
Abstract
Obesity is a growing problem worldwide. It is well reported that obesity is associated with various degrees of respiratory function compromise, which could be contributed by mechanical factors as well as co-morbid diseases such as asthma. While spirometry is the gold standard for lung function measurement, it does have the drawback of only being able to measure the global function of the lungs and is uncomfortable for those with difficulty using a large degree of effort. A prospective cross-sectional study was conducted in Queen Mary Hospital, Hong Kong to recruit Chinese obese and non-obese subjects, to compare and correlate the lung function parameters measured by electrical impedance tomography (EIT) and spirometry. Obesity was diagnosed based on the local definition of body mass index of 25 kg/m2 or above, using the cut-off value for Asian population. A total of 42 obese subjects and 35 non-obese subjects were included in this study. The spirometric values (Litres) measured by spirometry and EIT demonstrated good correlation among obese and non-obese subjects, with Pearson correlation coefficient of 0.705 and 0.673 for FEV1 among obese and non-obese subjects, p-value < 0.01. The Pearson correlation coefficients were 0.568 and 0.541 for FVC among obese and non-obese subjects respectively, p-value < 0.01. EIT technology has comparable performance in lung function measurement among obese and non-obese subjects. It can suggest that EIT is a potential tool for lung function measurement in obese subjects as in non-obese subjects.
Similar content being viewed by others


Introduction
Obesity is an increasing problem, both worldwide and in Hong Kong, where the proportion of adults who were obese increased by over 40%, from 21.2% in 2003–2004 to 29.9% in 2014–20151,2. Obesity is reported to be associated with reduced lung function in previous research, as the adipose tissue reduces the maximum volume for the lungs to expand into, as well as increasing the resistance to the movement of air in and out of the lungs3,4,5. Obesity also increases the likelihood of comorbidities such as asthma6,7. In the assessment of chronic respiratory diseases, the classical method for lung function assessment is spirometry. However, spirometry has the drawback of only being able to measure the global function of the lungs, with regional lung function assessment not being possible, and is uncomfortable for those with difficulty using a large degree of effort.
Electrical impedance tomography (EIT) can be an alternative non-invasive diagnostic measure that does not involve ionizing radiation8,9,10,11. EIT has been employed in clinical use for more than a decade to provide qualitative measurement of ventilation in patients. Using this technology, non-invasive and low-cost tomographic imaging of the body is employed to detect and monitor several key diseases, such as chronic obstructive pulmonary disease (COPD), asthma8 and fatty liver12. Using EIT to assess the lung function can detect where the inhalation and expiration of air results in large changes of conductivity.
It has been suggested that higher percentage of body fat to be associated with lower lung volumes with a greater effect in men than women13. Furthermore, the distribution of fat can also affect the lung function. Intrathoracic fat, the volume of visceral abdominal fat and subcutaneous thoracic fat were inversely associated with forced expiratory volume in 1 s (FEV1) percentage predicted in male patients14. Given the knowledge of how body fat percentage and obesity can affect lung function, with the potential limitations of spirometry in lung function assessment, we propose the use of EIT as an alternative way of lung function assessment in obese patients.
We conducted the current clinical study on obese and non-obese subjects, to establish the feasibility of using EIT devices in detecting lung functional changes. Specifically, we aimed to establish the relationship between EIT-derived functional indicators and standard pulmonary functional testing results (i.e., the spirometry results).
Methods
The study assessed the lung function of obese and non-obese subjects using spirometry and EIT. The Gense-EIT lung device to be used is a potentially self-administrable, portable and non-invasive imaging modality capable of capturing the cross-sectional bioelectrical impedance distribution of the lungs up to 50 frames per second using EIT. Simultaneous paired EIT/Spirometer measurements are recorded when the subject goes through a 40 s forced exhale paradigm, repeated three times. The Gense-EIT lung device employs a band consisting of 16 equally distributed electrodes around the thorax of a subject. The electrode band is connected to a control unit that switches the electrode stimulation and measurement pairs and subsequently sends the collected measurements to a computational unit for image reconstruction. The images are then processed to extract functional lung images and indicators. This device can be connected to a computer, a smartphone, and/or a large LED screen, allowing the lung functional images and indicators to be visualized. In this study, all the participants performed spirometry and EIT in dedicated research facility in the presence of trained technicians, who instructed patients to perform spirometry as well as performing EIT examination for the patients. The spirometry and EIT were performed by 2 independent technicians.
