A. et al. Lay health workers in primary and community health care. Cochrane Database Syst. Rev. CD004015 (2005).
Lv, Z. Z. et al. The design of evaluation of an AIDS/STD/safer sex peer education program. Chin. J. Health Educ. 5–8 (1999).
Knowles, M. et al. Community health worker integration with and effectiveness in health care and public health in the United States. Annu. Rev. Public Health 44, 363–381 (2023).
Luo, J. et al. The effect of peer support on HbA1c levels in middle-aged and elderly patients with type 2 diabetes: A systematic review and meta-analysis. PeerJ 13, e19803 (2025).
Azmiardi, A. et al. The effect of peer support in diabetes self-management education on glycemic control in patients with type 2 diabetes: A systematic review and meta-analysis. Epidemiol Health 43, e2021090 (2021).
Little, T. V. et al. Community health worker interventions for Latinos with type 2 diabetes: A systematic review of randomized controlled trials. Curr. Diab. Rep. 14, 558 (2014).
Tay, J. H. T. et al. Effectiveness of lay-led, group-based self-management interventions to improve glycated hemoglobin (HbA1c), self-efficacy, and emergency visit rates among adults with type 2 diabetes: A systematic review and meta-analysis. Int. J. Nurs. Stud. 113, 103779 (2021).
Evans, J., Ha, H. & White, P. T. Evaluating the effectiveness of community health worker interventions on glycaemic control in type 2 diabetes mellitus: A systematic review and meta-analysis. BMJ Open 15, e096651 (2025).
Dong, C. et al. Effect of exercise interventions based on family management or self-management on glycaemic control in patients with type 2 diabetes mellitus: A systematic review and meta-analysis. Diabetol. Metab. Syndr. 15, 232 (2023).
Verma, I. et al. The impact of peer coach-led type 2 diabetes mellitus interventions on glycaemic control and self-management outcomes: A systematic review and meta-analysis. Prim. Care Diabetes 16, 719–735 (2022).
Shamseer, L. et al. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015: Elaboration and explanation. BMJ 350, g7647 (2015).
Dennis, C.-L. Peer support within a health care context: A concept analysis. Int. J. Nurs. Stud. 40, 321–332 (2003).
Ben, P. L. “Internet +”based health management platform improves the management effect of type 2 diabetes among community citizens. J. Qiqihar Med. Coll. 41, 2835–2839 (2020).
Cai, Y. N. & Zhang, C. M. The impact of traditional Chinese medicine-based health education on dietary habits and blood glucose control among diabetes patients in a community in Shanghai. Chin. J. Prev. Contr. Chron. Dis. 27, 786–789 (2019).
Shen, Y. et al. Study on the application value of Chinese medicine five-in-one in type 2 diabetes patients signed by family doctors. Chin. J. Gen. Pract. 18, 976–979 (2020).
Fan, L. M. et al. Effectiveness analysis of family doctor-led precision diabetes management and traditional management models. Chin. J. Prev. Contr. Chron. Dis. 24, 953–955 (2016).
Gong, W. J. et al. Application of the remote blood glucose control system for type 2 diabetes mellitus management in community. Chin. Gen. Pract. 21, 465–470 (2018).
Huang, C. Analysis on effect of chronic disease management of traditional Chinese medicine based on holistic view in patients with type 2 diabetes mellitus. Chin. Community Doct. 40, 131–133 (2024).
Li, H., Cui, H. & Huang, B. L. Observation on effect of team interactive management mode applied for patients with type 2 diabetes in community. Chin. Nurs. Res. 26, 2102–2104 (2012).
Li, X. B. et al. Effectiveness of systematic self-management education on blood sugar level of patients in the community with type 2 diabetes. J. Cent. South Univ. 37, 36–39 (2012).
Liu, H. J., Shi, M. H. & Xing, L. L. Long-term effect of peer support intervention on diabetes-related knowledge level and self-management in type 2 diabetic patients. Chin. Gen. Pract. 22, 4240–4245 (2019).
