
Abstract
Fibrinogen serves as a vital hemostatic factor and an early marker of inflammation, with established associations to unfavorable clinical outcomes, particularly in cardiovascular contexts. However, its specific effects in female populations are not well understood. This research aims to evaluate the relationship between serum fibrinogen concentrations and long-term mortality among female patients undergoing coronary artery bypass grafting (CABG). We analyzed data from the Medical Information Mart for Intensive Care IV (MIMIC-IV) database. The primary outcome assessed was one-year mortality, while secondary outcomes included hospital length of stay and incidence of sepsis. The associations between fibrinogen concentrations and clinical outcomes were evaluated retrospectively utilizing Cox proportional hazards models, along with subgroup analyses and restricted cubic splines (RCS). A total of 1,097 patients were included, with an average age of 70.8 years (range: 60.8–80.8) and a mean body mass index (BMI) of 31 kg/m² (range: 24–38). Analysis using Cox regression revealed a significantly elevated risk of one-year mortality linked to both low and high fibrinogen levels (Q1: Hazard ratio (HR) 2.91, 95%ConfidenceInterval (95% CI) 1.14 ~ 7.46; Q6: HR 4.3, 95% CI 1.66 ~ 11.13). Additionally, RCS analysis illustrated a U-shaped relationship between fibrinogen levels and mortality, identifying an inflection point at 174 mg/dL. These findings were corroborated by stratified and sensitivity analyses. In female patients undergoing CABG, both low and high fibrinogen levels are associated with an elevated risk of one year, mortality, exhibiting a U-shaped relationship. Further prospective research is warranted to validate the associations identified in this study.
Similar content being viewed by others

Introduction
Coronary artery bypass grafting (CABG) remains the gold-standard treatment for multivessel coronary artery disease, particularly in patients with diabetes mellitus, by restoring normal coronary blood flow and significantly improving long-term survival. Globally, approximately 470,000 CABG and valve replacement procedures are performed annually, establishing CABG as one of the most frequently performed cardiovascular interventions1,2,3. However, recent high-quality studies have demonstrated that female patients undergoing CABG experience higher short- and long-term mortality compared with male patients4,5,6,7, underscoring the need for more proactive management in women8. It is therefore essential to recognize women as a distinct patient subgroup and to establish simple, clinically applicable risk indicators tailored to this population. Such tools may facilitate the development of targeted clinical strategies and improve early postoperative outcomes9.
Inflammation plays a central role in atherosclerosis, and inflammatory markers may be valuable for risk assessment and management of CABG patients10,11. Among these markers, fibrinogen—a major acute phase reactant and coagulation factor - has emerged as a potential prognostic indicator in cardiovascular disease12. Fibrinogen not only mediates platelet aggregation13, but also contributes significantly to the development and progression of atheromatous plaques14. Previous studies have shown that abnormal fibrinogen levels are associated with an increased risk of mortality in several cardiovascular diseases, including heart failure15, myocardial infarction16, coronary heart disease17, end-stage renal disease18, even in asymptomatic individuals19. Research in CABG has identified preoperative fibrinogen levels as important predictors of mortality20, hospital length of stay21 and graft failure22. Nevertheless, factors such as cardiopulmonary bypass (CPB), aprotinin administration, hemofiltration, and surgical duration can influence fibrinogen levels, suggesting that early postoperative fibrinogen measurement may offer superior prognostic value compared with preoperative assessment23.
To date, no large-scale study has systematically evaluated the association between postoperative fibrinogen levels and one-year mortality specifically among female CABG patients. Using the Medical Information Mart for Intensive Care (MIMIC-IV) database, this study aims to elucidate the relationship between fibrinogen levels and 1-year mortality in women undergoing CABG. By analyzing a robust real-world cohort, we seek to determine whether fibrinogen acts as an independent risk factor for mortality in this high-risk population, while adjusting for potential confounders.
Method
Study design and ethics
This study employed a retrospective cohort design using deidentified patient-level data from intensive care unit (ICU) admissions. We accessed the MIMIC-IV database, an enhanced iteration of MIMIC-III that includes updated data and reconstructed tables containing clinical information for over 190,000 patients and 450,000 hospitalisations at Beth Israel Deaconess Medical Center (BIDMC) in Boston, MA, USA24. Access to this data was granted following completion of the National Institutes of Health Human Research Participant Protection course and successful completion of the Collaborative Institutional Training Initiative (CITI) review. The study adhered to the tenets of the 1975 Declaration of Helsinki. The Medical Information Mart for Intensive Care is publicly available and has received Institutional Review Board (IRB) approval from BIDMC(2001-P-001699/14) and the Massachusetts Institute of Technology (0403000206).
