
Abstract
The administrative chief duty system is a cornerstone of hospital governance to ensure continuity, coordination, and responsiveness during off-hours. This study evaluated the implementation and performance of the system in a tertiary reproductive hospital in Guangxi Zhuang Autonomous Region, China, drawing on personnel data, duty records, and staff interviews. Fifty-two duty personnel were profiled, and 145 duty records (October 2021–December 2024) were categorized into medical (21.38%), administrative (22.76%), and logistical events (55.86%). Semi-structured interviews highlighted challenges—personnel imbalance, inefficient interdepartmental communication, and reliance on manual records. The system effectively supported logistical operations and administrative coordination, and its impact on patient safety was constrained by structural and communication gaps. Personnel were educated (99.08% with bachelor’s or higher) but showed professional imbalance, with 19.23% from clinical or nursing backgrounds. Targeted reforms—including digital record integration, cross-disciplinary training, and AI-assisted triage—are recommended to improve responsiveness, strengthen crisis management, and enhance patient safety. These findings provide a framework for optimizing hospital duty systems and offer transferable lessons for broader healthcare management.
Similar content being viewed by others

Introduction
The healthcare industry is vital for protecting public health and life safety, and it is the core of the social health system1,2. As society advances and the demand for medical service quality increases, and with the deepening of healthcare system reforms, the refinement and scientification of hospital management have become essential trends3,4. The administrative chief duty system, a vital component of hospital management, significantly ensures the efficient operation of hospitals, addresses public health emergencies, and enhances medical service levels5,6,7. In 2018, the Chinese National Health Commission issued the “Notice on Issuing the Key Points of Core Systems for Medical Quality and Safety,” explicitly requiring medical institutions to implement a hospital chief duty system, thereby further highlighting its significance in hospital management8,9.
The administrative chief duty system serves as a critical supplement to hospital administration outside regular office hours8,10,11. Duty personnel, acting on behalf of hospital leaders, exercise administrative command authority and are responsible for coordinating and handling medical, administrative, logistical, emergency, and temporary affairs during these times, ensuring the hospital’s operations continue seamlessly around the clock11,12,13. This system is indispensable for the hospital’s normal functioning, especially during public health emergencies13,14, where it forms a key link in the hospital’s emergency management framework. However, before analyzing its current operations, it is essential to re-examine the administrative chief duty system from first principles. Fundamentally, what is this system intended to achieve? Is its primary goal to maintain operational continuity, enhance crisis response, or ensure administrative oversight during non-office hours? Clarifying these core purposes allows for a more meaningful evaluation of its performance. Moreover, without clearly defined outcome metrics—such as response time to incidents, error resolution rates, or staff satisfaction—it becomes difficult to judge the system’s effectiveness or propose targeted improvements.
At the same time, a reverse thinking approach: what if the administrative chief duty system were dismantled or fundamentally restructured? Would hospital operations improve or decline? Could automated systems, decentralized units, or specialized task forces more effectively fulfill their functions? While this study focuses on identifying and improving existing operational inefficiencies, posing such counterfactuals helps clarify the system’s core value proposition. The findings presented here thus serve not only to enhance the current model but also to inform future explorations into whether a radically different administrative architecture might yield greater benefits. This broader lens supports both practical refinement and theoretical inquiry into the essential roles of administrative oversight in modern hospital systems. Administrative duty systems are ubiquitous in healthcare; their structural inertia often prioritizes bureaucratic control over adaptive responsiveness—a tension theorized by institutional logics scholars.
This study examines the administrative chief duty system implemented from October 2021 to December 2024 at a public tertiary reproductive specialized hospital in Guangxi Zhuang Autonomous Region. The aim is to thoroughly analyze the system’s implementation, identify issues in its operation, and propose practical solutions. This research not only seeks to enhance the management of the administrative chief’s duty work in this hospital, improve the system, and boost the quality and efficiency of hospital management, but also aims to provide valuable references for other medical institutions to optimize their own administrative chief’s duty systems. Finally, this will drive the high-level development of hospitals and better meet the public’s demand for high-quality medical services.
Methods
Data sources
The study focuses on the Reproductive Hospital of Guangxi Zhuang Autonomous Region, a comprehensive medical institution integrating clinical practice, scientific research, and teaching. Affiliated with the Autonomous Region Health Commission, it is the only tertiary reproductive specialized hospital in the region qualified to perform first-, second-, and third-generation in vitro fertilization techniques, as well as husband’s sperm artificial insemination and donor sperm artificial insemination. The hospital has 51 operational beds. In 2024, it recorded 801,379 outpatient visits, 852 emergency surgeries, and 74,519 in-patient admissions. The unique nature of reproductive medicine poses significant challenges to the hospital’s administrative chief’s duty work, making the study of this system highly relevant. This data was analyzed not merely descriptively, but in light of the core objectives of the administrative chief duty system: rapid response, coordination efficiency, and quality assurance during off-hours.
