
Abstract
This population-based, individually matched case–control study aimed to examine the association between tobacco use disorder (TUD) and cardiomyopathy. We conducted a retrospective case-control analysis using data from the 2005 Longitudinal Health Insurance Database, a subset of Taiwan’s National Health Insurance Research Database (NHIRD). A total of 10,426 newly diagnosed cardiomyopathy cases and 41,704 matched controls (matched 1:4 by age, sex, and index year) from 2000 to 2015 were identified. TUD exposure was defined using ICD-9-CM codes. Conditional logistic regression was applied to estimate adjusted odds ratios (aORs) and 95% confidence intervals (CIs), adjusting for demographic and clinical covariates. Analyses evaluated both the timing and total duration of TUD exposure preceding cardiomyopathy diagnosis to explore temporal patterns in odds. Prior TUD exposure was associated with higher odds of cardiomyopathy (aOR = 1.376, 95% CI = 1.102–1.598). A recency-related gradient in odds was observed: exposure within < 1 year before diagnosis (aOR = 2.990), 1–5 years (aOR = 1.401), and > 5 years (aOR = 1.126; not significant after Bonferroni correction). A similar duration-related increase in odds was identified: <1 year (aOR = 1.288; not significant after Bonferroni), 1–5 years (aOR = 1.592), and > 5 years (aOR = 2.743). Tobacco use disorder was associated with higher odds of cardiomyopathy, showing both recency-and duration-related gradients in odds. These findings emphasize the importance of early and sustained tobacco cessation to reduce the burden of cardiomyopathy, while acknowledging that causal inference cannot be established due to the case-control design.
Similar content being viewed by others

Introduction
Cardiomyopathy comprises a heterogeneous group of myocardial disorders—including dilated cardiomyopathy (DCM)1,2,3,4, hypertrophic cardiomyopathy (HCM)5,6, restrictive cardiomyopathy (RCM)7,8, arrhythmogenic cardiomyopathy (ARVC)9,10, and stress-induced or Takotsubo cardiomyopathy11,12,13,14. Despite differing etiologies, these conditions share structural and functional abnormalities of the myocardium that contribute substantially to heart failure, arrhythmias, and premature mortality.
Tobacco use disorder (TUD) is a chronic, relapsing condition characterized by compulsive tobacco consumption despite known adverse health consequences15. It is a leading contributor to global cardiovascular morbidity and mortality16,17. Emerging evidence suggests that tobacco exposure may induce oxidative stress, autonomic dysregulation, inflammation, and myocardial remodeling18,19,20,21,22,23, mechanisms that could plausibly predispose individuals to cardiomyopathy. However, limited longitudinal population-based research has directly investigated whether TUD increases the risk of cardiomyopathy. Most prior studies have primarily focused on coronary artery disease or heart failure, leaving uncertainty about cardiomyopathy as a distinct clinical outcome24,25.
To address this gap, we conducted a nationwide, population-based case-control study in Taiwan to examine whether individuals with TUD are at elevated risk of developing cardiomyopathy, with particular attention to dose–response relationships by exposure timing and duration.
Materials and methods
Data source
Taiwan’s National Health Insurance launched a single payment system on March 1, 1995. As of 2017, 99.9% of Taiwan’s population participated in the program. The data for this study comes from the 2005 Longitudinal National Health Insurance Database (LHID 2005), which is part of the National Health Insurance Research Database (NHIRD) and randomly selected 2,000,000 people from the entire population. All personal information in LHID2005 was de-identified before release to protect patient privacy. In LHID2005, the disease diagnosis code is based on the “International Classification of Diseases, Ninth Revision, Clinical Modification” (ICD-9-CM) standard26. Additionally, certified medical records technicians review and confirm diagnosis codes prior to hospital reimbursement claims processing27. NHIRD administration also conducts random audits of outpatient records and periodically reviews inpatient claims to ensure diagnostic accuracy28. The administrative accuracy of Taiwan’s NHIRD has been validated in prior studies, and coding reliability is ensured due to its linkage with hospital reimbursement claims processing.
