
Abstract
Peripheral artery disease (PAD) with hyperlipidemia adds significantly to the national burden of cardiovascular disease. However, population-level trends in mortality for these conditions are not well understood. We used nationally representative data to investigate long-term temporal patterns and disparities in PAD and hyperlipidemia related mortality in the United States. This descriptive analysis analyzed death records from the CDC WONDER database from 1999 to 2024. The age-adjusted mortality rates (AAMRs) per 100,000 people were calculated for each demographic and geographic strata. AAMRs were standardized to 2000 U.S. standard population. Temporal trends in AAMRs were analyzed using Joinpoint regression to estimate the average annual percent change (AAPC) with 95% confidence intervals (CIs) and p value. Between 1999 and 2024, a total of 148,416 PAD with hyperlipidemia–related deaths were recorded among U.S. adults ≥ 25 years. The national AAMR rose from 0.74 in 1999 to 3.92 in 2024, corresponding to an overall AAPC of 6.32. Both sexes experienced increasing mortality, though men had higher rates and faster growth compared with women. By race/ethnicity, AAMRs increased across all groups, with the steepest relative rise among Hispanic individuals, followed by Non-Hispanic (NH) Black, NH White, and NH Asian or Pacific Islander populations. Geographic disparities were observed, with state-level AAMRs ranging from 0.92 in Georgia to 5.06 in Vermont, and the highest regional mean AAMR in the West (2.93). Finally, rural areas consistently exhibited higher mean AAMRs than urban areas, with slightly steeper increase over time. AAMRs related to PAD and hyperlipidemia have increased more than fivefold, with disproportionately higher rates among men, Hispanic populations, residents of Western regions, and those in rural areas. These patterns suggest widening disparities in vascular health and underscore the need for strengthened preventive efforts, improved lipid management, and more equitable access to cardiovascular care.
Similar content being viewed by others
Introduction
Peripheral artery disease (PAD) can be defined as a condition that develops when atherosclerosis, or plaque accumulation, occurs in peripheral arteries, which carry blood away from the heart and toward the peripheral regions of the body, narrowing them and limiting blood flow to the limbs and other parts of the body1. PAD affects approximately 200 million people globally and is frequently asymptomatic or misattributed to musculoskeletal causes, delaying detection and treatment2. In contrast, hyperlipidemia refers to a variety of conditions associated with elevated lipid levels in the bloodstream3. Approximately 25 million adults in the United States have total cholesterol levels over 240 mg/dL, which places them in the hyperlipidemic range4. Lower extremity PAD is the third most common cause of atherosclerotic cardiovascular events, following coronary artery disease and stroke4. Despite statin availability, guideline-concordant lipid management in PAD remains suboptimal in practice, with undertreatment linked to higher limb events and mortality5.
High cholesterol is a major contributor to peripheral artery disease6. LDL-C and other lipid abnormalities—such as high triglycerides, low HDL-C, elevated apolipoprotein B, and lipoprotein(a)—are linked to PAD and adverse limb outcomes, independent of traditional risks7,8,9. Dyslipidemia, diabetes, obesity, genetic hypercholesterolemia, and physical inactivity further contribute to PAD9. Conversely, healthy lifestyle practices and appropriate medical management can help prevent its onset10,11.
This study utilizes CDC Wonder database, which provides nationwide, standardized publicly available mortality data, making it ideal for evaluation of population-level mortality trends associated with PAD and hyperlipidemia. Additionally, this study emphasizes mortality trends derived from death certificates to capture population-level burden rather than clinical incidence. While individual effects of PAD and hyperlipidemia on patient outcomes are well-documented, there is still a considerable lack of literature examining their combined impact on mortality trends. Leveraging data from the CDC WONDER database (1999–2024), this analysis examines mortality trends among individuals with PAD and hyperlipidemia. We believe that this grouping represents a particularly high-risk phenotype, influenced by shared atherogenic processes and inconsistent adherence to lipid-lowering treatments. These findings may help with early detection, guideline-directed treatment, and policy actions aimed at lowering excess cardiovascular and limb mortality.
Methods
Study design and data source
This present study leveraged database of Centers for Disease Control and Prevention’s Wide-ranging Online Data for Epidemiologic Research (CDC WONDER)12 database, covering the time period from 1999 to 2024. The data were derived from U.S. death certificates as part of the Multiple Cause-of-Death Public Use data set, which include information from all 50 states and the District of Columbia. The database has been extensively used in prior epidemiologic studies for analyzing nationwide mortality trends.
Study population
Mortality data were obtained using International Classification of Diseases, 10th Revision (ICD-10) codes. Death certificates listing PAD as either the underlying or as a contributing cause of death were identified with ICD-10 codes (E10.5, E11.5, E12.5, E13.5, E14.5, I70.0–I70.2, I70.8–I70.9, I71.1–I71.6, I71.8–I71.9, I72.1–I72.4, I72.8–I72.9, I73.8–I73.9, I74.0, I74.1–I74.5, I74.8–I74.9, and I77.8–I77.9) in patients ≥ 25 years of age13. The code E78 refers to hyperlipidemia14. Mortality events were considered if the condition of interest appeared anywhere on the death certificate, whether as a primary or contributing cause of death.