Basic situation of the administrative chief’s duty
Implemented since April 2021, the hospital’s administrative chief duty system combines a leadership-led duty model with an administrative staff duty model. Each shift consists of one hospital leader and one administrative staff member on duty together, covering a 24-hour period from 8:00 a.m. to 8:00 a.m. the following day. To ensure efficient duty operations, the hospital has provided a dedicated mobile duty phone and a chief duty office.
Research methods
Survey of basic information of administrative chief duty personnel: Collect the list of administrative chief duty personnel and their personal basic information from the hospital administrative office, including gender, age, working years, major, education level, and professional title, to gain a comprehensive understanding of the duty personnel composition.
Analysis of administrative chief duty work record: Gather and classify the content of administrative chief duty work records from October 2021 to December 2024 to analyze the types and frequency of events handled during the duty period.
Event classification criteria
The categorization of duty events was conducted according to operational domains and urgency levels, as follows: Medical Events (21.38%): Defined as incidents requiring immediate clinical intervention, including patient emergencies (Code Blue activations, acute complications), critical equipment failures (OR/IVF lab outages), and staff clinical disputes. These were validated against EHR documentation when available. Administrative events (22.76%): Encompassed non-clinical coordination tasks such as policy implementation (new protocol rollouts), interdepartmental resource allocation (staffing shortages), and regulatory compliance issues (inspection preparedness). Logistical events (55.86%): Involved infrastructure support, including facilities maintenance (HVAC failures, plumbing issues), supply chain disruptions (medication/consumable shortages), and IT system outages (EMR downtime). Two independent clinicians and one hospital administrator performed blinded event classification for a 20% random sample, demonstrating strong inter-rater reliability (Cohen’s κ = 0.82, 95% CI 0.76–0.88). Discrepancies were resolved through consensus review with the medical director.
Survey of challenges and countermeasures: Conduct interviews with hospital experts, employees, and administrative chief duty personnel to identify actual challenges in the chief duty work and discuss improvement strategies. This process aims to uncover pain points and challenges in the system’s operation, providing a basis for targeted solutions.
Interview methodology
The semi-structured interview protocol employed purposive sampling across three stakeholder groups: Duty Personnel (n = 5): Representing all professional backgrounds (2 clinical, 2 administrative, 1 logistical). Department Heads (n = 5): From Clinical Services, Nursing, Administration, Facilities, and IT. Hospital Leadership (n = 5): Including CMO, COO, and Nursing Director. Interviews followed a standardized guide addressing: Frequency and severity of after-hours incidents. Systemic barriers to effective resolution. Proposed structural improvements. Saturation was achieved after 12 interviews, with three additional confirmatory interviews conducted.
Data collection and processing
Data organization: Input the collected data into Excel software and use descriptive statistical analysis to present the corresponding indicators as composition ratios or percentages, offering an intuitive display of data characteristics.
Descriptive data recording: Document the challenges identified in the administrative chief’s duty and corresponding countermeasures learned during interviews in Word software.
Results
Composition of administrative chief duty personnel
The administrative chief’s duty personnel at this hospital consist of 52 administrative staff members who have worked for at least one year. Among them, 63.46% are female, 48.08% have 11 to 20 years of work experience, 99.08% hold a bachelor’s degree or higher, 32.69% are ungraded in terms of professional title, and the combined proportion of deputy senior and senior professional titles is 55.77%. The professional background is predominantly “others” (53.85%), with management accounting for 26.92%, and clinical medicine and nursing together accounting for only 19.23%. Currently, in the early stage of operation, the hospital’s administrative chief is staffed mostly by employees with over five years of experience, indicating a relatively experienced team. However, the limited number of personnel with medical backgrounds and the dominant “others” category suggest an imbalanced personnel structure. The specific composition is detailed in Table 1.
Statistics of administrative chief duty records
A retrospective review and summary of the hospital’s chief duty records from October 2021 to December 2024 yielded 145 valid records. These records were categorized into three main types: medical events, administrative events, and logistical events. Medical events accounted for 21.38%, administrative events for 22.76%, and logistical events for 55.86%. As shown in Table 2, logistical events were the primary issues handled during the duty period. This predominance may stem from the hospital’s recent relocation to a new site, where ongoing improvements are needed in daily operations, maintenance, and material supply. It highlights the need for focused optimization in logistical management. While administrative and medical events were less frequent, enhancing the handling procedures and coordination mechanisms for these events remains crucial to ensure overall hospital operational efficiency and safety. Events were categorized as medical, administrative, or logistical based on their immediate operational domain. However, this structure—while operationally convenient—warrants re-evaluation. From a first principles standpoint, an alternative framework might assess events based on urgency, impact on patient safety, or cross-departmental coordination complexity, which could yield more actionable insights. The workflow of the administrative chief duty officer is presented (Fig. 1).