All procedures performed in research involving human participants comply with the ethical standards of the institution and/or the National Research Council, and comply with the 1964 Declaration of Helsinki and its subsequent amendments or similar ethical standards. All methods are carried out following relevant guidelines and regulations. This study was approved by the Institutional Review Board of the Tri-Service General Hospital (TSGHIRB No. E202516008), which waived the requirement for informed consent due to the use of de-identified secondary data from the NHIRD, in accordance with institutional and national ethical guidelines.
Research design and samples
This study employed a nested case-control design using data from Taiwan’s NHIRD between January 1, 2000, and December 31, 2015. We first identified 10,504 patients with a new diagnosis of cardiomyopathy (ICD-9-CM code 425.x). To ensure incident cases, those with any cardiomyopathy diagnosis during the one-year lookback period (January 1 to December 31, 1999) were excluded, leaving 10,426 eligible cases.
For the control group, 41,704 individuals without cardiomyopathy were randomly selected from the same database. Controls were matched to cases at a 1:4 ratio based on sex, age (in years), and index date. The index date was defined as the date of the first cardiomyopathy diagnosis for each case, and the same date was assigned to its matched controls. This matching strategy minimized potential confounding by demographic factors and temporal trends in diagnosis or coding practices.
TUD was defined as having at least three outpatient claims with the ICD-9-CM code 305.1 prior to the index date. This threshold was selected to enhance diagnostic specificity and reduce misclassification, given that a single claim may reflect a provisional or rule-out diagnosis. In contrast, cardiomyopathy was identified based on at least one outpatient or inpatient claim (ICD-9-CM code 425.x), reflecting its greater clinical severity and lower likelihood of miscoding. These criteria ensured that TUD cases represented clinically meaningful, chronic conditions while maximizing sensitivity for identifying cardiomyopathy cases.
Covariates included sociodemographic characteristics (sex, age groups [20–49, 50–64, ≥ 65 years], monthly insurance premium, urbanization level, and area of residence), healthcare level, and comorbidities quantified using the revised Charlson Comorbidity Index (CCI). The monthly insurance premium, a proxy for socioeconomic status, was categorized into three groups (< 18,000; 18,000–34,999; and ≥ 35,000 New Taiwan Dollars) according to the official National Health Insurance (NHI) insured salary brackets, which serve as a proxy for socioeconomic status in Taiwan. Urbanization level was classified into four strata based on population size and development indicators, while healthcare level was categorized into medical center, regional hospital, and local hospital.
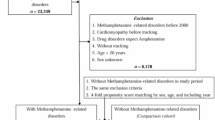
Comorbidities were identified using validated ICD-9-CM codes and included diabetes mellitus (DM), hypertension, hyperlipidemia, congestive heart failure (CHF), cerebrovascular accident (CVA), chronic obstructive pulmonary disease (COPD), chronic kidney disease (CKD), depressive disorders, anxiety, bipolar disorder, psychotic disorders, alcohol use disorders (AUD), and illicit drug use disorders (IDUD). To avoid redundancy in adjustment, we applied a revised CCI score excluding those conditions already modeled as individual covariates. The complete list of diagnostic codes is provided in Table S1, which has been reviewed and corrected to ensure consistency with the main text. This comprehensive design ensured rigorous case identification, reliable exposure classification, and control for major confounders, thereby strengthening the validity of our findings.The sample selection flow is summarized in Fig. 1, which has been revised to clarify that matching was based on age, sex, and index date, and that no propensity score matching was applied.

Flowchart of sample selection and 1:4 individual matching process based on age, sex, and index date.
This study adopted a nested case–control design using data from Taiwan’s NHIRD. Cases were patients newly diagnosed with cardiomyopathy (ICD-9-CM 425.x) between 2000 and 2015, and controls were randomly selected individuals without cardiomyopathy, matched at a 1:4 ratio by age, sex, and index date. After applying exclusion criteria and ensuring the temporal sequence of exposure, a total of 10,426 cases and 41,704 matched controls were included for analysis.
Note
No propensity score matching was performed; conditional logistic regression was used for all inferential analyses.
Statistical analysis
Descriptive statistics were used to summarize the characteristics of cardiomyopathy cases and matched controls. Categorical variables were presented as counts and percentages and compared using the chi-square test. Continuous variables were expressed as means ± standard deviations and compared using the t-test.
