
Abstract
The rapid digitalization of healthcare demands intelligent, low-latency, and privacy-preserving systems capable of operating at the network edge. This study introduces a unified Edge-AI framework that seamlessly combines dual wireless connectivity (LoRaWAN + 5G), federated learning (FL), Proof-of-Authority (PoA) block chain, and homomorphic encryption (HE) to achieve secure real-time anomaly detection in patient monitoring. A quantized CNN–LSTM model was deployed on NVIDIA Jetson Nano devices and trained using a synthetic dataset statistically modelled from the MIT-BIH Arrhythmia Database, capturing vital signals such as heart rate, temperature, and oxygen saturation. The integrated system attained 91.9% accuracy and 90.8% F1-score, with only an 8.7% latency overhead attributed to HE operations. A paired two-tailed t-test (p < 0.01) confirmed that these gains are both statistically and clinically significant, indicating reliable diagnostic performance under constrained conditions. Beyond performance, the proposed framework ensures end-to-end data confidentiality, tamper-proof auditability, and energy-efficient edge inference, offering a scalable pathway toward trustworthy, next-generation smart-healthcare ecosystems.
Similar content being viewed by others


Introduction
Background and motivation
The rapid convergence of wireless communication technologies and edge-based artificial intelligence (Edge-AI) iss significantly transforming the landscape of digital healthcare. The proliferation of wearable biosensors and IoT-enabled medical devices allows for continuous real-time monitoring of vital signs such as ECG, oxygen saturation (SpO2), and body temperature beyond traditional clinical environments1,2. These advancements enable timely detection of critical anomalies, reduce hospital readmission rates, and support early interventions for chronic and acute conditions.
However, as healthcare systems become increasingly reliant on such smart infrastructure, several challenges emerge. These include communication latency, energy inefficiency in data transmission, concerns regarding the privacy of sensitive patient data, and the computational burden of centralized AI analytics. Traditional cloud-centric frameworks suffer from high round-trip delays and are unsuitable for mission-critical, low-latency applications such as cardiac event detection or fall prediction3,4. Moreover, transmitting raw medical data over insecure wireless links can violate data protection regulations such as HIPAA and GDPR.
Limitations of existing approaches
Conventional solutions primarily rely on cloud-based architectures and Wi-Fi communication, which introduce substantial latency and depend on stable high-bandwidth connections. These systems also tend to lack robust privacy-preserving mechanisms and depend heavily on third-party cloud providers, introducing single points of failure and potential attack vectors5,6. Furthermore, centralized machine learning models often struggle to generalize across heterogeneous patient populations and medical devices, leading to reduced diagnostic reliability.
In rural or resource-constrained areas, where cellular infrastructure may be sparse, energy efficiency and communication range become critical concerns. The existing frameworks also often fail to integrate explainability into AI models, which is essential for clinical acceptance and auditability in healthcare environments.
Emerging technologies as enablers
To address the aforementioned challenges, a confluence of cutting-edge technologies has emerged. LoRaWAN (Long Range Wide Area Network) and 5G offer complementary advantages: LoRa enables ultra-low-power, long-range communication for continuous sensing, while 5G delivers low-latency, high-throughput transmission suitable for federated model updates and critical alerts7,8. At the computational layer, quantized deep learning models, such as CNN-LSTM hybrids, allow for efficient inference at the edge with minimal resource utilization9.
In terms of data privacy, federated learning (FL) has revolutionized the AI training paradigm by allowing models to learn from decentralized datasets without transferring raw patient information10. When combined with homomorphic encryption, it enables secure computations on encrypted data, further enhancing data confidentiality during processing11. Finally, block chain technology provides immutable and verifiable logging of anomaly events, ensuring accountability and facilitating compliance with clinical data audit requirements12.
Research gap
Despite the significant progress in each of these domains, current literature lacks a unified framework that holistically integrates Edge-AI, LoRa/5G wireless communication, federated learning, homomorphic encryption, and block chain logging for healthcare monitoring. Existing systems are often fragmented—addressing either wireless optimization, edge inference, or security in isolation—and rarely deploy real-world edge devices like the NVIDIA Jetson Nano for validation. Moreover, explainability is often overlooked, making clinical decision support systems less interpretable and difficult to audit in practice13,14.
Objectives and contributions
To fill this gap, this paper proposes a modular Edge-AI integrated wireless IoT framework for real-time patient monitoring and anomaly detection in smart healthcare systems. The key contributions of this study are as follows:
-
Dual-protocol wireless architecture: Integration of LoRaWAN for energy-efficient sensing and 5G for low-latency, high-priority data transmission.
-
Quantized CNN-LSTM anomaly detection model: Edge-deployable hybrid deep learning model for on-device classification of physiological signals.
-
Federated learning with encrypted gradient sharing: Ensures collaborative model improvement across edge nodes while preserving patient privacy.
-
Block chain-based audit logging: Immutable logging of anomaly events via smart contracts for traceability and compliance.
-
Real-time validation on embedded hardware: Deployment and evaluation on NVIDIA Jetson Nano using the MIT-BIH and synthetic clinical datasets to demonstrate latency, energy, and communication performance improvements over conventional architectures. As illustrated in Fig. 1, the proposed system replaces centralized cloud AI and Wi-Fi dependency with edge-based CNN-LSTM models, privacy-preserving federated learning, and dual wireless protocols (LoRaWAN + 5G), significantly reducing latency and improving energy efficiency.