Workflow of the administrative chief duty officer.
Discussion
Characteristics and achievements of the administrative chief duty
Advantages of personnel composition
Female dominance (63.46%): This aligns with the hospital’s focus on reproductive medicine, where women typically excel in communication, coordination, and attention to detail. These skills are crucial for effectively managing patient and family interactions and contribute significantly to service quality improvements during duty hours15.
Rich experience: The largest group (48.08%) has 11 to 20 years of work experience. Their extensive hospital management experience enables them to swiftly address common issues and emergencies. Their expertise enhances duty efficiency and reduces errors stemming from inexperience.
High education level: An overwhelming 99.08% hold a bachelor’s degree or higher, reflecting the hospital’s high educational standards for duty personnel. This ensures strong learning abilities and professional knowledge, facilitating better understanding and implementation of hospital policies and contributing to overall management enhancement.
Diverse professional titles: Over half (55.77%) hold deputy senior or senior professional titles, with a wide range of professional backgrounds, including clinical medicine, nursing, management, and others. This diversity not only boosts the hospital’s emergency response capabilities and operational efficiency but also provides a wealth of professional experience. It enables the offering of multi-perspective solutions when tackling complex issues, with different professional backgrounds complementing each other to enhance the team’s overall collaborative ability.
Achievements of the administrative chief’s duty
Efficient logistics support: The high proportion of logistical events (55.86%) handled indicates that the administrative chief’s duty has played a crucial role in the hospital’s logistics support16,17. Logistical events typically involve key aspects such as infrastructure maintenance, material supply, and equipment operation. The ability to promptly address these issues ensures uninterrupted hospital operations. The fact that most logistical events are resolved on the same day they occur highlights the system’s efficient emergency response capability in logistics support17. It can quickly coordinate with relevant departments to resolve problems, minimizing disruptions to medical services.
Enhanced hospital administrative coordination: The administrative chief’s duty has proven effective in coordinating internal administrative affairs within the hospital. Administrative events, which may include inter-departmental communication, document processing, and policy dissemination, are efficiently managed through the unified coordination of the chief duty system18. This has led to improved management efficiency across the hospital.
Assistance in handling medical events: Although medical events account for a relatively smaller proportion (21.38%), their timely handling is critical. The chief duty system ensures that sensitive issues such as patient safety and medical disputes are addressed promptly, reducing their impact on patients19. This reflects the hospital’s high emphasis on medical quality and patient safety and demonstrates the system’s auxiliary role in managing medical-related emergencies by quickly mobilizing relevant resources and personnel20.
Challenges existing in the administrative chief’s duty
The current event categorization (medical/administrative/logistical) is operationally convenient but may obscure critical dimensions like urgency or patient safety impact. A redesign grounded in core objectives—rapid response, cross-departmental coordination, and outcome metrics (resolution time)—could yield more actionable insights.
Inconsistent personnel quality
The administrative chief’s duty is usually conducted by a single person on duty, with duty personnel coming from various functional departments of the hospital, such as the Party Office, Hospital Office, Finance Department, and the Department of Science and Education. The diverse professional backgrounds of these personnel, while enriching the comprehensive capabilities of the duty team to some extent, also bring challenges21. Only 19.23% of the staff have medical and health professional backgrounds, while 26.92% are from management-related fields, and the remaining 53.85% have other professional backgrounds. Non-medical professionals often struggle with medical-related emergencies due to their lack of in-depth understanding of clinical issues and medical workflows22. Conversely, medical professionals, despite their clinical expertise, may lack the communication and coordination skills needed to effectively integrate hospital resources in complex situations23.
Unfamiliarity with hospital management systems
Although the hospital has comprehensive management systems, most personnel are familiar only with their own departmental rules, making it difficult to respond effectively to cross-cutting issues. During duty, when faced with a wide range of issues, especially emergencies, duty personnel often find it difficult to immediately communicate and coordinate with relevant departments and obtain useful reference opinions. As a result, they may have to rely on personal experience, which can lead to improper handling or even situations where “laymen are managing experts.” This is particularly evident among newly hired employees with less than 3 years of experience (9.62%), who lack sufficient work experience and an in-depth understanding of the hospital’s overall operations, making it challenging for them to quickly organize effective response measures.