Selection of participants
The analysis included 6318 patients aged 18 years or older who underwent CABG and were admitted to the ICU for the first time. Exclusion criteria comprised: (1) repeat ICU admissions; (2) lack of fibrinogen data within 24 h of admission; and (3) male patients. After applying these criteria, the final cohort comprised 1097 patients (Fig. 1).

Flowchart of the study cohort selection criteria.
Covariates extraction
Initial measurements taken within the first 24 h of ICU admission served as the parameters for this study. To extract the relevant patient information, we utilized SQL alongside Navicat software (version 15). The variables analyzed were categorized as follows: (1) Demographics: age and BMI; (2) Vital Signs: arterial systolic pressure (ABPS), arterial diastolic pressure (ABPD), temperature, and heart rate; (3) Blood Biochemical Markers: white blood cell (WBC) count, red blood cell (RBC) count, platelet count, sodium, potassium, total calcium, chloride, glucose, anion gap, lactate, urea nitrogen, and creatinine; and (4) Clinical Scores: Sequential Organ Failure Assessment (SOFA), Acute Physiology Score III (APS III), Simplified Acute Physiology Score II (SAPS II), Glasgow Coma Scale (GCS), and Charlson Comorbidity Index (CHARLSON).
Expose and outcome
The primary exposure variable was early fibrinogen measurement, defined as the first fibrinogen level within 24 h postoperatively, a method validated in previous studies15. Patients were divided into six groups based on serum fibrinogen levels: Q1 (< 155 mg/dL), Q2 (155–178 mg/dL), Q3 (178–201 mg/dL), Q4 (201–230 mg/dL), Q5 (230–267 mg/dL) and Q6 (>267 mg/dL). This method ensures that the sample size of each group is relatively balanced. It also facilitates comparison of clinical outcomes among patients with different fibrinogen levels, thereby minimizing bias. For the MIMIC-IV data, the primary outcome was one-year mortality, with secondary outcomes including sepsis and length of hospital stay. Follow-up began at the time of patient admission, and mortality data were obtained from the US Social Security Death Index.
Statistical analyses
Continuous variables are presented as mean ± standard deviation or median (interquartile range), as appropriate, and categorical variables are presented as proportions. Statistical analyses included Student’s t-test, analysis of variance and Mann-Whitney U test, where appropriate. Categorical variables were compared using the χ² test.
Cox regression analyses used multivariate models to assess the predictive role of fibrinogen on mortality, considering fibrinogen levels as both categorical and continuous variables. Confounders were selected on the basis of statistical significance and clinical relevance. Five Cox regression models were developed, with results reported as hazard ratios and 95% confidence intervals (CIs). Selection of covariates for the final model was based on clinical significance, previous studies, and degree of correlation with the exposure. We check the models for multicollinearity, and we did not find multicollinearity between the variables in models. Model 1 included no covariates. Model 2 adjusted for demographic variables, including age and BMI. In Model 3, eleven additional covariates related to basic vital signs were incorporated, such as heart rate, ABPS, ABPD, and temperature. Model 4 further included eleven blood biochemical indicators based on Model 3, encompassing WBC count, RBC count, platelet count, sodium, potassium, total calcium, chloride, glucose, anion gap, lactate, urea nitrogen, and creatinine. Finally, Model 5 added eleven clinical scores based on Model 4, including the SOFA, APS III, SAPS II, GCS, and CHARLSON. Fibrinogen levels were further evaluated as a continuous variable using RCS to investigate the dose-response relationship with long-term mortality risk. Non-linear associations were assessed using a recursive algorithm to identify inflection points for fibrinogen and one-year mortality. A two-stage Cox proportional hazards model was used to analyse the relationship before and after the identified inflection point.