Data abstraction
Variables collected included year of death, demographic characteristics (sex, race/ethnicity), location of death, geographic region, state, and urban–rural classification. Place of death was categorized into medical facilities (including outpatient, emergency room, inpatient, death on arrival, or status unknown), home, hospice, and long-term care facilities. Race/ethnicity were categorized as NH White, NH Black, Hispanic, and NH Asian or Pacific Islander. Urban–rural grouping was determined using the National Center for Health Statistics Urban–Rural Classification Scheme based on 2013 U.S. Census data15. Geographic regions were designated in accordance with the U.S. Census Bureau’s regional designations (Northeast, Midwest, South, and West).
Statistical analysis
We calculated Age-adjusted mortality rates (AAMRs) per 100,000 population by year, sex, race/ethnicity, state, and urban–rural status, along with 95% confidence intervals (CIs). National temporal patterns in AAMRs were assessed using the Joinpoint Regression Program version 5.4.0, National Cancer Institute16, which identifies statistically significant changes in trends over time using log-linear models. Annual percent change (APC) and corresponding 95% CIs were reported. The APC measures the yearly rate of change in mortality within a given period, while the AAPC summarizes these changes to show overall long-term trend by providing a weighted average across multiple time segments. These indicators are integral to population-level analyses using CDC WONDER mortality data, as they account for non-linear trends over time and quantify the change in patterns over time. Statistical significance defined as a two-tailed P-value < 0.05.
Results
Between 1999 and 2024, PAD with hyperlipidemia accounted for a total of 148,416 deaths among adults aged 25 years and more in the United States (Supplemental Table 1). These deaths were prevalent across various different places, with the leading most occurring in decedent’s homes [38.2%], followed by medical facilities [34.6%], [19.7%] in the nursing home/ long term care facilities, [3.1%] in hospice facilities, and [4.2%] at other locations (Supplemental Table 2).
Annual trends for peripheral artery disease with hyperlipidemia-related AAMR
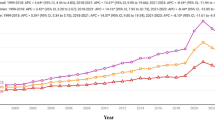
The overall AAMR for peripheral artery disease with hyperlipidemia-related deaths among adults increased from 0.74 (95% CI: 0.70–0.79) in 1999 to 3.92 (95% CI: 3.85–4.00) in 2024, with an AAPC of 6.32 (95% CI: 5.65–7.00; p value < 0.001) (Table 1) (Fig. 1) (Supplemental Table 3).

Peripheral artery disease with hyperlipidemia AAMR stratified by sex and overall, per 100,000 population.
Peripheral Artery Disease with Hyperlipidemia-Related AAMR Stratified by Sex
AAMR for both men and women increased from 1999 to 2024. Among men, the AAMR increased from 0.90 (95% CI: 0.83 to 0.98) in 1999 to 4.93 (95% CI: 4.8–5.06) in 2024. Similarly, among women, the AAMR increased from 0.66 (95% CI: 0.61–0.71) in 1999 to 3.13 (95% CI: 3.04–3.22) in 2024.
Over the span of the study period, adult men exhibited slightly higher mean AAMRs compared to adult women (mean AAMR for men: 3.11, 95% CI: 2.99–3.22; for women: 1.89, 95% CI: 1.82–1.97). On average, the AAMR of both men and women increased from 1999 to 2024, with men exhibiting a significantly greater magnitude of increment than women [men: AAPC 6.40 (95% CI: 5.72–7.29; p < 0.001); women: AAPC 4.89 (95% CI: 4.39–5.69; p < 0.001)] (Table 1) (Fig. 1) (Supplemental Table 3).
Peripheral artery disease with hyperlipidemia-related AAMR stratified by race/ethnicity
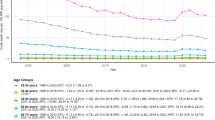
The AAMR increased across all racial/ethnic groups from 1999 to 2024: Hispanic (0.65–3.75); NH Asian or Pacific Islander (0.51–2.28); NH White (0.75–4.02); and NH Black (0.76–4.58).
The highest mean AAMRs were recorded among NH Blacks with only slight differences different among remaining racial/ethnic groups which included NH Whites, Hispanic, and NH Asian or Pacific Islander (mean AAMR: NH Black: 2.64, 95% CI: 2.41–2.86; NH White: 2.47, 95% CI: 2.39–2.54; Hispanic: 2.09, 95% CI: 1.87–2.32; NH Asian or Pacific Islander: 1.53, 95% CI: 1.27–1.82).
The AAMR trend of all the races increased from 1999 till 2024 [Hispanic: AAPC: 7.12, (95% CI: 5.92 to 8.52; p value < 0.001); NH Black: AAPC: 6.82, (95% CI: 6.20–7.67; p value < 0.001); NH White: AAPC: 6.34, (95% CI: 5.68 to 6.90; p value < 0.001); NH Asian or Pacific Islander: AAPC: 3.93, (95% Cl: 3.38 to 4.77; p value < 0.001) (Table 1) (Fig. 2) (Supplemental Table 4).

Peripheral artery disease with hyperlipidemia AAMR stratified by race per 100,000 population.