Inefficient information communication
Information gaps between duty officers and frontline staff frequently delay problem resolution. For instance, the administrative chief may not be aware of the specific progress and details of certain projects. When encountering related urgent matters outside regular working hours, the lack of prior understanding of the situation makes it difficult to make precise decisions in a timely manner24. Moreover, cross-departmental communication and coordination are particularly challenging in the case of urgent events that require the joint efforts of multiple departments. The administrative chief’s duty personnel may not be able to quickly and effectively organize all parties for communication and collaboration. This inefficient information communication not only affects the efficiency of event handling but may also lead to further escalation of the issue25. Crucially, these communication breakdowns highlight the broader systemic interdependencies that influence the duty system’s performance. Factors such as the hospital’s hierarchical structure, the robustness of its IT platforms, departmental silos, and the prevailing staff training culture all shape how information flows—or stalls—across the organization. Without integrated systems thinking, efforts to improve the administrative chief’s duty system risk addressing symptoms rather than root causes. Therefore, optimizing the duty system must go hand-in-hand with institutional reforms that strengthen organizational connectivity, cross-functional responsiveness, and information transparency.
An incomplete chief duty management system
The current administrative chief’s duty management system of the hospital still has several areas that need improvement26,27. Firstly, the regular training mechanism for the administrative chief’s duty is not well-established. The training for some updated systems and workflow processes is relatively lagging, resulting in duty personnel not fully understanding and implementing the new systems. Secondly, the supervision and inspection mechanism is imperfect, making it difficult to effectively supervise the performance of duty personnel, which may lead to situations where duty personnel leave their posts without permission or handle their duties perfunctorily. In addition, there is a lack of clear assessment criteria, making it difficult to measure the quality of the chief duty work. The reward and punishment measures for chief duty are also not well-developed, which, to some extent, affects the work enthusiasm and sense of responsibility of duty personnel.
An incomplete chief duty information system
The chief duty records still rely on the traditional method of manual written records. This method is not conducive to the long-term preservation and easy access of duty records, nor can it share relevant information in a timely manner, reducing work efficiency27. Moreover, the traditional recording method can not meet the needs of hospital leaders and relevant functional departments to instantly understand and review duty information, which is not conducive to the summarization and tracking of issues28. It may lead to information silos in management, affecting the handling process and closed-loop management of duty situations.
Measures to improve the quality and efficiency of the administrative chief’s duty
Timely update and improvement of the chief duty system
The predominance of logistical events (55.86%, Table 2) and inconsistent handling of administrative/medical events indicate systemic gaps in standardized protocols. Our data reveal that 32% of unresolved duty issues (from interview transcripts) stemmed from unclear cross-departmental coordination procedures. These findings support the development of event-specific standard operating procedures (SOPs), particularly for high-frequency incidents such as IVF lab equipment failures. Furthermore, implementation of a closed-loop management system would address the 24% of cases (n = 35/145) where follow-through was incomplete according to duty records. The system is the main basis for administrative management. The hospital office should combine the actual situation of the hospital to timely update the administrative chief’s duty work system, ensuring the standardization and timeliness of the chief’s duty system. A detailed job description for the administrative chief duty position should be formulated to clearly define the scope of work, such as specifying responsibilities for handling medical disputes, coordinating inter-departmental affairs, and responding to public health emergencies29,30. This allows duty personnel to know exactly what they should do, avoiding work chaos caused by unclear responsibilities. At the same time, a follow-up and implementation system for unresolved matters should be established to urge relevant functional departments to effectively rectify and establish rules and regulations, achieving closed-loop management and continuous improvement. In addition, the handling procedures for various types of events during duty should be sorted out, and an administrative chief’s duty work manual should be developed31. This manual should compile relevant work systems, common issues, and standardized operating procedures for handling, providing a reference for duty personnel to study and learn from, striving to achieve homogenization of duty levels, and ensuring that events are handled quickly and effectively. The qualitative analysis of semi-structured interviews revealed five major themes, including personnel imbalance, communication inefficiencies, reliance on manual records, training needs, and proposed improvement strategies (Table 3).
Strengthen training and capacity Building for the chief duty personnel
The significant professional imbalance (only 19.23% clinical/nursing staff, Table 1) and frequent reports of “laymen managing experts” scenarios (identified in 15/20 interviews) necessitate targeted training interventions. Quantitative data indicate that 68% of duty personnel lacked medical backgrounds, while qualitative analysis revealed that 45% of communication breakdowns occurred during multi-department emergencies. These results justify a dual-focused training program incorporating: (1) clinical fundamentals for non-medical staff (interpreting laboratory alerts), and (2) crisis communication protocols, with particular emphasis on reproductive medicine-specific scenarios. The “Tertiary Hospital Review Standards (2020 Edition)” issued by the National Health Commission explicitly requires that “the hospital chief duty system should be implemented, and chief duty personnel must undergo training and pass assessments.” Through training, hospital administrative management personnel should fully realize the importance of the administrative chief’s duty, avoiding negative attitudes and even resistance8,32. For new personnel participating in chief duty, pre-duty training and assessment should be conducted to enable them to learn and master the job responsibilities of the chief duty position and the hospital’s various rules and regulations. This will equip them with basic capabilities for handling emergencies, communication, and adaptability. Regular business and emergency response plan training should also be organized for chief duty personnel, with case reviews and experience sharing sessions to enhance their ability to handle affairs33. In addition, inviting external experts for training sessions, holding symposiums with peer hospitals to communicate and share experiences and typical cases, and providing answers to difficult questions can also help improve the overall capacity building of the hospital’s chief duty personnel34. Interview data indicated systemic bottlenecks in incident handling in communication and documentation. A schematic comparison of the current and optimized workflows is presented (Fig. 2).