Sensitivity analyses were performed to assess the robustness of the results. In addition to the primary outcomes, secondary outcomes were analysed using regression models. Stratified analyses examined whether the effect of fibrinogen differed between subgroups defined by BMI, SOFA, APS III, SAPS II and CHARLSON scores. Multiplicative interactions were tested using interaction terms and the likelihood ratio test. Missing data were handled using predictive mean adjustment with the Multivariate Imputation via Chained Equations method in R. Analyses of imputed datasets confirmed the stability of the results25.
All analyses were conducted using R (version 4.1.1) and Free Statistics software (version 1.8). A two-tailed P < 0.05 was considered statistically significant, unless otherwise specified. The STROBE checklist was adhered to for reporting purposes.
Results
Subject characteristics
Table 1 summarizes the baseline characteristics of the 1,097 participants categorized into six quartiles based on fibrinogen levels. The mean age of the cohort was 70.8 years, with significant age variations across the quartiles (p = 0.002); notably, patients in Q1 had a mean age of 73.0 ± 10.4 years, while those in Q6 were younger, averaging 68.5 ± 10.8 years. BMI differed significantly among the groups (p < 0.001), with Q6 exhibiting the highest mean BMI of 33.9 ± 7.4. Although vital signs, including heart rate, ABPS, and ABPD, did not show significant differences across quartiles, several blood biochemical markers did. These included WBC) counts (p < 0.001), RBC counts (p = 0.001), platelet counts (p < 0.001), sodium levels (p < 0.001), potassium levels (p < 0.001), calcium (p = 0.023), chloride (p < 0.001), lactate (p < 0.001), urea nitrogen (p < 0.001), and creatinine (p < 0.001). The SOFA score also varied significantly across quartiles (p = 0.001), reflecting differences in organ dysfunction. Regarding clinical outcomes, the length of hospital stay was significantly longer in Q6 (12.2 ± 9.9 days) compared to other quartiles (p < 0.001). The one-year mortality rate varied markedly, with 9.6% in Q1 compared to 3.3% in Q5, indicating a significant link between fibrinogen levels and mortality (p = 0.013). Furthermore, the incidence of sepsis was notably higher in Q1 (64%) than in Q6 (39.1%) (p < 0.001).
Relationship between fibrinogen and clinical outcomes in female patients with CABG
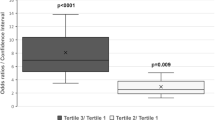
Table 2 details the results from the multivariable Cox regression analyses that evaluated the relationship between fibrinogen levels and one-year mortality. In Model 1, the hazard ratio (HR) for the continuous fibrinogen variable was not significant (HR: 1.02, p = 0.095); however, it became significant in Model 2 (HR: 1.03, p = 0.028) and Model 3 (HR: 1.02, p = 0.037), suggesting that higher fibrinogen levels may be associated with an increased mortality risk. This association diminished in Models 4 and 5, where the HRs were 1.02 (p = 0.308) and 1.01 (p = 0.563), respectively. When considering fibrinogen as a categorical variable, patients in the lowest quartile (Q1, ≤ 155 mg/dL) exhibited a significantly elevated risk of mortality, with HRs ranging from 2.72 (p = 0.026) in Model 1 to 2.91 (p = 0.026) in Model 5. In contrast, patients in the second (Q2, 155–178 mg/dL) and third quartiles (Q3, 178–201 mg/dL) did not show significant mortality risks compared to the reference group (Q4, 201–230 mg/dL). Notably, patients in the highest quartile (Q6, > 267 mg/dL) demonstrated a significantly increased mortality risk, with HRs of 2.71 (p = 0.025) in Model 1 and 4.30 (p = 0.003) in Model 5. Despite these findings, the trend across quartiles did not reach statistical significance (p for trend > 0.05), indicating a nonlinear relationship between fibrinogen levels and mortality.
Dose–response relationships
The analysis of RCS revealed a nonlinear, U-shaped relationship between fibrinogen levels and mortality across one year (Fig. 2). To investigate this association further, Cox proportional hazards models and two-piecewise Cox models were employed, yielding significant results (P for log-likelihood ratio < 0.05 in both models) (Table 3). An inflection point was identified at 174 mg/dL. Below this threshold, fibrinogen levels were inversely related to mortality (HR 0.969, 95% CI 0.947–0.991), whereas levels above this threshold correlated with increased mortality risk (HR 1.0057, 95% CI 1.0001–1.0114). SFigure 1 shows the Kaplan-Meier curve for patients in the different fibrinogen groups. A too-high or too-low fibrinogen was significantly associated with risk of 90-day mortality (P = 0.013 by the logrank test).