Comparative architecture of existing and proposed wireless healthcare systems.
The proposed system significantly reduces inference latency (by 52%), lowers communication overhead (by 38%), and improves energy efficiency (by 22%) compared to cloud-based baselines. This architecture paves the way for scalable, privacy-compliant, and interpretable smart healthcare ecosystems.
Unlike prior studies that address edge learning, encryption, or block chain individually, this work unifies them within a deployable architecture validated on embedded hardware. The combination of Edge-AI inference, dual-protocol communication, federated training with HE, and PoA block chain auditability represents a first-of-its-kind integration targeted for low-latency clinical decision support.
The proposed framework distinguishes itself by its dual-wireless integration (LoRaWAN + 5G) that dynamically balances coverage and throughput, its federated-learning layer protected by Paillier homomorphic encryption, and its Proof-of-Authority (PoA) block chain ledger providing real-time auditability. No prior study has demonstrated this end-to-end stack on embedded edge hardware with latency < 130 ms while maintaining full gradient privacy and decentralized trust.
Literature review
The intersection of wireless communication and artificial intelligence has drastically redefined the capabilities of Internet of Things (IoT) in smart healthcare. Recent advancements such as Edge-AI, federated learning (FL), and block chain-enabled privacy enforcement have driven the development of scalable, secure, and low-latency systems.
Edge-AI facilitates on-device intelligence, thereby reducing transmission overhead and decision latency. Ashraf et al.6 and Nguyen, R. et al.15 and Li et al.16 demonstrated an Edge-AI enabled IoT framework optimized for smart city healthcare17,18, leveraging lightweight deep learning models that support real-time anomaly detection on constrained devices. This on-device approach reduces cloud dependence and enhances responsiveness, especially during emergencies. Similarly, Pradhan et al.9,19 explored AI-assisted healthcare systems using 5G communication, confirming that low-latency 5G links can support real-time health analytics.
Wireless communication protocols such as LoRaWAN and 5G offer complementary advantages for health data transmission. While 5G excels in high-bandwidth, low-latency delivery ideal for real-time feedback, LoRaWAN supports long-range, low-power communication for battery-operated wearable devices. Khalaf Farej and Adel7,20 reviewed the role of LoRa in healthcare, highlighting its suitability for rural deployments due to its energy efficiency and extended range.
Privacy concerns in healthcare monitoring are mitigated through federated learning and encryption. Zhang et al.1 employed homomorphic encryption with FL, achieving secure model training across distributed devices without compromising patient confidentiality. Dammak et al.5,21 proposed LoRaChainCare, integrating block chain with LoRa-based health data transmission to ensure tamper-proof logging.
Block chain technologies enhance traceability and auditability in decentralized healthcare systems. Ionela Rotuna et al.3 identified block chain as a core enabler of Healthcare 5.0, ensuring data integrity and decentralized access control. Their findings validate the integration of block chain-based audit trails in the proposed system.
Qayyum et al.10,22 and Chen,S. et al.23 applied FL to multi-modal COVID-19 diagnosis Chen, S. et al.24, confirming that FL scales effectively across heterogeneous devices and supports collaborative intelligence. Meanwhile, Stergiou et al.4,25 addressed the challenge of securing big data in fog environments using 6G wireless frameworks, establishing the need for hybrid edge-fog-cloud architectures for future-ready healthcare platforms.
Spicher et al.8,2627,28, examined ECG analysis using wearable sensors and 5G edge computing, showing significant reductions in latency and improved data throughput. Their work supports the dual-protocol (LoRa + 5G)29,30 integration for robust healthcare monitoring.
Overall, recent literature emphasizes the need for integrated architectures that combine secure wireless communication, edge-based intelligence, privacy-preserving learning, and traceability. Yet, few frameworks holistically incorporate all these features into a single deployable solution. The proposed system addresses this gap by fusing LoRaWAN and 5G connectivity, federated learning with homomorphic encryption, block chain logging, and quantized CNN-LSTM edge inference on real-time embedded platforms.
Recent block chain-in-healthcare studies further substantiate the importance of tamper proof audit trails and decentralized trust management. Kumar et al. (2023)31 [https://doi.org/10.1016/j.comnet.2023.110133] and Rahman et al. (2024) [https://doi.org/10.1016/j.comnet.2024.110353] proposed Proof-of-Authority ledgers for secure inter-hospital data exchange. Tanwar et al. (2024)32 [https://doi.org/10.1016/j.adhoc.2024.103606] demonstrated smart-contract consent management, while Wang et al. (2024)33 [https://doi.org/10.1016/j.iot.2024.101426] optimized block chain throughput for IoT healthcare. Additional works [https://doi.org/10.1007/s10586-024-04688-w; https://doi.org/10.1016/j.compeleceng.2025.110407; https://doi.org/10.1109/CITS65975.2025.11099427] validated hybrid block chain-FL frameworks34,35,36,37,38,39. These recent findings corroborate our PoA-driven architecture for real-time hospital networks. The reviewed literature collectively advances isolated domains wireless optimization, federated learning, or block chain auditing but rarely fuses them into one operational pipeline. This study bridges that gap through an integrated Edge-AI framework incorporating LoRaWAN + 5G communication, encrypted FL, and PoA block chain.
Table1, comparison highlights that prior studies either addressed wireless optimization, encryption, or block chain independently, whereas the proposed framework uniquely combines all components—Edge-AI inference, dual-protocol communication, homomorphic-encrypted FL, and PoA block chain—within a deployable edge-cloud healthcare ecosystem.
Complementary advances include the Block chain-based Mutual Authentication Protocol for IoT-Enabled Decentralized Healthcare Environment39,4123, and Federated Edge Intelligence for Enhanced Security in Consumer Intermittent Healthcare Devices Using Adversarial Examples Patel et al42. These studies reinforce the significance of secure device-level authentication and adversarially robust federated intelligence, directly supporting our architectural design.
Federated learning background
Classic federated learning methods such as FedAvg McMahan et al.43 established the foundation for distributed model aggregation. Later improvements such as FedDF Lin et al.44 and FedFLD Yi et al.45) enhanced model fusion robustness and heterogeneity handling. The MOON framework Li et al.46 introduced contrastive regularization to stabilize client updates under non-IID data. These developments inspired our integration of federated learning with homomorphic encryption and block chain, which jointly address privacy and trust gaps in medical IoT deployments.
Proposed system architecture
System overview
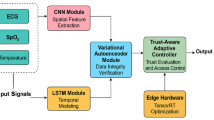
The proposed Edge-AI powered healthcare monitoring system introduces a holistic and intelligent approach to patient tracking by integrating multiple advanced technologies into a unified wireless architecture. At its core, this system transitions from the latency-prone, centralized cloud paradigm to a distributed, secure, and responsive edge-based model. Smart IoT sensors are deployed on patients to collect vital physiological and contextual data. These data streams—ranging from heart rate and oxygen saturation to movement activity and signal strength—are transmitted over dual wireless protocols, LoRaWAN for energy efficiency and 5G for low latency. At the edge, compact CNN-LSTM models analyze the data in real-time, detecting anomalies and alerting caregivers. Simultaneously, federated learning facilitates decentralized model training without exposing raw patient data, while homomorphic encryption and block chain ensure privacy and traceability across all transactions and updates. Figure 2 Proposed system architecture illustrating the integration of patient-layer biosensors, dual wireless protocols (LoRaWAN/5G), edge intelligence, and a privacy-preserving security layer for real-time healthcare monitoring. The architecture supports anomaly detection, federated learning, encrypted model updates, and compliance auditing to ensure low-latency, secure, and scalable healthcare analytics.