Peripheral artery disease with hyperlipidemia-related AAMR stratified by geographical regions
Stratified by census region
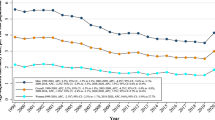
The AAMR increased across all census regions from 1999 to 2024. In the Northeast, the AAMR increased from 0.62 in 1999 to 3.35 in 2024; in the Midwest, from 0.80 to 3.58; in the South, from 0.80 to 4.08; and in the West, from 0.79 to 4.51.
The highest mean AAMRs were observed in the West (mean AAMR: 2.93; 95% CI: 2.78–3.08), followed by the Midwest (mean AAMR: 2.61; 95% CI: 2.47–2.75), South (mean AAMR: 2.27; 95% CI: 2.16–2.37) and Northeast regions (mean AAMR: 1.93; 95% CI: 1.80–2.06).
The AAMR trend of all the regions increased steadily between 1999 and 2024 [West: AAPC: 6.62, (95% CI: 5.35–8.65; p value < 0.001); Northeast: AAPC: 6.50, (95% CI: 5.78–7.62; p value < 0.001); South: AAPC: 5.67, (95% CI: 5.23–6.32; p value < 0.001); Midwest: AAPC: 5.45, (95% CI: 4.61–6.45; p value < 0.001) (Table 1) (Fig. 3) (Supplemental Table 5).

Peripheral artery disease with hyperlipidemia AAMR stratified by census per 100,000 population.
Stratified by urbanization
The AAMR exhibited rise in both urban and rural areas from 1999 to 2020. In urban areas, the AAMR increased from 0.73 in 1999 to 3.44 in 2020, while in rural areas it increased from 0.82 to 3.99.
Rural areas showed slightly higher mean AAMRs throughout the study period, with a mean AAMR of 2.41 for Rural (95% CI: 2.26–2.56) and 2.12 for Urban (95% CI: 2.06–2.19).
The AAMR trend of both rural and urban areas increased from 1999 to 2020 with the increase more pronounced in rural areas [(Rural: AAPC: 7.07, (95% CI: 6.35–8.12; p value < 0.001) (Urban: AAPC: 6.90, (95% CI: 6.06–7.64; p value < 0.001)] (Table 1) (Fig. 4) (Supplemental Table 6).

Peripheral artery disease with hyperlipidemia AAMR stratified by urbanization per 100,000 population.
Stratified by states
Disparities in AAMRs were manifested among different states, with AAMRs ranging from as low as 0.92 (95% CI: 0.86–0.97) in Georgia to 5.06 (95% CI: 4.63–5.49) in Vermont. States falling within the top 90th percentile included Vermont, Ohio, North Dakota, West Virginia, and California which had approximately twice higher AAMRs compared to states in the lower 10th percentile which included Georgia, Arkansas, Massachusetts, Mississippi, and Utah (Fig. 5) (Supplemental Table 7).

Peripheral artery disease with hyperlipidemia AAMr stratified by state per 100,000 population.
Discussion
The nationwide analysis of PAD with hyperlipidemia among U.S. adults over 25, based on CDC WONDER data, revealed dynamic trends and marked fluctuations in mortality. Overall mortality varied notably across the study period, with significant geographic and demographic disparities. Most deaths occurred at home, followed by medical or long-term care facilities. Men consistently showed higher mortality than women, while NH Blacks and residents of the Western region had greater mortality burdens (Fig. 6). States such as Vermont, Ohio, North Dakota, West Virginia, and California showed higher mortality compared with Georgia, Arkansas, Massachusetts, Mississippi, and Utah, highlighting pronounced geographic inequality. Rural populations also experienced slightly higher mortality, reflecting ongoing disparities in health care access and emphasizing the need for targeted interventions to reduce this burden.

Central illustration.
PAD is a progressive narrowing or blockage of peripheral vessels by atherosclerotic plaques, resulting in reduced blood flow, intermittent claudication, poor wound healing, and, in severe cases, critical limb ischemia17. Hyperlipidemia may promote plaque formation through endothelial injury and cholesterol deposition18. Additionally, patients with PAD have a higher risk of future cardiovascular complications19; therefore, controlling risk factors such as hyperlipidemia, smoking, and diet is crucial for prevention and disease management19,20. Many deaths among patients with PAD and hyperlipidemia occurred at home, suggesting late-stage complications, diagnostic challenges21, or a preference for home care22. Deaths in medical facilities, nursing homes, and hospices indicate that PAD is often not recognized as a terminal illness unless severe. These findings highlight the need for early diagnosis, better disease management, and improved access to supportive care.
Peripheral artery disease with hyperlipidemia is a common cause of death worldwide23,24. In our study, overall mortality rates significantly increased throughout the study period, showing notable fluctuations driven by multiple interacting factors. Early in the observation period, a sharp rise between 1999 and 2001 was likely influenced by the growing prevalence of cardiovascular risk factors such as obesity, diabetes, and hyperlipidemia, as well as limited awareness and diagnostic capacity for PAD and lipid disorders25,26,27. However, this rapid increase may also reflect improvements in diagnostic accuracy, reporting practices, and data collection during that time. Over the following years, modest progress in cardiovascular risk management through expanded use of antihypertensive drugs, smoking cessation efforts, and better primary care screening appeared to stabilize mortality trends between 2006 and 201828,29,30,31. Later, from 2018 to 2021, mortality spiked again, likely reflecting the combined effects of an aging population with accumulated vascular burden32, rising obesity prevalence33, persistent disparities in healthcare access, and the added burden of the COVID-19 pandemic34. More recently, mortality plateaued after 2021, possibly due to improvements in clinical recognition of PAD, the implementation of national public health strategies35, and updated cardiovascular health guidelines36.