Dose–response relationships between fibrinogen with 1-year mortality rate. Solid and dashed lines represent the predicted value and 95% confidence intervals. Adjusted for demographic variables (age, BMI), Basic vital signs (heart rate, ABPS, ABPD, Temperature), Blood biochemical indicators (WBC, RBC, platelet count, sodium, potassium, calcium total, chloride, glucose, anion gap, lactate, urea nitrogen, creatinine) SOFA, APS Ⅲ, SAPSⅡ, GCS, HARLSON Abbreviations: the unit of fibrinogen is mmol/L, BMI: body mass index; ABPS: Arterial systolic pressure; ABPD: Arterial diastolic pressure; WBC, white blood cell count; RBC, red blood cell count; sofa, Sequential Organ Failure Assessment; APS Ⅲ: Acute Physiology and Chronic Health Evaluation Ⅲ; SAPSⅡ: simplified acute physiology score ii, GCS, Glasgow Coma Scale; CHARLSON, Charlson comorbidity index, AKI: acute kidney injury, CRRT, Continuous Renal Replacement Therapy; CI: confidence interval; HR: hazard ratio; Ref: reference
Subgroup
Figure 3 illustrates the results from the stratified analysis of the relationship between serum fibrinogen levels and one-year mortality, showing adjusted hazard ratios (HRs) across various subgroups. We investigated fibrinogen’s predictive capacity regarding mortality outcomes across different population segments defined by BMI, SOFA, APS III, SAPS II and Charlson scores. No statistically significant interactions between the variables were identified, and the relationship between fibrinogen levels and mortality was consistent in direction. The stratified analysis results indicated a similar association of fibrinogen levels across most subpopulations.

Stratified analysis of the association of association of serum fibrinogen with one-year mortality. Adjusted HRs are shown. Interaction was tested adjusted. Subgroups with and adjusted P-interaction < 0.05 were considered effect modifiers on the association of serum fibrinogen with one-year mortality.
Sensitivity analysis
Several sensitivity analyses were conducted to evaluate the robustness of our findings. First, Table S1 summarizes the results from the multivariable Cox regression analyses concerning the association between fibrinogen levels and sepsis risk. The continuous fibrinogen variable consistently exhibited a significant inverse relationship with sepsis across all models, with HRs ranging from 0.95 to 0.96 and p-values below 0.003, suggesting that higher fibrinogen levels are associated with a reduced sepsis risk. When evaluated as a categorical variable, patients in the second quartile (Q2, 155–178 mg/dL) displayed a notably lower risk of sepsis compared to the reference group (Q1, ≤ 155 mg/dL), with HRs decreasing from 0.63 (p = 0.032) in Model 1 to 0.55 (p = 0.011) in Model 5. Patients in the third quartile (Q3, 178–201 mg/dL) also showed a substantial reduction in sepsis risk, with HRs ranging from 0.51 (p = 0.002) to 0.50 (p = 0.002) across models. The fourth quartile (Q4, 201–230 mg/dL) demonstrated a significant decrease in sepsis risk as well, with HRs ranging from 0.40 (p < 0.001) to 0.37 (p < 0.001). Furthermore, patients in the fifth (Q5, 230–267 mg/dL) and sixth quartiles (Q6, > 267 mg/dL) exhibited similar trends, with HRs of 0.39 (p < 0.001) and 0.36 (p < 0.001) for Q5, and 0.32 (p < 0.001) and 0.31 (p < 0.001) for Q6, respectively. The trend across quartiles exhibited statistical significance (p for trend < 0.001), reinforcing the association between higher fibrinogen levels and a decreased risk of sepsis.