Luo, M. L., Liang, X. L. & Lv, P. Effect evaluation of intensive blood glucose monitoring by family doctors on blood glucose control in type 2 diabetes mellitus. Chin. Gen. Pract. 23, 1181–1184 (2020).
Peng, Y. et al. Studying on the influence of internet-based health education on the health literacy and self-management ability of patients with type 2 diabetes mellitus in communities. Chin. Health Serv. Manag. 38, 237–240 (2021).
Ren, C., Luo, L. M. & Dong, W. Effectiveness analysis of community family doctor individualized strategies in the management of type 2 diabetes patients. Chin. J. Prev. Contr. Chron. Dis. 26, 77–80 (2018).
Shen, L. J., Huang, C. F. & Kong, Y. The management effect of type 2 diabetes service package in Hongshan street community in Guangzhou City. Chin. Gen. Pract. 22, 1608–1612 (2019).
Wang, C. Y. & Lu, Z. Y. Effectiveness analysis of community diabetes management based on the internet of things technology. Chin. J. Gen. Pract. 14, 618–620 (2016).
Yu, K. P. et al. Analysis of the effectiveness of mobile medical apps among patients with type 2 diabetes in Qixinggang community, Yuzhong district, Chongqing. South China. J. Prev. Med. 46, 574–576 (2020).
Zhang, Z. Y., Zhong, J. J. & Feng, X. Effect of intervention of type 2 diabetes patients participating in community self-management group activities. China Trop. Med. 17, 798–801 (2017).
Davies, M. J. et al. Effectiveness of the diabetes education and self management for ongoing and newly diagnosed (DESMOND) programme for people with newly diagnosed type 2 diabetes: Cluster randomised controlled trial. BMJ 336, 491–495 (2008).
Debussche, X. et al. Structured peer-led diabetes self-management and support in a low-income country: The ST2EP randomised controlled trial in Mali. PLoS ONE 13, e0191262 (2018).
Jia, W. et al. Evaluation of an mHealth-enabled hierarchical diabetes management intervention in primary care in China (ROADMAP): A cluster randomized trial. PLoS Med. 18, e1003754 (2021).
Kim, M. T. et al. The effect of a community-based self-help intervention: Korean Americans with type 2 diabetes. Am. J. Prev. Med. 49, 726–737 (2015).
Kong, J. X. et al. Effectiveness of the chronic care model in type 2 diabetes management in a community health service center in China: A group randomized experimental study. J. Diabetes Res. 2019, 6516581 (2019).
Lynch, E. B. et al. Randomized trial of a lifestyle intervention for urban low-income African Americans with type 2 diabetes. J. Gen. Intern. Med. 34, 1174–1183 (2019).
Pérez-Escamilla, R. et al. Impact of a community health workers-led structured program on blood glucose control among latinos with type 2 diabetes: The DIALBEST trial. Diabetes Care 38, 197–205 (2015).
Presley, C. et al. Mobile-enhanced peer support for African Americans with type 2 diabetes: A randomized controlled trial. J. Gen. Intern. Med. 35, 2889–2896 (2020).
Sherifali, D. et al. Effect of computer-generated tailored feedback on glycemic control in people with diabetes in the community: A randomized controlled trial. Diabetes Care 34, 1794–1798 (2011).
Simmons, D. et al. Impact of community based peer support in type 2 diabetes: A cluster randomised controlled trial of individual and/or group approaches. PLoS ONE 10, e0120277 (2015).
Spencer, M. S. et al. Effectiveness of a community health worker intervention among African American and Latino adults with type 2 diabetes: A randomized controlled trial. Am. J. Public Health 101, 2253–2260 (2011).
Tang, T. S. et al. Study protocol and baseline sample characteristics: from clinic to community: Using peer support as a transition model for improving long-term diabetes-related health outcomes. Contemp. Clin. Trials 79, 104–110 (2019).