Adult Chinese obese subjects with a BMI ≥ 25 and non-obese subjects with BMI < 25, based on the BMI cut-off for Asian population15; age from 18 to 75 were recruited in this study16. The participants’ age (± 5 years), sex, smoking status were matched among obese and non-obese subjects. All the participants were ambulatory with good physical functional status and could travel to the research facility for the assessment. All the included subjects had a structured questionnaire, together with cross checking with electronic medical records to ensure they do not have any clinical features of respiratory diseases. The exclusion criteria include subjects with underlying respiratory diseases, subjects with implanted electronic devices which would interfere with EIT assessment, subjects with spinal diseases, subjects who had with recent heart or lung surgery in past 3 months, pregnant women, subjects who were unable to perform spirometry and subjects whose exhale curve in EIT did not pass the noise-based quality criterion.
Spirometry was conducted using MIR Spirobank II®. EIT was conducted using Gense-EIT lung device. The subjects included had spirometry and EIT assessments the same day. The recruitment period was from 2024-01-12 to 2024-08-23.
Statistical analysis
The primary outcome of the study was testing the correlation of EIT assessed lung function in obese individuals against that of spirometry.
The demographic and clinical data were described as actual frequency, mean ± standard deviation (SD) or median [inter-quartile range (25th-75th centile)]. Baseline demographic and clinical data were compared between the two groups (with or without obesity) with independent t-tests (if normally distributed) or non-parametric tests (if not normally distributed). Chi square test was employed to compare the categorical variables in the two groups (with or without obesity). EIT-derived voxel-wise and regional bioimpedance, FEV1 and FVC, coefficient of variation (CV) and heterogeneity index (HI) parameters were measured/calculated. The correlation FEV1 and FVC (in Litres) measured by spirometry and EIT were assessed by Pearson correlation.
Ethical approval
The study was approved by the Institutional Review Board (IRB) of the University of Hong Kong and Hospital Authority Hong Kong West Cluster (UW 23–509). All the patients recruited signed the informed consent. The study was conducted in compliance with the Declaration of Helsinki.
Results
A total of 42 obese subjects and 35 non-obese subjects were included. 14 subjects were excluded based on an a priori curve index quality classification, as they had suboptimal EIT assessment limiting the interpretation. The mean age was 60 ± 14 years, with 62% of the subjects being male. The mean FEV1 and FVC measured by spirometry were 1.86 ± 0.69 L (77 ± 27%) and 2.57 ± 0.97 L (82 ± 30%). The mean FEV1 and FVC measured by EIT were 1.81 ± 0.77 L (74 ± 30%) and 2.76 ± 0.98 L (88 ± 31%). There was no statistically significant difference in the background clinical features and demographics among the obese and non-obese groups, except for their body weight and BMI. The baseline demographics of the subjects were illustrated in Table 1.
Correlation of EIT and spirometry parameters in obese and non-obese subjects
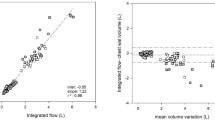
The correlation of FEV1 and FVC (in Litres) between spirometry and EIT among non-obese subjects measured by Pearson correlation coefficient were 0.673 and 0.541 respectively with both p-values < 0.001. This suggested a significantly strong correlation for FEV1 and a significant moderate correlation for FVC among non-obese subjects. The correlation was demonstrated in Fig. 1.

Correlation of EIT and spirometry parameters (FEV1 and FVC in Litres) in non-obese subjects.
The correlation of FEV1 and FVC (in Litres) between spirometry and EIT measured by Pearson correlation coefficient among obese subjects were 0.705 and 0.568 respectively, with both p-values < 0.001. This suggested a significant strong correlation for FEV1 and significant moderate correlation for FVC among obese subjects. The correlation was demonstrated in Fig. 2.

Correlation of EIT and spirometry parameters (FEV1 and FVC in Litres) in obese subjects.
Images from EIT, representing the change in conductivity between the middle and highest part of the breathing were also shown in Fig. 3. The two subjects, one obese and one control, have been chosen with similar spirometry indexes. They display similar EIT images, suggesting that they have similar performances and findings in EIT assessment.

Lung conductivity image of (A) an obese subject and (B) a non-obese subject obtained from EIT.
Discussion
In the current study on lung function assessment by spirometry and EIT, we demonstrated moderate to strong correlation for lung function parameters (FEV1 and FVC) measured by both methods among obese and non-obese subjects. The findings in this study suggest that EIT is a potential tool for lung function measurement in patients regardless of their body build.