Men consistently showed higher mortality rates compared to women. The higher mortality among men can be explained by the increased prevalence of comorbidities, including diabetes, hypertension, and hyperlipidemia, as well as a higher prevalence of smoking and greater exposure to occupational and behavioral cardiovascular risks37,38,39,40,41, all of which can accelerate PAD progression. Moreover, men tend to develop atherosclerotic plaques earlier in life, making them more vulnerable to chronic vascular disease and the subsequent development of PAD42. In contrast, premenopausal women have higher estrogen levels, which exert a protective effect against chronic vascular diseases and atherosclerotic plaque formation43. Despite higher absolute mortality rates among men, women have shown greater increases in mortality in recent years, possibly due to an aging population, rising obesity rates, and decreased physical activity44,45. These sex-based differences in mortality underscore the need for sex-specific, multidimensional approaches and public health strategies to reduce the mortality burden in vulnerable groups.
Significant differences in mortality rates were observed among different ethnic and racial groups, with the highest mortality seen among NH Blacks, followed by NH Whites and other groups. This disparity may be explained by the higher prevalence of smoking, hyperlipidemia, and related complications among NH Whites compared to other racial groups46,47. Additionally, NH Whites have an older population, making them more vulnerable, as PAD and hyperlipidemia are chronic conditions whose incidence increases with age48. Moreover, NH Blacks, Hispanics, and other racial groups often have less access to health care and lower rates of disease documentation compared to NH Whites, which could also contribute to the higher recorded mortality in Whites49,50. These findings underscore the need for large-scale public health measures, improvements in the health care system, and enhanced disease documentation, particularly among disproportionately affected populations.
Substantial geographical heterogeneity is evident in the mortality trends of PAD with hyperlipidemia. The persistent rise mortality from PAD associated with hyperlipidemia across all U.S. regions from 1999 to 2024 highlights the complex interplay of risk factor prevalence, healthcare access, and demographic changes. The sharp increases in the early 2000s, most pronounced in the West and Northeast, likely reflect the rising rates of obesity, diabetes, and uncontrolled dyslipidemia during this period, which accelerated peripheral vascular damage51. The stabilization observed in the Midwest and South may be partly attributable to increased statin and antihypertensive use, alongside national initiatives promoting cardiovascular risk reduction, nationwide data support these trends, suggesting that other regions, including the Northeast and West, may similarly benefit; however, region-specific data on statin utilization are not available52,53,54,55,56. Further investigation is warranted to elucidate the impact of these interventions across different regions. However, the rise in mortality after 2017 indicates persistent regional disparities in healthcare access and preventive care delivery, particularly in the South, where obesity and smoking remain highly prevalent57,58,59,60. The upward trend in mortality from PAD associated with hyperlipidemia highlights significant public health challenges across both rural and urban populations. Rural communities consistently exhibited slightly higher AAMRs, reflecting enduring disparities in access to preventive healthcare and a greater burden of cardiovascular risk factors61,62. The initial rapid increase may reflect the growing prevalence of metabolic risk factors, while the subsequent period of stabilization likely corresponds to improvements in population-level interventions such as statin use, lifestyle modification programs, and blood pressure control53,54,55. Nevertheless, the recent increase in mortality underscores persistent gaps in risk management and preventive care delivery61. Despite being neighboring states, Massachusetts had one of the lowest AAMRs, whereas Rhode Island’s rate was comparatively higher. Such discrepancies may stem from differences in population size, socioeconomic characteristics, healthcare access, and the prevalence of cardiovascular risk factors. Variability in data reporting practices across states may also contribute. Moreover, Massachusetts’ long-standing public health initiatives, preventive screening programs, and widespread statin use may help explain its relatively lower mortality burden63.
Overall, the disproportionate rise in PAD with hyperlipidemia-related mortality between 2018 and 2021 coincided with the COVID-19 pandemic. Limited access to vascular care, including delays in routine surveillance, elective interventions, and timely revascularization, likely contributed to disease progression and more advanced ischemic presentations64. Additionally, SARS-CoV-2 infection has been associated with endothelial dysfunction, systemic inflammation, and a prothrombotic state, all of which can accelerate atherosclerotic progression and precipitate acute ischemic events65,66. These observations align with prior studies reporting worse outcomes in PAD patients treated during the pandemic compared to pre-pandemic cohorts67. Beyond the acute effects described previously, SARS-CoV-2 may exert synergistic vascular damage in patients with hyperlipidemia and PAD by sustaining low-grade endothelial inflammation and impairing vascular repair mechanisms, thereby accelerating atherosclerotic plaque progression68. Furthermore, the disruptions in outpatient follow-up, preventive care, and medication management during COVID-19 lockdowns further reduced adherence to lipid-lowering and antiplatelet therapies, predisposing patients to worsening atherosclerotic burden69.Together, these findings highlighted the need for timely intervention and extended follow-ups for PAD patients, particularly during global health crises, to mitigate the compounded risk imposed by both disease progression and pandemic-related limitations in care.