Zhang, P. et al. Improving the management of type 2 diabetes in China using a multifaceted digital health intervention in primary health care: The SMARTDiabetes cluster randomised controlled trial. Lancet Reg. Health West. Pac. 49, 101130 (2024).
Deng, K. et al. Peer support training improved the glycemic control, insulin management, and diabetic behaviors of patients with type 2 diabetes in rural communities of central China: A randomized controlled trial. Med. Sci. Monit. 22, 267–275 (2016).
Lee, J. J. N. et al. Effects of mobile health interventions on health-related outcomes in older adults with type 2 diabetes: A systematic review and meta-analysis. J. Diabetes 15, 47–57 (2023).
White, L. et al. The effectiveness of clinician-led community-based group exercise interventions on health outcomes in adults with type 2 diabetes mellitus: A systematic review and meta-analysis. Int. J. Environ. Res. Public Health 21(5), 601 (2024).
Plotnikoff, R. C. et al. Community-based physical activity interventions for treatment of type 2 diabetes: A systematic review with meta-analysis. Front. Endocrinol. 4, 3 (2013).
Pan, B. et al. Exercise training modalities in patients with type 2 diabetes mellitus: A systematic review and network meta-analysis. Int. J. Behav. Nutr. Phys. Act. 15, 72 (2018).
Seah, S. J., Zheng, H. & Lim, R. B. T. Efficacy of community-based self-care interventions to improve biophysical, psychosocial or behavioural outcomes among community-dwelling older adults with type 2 diabetes: A systematic review and meta-analysis. Diabetes Res. Clin. Pract. 169, 108411 (2020).
Jaiswal, M., Schinske, A. & Pop-Busui, R. Lipids and lipid management in diabetes. Best Pract. Res. Clin. Endocrinol. Metab. 28, 325–338 (2014).
Ivers, N. M. et al. Diabetes Canada 2018 clinical practice guidelines: key messages for family physicians caring for patients living with type 2 diabetes. Can. Fam. Physician 65, 14–24 (2019).
Lehmann, L. S. D. Community health workers: what do we know about them? The state of the evidence on programmes, activities, costs and impact on health outcomes of using community health workers. World Health Organization (2007).
USAID. Factors impacting the effectiveness of community health worker behavior change: A literature review. United States Agency for International Development (2015).
Liang, D. et al. The effectiveness of peer support on self-efficacy and self-management in people with type 2 diabetes: A meta-analysis. Patient Educ. Couns. 104, 760–769 (2021).
Kong, L. N., Hu, P. & Yang, L. The effectiveness of peer support on self-efficacy and quality of life in adults with type 2 diabetes: A systematic review and meta-analysis. J. Adv. Nurs. 75, 711–722 (2019).
Garn, S. D. et al. Understanding the mechanisms generating outcomes in a Danish peer support intervention for socially vulnerable people with type 2-diabetes: A realist evaluation. Arch. Public Health 79, 160 (2021).
Elsayyed, N. A. et al. 6. Glycemic targets: Standards of care in diabetes—2023. Diabetes Care 46, S97–S110 (2022).
UK Prospective Diabetes Study (UKPDS) Group. Intensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33). Lancet 352, 837–853 (1998).
Davies, M. J. et al. Management of hyperglycemia in type 2 diabetes, 2022. A consensus report by the American diabetes association (ADA) and the European association for the study of diabetes (EASD). Diabetes Care 45, 2753–2786 (2022).
Funding
The authors received no specific funding for this work.
Author information
Authors and Affiliations
Contributions
Conception or design: Xuanning Luo Acquisition, analysis, or interpretation of data: Chuanlei Zheng; Xuanning Luo. Drafting the work or revising: Xuanning Luo. Final approval of the manuscript: Xuanning Luo; Chuanlei Zheng; Qingfeng Wu.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Luo, X., Zheng, C. & Wu, Q. Systematic review of healthcare-led and lay-led interventions for type 2 diabetes in community settings. Sci Rep 15, 44433 (2025). https://doi.org/10.1038/s41598-025-28010-9
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-28010-9