Second, Table S2 displays the results of multivariable linear regression analyses assessing the association between fibrinogen levels and hospital length of stay. The continuous fibrinogen variable consistently demonstrated a significant positive correlation with length of stay across all models, with β coefficients ranging from 0.15 to 0.20 and p-values less than 0.001, indicating that higher fibrinogen levels correlate with longer hospital stays. Analyzing the data categorically, patients in the highest quartile (Q6, > 267 mg/dL) showed a substantial increase in length of stay, with β coefficients of 2.95 (p < 0.001) in Model 1 and 3.19 (p < 0.001) in Model 2, suggesting a significant impact of elevated fibrinogen levels on hospital duration. In contrast, patients in lower quartiles (Q1 to Q5) did not reveal significant differences in length of stay compared to the reference group (Q1, ≤ 155 mg/dL), with p-values exceeding 0.05 across all models. The trend across quartiles displayed statistical significance (p for trend < 0.001), reinforcing the relationship between higher fibrinogen levels and longer hospital stays. Lastly, multiple imputation analyses addressed missing data, and logistic regression on imputed datasets confirmed the stability of the results (Table S3).
Discussion
This study is, to our knowledge, the first retrospective investigation examining the association between fibrinogen levels and all-cause mortality in female patients undergoing CABG. Our Cox regression analysis reveals that both low and high fibrinogen levels correlate with an elevated risk of long-term mortality. Further validation through RCS analysis demonstrated a U-shaped relationship between fibrinogen levels and one-year mortality, suggesting that exceeding a certain fibrinogen threshold is associated with a higher likelihood of mortality. These results underscore the prognostic significance of fibrinogen as a biomarker for adverse outcomes in this high-risk population, particularly among women, who have historically been underrepresented in cardiovascular surgical research. Our findings are consistent with previous evidence linking fibrinogen to the pathophysiology of postoperative complications while extending existing knowledge by emphasizing sex-specific associations that may inform tailored risk stratification and therapeutic strategies.
In recent years, the gender disparities in outcomes following CABG have received increasing attention. A meta-analysis of 84 observational studies involving nearly one million patients highlighted that women (n = 224,340) face a significantly higher risk of operative mortality and major adverse cardiac events compared to men26. Despite improvements in CABG outcomes, this gender gap has persisted over time27,28. A large-scale study with over one million patients, including more than 300,000 women, confirmed that operative mortality remains disproportionately higher in women, with no observed reduction in this excess risk over the past decade5. Differences in anatomical, biological, and functional characteristics, including a greater burden of comorbidities and older age, are associated with increased mortality and likely contribute to this disparity29,30. Furthermore, the pathophysiology of ischemic heart disease varies significantly between men and women31,32. Given these factors, it is essential to consider women as a distinct group and to further explore the determinants of CABG outcomes specific to this population5,6,7. Addressing these unique challenges is vital for enhancing postoperative outcomes for female CABG patients.
Fibrinogen, a crucial component of blood coagulation and an inflammatory marker, has been recognized as a key predictor of mortality, hospital length of stay, and graft failure in CABG patients20,21,22,33. Considering that CABG is among the most frequently performed cardiac surgeries, fibrinogen levels are likely to influence outcomes in female patients. However, research in this area remains limited, and our study aims to fill this gap. We are the first to investigate the relationship between serum fibrinogen levels and long-term mortality in women undergoing CABG, employing RCS functions to analyze the dose-response relationship. Our findings reveal a U-shaped association between serum fibrinogen levels and HRs for all-cause mortality, indicating that both elevated and reduced fibrinogen levels are linked to an increased risk of mortality. This highlights the importance of managing serum fibrinogen levels in the clinical care of female CABG patients.
Previous studies have explored various perioperative inflammatory markers, such as the Systemic Inflammatory Response Index (SIRI)34 and triglyceride-glucose index35, in relation to long-term survival after CABG. However, these markers can be costly, time-consuming, and difficult to obtain, often lacking sensitivity to outcomes. In contrast, our findings provide a novel perspective on the relationship between fibrinogen levels and CABG outcomes. As a readily accessible and inexpensive marker derived from routine tests, fibrinogen can be easily measured in most CABG patients. Given its significant association with outcomes, healthcare professionals can utilize fibrinogen levels to monitor coagulation and anticoagulant status in female CABG patients across various clinical settings.