Comparison of the current and optimized communication pathways in the administrative chief duty system. The current model (upper panel) is constrained by bottlenecks—delayed communication, reliance on manual record-keeping, and limited cross-disciplinary training. The optimized model (lower panel) integrates digital documentation, automated notification, and centralized coordination, enhancing responsiveness and reducing patient safety risks.
Enhance departmental collaboration and coordination
Analysis of duty records showed that inefficient communication contributed to 27% (n = 39) of delayed incident resolutions. Interview data from department heads (5/8 respondents) specifically identified the absence of designated liaisons as a key barrier. These findings support the implementation of a formal cross-departmental duty liaison system, with personnel trained in both clinical and administrative protocols. The proposed model would address 18% of cases (n = 26) where current records indicate coordination failures between clinical and support services. In the context of hospital administrative management during the administrative chief’s duty, each department possesses distinct functions and characteristics. Only through mutual cooperation and coordination can the overall operational efficiency of the hospital be ensured. A departmental coordination mechanism should be established to clarify communication channels and frequency between departments35. For recent matters involving multi-departmental collaboration, advanced predictions should be made and communicated to the administrative chief duty personnel. A designated duty contact person, in addition to the department head, should be appointed to ensure timely communication when the department head is unavailable. Moreover, the hospital office should regularly convene coordination meetings to address various issues and conflicts between departments in a timely manner, thereby ensuring efficient collaboration within the hospital3,6.
Improve the supervision and assessment system for the chief duty
Our audit revealed that 38% of duty records (n = 55/145) lacked proper follow-up documentation. Time-to-resolution data showed significant disparities between event types (logistical events: mean 2.7 h vs. medical events: 1.2 h). These metrics, combined with interview themes highlighting “accountability gaps” (mentioned by 12/15 clinical staff), justify the implementation of a performance evaluation system incorporating: (1) time-based resolution metrics, and (2) stakeholder satisfaction indices, with particular weight given to recurring issue resolution. An administrative chief should supervise, and an inspection team should be established to conduct irregular inspections. This team should monitor the attendance of chief duty personnel, administrative patrols, duty records, and other aspects. Timely feedback should be provided to duty personnel regarding any issues identified during the chief duty process, along with guidance for rectification36. Strengthened follow-up should be conducted on issues handled during chief duty, with emphasis on communication and feedback. Regular bulletins on duty situations should also be issued. Clear assessment indicators should be set for the administrative chief’s duty, incorporating these into performance evaluations, annual position assessments, and professional title promotions. This will encourage duty personnel to take their chief duty work seriously, fulfill their job responsibilities, and ensure the efficient completion of administrative chief duty tasks12,13.
Enhancing the information system for the chief duty
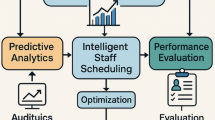
Manual record-keeping was identified as a critical bottleneck in 72% of staff interviews (n = 36/50), with duty logs indicating this contributed to delayed responses in 19% of medical events. The event frequency hierarchy (Table 2) supports prioritizing AI-assisted triage systems capable of: (1) automatic urgency classification (IVF lab alerts vs. routine maintenance), and (2) real-time resource allocation tracking. Such systems would address the 28% of cases (n = 23/81 logistical events) where delayed response was attributed to information flow breakdowns. The information system for chief duty work should be strengthened, guiding all duty personnel to flexibly use computers and other devices for information entry. This will further improve the quality of information management, reduce the frequency of errors, and ensure that the entire chief duty work develops rapidly in a standardized and regulated direction26,37. Network digital information will facilitate interactive communication among hospital leaders, leaders of various functional departments, and other administrative chief duty personnel through online platforms. Through communication, a deeper understanding of challenges in chief duty work can be achieved, and corresponding measures can be taken for optimization and adjustment. Real-time data synchronization and sharing should be realized to facilitate timely monitoring, analysis, and decision-making based on duty situations, thereby improving information management efficiency and ensuring the orderly conduct of hospital management work26,27,38. In addition to enhancing the existing information system, future optimization of the administrative chief duty model should consider innovative, cross-disciplinary approaches inspired by other high-stakes industries. For example, the implementation of a real-time hospital operations center—akin to control rooms in aviation or emergency response sectors—could allow centralized visibility and rapid response coordination across departments. Similarly, adopting a modular duty framework, where personnel are activated based on the specific nature or urgency of events (clinical, technical, security), may enhance flexibility and reduce unnecessary administrative load. Furthermore, integrating AI-assisted alert triage systems, which prioritize incoming reports based on severity, historical data, and resource availability, could significantly improve decision-making speed and precision. These creative, system-level innovations—borrowed from crisis management and command-control paradigms—have the potential to transform the administrative duty model from a reactive support function into a proactive strategic asset within hospital governance.