Currently, spirometry has been the gold standard in lung function assessment. However, spirometry has its own drawbacks which include the lack of spatial resolution and difficulty for patients who have hearing impairment or at extreme age to follow the instructions. As such, there is a need to look for alternative method for lung function measurement, with EIT being proposed.
Currently, the use of EIT among obese patients is mainly limited to those under general anaesthesia, to assess for development of atelectasis17, pretty much the same as the conventional use of EIT, which is limited to critically ill patients18,19. EIT demonstrated its role in guiding positive end-expiratory pressure (PEEP) optimization among patients with acute respiratory distress syndrome (ARDS) which improved lung compliance, reduced mechanical power and lowered driving pressure compared to traditional methods20. EIT has also been demonstrated to offer noninvasive bedside assessment of global and regional ventilation changes in the intensive care unit (ICU) setting, using various EIT indices such as tidal impedance variation, end-expiratory lung impedance, global inhomogeneity index and regional ventilation delay21. The benefits of EIT in having real-time tomographic functional images of the lungs allowed EIT to be introduced and used in dedicated aforementioned settings. It is also not surprised to see the use of EIT among coronavirus disease (COVID-19) patients with moderate-severe ARDS as a measure to titrate PEEP as in other ARDS patients22. Among obese patients, EIT also demonstrated its role in respiratory failure management among obese subjects, by reducing the mortality of these critically ill obese patients23.
The use of EIT among non-critically ill patients was also explored in recent years. There was a study suggesting the use of EIT for lung function assessment demonstrated good correlation among healthy non-obese subjects24. There is also ongoing development of a novel guided breathing paradigm which consists of a periodic inhalation and exhalation at 12 breaths per minute. Previous report suggested that such breathing paradigm could reflect both global and regional lung function changes among non-obese healthy subjects. This novel close-to-effortless guided breathing paradigm can potentially overcome a major hurdle of spirometry24. Regional lung assessment, including three-dimensional assessment, has been assessed with EIT as well19,25. EIT has also been shown to be useful in real-time monitoring, such as in acute pulmonary embolism26.
While EIT has been demonstrated to be able to predict standard spirometry indicators over a wide dynamic range, the data is mainly limited to healthy non-obese subjects. To our best knowledge, this is the first study reported the use of EIT in predicting spirometry values in obese subjects. The results are not only significant but also show comparable correlation as in subjects without obesity. This is a promising finding to suggest the high degree of correlation of lung function parameters measured by spirometry and EIT, which supports its use among subjects who are obese.
Th Gense-EIT lung device used in this study was a palm size and light-weight console with dimensions of 15.2 × 11.0 × 4.4 cm3 and < 300 g (Fig. 4). The portable console functions together with a reusable and disinfectable 16-channel electrode belt mobile app interface, and cloud-based processing pipeline. The portability function is supported through the integration of a power and battery management module enabling the complete system to operate with a constant power supply of 3.3 V; thus it can function either through a power socket or a Li-ion battery. This device has a major advantage over the other EIT devices which require a higher power supply ranging from ± 5 V (total of 10 V) to ± 15 V (total of 30 V). The Gense-EIT lung device allows clinical use in ambulatory settings given its small size with the lower power supply needed. Currently, the cost for 1 EIT exam is as low as USD 30, which is affordable when compared with spirometry. The costs of the Gense-EIT device is also cheaper than computed tomography machine by a factor of 100 or more, and also cheaper than traditional hospital-grade spirometry device by a factor of 50.

(A and B) Gense-EIT device and (C) schematic diagram on the process of data acquisition/processing by EIT.