Conditional logistic regression was applied to estimate adjusted odds ratios (AORs) and 95% confidence intervals (CIs) for the association between tobacco use disorder (TUD) and cardiomyopathy, accounting for the 1:4 individual matching on age, sex, and index date. Multivariable models further adjusted for sociodemographic factors (income level, urbanization level, level of care, and season) and comorbidities, including diabetes mellitus, hypertension, hyperlipidemia, chronic kidney disease, cerebrovascular accident, congestive heart failure, depressive disorders, anxiety, bipolar disorder, psychotic disorders, alcohol use disorder, and illicit drug use disorder.
To explore the temporal and dose-response associations, we examined the timing (interval between last TUD diagnosis and the index date) and total duration (interval between first and last TUD diagnoses) of TUD exposure, with individuals without TUD serving as the reference group. The Bonferroni correction was applied to adjust for multiple comparisons.
All statistical analyses were performed using SPSS version 22 (IBM Corp., Armonk, NY, USA). A two-tailed p < 0.05 was considered statistically significant.
The balance of covariates between matched groups was assessed using standardized mean differences (SMDs), with SMD < 0.1 indicating adequate balance (Table S2).
Results
Baseline characteristics of the study population
The study included 52,130 participants, comprising 10,426 cardiomyopathy cases and 41,704 matched controls (1:4 matching by age, sex, and index date). The mean age of the overall study population was 60.21 ± 18.52 years, and 56.32% were male.
Compared with their matched controls, cases showed a higher prevalence of several comorbidities and sociodemographic characteristics. Specifically, a greater proportion of cases were from low-income households, had higher CCI scores, and more frequently resided in less urbanized areas or received care at regional hospitals.
With respect to medical comorbidities, cases more often presented with diabetes mellitus, hypertension, hyperlipidemia, congestive heart failure, cerebrovascular accident, depressive disorders, anxiety, bipolar disorder, psychotic disorders, alcohol use disorder, and illicit drug use disorder than did their matched controls.
Table 1 summarizes the baseline characteristics of cardiomyopathy cases and matched controls. These differences reflect the distribution of demographic and clinical variables between groups and were evaluated using χ² and t-tests. No causal inferences are implied.
Association Between Tobacco Use Disorder and Risk of Cardiomyopathy
Table 2 presents the results of the multivariable conditional logistic regression analysis accounting for the 1:4 individual matching on age, sex, and index date. Compared with individuals without tobacco use disorder (TUD), those with TUD had higher odds of cardiomyopathy (adjusted odds ratio [AOR] = 1.376; 95% confidence interval [CI] = 1.102–1.598).
Among sociodemographic variables, low-income status was associated with higher odds of cardiomyopathy (AOR = 1.523; 95% CI = 1.094–2.106).
Several medical comorbidities also showed higher odds of cardiomyopathy, including diabetes mellitus (AOR = 2.623), hypertension (AOR = 2.812), hyperlipidemia (AOR = 1.986), chronic kidney disease (AOR = 1.333), cerebrovascular accident (AOR = 2.030), and congestive heart failure (AOR = 1.602). Each one-point increase in the revised Charlson Comorbidity Index (CCI-R) corresponded to a 13.2% increase in the odds of cardiomyopathy.
Psychiatric and substance-related comorbidities were also associated with higher odds of cardiomyopathy. Specifically, depressive disorders (AOR = 1.802), anxiety (AOR = 1.725), bipolar disorder (AOR = 1.532), psychotic disorders (AOR = 1.706), alcohol use disorder (AOR = 3.356), and illicit drug use disorder (AOR = 2.756) were all positively associated.
Regarding contextual factors, cardiomyopathy cases diagnosed during the winter season exhibited higher odds compared with those in spring (AOR = 1.996). Similarly, participants residing in more urbanized areas (Level 1: AOR = 2.245; Level 2: AOR = 1.914) or receiving care at medical centers (AOR = 2.140) or regional hospitals (AOR = 1.531) showed higher odds of cardiomyopathy. These findings may reflect differences in health-care access, diagnostic intensity, or residual confounding, rather than causal effects.
Stratified analysis of the association between tobacco use disorder and cardiomyopathy by demographic and clinical variables
Table 3 summarizes the stratified conditional logistic regression results accounting for the 1:4 matching (age, sex, index date).
Across most demographic and clinical strata, TUD vs. non-TUD (reference) was associated with higher odds of cardiomyopathy.