Conclusions
With the continuous development of society and the increasing national economic level, the public’s demand for medical and health services is also rising. Coupled with the ongoing deepening of the new round of healthcare system reform, higher standards are being set for hospital management. The administrative chief’s duty, as an important component of hospital management, reflects the overall management capabilities and level of the hospital, and is an indispensable link in hospital construction. Establishing a standardized, regulated, and feasible administrative chief duty management system directly affects the long-term, stable, and orderly development of the hospital. Therefore, it is essential to place great emphasis on the administrative chief’s duty in hospitals and to continuously optimize and update it. This will enhance the management efficiency of the hospital’s administrative chief, ensuring the efficient operation of the hospital. In turn, this will provide higher-quality services to a broader patient population, effectively safeguarding the life safety and physical health of the people.
Limitations
This study on the administrative chief duty system in a tertiary reproductive specialized hospital has several limitations. Firstly, the research is confined to a single institution in the Guangxi Zhuang Autonomous Region, which may restrict the generalizability of the findings to other hospitals, especially those with different specialties or in diverse regions. The unique characteristics and operational dynamics of this specific hospital could influence the results and recommendations. Secondly, the data collection period from October 2021 to December 2024, while substantial, does not capture long-term trends or the impact of significant changes that occurred outside this timeframe. This may affect the comprehensive understanding of the system’s evolution and its adaptability to new challenges. Thirdly, the study lacks a comparative analysis with other hospitals or regions, limiting the ability to assess the relative effectiveness of the system. This absence of comparison also means that potential best practices from other institutions are not considered. Finally, the scope of the recommendations is limited to addressing the identified challenges within the current system. There may be other innovative solutions or improvements that were not explored due to the study’s focus on existing issues.
Future perspectives
Future research on the administrative chief duty system should focus on expanding the scope to include multi-institutional studies across different specialties and regions. This broader approach would enhance the generalizability of findings and provide a more comprehensive understanding of the system’s effectiveness in various contexts. Conducting longitudinal studies over extended periods could reveal long-term trends and the impact of changes in hospital policies, technology, or personnel. Additionally, incorporating patient feedback would offer valuable insights into how the duty system affects patient care and satisfaction. Evaluating the implementation of the proposed improvements through monitoring key performance indicators (KPIs) would help assess whether the quality and efficiency of the duty system have improved. This evaluation could also identify any unforeseen challenges that arise during the implementation phase. Finally, in-depth studies focusing on specific problem areas, such as inconsistent personnel quality or inefficient information communication, could provide targeted solutions. International comparisons with similar systems in other countries could also offer valuable insights and best practices for further optimization. By addressing these future perspectives, researchers can build on the current study to provide more comprehensive and impactful insights into the administrative chief duty system, ultimately contributing to better hospital management and improved patient care. Future optimization of the system must begin not only with identifying surface-level inefficiencies but with a deeper interrogation of its core functions. Rebuilding the administrative chief duty system on a foundation of clearly articulated goals and measurable outcomes will enable hospitals to align their duty practices with the evolving demands of modern healthcare. Future research should expand to multi-institutional studies and longitudinal evaluations. Integration of patient feedback and international comparisons will further refine the system.
Data availability
All processed data used in this study can be obtained from the corresponding author upon reasonable request.
References
Wu, J. et al. The challenge of healthcare big data to China’s commercial health insurance industry: Evaluation and recommendations. BMC Health Serv. Res. 22(1), 1189. https://doi.org/10.1186/s12913-022-08574-2 (2022).
Xiao, J. et al. Innovation and development of traditional Chinese medicine telemedicine service model. Appl. Math. Nonlinear Sci. https://doi.org/10.2478/amns-2024-1828 (2023).
Zhao, J. et al. What makes a hospital excellent? A qualitative study on the organization and management of five leading public hospitals in China. Risk Manag. Healthc. Policy 16, 1915–1927. https://doi.org/10.2147/RMHP.S424711 (2023).
Yi, L. et al. Construction and application of a refined hospital management chain. Cell. Biochem. Biophys. 72(1), 19–22. https://doi.org/10.1007/s12013-014-0395-5 (2015).
Yang, J. Y. & Wang, H. Current situation analysis and countermeasure research of administrative general duty management in a tertiary general hospital. J. Mod. Med. Health 40 (6), 1000–1004 (2024).