While the precise mechanisms by which fibrinogen increases the risk of cardiovascular events are not fully elucidated, several potential explanations exist for the observed association between elevated fibrinogen levels and mortality risk. One possibility is that systemic inflammation stimulates the production and release of fibrinogen36. Inflammation is a key factor in the formation of atherosclerotic plaques10. Additionally, fibrinogen influences endothelial integrity and vascular permeability by binding to receptor ligands, recruiting leukocytes to the vessel wall, and inducing platelet aggregation and activation37. It also promotes smooth muscle cell proliferation and monocyte chemotaxis38. Elevated fibrinogen levels may lead to denser fibrin clots and impaired fibrinolysis, further exacerbating atherosclerosis39. As a marker of both inflammation and coagulation, fibrinogen may contribute to the increased all-cause mortality associated with coronary heart disease (CHD)40. Following CABG, multiple molecular pathways remain persistently activated, resulting in elevated inflammation, hemostasis, and oxidative stress41. Higher fibrinogen levels have been associated with worse postoperative pulmonary function decline42. While inflammation is essential for clearing infection and debris post-surgery, prolonged inflammation can result in tissue damage43.
This study benefits from national data, a large sample size, multiple outcomes, long-term follow-up, and robust statistical analyses. To our knowledge, it is the first to assess optimal early postoperative fibrinogen levels specifically for female patients undergoing CABG, thereby enhancing the understanding of managing this patient population. However, several limitations must be acknowledged. First, the retrospective, single-center design utilizing observational data from the MIMIC-IV database limits the ability to establish causality. Additionally, despite controlling for available confounders, the model may still be influenced by unmeasured factors. Third, while the MIMIC database provides ICU data, details on long-term medication use (e.g., antiplatelet agents, statins) and postoperative rehabilitation were not available, which may impact mortality risk. Finally, external validation in multi-center cohorts is necessary, particularly given the underrepresentation of racial and ethnic minorities in the MIMIC population.
Conclusions
In summary, our study reveals a U-shaped association between serum fibrinogen levels and mortality, indicating that both low and high fibrinogen levels are linked to increased overall mortality among female patients undergoing CABG. Future research should focus on assessing whether interventions aimed at lowering fibrinogen levels can enhance outcomes in high-risk female subgroups.
Data availability
The datasets used and analyzed during the current study are available from the corresponding author upon reasonable request. To obtain the application executable files, please contact the author Yuxuan Tang.
Abbreviations
- CABG:
-
Coronary artery bypass grafting
- MIMIC-IV:
-
Medical Information Mart for Intensive Care IV
- RCS:
-
Restricted cubic splines
- BMI:
-
Body mass index
- HR:
-
Hazard ratio
- CIs:
-
Confidence intervals
- CPB:
-
Cardiopulmonary bypass
- ICU:
-
Intensive care unit
- BIDMC:
-
Beth Israel Deaconess Medical Center
- CITI:
-
Collaborative Institutional Training Initiative
- IRB:
-
Institutional Review Board
- BIDMC:
-
Beth Israel Deaconess Medical Center
- SQL:
-
Structured Query Language
- ABPS:
-
Arterial systolic pressure
- ABPD:
-
Arterial diastolic pressure
- WBC:
-
White blood cell
- RBC:
-
Red blood cell
- SOFA:
-
Sequential Organ Failure Assessment
- APS III:
-
Acute Physiology and Chronic Health Evaluation III
- SAPS II:
-
Simplified Acute Physiology Score II
- GCS:
-
Glasgow Coma Scale
- CHARLSON:
-
Charlson Comorbidity Index
- SIRI:
-
Systemic Inflammatory Response Index
- CHD:
-
Coronary heart disease
References
LaPar, D. J. et al. Primary payer status is associated with mortality and resource utilization for coronary artery bypass grafting. Circulation 126 (11 Suppl 1), S132–S139 (2012).
Fihn, S. D. et al. ACC/AHA/AATS/PCNA/SCAI/STS focused update of the guideline for the diagnosis and management of patients with stable ischemic heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines, and the American Association for Thoracic Surgery, Preventive Cardiovascular Nurses Association, Society for Cardiovascular Angiography and Interventions, and Society of Thoracic Surgeons. J. Am. Coll. Cardiol. 64(18), 1929–1949. (2014).
Ayad, S. et al. Hepatocyte growth factor mimetic ANG-3777 for cardiac Surgery-Associated acute kidney injury. Kidney Int. Rep. 5 (12), 2325–2332 (2020).
Kennedy, J. W. et al. Clinical and angiographic predictors of operative mortality from the collaborative study in coronary artery surgery (CASS). Circulation 63 (4), 793–802 (1981).
Gaudino, M. et al. Operative outcomes of women undergoing coronary artery bypass surgery in the US, 2011 to 2020. JAMA Surg. 158 (5), 494–502 (2023).