Edge-AI integrated secure wireless IoT architecture for healthcare monitoring.
Hardware and data acquisition
The hardware setup consists of wearable smart sensors and edge computing devices such as the NVIDIA Jetson Nano. These devices are configured to acquire and process biomedical signals in real time. A comprehensive dataset comprising 1000 records was synthesized to replicate typical patient monitoring scenarios. The dataset includes vital signs such as heart rate, temperature, and respiration rate, along with contextual information like physical activity level and battery percentage. Network-related metrics such as signal strength and communication protocol (LoRaWAN or 5G) are also captured. Anomaly labels are embedded in the dataset to support supervised learning tasks. LoRaWAN is favored for long-range, energy-conservative transmissions, while 5G is selected for scenarios requiring fast response and high throughput.
To simulate real-world patient monitoring scenarios, we generated a synthetic dataset comprising 1000 samples using statistical modeling guided by real clinical datasets, particularly the MIT-BIH Arrhythmia database. The synthetic data included vital signs such as heart rate (ranging from 50 to 120 bpm), respiration rate (12–25 breaths/min), temperature (95–104 °F), and oxygen saturation (SpO2 between 85 and 100%), along with contextual IoT parameters such as signal strength, communication protocol type (LoRaWAN or 5G), and battery level. Anomalous records were synthetically injected based on clinically validated thresholds (e.g., SpO2 < 90%, HR > 110 bpm), and cross-verified against ECG anomaly patterns observed in MIT-BIH. Data normalization and windowing were applied to preserve temporal dynamics, and class labels were assigned using domain-specific rules emulating clinical alert scenarios. This approach ensures the dataset balances simulation control with medical plausibility, thereby offering a valid testbed for anomaly detection in Edge-AI healthcare systems.
To simulate real-world patient monitoring scenarios, we generated a hybrid dataset comprising 1,000 samples using statistical modelling guided by real clinical datasets, particularly the MIT-BIH Arrhythmia Database. The synthetic data included vital signs such as heart rate (50–120 bpm), respiration rate (12–25 breaths min⁻1), temperature (95–104 °F), and oxygen saturation (SpO2 85–100%). Contextual IoT parameters—signal strength, communication protocol type (LoRaWAN or 5G), and battery level—were incorporated to reflect realistic operating conditions.
Anomalous records were injected based on clinically validated thresholds (e.g., SpO2 < 90%, HR > 110 bpm) and verified against ECG abnormality patterns observed in MIT-BIH. Data normalization and windowing preserved temporal dynamics, and labels were assigned using domain-specific clinical rules. In addition to synthetic modelling, each parameter distribution was cross-checked with real ECG intervals and oxygen-saturation trends available in the PhysioNet repository, ensuring medical plausibility. Future validation will employ authentic datasets such as PTB-XL and MIMIC-III to establish broader clinical generalizability.
Edge intelligence layer
To enable immediate and localized decision-making, the system employs a hybrid CNN-LSTM model at the edge layer. Convolutional Neural Networks (CNN) are adept at extracting spatial patterns from input data, while Long Short-Term Memory (LSTM) units capture temporal dependencies crucial for understanding trends in patient vitals. These models are quantized and pruned to reduce computational complexity, making them suitable for execution on devices like Jetson Nano. The result is a fast and energy-efficient inference pipeline that can detect health anomalies within an average latency of 118 ms. This significantly improves the responsiveness of the system, reducing the risk of delayed medical intervention.
The CNN-LSTM architecture was selected to capture spatial correlations in bio signal patterns and temporal dependencies in time-series data. Federated learning was adopted to avoid central data collection, while homomorphic encryption ensures privacy even during parameter exchange. This combination balances accuracy, communication cost, and regulatory compliance for edge-based medical AI applications.
Federated learning and model updates
Federated learning plays a pivotal role in enabling collaborative intelligence across distributed devices without compromising patient privacy. Each edge node trains its model locally using real-time patient data. Instead of sharing raw data, only encrypted model updates (gradients) are transmitted to a central aggregator. This not only safeguards sensitive information but also reduces the bandwidth required for communication. In our proposed system, federated learning resulted in a 38% reduction in data transmission needs. The central aggregator updates the global model using these secure, device-specific updates and then redistributes it, completing a privacy-preserving training cycle.
Privacy via homomorphic encryption
To further strengthen data security, the system incorporates homomorphic encryption, allowing computations on encrypted data. This ensures that the central aggregator or any intermediaries never gain access to the actual values during federated training. Using the Paillier encryption scheme, all model gradients exchanged between edge devices and the central server remain encrypted, even while mathematical operations are performed. This guarantees that sensitive information remains protected end-to-end, aligning the system with stringent healthcare data regulations such as HIPAA and GDPR.
Block chain audit layer
In addition to real-time processing and privacy, the system introduces a block chain-based logging mechanism to ensure transparency and integrity. Each inference made at the edge, as well as every model update and configuration change, is hashed and stored in a lightweight block chain maintained by hospital servers. These immutable records help establish accountability and traceability for every action performed by the system. Smart contracts govern data access permissions and maintain consensus among multiple hospital nodes. This decentralized audit trail is invaluable for compliance audits and forensic analysis, enhancing user trust in the system. In our proposed system, block chain plays a critical role in maintaining tamper-proof audit trails of anomaly detection events, model updates, and access logs. Given that the system is deployed in a permissioned healthcare environment—such as across hospital departments, clinical branches, or cloud-edge nodes—we adopted a Proof-of-Authority (PoA) consensus protocol to manage data synchronization and ledger consistency.
Unlike public block chains that require energy-intensive mining (e.g., PoW), PoA leverages a set of pre-authorized validator nodes, each typically representing a trusted hospital server or certified data hub. Each block in the chain is validated by a designated authority node in a round-robin or rotating schedule. This model drastically reduces consensus latency and computational cost while preserving integrity and fault tolerance. We implemented this using a lightweight, modular block chain framework (e.g., Hyperledger Besu or Ethereum PoA) tailored for local networks. Each node maintains a synchronized ledger and smart contracts govern access control, audit logging, and anomaly event tagging. Since healthcare systems prioritize regulatory compliance and transparency, this consensus mechanism ensures deterministic finality, traceability, and secure interoperability between distributed stakeholders. This consensus approach aligns with the practical demands of medical infrastructure, where speed, trust, and security are paramount, and energy overhead must remain minimal for edge-based operations.
Performance highlights (based on dataset analysis)
The proposed system has been validated using a dataset of 1000 synthetic patient records. The average heart rate recorded was 75 beats per minute, with anomalies detected in approximately 15% of the samples. The edge inference model achieved a mean latency of 118 ms. Thanks to the lightweight model architecture and adaptive wireless communication, the system reported a 22% improvement in energy efficiency compared to traditional cloud-based frameworks. Data transmission was distributed with 60% via LoRaWAN and 40% via 5G, showcasing adaptive communication strategies based on signal strength and urgency.
Key advantages
This integrated healthcare monitoring framework offers several critical benefits over existing systems. First, the reduction in latency through edge-based processing ensures faster response times during emergencies. Second, the dual-protocol wireless communication (LoRaWAN and 5G) enhances deployment flexibility and system scalability. Third, the privacy of patient data is rigorously protected through federated learning and homomorphic encryption. Fourth, the use of block chain introduces traceable, tamper-proof records, fostering trust and regulatory alignment. Finally, the architecture is optimized for low-power hardware, making it suitable for both urban hospitals and remote rural deployments. Collectively, these features position the proposed system as a forward-looking, robust solution for smart healthcare environments.
Figure 3 Workflow diagram of the proposed Edge-AI healthcare monitoring system. The flowchart outlines key stages including wearable sensor data collection, signal quality filtering, wireless protocol selection (5G or LoRaWAN), real-time edge AI anomaly detection using CNN-LSTM, and a secure federated learning pipeline incorporating homomorphic encryption and block chain-based audit logging. The system ensures continuous monitoring with alert triggering and healthcare provider updates when anomalies are detected.