The future management of PAD in hyperlipidemic populations requires a systems-based approach that combines therapeutic innovation with structural reforms. Next-generation lipid-lowering therapies such as PCSK9 inhibitors and bempedoic acid represent important pharmaceutical advances for aggressive lipid control70,71. Incorporating dual antithrombotic therapy into standard protocols has the potential to reduce rehospitalizations and health care costs72. Regenerative medicines, including nanoparticles and gene editing represent a frontier for vascular repair73,74. Finally, embedding early diagnosis and medical management into health systems will be critical to maximizing the global reach of both digital and pharmacological innovations75,76.
Limitations
This study is subject to several limitations. First, because of the dependence on ICD codes and death certificates, there is a risk of misclassification or omission of PAD with hyperlipidemia as a cause of death. Second, reliance on specific coding and documentation may lead to underreporting or missed cases of PAD with hyperlipidemia. Third, the increased use of electronic health records for diagnosing PAD may lead to potential overestimation of PAD–hyperlipidemia co-listing on death certificates, potentially skewing the perception of PAD-related mortality trends. Fourth, certain variables, such as patients’ socioeconomic status, were not evaluated due to the unavailability of relevant data. Fifth, certain variables, such as patients’ socioeconomic status, laboratory data, clinical findings, treatment histories, and disease-specific characteristics (e.g., ankle-brachial index, vascular imaging, lipid profile, or genetic data), were unavailable, limiting the depth of analysis. Sixth, co-morbid conditions, including diabetes, hypertension, coronary artery disease, end-stage renal disease, heart failure, and treatment variables may confound mortality trends. Seventh, urbanization data were not available after 2020, restricting stratified analyses beyond that year. Finally, the database lacks information on disease-specific characteristics necessary to further define PAD with hyperlipidemia, such as ankle-brachial index, vascular imaging findings, lipid panel results, or genetic testing data.
Data availability
The data supporting the findings of this study were obtained from the CDC WONDER online database (Centers for Disease Control and Prevention Wide-ranging Online Data for Epidemiologic Research). The datasets used and analyzed during the current study are publicly available and can be accessed at [CDC WONDER] (https://wonder.cdc.gov).
References
National Heart, Lung, and Blood Institute. What Is Peripheral Artery Disease? [Internet]. Bethesda (MD): National Institutes of Health; [cited 2025 Oct 24]. Available from: https://www.nhlbi.nih.gov/health/peripheral-artery-disease (2022).
Mandaglio-Collados, D., Marin, F. & Rivera-Caravaca, J. M. Peripheral artery disease: update on etiology, pathophysiology, diagnosis and treatment. Med. Clin. (Barc). 161(8), 344–350 (2023).
Hill, M. F., Bordoni, B. Hyperlipidemia. In StatPearls [Internet] (StatPearls Publishing, Treasure Island (FL), 2025); [cited 2025 Aug 15]. Available from: http://www.ncbi.nlm.nih.gov/books/NBK559182/
Qiu, X. et al. Global, regional, and national trends in peripheral arterial disease among older adults: Findings from the Global Burden of Disease Study 2021. Aging Clin. Exp. Res. [Internet] 37(1), 150. https://doi.org/10.1007/s40520-025-03037-0 (2025).
Dopheide, J. F., Papac, L., Schindewolf, M., Baumgartner, I. & Drexel, H. Poor attainment of lipid targets in patients with symptomatic peripheral artery disease. J. Clin. Lipidol. 12(3), 711–717 (2018).
Centers for Disease Control and Prevention (CDC). High cholesterol facts. In CDC – Cholesterol: data & research [Internet] (CDC, Atlanta (GA), 2024); [cited 2025 Aug 23]. Available from: https://www.cdc.gov/cholesterol/data-research/facts-stats/index.html.
Joosten, M. M. et al. Associations between conventional cardiovascular risk factors and risk of peripheral artery disease in men. JAMA [Internet] 308(16), 1660. https://doi.org/10.1001/jama.2012.13415 (2012).
Jansen-Chaparro, S. et al. Statins and peripheral arterial disease: A narrative review. Front. Cardiovasc. Med. [Internet] 8, 777016. https://doi.org/10.3389/fcvm.2021.777016/full (2021).
Kou, M. et al. Conventional and novel lipid measures and risk of peripheral artery disease. Arterioscler. Thromb. Vasc. Biol. 41(3), 1229–1238 (2021).
Bays, H. E. et al. Ten things to know about ten cardiovascular disease risk factors. Am. J. Prev. Cardiol. [Internet] 5, 100149 (2021).
American Heart Association. Prevention and treatment of PAD [Internet] (American Heart Association, Dallas (TX), 2025); [cited 2025 Aug 23]. Available from: https://www.heart.org/en/health-topics/peripheral-artery-disease/prevention-and-treatment-of-pad.
Friede, A., Reid, J. A. & Ory, H. W. CDC WONDER: A comprehensive on-line public health information system of the centers for disease control and prevention. Am. J. Public Health. 83(9), 1289–1294. https://doi.org/10.2105/AJPH.83.9.1289 (1993).