Pölzl, L. et al. Sex-Specific Troponin and Creatine Kinase Thresholds after Coronary Bypass Surgery (Ann Thorac Surg, 2024).
Robinson, N. B. et al. Coronary artery bypass with single versus multiple arterial grafts in women: A meta-analysis. J. Thorac. Cardiovasc. Surg. 165 (3), 1093–1098 (2023).
Spadafora, L. et al. Appraising features and outlook of women and men discharged after an acute coronary syndrome: evidence from the 23,700-patient PRAISE international registry. Panminerva Med. 65 (4), 454–460 (2023).
Lawton, J. Improving outcomes for women after coronary artery bypass grafting. JAMA Netw. Open. 7 (6), e2414287 (2024).
Hansson, G. K. Inflammation, atherosclerosis, and coronary artery disease. N Engl. J. Med. 352 (16), 1685–1695 (2005).
Zakynthinos, E. & Pappa, N. Inflammatory biomarkers in coronary artery disease. J. Cardiol. 53 (3), 317–333 (2009).
Kaptoge, S. et al. C-reactive protein, fibrinogen, and cardiovascular disease prediction. N Engl. J. Med. 367 (14), 1310–1320 (2012).
Feng, D. et al. Platelet glycoprotein IIIa Pl(a) polymorphism, fibrinogen, and platelet aggregability: the Framingham heart study. Circulation 104 (2), 140–144 (2001).
Tousoulis, D. et al. Fibrinogen and cardiovascular disease: genetics and biomarkers. Blood Rev. 25 (6), 239–245 (2011).
Meng, Z., Zhao, Y. & He, Y. Fibrinogen Level Predicts Outcomes in Critically Ill Patients with Acute Exacerbation of Chronic Heart Failure. Dis Markers, 2021: p. 6639393. (2021).
Ma, J. et al. A prospective study of fibrinogen and risk of myocardial infarction in the physicians’ health study. J. Am. Coll. Cardiol. 33 (5), 1347–1352 (1999).
Danesh, J. et al. Plasma fibrinogen level and the risk of major cardiovascular diseases and nonvascular mortality: an individual participant meta-analysis. Jama 294 (14), 1799–1809 (2005).
Xie, E. et al. High fibrinogen levels with diabetes mellitus are associated with All-Cause and cardiovascular mortality in patients with End-Stage renal disease and acute coronary syndrome. J. Inflamm. Res. 17, 7409–7422 (2024).
Lassé, M. et al. Fibrinogen and hemoglobin predict near future cardiovascular events in asymptomatic individuals. Sci. Rep. 11 (1), 4605 (2021).
Völzke, H. et al. Preoperative plasma fibrinogen levels predict mortality after coronary artery bypass grafting. Thromb. Haemost. 89 (5), 885–891 (2003).
Huang, C. et al. Fibrinogen is an independent preoperative predictor of hospital length of stay among patients undergoing coronary artery bypass grafting. J. Cardiothorac. Surg. 18 (1), 112 (2023).
Yanagawa, B. et al. Clinical, biochemical, and genetic predictors of coronary artery bypass graft failure. J. Thorac. Cardiovasc. Surg. 148 (2), 515–520e2 (2014).
Momeni, M. et al. Fibrinogen concentration significantly decreases after on-pump versus off-pump coronary artery bypass surgery: a systematic point-of-care ROTEM analysis. J. Cardiothorac. Vasc Anesth. 27 (1), 5–11 (2013).
Johnson, A. E. W. et al. MIMIC-IV, a freely accessible electronic health record dataset. Sci. Data. 10 (1), 1 (2023).
Sterne, J. A. et al. Multiple imputation for missing data in epidemiological and clinical research: potential and pitfalls. Bmj 338, b2393 (2009).
Bryce Robinson, N. et al. Sex differences in outcomes following coronary artery bypass grafting: a meta-analysis. Interact. Cardiovasc. Thorac. Surg. 33 (6), 841–847 (2021).
Alkhouli, M. et al. Trends in characteristics and outcomes of patients undergoing coronary revascularization in the united States, 2003–2016. JAMA Netw. Open. 3 (2), e1921326 (2020).