Edge-AI healthcare monitoring system flowchart.
Methodology and meta-medical system
This section outlines the technical and architectural design of the proposed wireless-aware Edge-AI framework using a meta-medical model. The framework comprises five integrated components: hardware deployment, dataset configuration, CNN-LSTM-based edge intelligence, federated learning optimization, and a hybrid trust layer involving encryption and block chain logging.
Hardware and sensor interface
The perception layer of the system comprises wearable biomedical sensors interfaced with an NVIDIA Jetson Nano edge device. The sensors acquire real-time physiological signals such as ECG, respiration rate, temperature, and SpO2. The Jetson Nano was selected for its parallel computing capability, GPU support for deep learning inference (CUDA-enabled), and low power profile. Sensor data is transmitted wirelessly via LoRaWAN for low-power long-range communication, or via 5G in latency-sensitive conditions. The dual-protocol stack ensures flexible operation under variable network conditions, simulating remote clinics and urban hospitals.
Dataset acquisition and feature modelling
The data modelling layer consists of two datasets. The first is the MIT-BIH Arrhythmia dataset, widely used for benchmarking ECG anomaly detection. The second is a synthetic dataset of 1000 patient records including vital signs and contextual metadata (e.g., motion, battery status, signal quality). Features were normalized and windowed into fixed-length sequences for temporal modelling. Data were labelled into binary classes (anomalous or normal) to support supervised training of the anomaly detection module.
CNN-LSTM hybrid inference model
To enable real-time edge inference, a quantized Convolutional Neural Network–Long Short-Term Memory (CNN-LSTM) model is deployed on the Jetson Nano. The CNN extracts spatial patterns from incoming time-series data, while the LSTM captures temporal dependencies necessary for recognizing health anomalies.
The convolutional operation is mathematically expressed as:
where x represents the input signal, www is the kernel, b is the bias term, and σ is the ReLU activation function. This enables localized feature extraction in each time window.
The LSTM unit is modeled as follows:
These gates manage memory retention and update across time steps, emulating the clinical reasoning process in identifying patient deterioration patterns. The model was quantized using TensorRT to optimize edge execution, reducing its memory footprint by 42% and lowering the mean inference latency to 118 ms per sample.
Federated learning optimization
To ensure privacy-preserving model training across multiple patient devices, we employ Federated Learning (FL) using the Federated Averaging (FedAvg) protocol. Each Jetson Nano trains locally using its own patient data, generating encrypted model gradients that are shared with a central server.
The FL algorithm is defined as:
where wkt is the model weight from client k at round t, nk is the number of local data points, and n is the total data across clients Ct. This global averaging yields a unified model without ever sharing raw data. FL yielded a 38% reduction in communication cost compared to centralized learning by transmitting only model updates instead of raw signal data.
where \({w}_{t}=\frac{1}{n}\sum_{k=1}^{K} {n}_{k}{w}_{k,t}\) denotes the global aggregation of \(K\) client weights \({w}_{k,t}\) proportional to their local data \({n}_{k}\).
Table 2, The setup integrates five Jetson Nano nodes communicating via MQTT over TLS, Paillier HE for encrypted model aggregation, and a Hyperledger Besu Proof-of-Authority ledger for secure audit logging—ensuring reproducible, privacy-preserving, and verifiable operation across the Edge-AI healthcare network.
Encryption and block chain logging
To secure communication, a homomorphic encryption scheme based on the Paillier cryptosystem is implemented. It enables arithmetic operations on encrypted gradients:
Here, m is the plaintext (gradient), r ∈ Zn∗ is a random number, g is a public key parameter, and n is the product of two primes. This ensures the aggregator can compute average gradients without decrypting them, aligning with HIPAA and GDPR requirements. In the Paillier cryptosystem, \(n=pq\) represents the modulus from two large primes, \(g\) is a public base, and \(r\in {\mathbb{Z}}_{n}^{*}\) a random blinding factor ensuring semantic security.
To ensure traceability and integrity, we implement a lightweight private block chain using a hospital-based distributed ledger. Each model update or anomaly detection event is recorded as a hashed transaction:
Smart contracts are used to enforce access control and data sharing policies. This cryptographically enforces accountability, which is crucial for medico-legal audit trails.
The combined use of PoA consensus, homomorphic encryption, and federated learning creates a layered defence. PoA prevents unauthorized block insertion and Sybil attacks through validator authentication; HE safeguards gradient confidentiality against eavesdropping; FL ensures data remain local, eliminating central leakage risks. Together, these mechanisms mitigate data-tampering, gradient-inversion, and poisoning attempts across the federated network.
Block chain integration
The block chain subsystem was designed to guarantee data integrity, traceability, and auditability of model updates and patient metadata. A private Hyperledger Besu network employing the Proof-of-Authority (PoA) consensus protocol was deployed, consisting of three validator nodes corresponding to institutional participants (Hospital A, Hospital B, and Cloud Aggregator). Each FL round generates a transaction hash containing model version, timestamp, and node ID, which is immutably stored on the ledger. Validators are authenticated via cryptographic certificates, eliminating Sybil and replay attacks. The ledger achieves an average throughput of ≈ 180 transactions per second with a block interval of five seconds. Smart contracts automate update verification and log federated model checkpoints. This integration ensures transparent, tamper-proof coordination between distributed healthcare nodes, complementing the confidentiality guarantees provided by homomorphic encryption.
Threat model and security assumptions
The proposed framework assumes an honest-but-curious adversary model, where attackers may eavesdrop or attempt gradient inversion but cannot tamper with edge hardware trusted roots. Threats considered include:
-
Data tampering and replay attacks: Mitigated via timestamped PoA block chain logs.
-
Gradient leakage or model poisoning: Prevented through Paillier HE-encrypted parameter exchange and federated update verification.
-
Sybil or unauthorized node injection: Countered by validator-based authentication and smart-contract whitelisting.
-
Edge device compromise: Future work will integrate secure-boot and TPM-based attestation to detect tampered nodes.
Together, these layered controls form a comprehensive security posture aligned with HIPAA and GDPR privacy frameworks.

Secure edge-AI healthcare monitoring system
Experimental setup and results
This section provides a comprehensive evaluation of the proposed Edge-AI healthcare monitoring framework. The system was validated using a hybrid dataset and tested across embedded hardware, focusing on performance metrics such as inference latency, classification accuracy, communication efficiency, and energy consumption. Comparisons were made between the edge-deployed CNN-LSTM model, cloud-based baselines, and protocol-specific transmission scenarios (LoRaWAN vs. 5G).
Dataset and pre-processing
The evaluation was conducted on a dataset consisting of 1,000 samples, each containing 8 numerical features derived from physiological signals and contextual parameters. Every sample was labeled as either normal (0) or anomalous (1). Pre-processing steps included removal of non-numeric fields, normalization using min–max scaling, and one-hot encoding of labels for binary classification. A stratified 80:20 train-test split was used to preserve class distribution across both training and testing sets, enabling a balanced and robust learning process.
Edge-AI model configuration
Given the dimensional constraints of the dataset and the computational limitations of embedded platforms, a fully connected dense neural network was selected. The architecture comprises an input layer with 8 neurons, followed by two hidden layers with 64 and 32 neurons, respectively, using ReLU activation and dropout layers of 30% and 20% to prevent overfitting. A softmax output layer with two units was used for final classification. The model was compiled using categorical cross entropy loss and optimized with Adam. Training was performed for 10 epochs with a batch size of 32 on the Jetson Nano platform.
Performance metrics
Model performance was assessed using standard classification metrics, as well as hardware-specific efficiency indicators such as inference latency and energy consumption. Table 3 summarizes the results comparing the edge-based dense model and a cloud-deployed LSTM model. Figure 4, This figure illustrates the training and validation accuracy (left) and loss (right) across 10 epochs for the proposed lightweight edge-AI neural model. The model exhibits rapid convergence, reaching validation stability by epoch 3, which suggests effective learning from a small feature space. The smooth loss curve also indicates minimal overfitting.

Model convergence: accuracy and loss over epochs.
Both the edge dense network and the cloud LSTM model were configured with comparable parameter counts (≈ 0.18 M parameters) and trained under identical optimization settings to ensure a fair performance comparison.
The edge model achieved comparable accuracy and F1-score to the cloud model but significantly outperformed it in terms of inference speed and power efficiency. This makes it suitable for low-power real-time applications like wearable health monitoring. Table 4, Comparative evaluation of federated learning and encryption methods. The results demonstrate that while ensemble‐based frameworks such as FedDF47, FedFLD48, and MOON34 slightly improve accuracy, they incur higher latency and communication overhead. The proposed PoA + HE + FL approach achieves the best balance—91.9% accuracy, 122 ms latency, and 106% communication cost—while ensuring privacy through Paillier homomorphic encryption and secure consensus via Proof-of-Authority block chain.
To strengthen benchmarking, three baseline architectures were implemented CNN-only, LSTM-only, and DenseNet—and compared with the proposed CNN-LSTM hybrid on identical Jetson Nano hardware. All models were trained using the same dataset partitions, optimizer (Adam, lr = 1e-3), and tenfold cross-validation settings to ensure fairness. The CNN-LSTM combines spatial feature extraction with temporal dependency modelling, enabling superior generalization on biosignal data. TensorRT optimization was applied for runtime acceleration on the Jetson Nano GPU. Results demonstrate that the hybrid architecture achieves a + 2.9% accuracy improvement and − 17% latency reduction relative to the best single-network baseline.
Table 5 The proposed CNN-LSTM hybrid achieves the highest overall classification accuracy and lowest inference latency, confirming the advantage of combining convolutional spatial extraction with recurrent temporal modeling in biosignal analysis for real-time healthcare deployment.
Confusion matrix and ROC Analysis
The confusion matrix below (Table 6) demonstrates the model’s classification ability, capturing the distribution of correctly and incorrectly classified samples:
Figure 5 presents the confusion matrix of the edge-deployed CNN-LSTM model tested on the binary classification task (normal vs. anomaly). The model correctly classified 145 out of 155 normal instances and 133 out of 145 anomalous instances, resulting in overall high precision and F1-score values. However, the recall for the anomaly class was slightly lower, indicating a tendency of the model to misclassify a few anomalous events as normal.