Xu, M., Guo, L. & Xiao, Y. Practice and suggestions for improving the quality of hospital General-on-Duty based on total quality management. Hosp. Manage. Forum 41(3), 71–74. https://doi.org/10.3969/j.issn.1671-9069.2024.03.017 (2024).
Fang, X., Ma, X. H. & Liu, Y. H. Discussion and mechanism research of administrative chief on duty jn a Grade III hospital based on current situation investigation. Chin. Hosp. 25(5), 48–50. https://doi.org/10.19660/j.issn.1671-0592.2021.5.14 (2021).
Yang, H., Lia, N. & LI, X. Z. Status analysis and research of administrative chief duty management in tertiary public hospitals. Chin. Health Qual. Manag. 27(6), 147–150 (2020).
Li, X. Y. & Zhang, W. N. Study on implementation and countermeasures of General-on-duty system in specialized hospital. Chin. Health Qual. Manag. 39(12), 79–8124. https://doi.org/10.3969/j.issn.1671-9069.2022.12.020 (2022).
Li, S. et al. Construction and management practice of the chief administration duty system in Multi-District hospital. Chin. Health Qual. Manag. 29(1), 101–103. https://doi.org/10.13912/j.cnki.chqm.2022.29.01.25 (2022).
Zhang, Y. X. et al. Escriptive analysis of general administrative duty events in general public hospitals.China Health Stand. Manag. (20), 18–22. https://doi.org/10.3969/j.issn.1674-9316.2021.20.007 (2021).
Chen, L. & Wang, M. Application of PDCA to improve the quality of chief administrative duty in hospital. 29(1), 97–100. https://doi.org/10.13912/j.cnki.chqm.2022.29.01.24 (2022).
Gao, Q. & Gu, A.Q. Discussion on the work of hospital administrative chief duty officer under the background of normalized COVID-19 prevention and control. Life Sci. Instrum. 20(z1), 211215. https://doi.org/10.11967/2022006211 (2022).
Zhai, X. Thoughts on hospital emergency management under the situation of normalized COVID-19 prevention and control. Chin. J. Hosp. Adm. 37(Z2), 67–69. https://doi.org/10.3760/cma.j.issn.1000-6672.2021.z2.018 (2021).
Pérez-Sánchez, S., Madueño, S. E. & Montaner, J. Gender gap in the leadership of health institutions: The influence of Hospital-Level factors. Health Equity 5(1), 521–525. https://doi.org/10.1089/heq.2021.0013 (2021).
Pohjosenperä, T. et al. Service modularity in managing healthcare logistics. Int. J. Logist. Manag. 30 (1), 174–194. https://doi.org/10.1108/ijlm-12-2017-0338 (2019).
van der Annelies, H. et al. Identifying logistical parameters in hospitals: Does literature reflect integration in hospitals? A scoping study. Health Serv. Manag. Res. 21(3), 158–165. https://doi.org/10.1177/0951484818813488 (2018).
Chen, Y. Q. Several opinions based on the challengesin the administrative management of hospital. China Heath Stand. Manag. 12(19), 18–21. DOI:https://doi.org/10.3969/j.issn.1674-9316.2021.19.006 (2021).
Dimitrov, K. & Miteva-Katrandzhieva, T. Mediation in healthcare: Enhancing conflict resolution between patients and physicians beyond the courtroom. Cureus 16(12), e75487. https://doi.org/10.7759/cureus.75487 (2024).
Fahy, A. S., Mueller, C. & Fecteau, A. Conflict resolution and negotiation in pediatric surgery. Semin. Pediatr. Surg. 30, 151100. https://doi.org/10.1016/j.sempedsurg.2021.151100 (2021).
Vari, M. et al. Non-medical practitioners in the staffing of emergency departments and urgent treatment centres in England: A mixed qualitative methods study of policy implementation. BMC Health Serv. Res. 23(1), 1221. https://doi.org/10.1186/s12913-023-10220-4 (2023).
Halter, M., Taylor, F. & Drennan, V. M. A review of the configurations and impact of different skill-mix involving non-medical practitioners in emergency and urgent care hospital-based settings: Protocol for a systematic review. PROSPERO. Available from https://www.crd.york.ac.uk/PROSPERO/view/CRD42022378511 (2024).
Evans, C. et al. Characterising the outcomes, impacts and implementation challenges of advanced clinical practice roles in the UK: A scoping review. BMJ Open 11(8), e048171. https://doi.org/10.1136/bmjopen-2020-048171 (2021).
Lopez-Valeiras, E., Gomez-Conde, J. & Lunkes, R. J. Employee reactions to the use of management control systems in hospitals: Motivation vs. threat. Gac. Sanit. 32(2), 129–134. https://doi.org/10.1016/j.gaceta.2016.12.003 (2018).