Overall, individuals with TUD had 1.38-fold higher odds of cardiomyopathy (AOR = 1.376; 95% CI = 1.102–1.598).
When stratified by sex, the association persisted in both men (AOR = 1.440; 95% CI = 1.153–1.671) and women (AOR = 1.251; 95% CI = 1.006–1.452).
By age group, higher odds of cardiomyopathy were observed among those aged 20–49 years (AOR = 1.253; 95% CI = 1.005–1.453), 50–64 years (AOR = 1.591; 95% CI = 1.278–1.849), and ≥ 65 years (AOR = 1.298; 95% CI = 1.040–1.506).
Similar associations were found within most comorbidity strata. For instance, the odds of cardiomyopathy for TUD vs. non-TUD (reference) were higher among participants with diabetes mellitus, hypertension, hyperlipidemia, or cerebrovascular accident. Psychiatric and substance-related conditions—such as depressive, anxiety, bipolar, or psychotic disorders, alcohol use disorder, and illicit drug use disorder—also showed consistent positive associations.
Seasonal, urbanization, and level-of-care strata showed modest variation: cases diagnosed during winter, residents of more urbanized regions, and individuals treated at higher-level hospitals exhibited higher odds of cardiomyopathy for TUD vs. non-TUD (reference). These differences likely reflect variation in diagnostic opportunity or health-care utilization rather than causal effects.
Association between timing of last tobacco use disorder exposure and cardiomyopathy
Table 4 presents the results from the conditional logistic regression analysis (accounting for the 1:4 matching on age, sex, and index date) examining how the time elapsed since the most recent TUD diagnosis relates to the odds of cardiomyopathy.
Compared with non-TUD individuals (reference), participants with more recent TUD exposure showed higher odds of cardiomyopathy, forming a clear temporal (recency) gradient.
-
Those with a TUD diagnosis within < 1 year before the index date had nearly threefold higher odds (AOR = 2.990; 95% CI = 1.978–3.452).
-
Those with exposure 1–5 years prior showed moderately higher odds (AOR = 1.401; 95% CI = 1.113–1.607).
-
Exposure > 5 years before the index date was not statistically significant (AOR = 1.126; 95% CI = 0.835–1.464).
These findings indicate that more recent TUD exposure was associated with higher odds of cardiomyopathy, while distant exposure did not differ significantly from non-TUD individuals.

Adjusted odds ratios for cardiomyopathy by time since last TUD diagnosis.
-
Title (revised): Adjusted odds ratios for cardiomyopathy by time since last TUD diagnosis.
-
X-axis: Odds Ratio (reference = non-TUD); vertical line at 1.0 (no association).
-
Plotted values (AOR [95% CI]):
-
Overall 1.376 (1.102–1.598).
-
< 1 year 2.990 (1.978–3.452).
-
1–5 years 1.401 (1.113–1.607).
-
5 years 1.126 (0.835–1.464; NS).
-
The forest plot displays these point estimates and confidence intervals accurately, with < 1 year on the rightmost (highest odds) side and > 5 years closest to the null line (OR ≈ 1).
Figure 2 shows the AOR and 95% CIs estimated based on the time between the most recent smoking cessation disorder (TUD) diagnosis and the diagnosis of cardiomyopathy. Compared with those without TUD, those with TUD exposure closer to the time of cardiomyopathy diagnosis had higher odds ratios for cardiomyopathy, showing a clear recency gradient. The AOR for those diagnosed within < 1 year was 2.990 (95% CI = 1.978–3.452), while for those diagnosed 1–5 years ago, it was 1.401 (95% CI = 1.113–1.607). However, there was no significant association for those exposed more than 5 years ago (AOR = 1.126; 95% CI = 0.835–1.464). This suggests that more recent TUD exposure is associated with cardiomyopathy, while no significant difference is observed for more recent exposure.
Total duration of TUD exposure and cardiomyopathy
Table 5; Fig. 3 summarize the association between total duration of tobacco use disorder (TUD) exposure and cardiomyopathy, derived from the conditional logistic regression model accounting for 1:4 matching (age, sex, index date).
Compared with non-TUD individuals (reference), participants with any TUD exposure prior to the index date had higher odds of cardiomyopathy (AOR = 1.376; 95% CI = 1.102–1.598).