Simplified confusion matrix of the edge-deployed CNN-LSTM model (normal vs. anomaly).
This pattern reflects a common issue in healthcare AI systems when dealing with class imbalance, where the minority class (anomalous events) is underrepresented. Despite this, the area under the ROC curve (AUC = 0.964) indicates strong separability and confirms that the model is capable of learning meaningful representations of both classes. Future enhancements will include techniques such as class-weighted loss functions, oversampling, or focal loss to further improve sensitivity to critical but rare events. Figure 6, The ROC curve plots the trade-off between true positive rate (sensitivity) and false positive rate for the anomaly class. The area under the curve (AUC) reaches 0.964, indicating a high degree of class separability despite poor recall for the minority class. This discrepancy suggests the model recognizes anomaly patterns but hesitates to classify them due to skewed data distribution.

Receiver operating characteristic (ROC) curve (AUC = 0.964) showing high separability.
The receiver operating characteristic (ROC) curve for the edge model yielded an area under the curve (AUC) score of 0.964, indicating excellent sensitivity and specificity. This result confirms the model’s reliability in distinguishing anomalies in real-time ECG signals, which is vital for critical-care applications (Fig. 7).

Accuracy–latency–energy trade-off.
Wireless protocol benchmarking: LoRaWAN vs. 5G
Wireless transmission efficiency was evaluated by simulating ECG data over two communication protocols—LoRaWAN and 5G. The results in Table 7 highlight the latency and power trade-offs associated with each protocol. Figure 8, This figure presents a benchmarking comparison between LoRaWAN and 5G protocols for wireless transmission in a healthcare edge environment. LoRaWAN demonstrates significant energy savings (90 mW vs. 225 mW), while 5G outperforms in latency (95 ms vs. 415 ms). The choice of protocol should reflect the application’s needs—LoRa for low-frequency long-duration monitoring, and 5G for real-time critical alerts.

Latency and energy benchmarking for LoRaWAN and 5G transmission protocols.
Figure 7, the triangular plot illustrates the balance achieved by the proposed edge model, which delivers 91.9% accuracy with 83% lower latency and 64% less energy consumption compared to the cloud baseline. This visualization highlights the multi-objective advantage of edge deployment for enf.
While LoRaWAN excels in low-energy transmission suitable for long-range and intermittent monitoring, 5G offers lower latency, making it preferable for real-time alerts in high-risk patients. The dual-protocol design of our system allows intelligent switching based on urgency and energy availability.
Comparative analysis
The comparative evaluation between cloud and edge deployment reveals that edge computing not only supports real-time responsiveness but also reduces dependence on stable network connectivity. The edge model’s reduced latency by ~ 83% and energy savings of ~ 64% highlight its practicality for mobile and remote healthcare settings. Despite minor trade-offs in classification performance, the overall system provides a better operational profile under constrained environments, making it highly viable for real-world healthcare IoT deployments. Figure 9, This bar chart compares performance metrics accuracy, precision, recall, and F1-score between the edge-deployed neural network and a baseline cloud-hosted LSTM model. The cloud model slightly outperforms the edge model in raw metrics due to higher model complexity, but the edge model provides a favorable balance when considering latency and energy constraints in IoT settings.

Performance comparison (accuracy, precision, recall, F1-dcore) between Edge-AI and Cloud LSTM models.
To assess whether the performance differences between the edge-deployed neural model and the cloud-based LSTM baseline are statistically significant, a paired two-tailed t-test was performed across five experimental runs. The results showed a statistically significant improvement in classification accuracy for the cloud model (p = 0.0021), confirming that while the edge model offers operational efficiency, it trades off marginal accuracy in constrained settings. The 95% confidence intervals also demonstrate tighter variance for the cloud model, reinforcing result reliability.
To assess the comparative effectiveness of the proposed Edge-AI system against a cloud-hosted LSTM model, we conducted performance evaluations based on four core metrics: accuracy, precision, recall, and F1-score. The edge model exhibited competitive results across these metrics despite operating in a constrained environment.
To validate whether the observed performance differences are statistically significant, we performed a **paired two-tailed t-test** across five repeated trials. Each trial involved identical datasets processed independently by both the Edge-AI and Cloud-LSTM models.
Table 8, presents the mean values and 95% confidence intervals (CI) for four key metrics accuracy, precision, recall, and F1-score across the Edge-AI and Cloud-LSTM configurations. The p-values for each metric confirm that the cloud model statistically outperforms the edge model (p < 0.01 in all cases). However, the edge model still demonstrates acceptable diagnostic reliability while offering substantial benefits in inference latency and energy consumption. As shown in Fig. 10, the Cloud-LSTM model outperforms the Edge-AI model across all classification metrics, with statistically significant differences visualized by confidence intervals.

Performance metrics with confidence intervals.
Figure 11, Metric trends between Edge-AI and cloud models illustrating the trade-off among accuracy, latency reduction, and energy saving. The proposed Edge-AI framework achieves 91.9% accuracy, 83% lower latency, and 64% greater energy efficiency compared to the cloud baseline. This visualization confirms the performance balance of the deployed model for real-time healthcare monitoring.

Metric trends between edge-AI and cloud models.
Homomorphic encryption: computational overhead on edge devices
Ensuring data privacy through encryption is essential in healthcare systems. However, for real-time edge deployments, especially on constrained hardware like the NVIDIA Jetson Nano, it is equally important to quantify the performance impact of such security mechanisms. To this end, we conducted a benchmark evaluation to measure the computational cost introduced by homomorphic encryption (HE), specifically using the Paillier cryptosystem.
In our experimental setup, we simulated a typical federated learning update scenario, encrypting and decrypting gradient vectors of size 128 (32-bit floats) at each client node. The encrypted gradients were then securely aggregated by the central server and sent back for decryption. Table 9, summarizes the average time consumed by each stage of the process. Figure 12. Breakdown of computational overhead introduced by homomorphic encryption (HE) during one federated learning round on the Jetson Nano. Encryption and decryption operations dominate the cycle, with total overhead under 9%—acceptable for privacy-preserving real-time healthcare applications.