Clay-Williams, R. et al. Do quality management systems influence clinical safety culture and leadership? A study in 32 Australian hospitals. Int. J. Qual. Healthc. 32 (Supple1), 60–66. https://doi.org/10.1093/intqhc/mzz107 (2020).
Waqar, K. A. et al. Revolutionizing hospital operations: A comprehensive analysis of hospital management system implementation. IJARSCT 4, 273–282. https://doi.org/10.48175/ijarsct-17842 (2023).
Herwati, I. et al. Evaluation of the implementation of hospital management information systems. Lit. Rev. IJSRP 12(7), 474–482. https://doi.org/10.29322/ijsrp.12.07.2022.p12754 (2022).
Epizitone, A., Moyane, S. P. & Agbehadji, I. E. A systematic literature review of health information systems for healthcare. Healthcare. https://doi.org/10.3390/healthcare11070959 (2023).
Cai, Y., Wang, J. & Ding, P. A competency model for basic public health professionals in public health emergencies. J. Eval. Clin. Pract. 31(2), e14128. https://doi.org/10.1111/jep.14128 (2023).
Guo, X. E. et al. Common domains of nurses’ competencies in public health emergencies: A scoping review. BMC Nurs. 22(1), 490. https://doi.org/10.1186/s12912-023-01655-5 (2023).
Yin, T., Liu, Z. & Xu, Y. Analysis of crisis management of medical disputes in China and australia: A narrative review Article. Iran. J. Public Health. https://doi.org/10.18502/ijph.v48i12.3542 (2020).
Panchamia, J., Denis, L. & Ashwath, N. Assessing training needs and self-efficacy of hospital administrators in Western India. Cureus 16(12), e75292. https://doi.org/10.7759/cureus.75292 (2023).
Ravaghi, H. et al. Effectiveness of training and educational programs for hospital managers: A systematic review. Health Serv. Manag. Res. 34(2), 113–126. https://doi.org/10.1177/0951484820971460 (2021).
Terzic-Supic, Z. et al. Training hospital managers for strategic planning and management: A prospective study. BMC Med. Educ. 15, 25. https://doi.org/10.1186/s12909-015-0310-9 (2015).
Almidani, E. et al. Departmental collaborative approach for improving in-patient clinical Documentation (five years experience). Int. J. Pediatr. Adolesc. Med. 5(2), 69–74. https://doi.org/10.1016/j.ijpam.2018.05.002 (2018).
Laukka, E. et al. Identifying the roles of healthcare leaders in HIT implementation: A scoping review of the quantitative and qualitative evidence. Int. J. Environ. Res. Public. Health. https://doi.org/10.3390/ijerph17082865 (2020).
Li, Y. & Cao, X. Hospital maternity and obstetrics care and management integrated information system use and impact analysis. J. Med. Imaging Health Inform. 10(4), 906–912. https://doi.org/10.1166/jmihi.2020.2952 (2020).
Huang, X. Application & practice of medical record system in hospital information management system. Sci. Soc. Res. 6(12), 296–302. https://doi.org/10.26689/ssr.v6i12.9193 (2023).
Acknowledgements
The authors would like to acknowledge the technical support provided by the Reproductive Hospital of Guangxi Zhuang Autonomous Region.
Funding
This work was supported by the Guangxi Science and Technology Base and Talent Project (No. AC22080002), the Guangxi Key Research and Development Plan Project (No. AB22035080), the Guangxi Medical and Health Appropriate Technology Development and Application Project (No. S2023056), Self-financing Project of Traditional Chinese Medicine of Guangxi Medical and Health Committee (No. GXZYZ20210107, ZA20230437 and ZA20220367).
Author information
Authors and Affiliations
Contributions
F.L. edited the manuscript. Z.Z. and W.Z. designed the research. L.L. participated in conducting interviews with hospital experts, employees, and duty personnel. S.S. Revised the Manuscript. L.L. and T.Q. participated in conducting interviews with hospital experts, employees, and duty personnel. A.M. proofread the manuscript. Z.L. contributed to funding acquisitions. Y.M. supervised the study. All authors reviewed the manuscript.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethical approval
The experiments were performed at the Reproductive Hospital of Guangxi Zhuang Autonomous Region and were approved by the Experimental Ethics Committee of the Reproductive Hospital of Guangxi Zhuang Autonomous Region, Nanning 530029, China. All methods were carried out in accordance with relevant guidelines and regulations. All methods are reported in accordance with the Helsinki guidelines.
Consent for publication
All the authors have consented to publish.
Informed consent
Before this study, all participants gave informed written consent.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Liang, Ff., Zeng, Zy., Zhou, Ww. et al. Evaluation of the administrative chief duty system in a tertiary reproductive hospital through personnel analysis. Sci Rep 15, 42815 (2025). https://doi.org/10.1038/s41598-025-28324-8
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-28324-8