Issa, R. et al. Demographic and regional trends of peripheral artery disease-related mortality in the United States, 2000 to 2019. Vasc. Med. 28(3), 205–213. https://doi.org/10.1177/1358863X221140151 (2023).
Naveed, M. A. et al. Trends in coronary artery disease mortality among hyperlipidemic patients: Geographic, gender, and racial insights from CDC WONDER data (1999–2020). Int. J. Cardiol. Cardiovasc. Risk Prev. 25, 200416. https://doi.org/10.1016/j.ijcrp.2025.200416 (2025).
Ingram, D. D. & Franco, S. J. 2013 NCHS urban-rural classification scheme for counties. Vital Health Stat. 166, 1–73 (2014).
National Cancer Institute. Joinpoint Regression Program [Internet] (National Cancer Institute, Bethesda (MD), 2025); [cited 2025 Apr 12]. Available from: https://surveillance.cancer.gov/joinpoint/
Nelson, R. H. Hyperlipidemia as a risk factor for cardiovascular disease. Prim. Care Clin. Office Pract. 40(1), 195–211. https://doi.org/10.1016/j.pop.2012.11.003 (2013).
Gaggini, M., Gorini, F. & Vassalle, C. Lipids in atherosclerosis: Pathophysiology and the role of calculated lipid indices in assessing cardiovascular risk in patients with hyperlipidemia. Int. J. Mol. Sci. 24(1), 75 (2022).
Zemaitis, M. R., Boll, J. M., Dreyer, M. A. Peripheral arterial disease. In: StatPearls [Internet]. Available from: https://www.ncbi.nlm.nih.gov/books/NBK430745/ (2023).
Belur, A. D., Shah, A. J., Virani, S. S., Vorla, M. & Kalra, D. K. Role of lipid-lowering therapy in peripheral artery disease. J. Clin. Med. 11(16), 4872 (2022).
Hackam, D. G. Cardiovascular risk prevention in peripheral artery disease. J. Vasc. Surg. 41(6), 1070–1073 (2005).
Nordanstig, J. et al. Peripheral arterial disease (PAD) – A challenging manifestation of atherosclerosis. Prev. Med. 7(171), 107489 (2023).
Pinto, S., Lopes, S., De Sousa, A. B., Delalibera, M. & Gomes, B. Patient and family preferences about place of end-of-life care and death: An umbrella review. J. Pain Symptom Manage. 67(5), e439–e452 (2024).
Issa, R. et al. Demographic and regional trends of peripheral artery disease-related mortality in the United States, 2000 to 2019. Vasc. Med. 28(3), 205–213 (2023).
Pham, H. N. et al. Burden of hyperlipidemia, cardiovascular mortality, and COVID-19: A retrospective-cohort analysis of US data. J. Am. Heart Assoc. 14(5), e037381 (2024).
Mokdad, A. H. et al. Prevalence of obesity, diabetes, and obesity-related health risk factors, 2001. JAMA 289(1), 76 (2003).
Aguilar-Salinas, C. A. et al. High prevalence of low HDL cholesterol concentrations and mixed hyperlipidemia in a Mexican nationwide survey. J. Lipid Res. 42(8), 1298–1307 (2001).
Hirsch, A. T. Peripheral arterial disease detection, awareness, and treatment in primary care. JAMA 286(11), 1317 (2001).
Erhardt, L., Moller, R., Puig, J. G. Comprehensive cardiovascular risk management – what does it mean in practice? [Internet]. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC2291303/ (2007).
Santos, D. & Dhamoon, M. S. Trends in antihypertensive medication use among individuals with a history of stroke and hypertension, 2005 to 2016. JAMA Neurol. 77(11), 1382 (2020).
American Lung Association. Tobacco trends brief: Overall tobacco trends brief. [Internet]. Available from: https://www.lung.org/research/trends-in-lung-disease/tobacco-trends-brief/overall-smoking-trends
Tóth-Vajna, Z. et al. Screening of peripheral arterial disease in primary health care. Vasc. Health Risk Manag. 1(15), 355–363 (2019).
Wong, J. J. et al. Atherosclerotic cardiovascular disease in aging and the role of advanced cardiovascular imaging. npj Cardiovasc. Health 1(1), 11 (2024).
World Health Organization (WHO). Obesity and overweight [Internet]. Available from: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (2025).
Smolderen, K. G., Lee, M., Arora, T., Simonov, M. & Mena-Hurtado, C. Peripheral artery disease and COVID-19 outcomes: Insights from the Yale DOM-CovX Registry. Curr. Probl. Cardiol. 47(12), 101007 (2021).
Bevan, G. H. & Solaru, K. T. W. Evidence-based medical management of peripheral artery disease. Arterioscler. Thromb. Vasc. Biol. 40(3), 541–553. https://doi.org/10.1161/ATVBAHA.119.312142 (2020).
Lichtenstein, A. H. et al. 2021 dietary guidance to improve cardiovascular health: A scientific statement from the American Heart Association. Circulation 144(23), e472–e487 (2021).