ElBardissi, A. W. et al. Trends in isolated coronary artery bypass grafting: an analysis of the society of thoracic surgeons adult cardiac surgery database. J. Thorac. Cardiovasc. Surg. 143 (2), 273–281 (2012).
Lemaire, A. et al. The impact of age on outcomes of coronary artery bypass grafting. J. Cardiothorac. Surg. 15 (1), 158 (2020).
Enumah, Z. O. et al. Persistent racial and sex disparities in outcomes after coronary artery bypass surgery: a retrospective clinical registry review in the drug-eluting stent era. Ann. Surg. 272 (4), 660–667 (2020).
Wenger, N. K. Women and coronary heart disease: a century after herrick: understudied, underdiagnosed, and undertreated. Circulation 126 (5), 604–611 (2012).
Aggarwal, N. R. et al. Sex differences in ischemic heart disease: advances, obstacles, and next steps. Circ. Cardiovasc. Qual. Outcomes. 11 (2), e004437 (2018).
Williams, S. R. et al. Shared genetic susceptibility of vascular-related biomarkers with ischemic and recurrent stroke. Neurology 86 (4), 351–359 (2016).
Urbanowicz, T. et al. Neutrophil Counts, Neutrophil-to-Lymphocyte Ratio, and Systemic Inflammatory Response Index (SIRI) predict mortality after off-pump coronary artery bypass surgery. Cells. 11(7). (2022).
Wu, Z. et al. Triglyceride-glucose index in the prediction of adverse cardiovascular events in patients without diabetes mellitus after coronary artery bypass grafting: a multicenter retrospective cohort study. Cardiovasc. Diabetol. 22 (1), 230 (2023).
Gabay, C. & Kushner, I. Acute-phase proteins and other systemic responses to inflammation. N Engl. J. Med. 340 (6), 448–454 (1999).
Pretorius, E. Platelets as potent signaling entities in type 2 diabetes mellitus. Trends Endocrinol. Metab. 30 (8), 532–545 (2019).
Naito, M. et al. Smooth muscle cell outgrowth stimulated by fibrin degradation products. The potential role of fibrin fragment E in restenosis and atherogenesis. Thromb. Res. 98 (2), 165–174 (2000).
Undas, A. Fibrin clot properties and their modulation in thrombotic disorders. Thromb. Haemost. 112 (1), 32–42 (2014).
Hale, L. et al. Fibrinogen May mediate the association between long sleep duration and coronary heart disease. J. Sleep. Res. 22 (3), 305–314 (2013).
Parolari, A. et al. Biomarkers in coronary artery bypass surgery: ready for prime time and outcome prediction? Front. Cardiovasc. Med. 2, 39 (2015).
Salzmann, S. et al. IL-8 and CRP moderate the effects of preoperative psychological interventions on postoperative long-term outcomes 6 months after CABG surgery - The randomized controlled PSY-HEART trial. Brain Behav. Immun. 91, 202–211 (2021).
Zhao, R. et al. Inflammation in chronic wounds. Int. J. Mol. Sci., 17(12). (2016).
Acknowledgements
We appreciate Dr. Jie Liu of the Department of Vascular and Endovascular Surgery, Chinese PLA General Hospital for statistics, study deign consultations and editing the manuscript.
Funding
The study has no foundation.
Author information
Authors and Affiliations
Contributions
XJY contributed as First authors of this manuscript. MXH and RZ were responsible for the concept and design of the study. KZ explain the analysis. RZ and KZ are responsible for data recovery. JXY and TYX are responsible for revising the manuscript. YXT is the primary corresponding author. All authors critically revised the important intellectual content of the paper and approved the final draft.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
The establishment of this database was approved by the Massachusetts Institute of Technology (Cambridge, MA, USA) and Beth Israel Deaconess Medical Center (Boston, MA, USA), and informed consents were exempted due to all patients’ data were anonymized before the data were obtained. We also complied with all relevant ethical regulations regarding the use of the data in our study. All reports adhered to the guidelines for Strengthening the Reporting of Observational Studies in Epidemiology and the Declaration of Helsinki.
Consent to publish
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Yao, X., Zhang, K., Zhang, R. et al. U shaped association between fibrinogen and one year mortality in women undergoing coronary artery bypass grafting. Sci Rep 16, 340 (2026). https://doi.org/10.1038/s41598-025-29837-y
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-29837-y