There are several limitations in this study to be addressed. Firstly, all the subjects did not have underlying respiratory diseases based on the screening questionnaire and medical record, together with relatively normal lung function in both spirometry and EIT. This may affect the applicability among patients with underlying respiratory diseases. Yet, the establishment of the basis with healthy subjects is needed before extending the subject to diseased subjects. Secondly, all the subjects included are Chinese which affects the generalizability to other ethnic groups, though there have not been any reports on the important difference in lung function assessment across different ethnic groups by EIT or spirometry while the lung function assessment by spirometry was based on local reference that is well established27. Thirdly, the presence of corrupted signal data due to inadequate electrode contact was caused by perspiration. This issue was particularly prevalent during the summer months in which this study was performed, when many subjects experienced heavy sweating. The mean age of the excluded subjects was 61.9 ± 17.2 years, with 9 (64.2%) being male. The mean BMI of the excluded subjects was 25.9 ± 4.9. Overall, the excluded subjects showed similar baseline characteristics as the whole cohort. Although remedial actions were taken, including allowing affected participants 10–20 min of rest in an air-conditioned room prior to testing, sweating persisted in some subjects, impacting the quality of the EIT data of almost 20% of the cohort. Based on this observation, we will recommend the patients to have a quick body cleansing mainly aiming at removing the sweat before EIT examination to ensure the quality of the EIT signals collected to be suitable for analysis. Another limitation is a relatively small sample size in this pilot study, and we believe conducting a larger scale study that includes obese and non-obese subjects, as well as including patients with or without underlying respiratory diseases, is warranted. While subjects without the symptoms or history of chronic respiratory diseases were included, we still noted some patients having impaired lung function, which could be due to undiagnosed respiratory diseases. However, this would not impair the interpretation of the findings as the purpose of this study was to assess the correlation of lung function assessment by spirometry and EIT among obese and non-obese subjects. Also, the lung function parameters did not significantly differ among the obese and non-obese subgroups.
Yet, what is presented here is just the beginning of the journey of EIT measurement among obese subjects. Moving a step forward, further refinement of EIT technique with higher resolution, more extensive lung coverage with more belts, potential three-dimensional reconstruction, as well as effort-independent breathing paradigms shall be the future of EIT development, which makes EIT a lung function assessment tool that can be done at low costs, high accuracy, and risk free.
Conclusion
EIT technology has comparable performance among obese and non-obese subjects. It can suggest that EIT is a potential tool for lung function measurement in obese subjects as in non-obese subjects.
Data availability
All available data are presented in the manuscript.
References
Apovian, C. M. Obesity: definition, comorbidities, causes, and burden. Am. J. Manag Care. 22, s176–185 (2016).
Engin, A. The definition and prevalence of obesity and metabolic syndrome. Adv. Exp. Med. Biol. 960, 1–17. https://doi.org/10.1007/978-3-319-48382-5_1 (2017).
Melo, L. C., Silva, M. A. & Calles, A. C. Obesity and lung function: a systematic review. Einstein (Sao Paulo). 12, 120–125. https://doi.org/10.1590/s1679-45082014rw2691 (2014).
Salome, C. M., King, G. G. & Berend, N. Physiology of obesity and effects on lung function. J. Appl. Physiol. (1985). 108, 206–211. https://doi.org/10.1152/japplphysiol.00694.2009 (2010).
Dixon, A. E. & Peters, U. The effect of obesity on lung function. Expert Rev. Respir Med. 12, 755–767. https://doi.org/10.1080/17476348.2018.1506331 (2018).
Miethe, S., Karsonova, A., Karaulov, A. & Renz, H. Obesity and asthma. J. Allergy Clin. Immunol. 146, 685–693. https://doi.org/10.1016/j.jaci.2020.08.011 (2020).
Mohan, A., Grace, J., Wang, B. R. & Lugogo, N. The effects of obesity in asthma. Curr. Allergy Asthma Rep. 19, 49. https://doi.org/10.1007/s11882-019-0877-z (2019).
Nakamura, H. et al. Current advances in pulmonary functional imaging. Respir Investig. 62, 49–65. https://doi.org/10.1016/j.resinv.2023.09.004 (2024).
Frerichs, I. Electrical impedance tomography (EIT) in applications related to lung and ventilation: a review of experimental and clinical activities. Physiol. Meas. 21, R1–21. https://doi.org/10.1088/0967-3334/21/2/201 (2000).
Jang, G. Y. et al. Integrated EIT system for functional lung ventilation imaging. Biomed. Eng. Online. 18, 83. https://doi.org/10.1186/s12938-019-0701-y (2019).
Adler, A. et al. Whither lung EIT: where are we, where do we want to go and what do we need to get there? Physiol. Meas. 33, 679–694. https://doi.org/10.1088/0967-3334/33/5/679 (2012).
Touboul, A. et al. Unmixing multi-spectral electrical impedance tomography (EIT) predicts clinical-standard controlled Attenuation parameter (CAP) for nonalcoholic fatty liver disease classification: a feasibility study. Annu. Int. Conf. IEEE Eng. Med. Biol. Soc. 2022, 576–579. https://doi.org/10.1109/EMBC48229.2022.9871313 (2022).