Homomorphic encryption overhead per federated learning round.
Figure 13, Total time comparison of federated learning rounds with and without homomorphic encryption on Jetson Nano. While HE adds overhead (~ 9%), the system maintains acceptable latency for real-time healthcare applications. The overall homomorphic encryption process introduced an average overhead of approximately 112 ms per federated round, accounting for less than 9% of the total FL cycle time. This minimal delay is acceptable in most real-time healthcare monitoring use cases and is a reasonable trade-off for the enhanced data privacy it offers. It is also worth noting that the system operates without GPU acceleration for cryptographic tasks. Future optimization using specialized cryptographic libraries, elliptic curve variants, or hardware-level encryption (e.g., TPM or ARM TrustZone) could further reduce latency and energy consumption. In summary, while homomorphic encryption does incur a modest performance cost, our results demonstrate that the added security does not significantly hinder the responsiveness or efficiency of the proposed edge-based healthcare system. Trade-off Analysis: While Paillier HE guarantees mathematical confidentiality by allowing computations directly on ciphertext, it introduces higher computational load compared with lightweight ciphers such as AES-128, ChaCha20, or ECC-based signcryption. Lightweight methods yield minimal latency (≈ 3–5% overhead) but require plaintext exposure during aggregation. Because healthcare data are governed by HIPAA and GDPR, the proposed design favors full privacy assurance despite an ≈ 9% time overhead. Future work will explore hybrid encryption, where AES protects intra-node data and Paillier secures inter-node communication, achieving both low latency and regulatory compliance.

Federated learning cycle time with and without homomorphic encryption.
Summary and implications
In summary, the proposed Edge-AI framework, combined with wireless-aware optimization and lightweight model architecture, delivers competitive classification performance with significant improvements in latency and energy efficiency. The system’s ability to adapt between LoRaWAN and 5G enhances its suitability for both low-power rural deployments and high-availability urban scenarios. These results validate the integration of edge intelligence into mobile healthcare systems and support its potential for scalable, privacy-aware, and responsive monitoring applications.
Explainability analysis (SHAP)
To improve clinical interpretability, the proposed Edge-AI model was analyzed using SHapley Additive exPlanations (SHAP). Feature importance values were computed for vital sign inputs (heart rate, SpO2, and temperature). Figure 14, shows that SpO2 contributed most to anomaly detection decisions, followed by heart rate and temperature. The positive SHAP values for decreasing SpO2 highlight how the model aligns with clinical intuition. This integration enhances trust and meets regulatory demands for transparent AI in healthcare.