Baumblatt, J., Fryar, C., Gu, Q., Ashman, J. Prevalence of total, diagnosed, and undiagnosed diabetes in adults: United States, August 2021–August 2023. [Internet]. Available from: https://www.cdc.gov/nchs/products/databriefs/db516.htm (2024).
Connelly, P. J., Currie, G. & Delles, C. Sex differences in the prevalence, outcomes and management of hypertension. Curr. Hypertens. Rep. 24(6), 185–192 (2022).
Bae, J. P., Nelson, D. R., Boye, K. S. & Mather, K. J. Prevalence of complications and co-morbidities in males and females with obesity: Real-world insights from claims data analysis. Diabetes Obes. Metab. https://doi.org/10.1111/dom.15914 (2024).
National Institute on Drug Abuse (NIDA). Are there sex differences in tobacco smoking? [Internet]. Available from: https://nida.nih.gov/publications/research-reports/tobacco-nicotine-e-cigarettes/are-there-sex-differences-in-tobacco-smoking (2025).
Najman, J. M. et al. Gender differences in cardiovascular disease risk: Adolescence to young adulthood. Nutr. Metab. Cardiovasc. Dis. 34(1), 98–106 (2023).
Laban, D. et al. Sex differences in features of atherosclerotic plaques as revealed by various imaging techniques: A historical review. Front. Physiol. 16, 1579885 (2025).
Xie, F. et al. Estrogen mediates an atherosclerotic-protective action via estrogen receptor alpha/SREBP-1 signaling. Front. Cardiovasc. Med. 9, 895916 (2022).
National Heart, Lung, and Blood Institute (NHLBI). Obesity and women’s health [Internet]. Available from: https://www.nhlbi.nih.gov/health/overweight-and-obesity/women (2022).
World Health Organization (WHO). Physical activity [Internet]. Available from: https://www.who.int/europe/news-room/fact-sheets/item/physical-activity (2021).
Arrazola, R. A. et al. US cigarette smoking disparities by race and ethnicity — Keep going and going!. Prev. Chronic Dis. 20, E45 (2023).
Hill, M. F., Bordoni, B. Hyperlipidemia. In StatPearls [Internet]. Available from: https://www.ncbi.nlm.nih.gov/books/NBK559182/ (2023).
Geiger A. The most common age among whites in U.S. is 58 – more than double that of racial and ethnic minorities. Pew Research Center [Internet]. Available from: https://www.pewresearch.org/fact-tank/2019/07/30/most-common-age-among-us-racial-ethnic-groups/ (2024).
Richardson, L. D. & Norris, M. Access to health and health care: How race and ethnicity matter. Mt. Sinai J. Med. 77(2), 166–177. https://doi.org/10.1002/msj.20174 (2010).
McCrear, S. Electronic health records suggest racial bias in assessment of patients’ claims. AJMC [Internet]. Available from: https://www.ajmc.com/view/electronic-health-records-suggest-racial-bias-in-assessment-of-patients-claims (2025).
Smyth, S. & Heron, A. Diabetes and obesity: The twin epidemics. Nat. Med. 12(1), 75–80. https://doi.org/10.1038/nm0106-75 (2006).
Laleman, N. et al. Time trends in statin use and incidence of recurrent cardiovascular events in secondary prevention between 1999 and 2013: A registry-based study. BMC Cardiovasc. Disord. 18(1), 209. https://doi.org/10.1186/s12872-018-0941-y (2018).
Mann, D., Reynolds, K., Smith, D. & Muntner, P. Trends in statin use and low-density lipoprotein cholesterol levels among US adults: Impact of the 2001 National Cholesterol Education Program Guidelines. Ann. Pharmacother. 42(9), 1208–1215. https://doi.org/10.1345/aph.1l181 (2008).
Gu, Q., Burt, V. L., Dillon, C. F. & Yoon, S. Trends in antihypertensive medication use and blood pressure control among United States adults with hypertension. Circulation 126(17), 2105–2114. https://doi.org/10.1161/circulationaha.112.096156 (2012).
Benjamin, R. M. The Million Hearts™ initiative: Progress in preventing heart attacks and strokes. Public Health Rep. 127(6), 558–560. https://doi.org/10.1177/003335491212700602 (2012).
Centers for Disease Control and Prevention. Heart Disease and Stroke Prevention [Internet] (CDC, Atlanta, GA, 2024); [cited 2025 Oct 26]. Available from: https://www.cdc.gov/heart-disease-and-stroke-prevention/index.html
Armour, B. S. The quality of preventive and diagnostic medical care: Why do Southern states underperform? ProQuest Dissertations Publishing. Available from: https://www.proquest.com/openview/008befc31bc8b0d5afa746c9558cb498/1?pq-origsite=gscholar&cbl=34496.
Dwyer-Lindgren, L. et al. Cigarette smoking prevalence in US counties: 1996–2012. Popul. Health Metr. 12, 5. https://doi.org/10.1186/1478-7954-12-5 (2014).
Myers, C. A., Slack, T., Martin, C. K., Broyles, S. T. & Heymsfield, S. B. Regional disparities in obesity prevalence in the United States: A spatial regime analysis. Obesity (Silver Spring) 23(2), 481–487. https://doi.org/10.1002/oby.20963 (2015).