Sutherland, T. J., McLachlan, C. R., Sears, M. R., Poulton, R. & Hancox, R. J. The relationship between body fat and respiratory function in young adults. Eur. Respir J. 48, 734–747. https://doi.org/10.1183/13993003.02216-2015 (2016).
Kwack, W. G. et al. Association between thoracic fat measured using computed tomography and lung function in a population without respiratory diseases. J. Thorac. Dis. 11, 5300–5309. https://doi.org/10.21037/jtd.2019.11.54 (2019).
Li, Z., Daniel, S., Fujioka, K. & Umashanker, D. Obesity among Asian American people in the united states: A review. Obes. (Silver Spring). 31, 316–328. https://doi.org/10.1002/oby.23639 (2023).
W.H.O.Expert Consultation. Appropriate body-mass index for Asian populations and its implications for policy and intervention strategies. Lancet 363, 157–163. https://doi.org/10.1016/S0140-6736(03)15268-3 (2004).
Nothofer, S. et al. Electrical impedance tomography-based evaluation of anesthesia-induced development of atelectasis in obese patients. J. Clin. Med. https://doi.org/10.3390/jcm13247736 (2024).
Kazakov, D. et al. PEEP Titration guided by electrical impedance tomography in critically ill mechanically ventilated patients with acute hypoxemic respiratory failure. Folia Med. (Plovdiv). 66, 869–875. https://doi.org/10.3897/folmed.66.e134512 (2024).
Barbosa da Rosa, N. Jr. et al. Three-Dimensional electrical impedance imaging during spontaneous breathing trials in patients with acute hypoxic respiratory failure: A pilot study. Crit. Care Explor. 7, e1198. https://doi.org/10.1097/CCE.0000000000001198 (2025).
Songsangvorn, N. et al. Electrical impedance tomography-guided positive end-expiratory pressure Titration in ARDS: a systematic review and meta-analysis. Intensive Care Med. 50, 617–631. https://doi.org/10.1007/s00134-024-07362-2 (2024).
Franchineau, G. et al. Electrical impedance tomography to monitor hypoxemic respiratory failure. Am. J. Respir Crit. Care Med. 209, 670–682. https://doi.org/10.1164/rccm.202306-1118CI (2024).
Jonkman, A. H. et al. Lung recruitment assessed by electrical impedance tomography (RECRUIT): A multicenter study of COVID-19 acute respiratory distress syndrome. Am. J. Respir Crit. Care Med. 208, 25–38. https://doi.org/10.1164/rccm.202212-2300OC (2023).
Kacmarek, R. M., Wanderley, H. V., Villar, J. & Berra, L. Weaning patients with obesity from ventilatory support. Curr. Opin. Crit. Care. 27, 311–319. https://doi.org/10.1097/MCC.0000000000000823 (2021).
Zouari, F. et al. Affordable, portable and self-administrable electrical impedance tomography enables global and regional lung function assessment. Sci. Rep. 12, 20613. https://doi.org/10.1038/s41598-022-24330-2 (2022).
Janulionis, A. et al. Regional differences in lung ventilation during the early transition period in late preterm and term neonates assessed by electrical impedance tomography. Child (Basel) https://doi.org/10.3390/children11111314 (2024).
Li, J. et al. Dynamic EIT technology for real-time non-invasive monitoring of acute pulmonary embolism: a Porcine model experiment. Respir Res. 26, 7. https://doi.org/10.1186/s12931-024-03090-9 (2025).
Ip, M. S. et al. Updated spirometric reference values for adult Chinese in Hong Kong and implications on clinical utilization. Chest 129, 384–392. https://doi.org/10.1378/chest.129.2.384 (2006).
Funding
This research was supported by Hong Kong Obesity Society Research Grant.
Author information
Authors and Affiliations
Contributions
W.C.K. and A.T. were involved with study concept and design; analysis and interpretation of data; acquisition of data; drafting of manuscript; critical revision of the manuscript for important intellectual content; study supervision; and approval of the final version of the manuscript. J.C, W.S.C., V.S. and M.M.A.Y. were involved with critical revision of the manuscript for important intellectual content, and approval of the final version of the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Kwok, W.C., Touboul, A., Chow, W.S. et al. Lung function assessment by electrical impedance tomography among obese patients. Sci Rep 15, 45337 (2025). https://doi.org/10.1038/s41598-025-29559-1
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-29559-1