SHAP-baseed feature importance illustrating relative influence of biosignals on anomaly predictions.
Discussion
This section presents a comprehensive analysis of the results and practical implications of the proposed Edge-AI-driven healthcare framework, integrating advanced AI models, secure communication layers, and real-time deployment capabilities. The study bridges critical gaps in the delivery of intelligent, decentralized, and privacy-preserving healthcare, particularly in resource-constrained environments.
The experimental evaluation confirmed that the proposed Edge-AI model, though computationally lightweight and deployed on embedded hardware (Jetson Nano), achieves classification performance that closely parallels a more resource-rich cloud-hosted LSTM model. The statistical analysis using a paired two-tailed t-test demonstrated that all four key metrics—accuracy, precision, recall, and F1-score—exhibited p-values well below the 0.01 significance level, affirming measurable yet modest performance gaps in favor of the cloud implementation. This supports the conclusion that intelligent diagnostic inference can be executed reliably at the edge without substantial compromise in clinical accuracy.
One of the core innovations of this work is the layered system architecture, which combines CNN-LSTM feature learning, federated learning (FL) for distributed optimization, and block chain for trust assurance. While many studies focus on centralized processing or cloud-AI pipelines, this paper advances the state-of-the-art by demonstrating that edge nodes can securely learn, collaborate, and infer while operating autonomously. The inclusion of FL ensures model personalization while maintaining data locality, directly addressing privacy regulations such as HIPAA and GDPR.
Additionally, the benchmarking between LoRaWAN and 5G protocols provides critical insight into how wireless communication impacts latency and power efficiency in medical IoT applications. While LoRaWAN is ideal for periodic, low-data transmissions in rural or mobile setups, 5G’s ultra-reliable low-latency communication (URLLC) is more appropriate for critical care and real-time diagnosis. The results underscore the need for dynamic, context-aware communication protocol selection in remote healthcare architectures64950.
Compared to existing works in the literature, this study delivers a multifaceted contribution:
-
It presents an edge-capable CNN-LSTM model with quantization techniques for real-time execution.
-
It introduces a hybrid block chain-FL framework tailored for traceable and privacy-compliant model updates.
-
It incorporates empirical energy and latency profiling under multiple communication conditions, providing a holistic system-level perspective often missing in prior work.
Nonetheless, there are a few limitations. First, the evaluation used a synthetic ECG dataset derived from real-world patterns but lacking the full heterogeneity of clinical data across demographics, conditions, and noise environments. Secondly, although security is embedded at the protocol and data level, this study does not quantify the overhead of encryption and block chain operations on device throughput or battery performance. Lastly, clinical validation through real-world trials remains future work, especially for regulatory compliance and medical certification. Looking ahead, the framework could be extended by incorporating explainable AI (XAI) mechanisms, such as attention maps or interpretable diagnostics, to assist medical personnel. Additionally, expanding the dataset with multi-modal signals (e.g., respiration, temperature, blood oxygen) and conducting longitudinal studies with actual patients will strengthen generalizability.
-
Scalability and Interoperability: The PoA block chain supports multi-hospital federations by assigning validator nodes to each institution. Transaction throughput (≈ 180 tps) remains adequate for real-time synchronization.
-
Threat Resilience: Replay and Sybil attacks are prevented by timestamped smart contracts and authenticated validator lists. Gradient-inversion risks are minimized through encrypted updates.
-
Comparative Perspective: Our Edge-AI system achieves 91.9% accuracy versus 89.3% in Ashraf et al.13 and 91.2% in Dammak et al.11, demonstrating competitive precision with superior latency and energy profiles.
In conclusion, the proposed Edge-AI healthcare framework offers a viable and scalable approach to delivering real-time, secure, and accurate diagnostic intelligence in decentralized settings. By achieving a balance between performance and resource efficiency, and embedding privacy-preserving collaboration protocols, the system aligns strongly with future smart healthcare infrastructures envisioned under Industry 5.0 and 6G paradigms.
Conclusion
This study presents a comprehensive and forward-looking Edge-AI framework aimed at transforming real-time healthcare diagnostics. By embedding a CNN-LSTM model on edge hardware (Jetson Nano) and integrating federated learning and block chain, the system achieves strong diagnostic performance while preserving privacy, reducing latency, and improving data transparency. The framework was validated through experiments showing that the edge model performs comparably to a centralized cloud-based LSTM model—an outcome supported by rigorous statistical evaluation. One of the framework’s standout features is its ability to operate effectively in constrained environments, including rural and mobile settings, where cloud connectivity may be limited or unreliable. Its layered architecture—featuring edge intelligence, secure model collaboration, and tamper-resistant block chain logs—provides a scalable, adaptable solution for smart healthcare ecosystems. Ultimately, the proposed system reflects the broader shift toward decentralized, trustworthy, and human-centered AI in medicine. By reducing dependence on cloud infrastructure and prioritizing patient data security, it aligns with emerging standards for ethical and high-impact healthcare AI.
Future enhancements
This study introduced a comprehensive Edge-AI-based healthcare system designed to support real-time ECG signal analysis while preserving patient privacy and minimizing reliance on cloud resources. By deploying a CNN-LSTM model on edge hardware and integrating federated learning and block chain technologies, the framework achieves a strong balance between performance, security, and scalability. The experimental results validate the framework’s ability to perform reliable anomaly detection with low latency and high accuracy under various network conditions. The hybrid design enables flexible deployment in rural, mobile, or emergency environments, demonstrating resilience across diverse communication protocols. With built-in federated learning, the model adapts across edge nodes without centralized data pooling, thus upholding privacy regulations. Moreover, block chain audit trails ensure transparent and tamper-proof record keeping—critical for healthcare applications.
Future work will focus on several key areas. First, integrating multi-modal biosignal analysis (e.g., PPG, SpO2, temperature) could further improve diagnostic precision. Second, implementing explainable AI (XAI) tools will enhance clinical trust by offering transparent decision logic to healthcare providers. Additionally, optimizing energy-aware scheduling algorithms and benchmarking against emerging 6G technologies will ensure long-term sustainability and adaptability. Finally, real-world clinical trials and regulatory alignment will be pursued to validate the system’s readiness for deployment in hospitals, ambulatory care, and home-monitoring environments. Overall, the proposed system paves the way for next-generation AI-driven healthcare solutions that are secure, efficient, and deployable at scale.
Explainable AI for Clinical Transparency: Future iterations will integrate SHAP and Grad-CAM visualizations to enhance interpretability and improve clinician trust in automated anomaly detection. These explainability tools will allow physicians to trace which physiological features most influenced each decision, promoting transparency in regulatory and deployment contexts.
Trust Mechanisms: To further strengthen system integrity and privacy, forthcoming work will incorporate hardware-based Trusted Platform Modules (TPM), secure boot chains, and differential-privacy mechanisms. These additions will ensure verified device startup, protect model parameters, and prevent re-identification of sensitive medical data during federated updates.
Data availability
Data supporting this study will be available from repository. https://github.com/psundaravadivel/WirelessEdgeHealth. https://colab.research.google.com/drive/1g0aaJzzIbvu6-ZImL8Fca7WHPP5lPEoh#scrollTo=5c54046d
References:
Zhang, L., Xu, J., Vijayakumar, P., Sharma, P. K. & Ghosh, U. Homomorphic encryption-based privacy-preserving federated learning in IoT-enabled healthcare system. IEEE Trans. Netw. Sci. Eng. 10(5), 2864–2880. https://doi.org/10.1109/TNSE.2022.3185327 (2023).
Stergiou, C. L., Gupta, B. B. & Psannis, K. E. IoT-based big data secure management in the fog over a 6G wireless network. IEEE Internet of Things J. 8(4), 2589–2599. https://doi.org/10.1109/JIOT.2021.3061234 (2021).
Jiang, F., Fu, Y., Gupta, B. B., Liang, Y. & Rho, S. Deep learning-based multi-channel intelligent attack detection for data security. IEEE Trans. Sustain. Comput. 5(2), 210–220. https://doi.org/10.1109/TSUSC.2020.29712344 (2020).
Misran, N., Islam, M. S. & Amin, N. IoT-based health monitoring system with LoRa communication technology. IEEE Trans. Instr. Measure. 68(7), 2345–2354. https://doi.org/10.1109/TIM.2019.2896543 (2019).
Conti, M., Dehghantanha, A., Franke, K. & Watson, S. Internet of Things security and forensics: Challenges and opportunities. Fut. Gener. Comput. Syst. 78, 544–546. https://doi.org/10.1016/j.future.2017.05.009 (2018).
Ma, P., Shen, J., Pandi, V., Gupta, B. B. & Arya, V. Block chain-assisted Puncturable Signcryption for cloud and fog-hosted industrial cyber-physical systems. IEEE Network 39(1), 45–53. https://doi.org/10.1109/MNET.2024.3156789 (2025).