Centers for Disease Control and Prevention. Heart Disease and Stroke Data – Quick Maps [Internet]. (CDC, Atlanta, GA, 2024); [cited 2025 Oct 26]. Available from: https://www.cdc.gov/heart-disease-and-stroke-data/quick-maps/heart-disease-stroke.htm.
Casey, M. M., Call, K. T. & Klingner, J. M. Are rural residents less likely to obtain recommended preventive healthcare services?. Am. J. Prev. Med. 21(3), 182–188. https://doi.org/10.1016/s0749-3797(01)00349-x (2001).
Nuotio, J. et al. CVD risk factors and surrogate markers—urban-rural differences. Scand. J. Public Health. 48(7), 752–761. https://doi.org/10.1177/1403494819869816 (2020).
Massachusetts Department of Public Health. Heart Disease and Stroke Prevention and Control Program: Massachusetts Health Promotion Clearinghouse [Internet] (Commonwealth of Massachusetts, Boston (MA), 2025); [cited 2025 Oct 29]. Available from: https://massclearinghouse.ehs.state.ma.us/category/HDSPPROG.html?utm_source=chatgpt.com
Panzavolta, C., Zalunardo, B., Irsara, S., Ferretto, L. & Visonà, A. Peripheral artery disease, the ‘lost syndrome’ during lockdown for COVID-19: A report of three cases. Med. Int. 1(5), 15. https://doi.org/10.3892/mi.2021.15 (2021).
Boccatonda, A., Campello, E., Simion, C. & Simioni, P. Long-term hypercoagulability, endotheliopathy and inflammation following acute SARS-CoV-2 infection. Expert Rev. Hematol. 16(12), 1035–1048. https://doi.org/10.1080/17474086.2023.2288154 (2023).
Burley, N. B., Dy, P. S., Kalantri, S. & Razzaq, K. Aortic thrombosis and acute limb ischemia secondary to COVID hypercoagulability. Cureus. 13(7), e16171. https://doi.org/10.7759/cureus.16171 (2021).
Keller, K. et al. Temporal trends in patients with peripheral artery disease influenced by COVID-19 pandemic. J. Clin. Med. 11(21), 6433. https://doi.org/10.3390/jcm11216433 (2022).
Ambrosino, P. et al. Persistent endothelial dysfunction in post-acute COVID-19 syndrome: A case-control study. Biomedicines 9(8), 957. https://doi.org/10.3390/biomedicines9080957 (2021).
Khera, A. et al. Continuity of care and outpatient management for patients with and at high risk for cardiovascular disease during the COVID-19 pandemic: A scientific statement from the American Society for Preventive Cardiology. Am. J. Prev. Cardiol. 1(1), 100009. https://doi.org/10.1016/j.ajpc.2020.100009 (2020).
Sabatine, M. S. PCSK9 inhibitors: Clinical evidence and implementation. Nat. Rev. Cardiol. 16(3), 155–165. https://doi.org/10.1038/s41569-018-0107-8 (2019).
Ray, K. K. et al. Safety and efficacy of bempedoic acid to reduce LDL cholesterol. N. Engl. J. Med. 380(11), 1022–1032. https://doi.org/10.1056/NEJMoa1803917 (2019).
Alonso-Coello, P. et al. Antithrombotic therapy in peripheral artery disease. Chest 141(2 Suppl), e669S-e690S. https://doi.org/10.1378/chest.11-2307 (2012).
Noukeu, L. C., Wolf, J., Yuan, B., Banerjee, S. & Nguyen, K. T. Nanoparticles for detection and treatment of peripheral arterial disease. Small 14(32), e1800644. https://doi.org/10.1002/smll.201800644 (2018).
Hermel, M., Lieberman, M., Slipczuk, L., Rana, J. S. & Virani, S. S. Monoclonal antibodies, gene silencing and gene editing (CRISPR) therapies for the treatment of hyperlipidemia—The future is here. Pharmaceutics 15(2), 459. https://doi.org/10.3390/pharmaceutics15020459 (2023).
Grant, C. et al. Perspectives on lower extremity peripheral artery disease: A qualitative study of early diagnosis and treatment and the impact of health disparities. Popul. Health Manag. 26(6), 387–396. https://doi.org/10.1089/pop.2023.009 (2023).
Acknowledgements
Not applicable.
Funding
The authors received no funds, grants, or financial support for this study.
Author information
Authors and Affiliations
Contributions
S.K., M.H., M.Hu., H.A.A.D., W.F., J.N., M.B., and A.A. wrote the main manuscript text. M.Q., A.A.Q., and F.P. prepared the figures. S.K. analyzed the data. N.K. prepared the tables. S.A.W., G.C.F., S.E., R.A., M.K.A., P.M., and H.A. reviewed the manuscript. S.A.W. and G.C.F. supervised the project. M.H., S.K., and M.Hu. contributed to the discussion. All authors reviewed and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare that they have no competing interests.
Ethical approval
Not applicable.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Khan, S., Hassan, M., Hussain, M. et al. Trends and disparities in mortality associated with peripheral artery disease and hyperlipidemia, 1999–2024. Sci Rep 15, 45008 (2025). https://doi.org/10.1038/s41598-025-29224-7
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-29224-7