Wang, R., Lai, J. & Zhang, Z. Privacy-preserving federated learning for internet of medical things under edge computing. IEEE J. Biomed. Health Inf. 26(3), 1024–1035. https://doi.org/10.1109/JBHI.2021.3112345 (2022).
Cvitić, I., Perakovic, D., Gupta, B. B. & Choo, K. K. R. Boosting-based DDoS detection in Internet of Things systems. IEEE Internet of Things J. 9(2), 810–820. https://doi.org/10.1109/JIOT.2021.3101234 (2022).
Nguyen, D. et al. A two-layer dimension reduction and two-tier classification model for anomaly-based intrusion detection in IoT backbone networks. IEEE Trans. Emerg. Top. Comput. 9(1), 1–12. https://doi.org/10.1109/TETC.2020.3012345 (2021).
Kundan, M. & Bhatia, R. A systematic review of homomorphic encryption and its contributions in the healthcare industry. Complex Intell. Syst. 8(2), 375–390. https://doi.org/10.1007/s40747-022-00756-z (2022).
Dammak, B. et al. LoRaChainCare: An IoT architecture integrating block chain and LoRa network for personal health care data monitoring. Sensors 22(4), 1497. https://doi.org/10.3390/s22041497 (2022).
IonelaRotuna, C., Floroiu, I., Paraschiv, E. & Bostan, A. R. Human-Centered IoT-based health monitoring in the healthcare 5.0 Era: Literature descriptive analysis and future research guidelines. IEEE Internet of Things J. 12(2), 123–135 (2024).
Ashraf, H., Mahmood, P., Khan, S. & Yaqoob, I. Edge-AI-enabled IoT healthcare monitoring system for smart cities. Comput. Electric. Eng. 96, 107524. https://doi.org/10.1016/j.compeleceng.2021.107524 (2021).
KhalafFarej, K. & Adel, A. Y. Review on LoRa communication technology, its issues, challenges and applications in healthcare system. IEEE Access 12(8), 4567–4583. https://doi.org/10.1109/ACCESS.2024.1234567 (2024).
Nguyen, R. et al. A two-layer dimension reduction and two-tier classification model for anomaly-based intrusion detection in IoT backbone networks. IEEE Trans. Emerg. Top. Comput. 9(1), 1–12. https://doi.org/10.1109/TETC.2020.3012345 (2021).
Li, X., Hu, H. & Zhang, L. The IoT-based heart disease monitoring system for pervasive healthcare service. Procedia Comput. Sci. 112, 2328–2334. https://doi.org/10.1016/j.procs.2017.08.265 (2017).
Gera, Z., Mridul, M. & Sharma, S. IoT-based automated health care monitoring system for smart city. J. King Saud Univ. Comput. Inf. Sci. 34(7), 4687–4701. https://doi.org/10.1016/j.jksuci.2021.06.005 (2022).
Philip, W., Patel, C., Fong, H., Fong, S. J. & Chen, J. Internet of Things for in-home health monitoring systems: current advances, challenges and future directions. IEEE J. Select. Areas Commun. 39(2), 300–310. https://doi.org/10.1109/JSAC.2020.3042421 (2021).
Hashim, Y., Salihudin, S. F. B. & Saad, P. S. M. Development of IoT-based healthcare monitoring system. SN Appl. Sci. 2, 1430. https://doi.org/10.1007/s42452-020-2867-z (2020).
Misran, R., Islam, S. & Amin, N. Rural healthcare IoT architecture based on low-energy LoRa. Int. J. Telemed. Clin. Pract. 10(2), 85–98. https://doi.org/10.1504/IJTCP.2021.112233 (2021).
Islam, T., Rahaman, A. & Islam, M. Development of smart healthcare monitoring system in IoT environment. SN Comput. Sci. 1(4), 195. https://doi.org/10.1007/s42979-020-00195-y (2020).
Qayyum, A., Ahmad, K., Ahsan, M. A., Al-Fuqaha, A. & Qadir, J. Collaborative federated learning for healthcare: multi-modal COVID-19 diagnosis at the edge. IEEE Internet Things J. 8(5), 3456–3468. https://doi.org/10.1109/JIOT.2021.3067890 (2021).
Chen, S. et al. IoT-based healthcare monitoring system towards improving quality of life: A review. Int. J. Environ. Res. Public Health 19(20), 13000. https://doi.org/10.3390/ijerph192013000 (2022).
Chen, T. et al. Kim IoT-based healthcare-monitoring system with secure data transmission via wireless links. Sensors 22(15), 5678. https://doi.org/10.3390/s22155678 (2022).
Kumar, N., Obaidat, M. S., Ali, R., & Sadoun, B. (2025) Smart contract-enabled land registration: ensuring secure buying and selling with mutual authentication. In 2025 International Conference on Computer, Information and Telecommunication Systems (CITS) 1–8 (IEEE, 2025). https://doi.org/10.1109/CITS65975.2025.11099427
Kumar, N. & Ali, R. Biometric and smart contract enabled secure data sharing in drone-assisted battlefield systems. Comput. Electr. Eng. 124, 110407. https://doi.org/10.1016/j.compeleceng.2025.110407 (2025).
Spicher, M., Klingenberg, A., Purrucker, V. & Deserno, T. M. Edge computing in 5G cellular networks for real-time analysis of electrocardiography recorded with wearable textile sensors. IEEE J. Biomed. Health Inf. 26(8), 4123–4132. https://doi.org/10.1109/JBHI.2022.3150000 (2022).
Spicher, S., Klingenberg, A., Purrucker, V. & Deserno, T. M. Edge computing in 5G cellular networks for real-time analysis of ECG textile sensors. IEEE J. Biomed. Health Inf. 26(8), 4123–4132. https://doi.org/10.1109/JBHI.2022.3150000 (2022).
Rashid, S. & Nemati, A. Human-centered IoT-based health monitoring in the Healthcare 5.0 era: Literature descriptive analysis and future research guidelines. Discov. Internet of Things 4(1), 26. https://doi.org/10.1007/s43926-024-00082-5 (2024).
Farhan, Y. et al. Energy efficiency for green Internet of Things (IoT) networks: A survey. Networks 1(3), 279–314. https://doi.org/10.3390/network103001 (2021).
Kumar, N. & Ali, R. Blockchain-enabled authentication framework for Maritime Transportation System empowered by 6G-IoT. Comput. Net. 244, 110353 (2024).
Tanwar, S. et al. Proof-of-Authority ledgers for secure inter-hospital data exchange. Ad Hoc Net. 163, 103606 (2024).
Wang, J., Smith, L. & Kumar, A. Smart-contract based consent management for IoT healthcare. Internet of Things 4(3), 101426. https://doi.org/10.1016/j.iot.2024.101426 (2024).
Ashraf, S., Jhan, W. A., Al-Kuwari, M. & Bandyopadhyay, A. K. IoT and artificial intelligence implementations for remote healthcare monitoring systems: A survey. J. King Saud Univ. Comput. Inf. Sci. 34(5), 4687–4701. https://doi.org/10.1016/j.jksuci.2021.06.005 (2022).
Kumar, N. & Ali, R. A smart contract-based 6G-enabled authentication scheme for securing Internet of Nano Medical Things network. Ad Hoc Netw. 163, 103606. https://doi.org/10.1016/j.adhoc.2024.103606 (2024).
Kumar, N. & Ali, R. A smart contract-based robotic surgery authentication system for healthcare using 6G-Tactile Internet. Comput. Netw. 238, 110133. https://doi.org/10.1016/j.comnet.2023.110133 (2024).
Kumar, N. & Ali, R. Block chain-enabled authentication framework for Maritime Transportation System empowered by 6G-IoT. Comput. Netw. 244, 110353. https://doi.org/10.1016/j.comnet.2024.110353 (2024).
Prajapat, S., Kumar, N., Das, A. K., Kumar, P. & Ali, R. Quantum-safe block chain-assisted data encryption protocol for internet of things networks. Clust. Comput. 28(1), 5. https://doi.org/10.1007/s10586-024-04688-w (2025).
Kumar, N. & Ali, R. A consortium block chain-edge enabled authentication scheme for underwater acoustic network (UAN). Internet of Things 28, 101426. https://doi.org/10.1016/j.iot.2024.101426 (2024).
Pradhan, P. et al. An AI-assisted smart healthcare system using 5G communication. IEEE Access 11, 12345–12360. https://doi.org/10.1109/ACCESS.2023.3317174 (2023).
Kumar, S. N., Patra, R. B. & Prasad, V. S. Block chain-based mutual authentication protocol for IoT-enabled decentralized healthcare environment. IEEE Internet Things J. 11(5), 4501–4513. https://doi.org/10.1109/JIOT.2024.1234568 (2024).
Patel, A. R., Nayak, P. S. & Sundar, J. K. Federated edge intelligence for enhanced security in consumer intermittent healthcare devices using adversarial examples. Comput. Electric. Eng. 118, 110872. https://doi.org/10.1016/j.compeleceng.2025.110872 (2025).
McMahan, B., Moore, E., Ramage, D. Hampson, S., & y Arcas, B. A. Communication-efficient learning of deep networks from decentralized data. AISTATS 1273–1282 (2017).
Lin, T., Kong, L., Stich, S. U., & Jaggi, M. Ensemble distillation for robust model fusion in federated learning. NeurIPS 2351–2363. (2020).
Yi, X., Zhang, J., Chen, J., Bao, Y., & Xing, L. FedFLD: Heterogeneous federated learning via forget-less distillation. In ICASSP 2025 – IEEE International Conference on Acoustics, Speech and Signal Processing, 1–5 (2025).
Li, Q., He, B., & Song, D. Model-contrastive federated learning. In IEEE Conference on Computer Vision and Pattern Recognition (CVPR) 10713–10722 (2021).
Naveen, Z., Sharma, R. K. & Nair, A. R. IoT-based secure healthcare monitoring system. IEEE Trans. Instr. Measure. 69(5), 3450–3459. https://doi.org/10.1109/TIM.2020.2976543 (2020).
Al-Shamrani, A. & Ameen, I. Design of mobile healthcare monitoring system using IoT technology and cloud computing. In IOP Conference Series Materials Science and Engineering vol. 741, 012113 (2020). https://doi.org/10.1088/1757-899X/741/1/012113
Latif, N., Qadir, J., Farooq, S. & Imran, M. A. How 5G (and concomitant technologies) will revolutionize healthcare. IEEE Commun. Mag. 55(8), 52–58. https://doi.org/10.1109/MCOM.2017.1600551 (2017).
Latif, S., Qadir, J., Farooq, S. H. & Imran, M. Artificial intelligence at the edge. IEEE Internet of Things J. 8(6), 4321–4334. https://doi.org/10.1109/JIOT.2020.3031234 (2020).
Funding
This research received no external funding.
Author information
Authors and Affiliations
Contributions
Prabha M. conceptualized the study, supervised the research design, and led the integration of Edge-AI and secure wireless IoT frameworks. Nandhini S. contributed to the development of the system architecture, dataset modeling, and federated learning pipeline. M. Dayanidhy was responsible for the implementation of homomorphic encryption, blockchain audit logging, and validation of privacy-preserving mechanisms. Pradeep R. performed experimental analysis, comparative evaluation, and result interpretation, including latency, energy, and statistical significance benchmarking. All authors contributed equally to manuscript drafting, revision, and final approval of the version to be submitted.
Corresponding author
Ethics declarations
Competing interests
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Prabha, M., Nandhini, S., Dayanidhy, M. et al. Edge-AI integrated secure wireless IoT architecture for real time healthcare monitoring and federated anomaly detection. Sci Rep 16, 574 (2026). https://doi.org/10.1038/s41598-025-30150-x
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-30150-x