When stratified by exposure duration, longer cumulative exposure was associated with progressively higher odds:
-
< 1 year: AOR = 1.288 (95% CI = 1.060–1.524; p = 0.020). This difference did not reach statistical significance after Bonferroni correction (α = 0.0167).
-
1–5 years: AOR = 1.592 (95% CI = 1.270–1.789; p < 0.001), statistically significant after correction.
-
> 5 years: AOR = 2.743 (95% CI = 1.625–3.891; p < 0.001), statistically significant after correction.
These findings indicate that prolonged TUD exposure (> 1 year) was associated with higher odds of cardiomyopathy, whereas shorter exposure (< 1 year) showed only a nonsignificant trend after adjustment for multiple comparisons.

Adjusted odds ratios for cardiomyopathy by total duration of TUD exposure.
-
X-axis: Adjusted Odds Ratio (aOR, 95% CI); vertical reference line at 1.0 (non-TUD reference).
-
Y-axis: Duration categories - < 1 year/1–5 years/> 5 years.
-
Plotted values:
-
Overall 1.376 (1.102–1.598).
-
< 1 year 1.288 (1.060–1.524; NS after Bonferroni).
-
1–5 years 1.592 (1.270–1.789).
-
> 5 years 2.743 (1.625–3.891).
The forest plot’s points and confidence intervals match these exact values, the axis label reads “Adjusted Odds Ratio (aOR, 95% CI)”, and the duration labels use standardized phrasing (< 1 year/1–5 years/> 5 years).
Figure 3 shows the AORs and 95% CI for the association between total duration of exposure to smoking cessation (TUD) and cardiomyopathy.
Compared with those without TUD, those with a prior TUD diagnosis had a higher odds ratio for cardiomyopathy (overall AOR = 1.376).
After stratification by duration of exposure, longer exposure was associated with a higher odds ratio for cardiomyopathy.
The association for those with less than one year of exposure was no longer significant after Bonferroni correction (AOR = 1.288, p = 0.020).
The results showed a clear time-dependent relationship, indicating that longer cumulative TUD exposure was associated with a stronger association with cardiomyopathy.
Discussion
Principal findings
This population-based, individually matched case–control study demonstrated that individuals with TUD had 1.376-fold higher odds of cardiomyopathy compared with those without TUD.
A recency-related gradient in odds was observed: both more recent and longer cumulative TUD exposures were associated with progressively greater odds of cardiomyopathy.
Specifically, TUD exposure within 1 year before the index date was associated with an AOR of 2.990, exposure 1–5 years before with an AOR of 1.401, and exposure > 5 years before showed no statistically significant association after Bonferroni correction (AOR 1.126, 95% CI 0.835–1.464).
Similarly, total TUD exposure lasting > 5 years corresponded to an AOR of 2.743, indicating higher odds among those with sustained exposure.
Stratified analyses further revealed elevated odds particularly for recent or prolonged TUD exposure, across sex, age groups, seasons, urbanization levels, levels of care, and comorbidity strata.
These findings align with prior evidence linking tobacco exposure to increased odds of cardiovascular disease and heart failure, although relatively few investigations have specifically addressed cardiomyopathy19,20,29,30,31,32,33.
The present results extend those observations by demonstrating a recency-related increase in odds-that is, cardiomyopathy odds rose as the most recent TUD exposure approached the index date-highlighting the temporal and cumulative relevance of TUD exposure within a large nationwide cohort.
Biological mechanisms supporting observed associations
Multiple pathophysiological mechanisms may underlie the observed association between TUD and cardiomyopathy. Tobacco smoke contains oxidizing agents, nicotine, carbon monoxide, and heavy metals, all of which contribute to endothelial dysfunction, increased oxidative stress, inflammation, and myocardial remodeling21,22,34,35,36. Nicotine stimulates sympathetic activity, raising blood pressure and heart rate, and promotes arrhythmogenesis and cardiac hypertrophy23,35,37. Moreover, the psychological and emotional burden associated with chronic heart disease may precipitate increased tobacco use as a coping strategy24,25. Studies on stress, anxiety, and nicotine dependence have shown that individuals with higher trait anxiety exhibit stronger urges to smoke under stress, and that smoking in turn may temporarily relieve negative affect but reinforce a cycle of dependence26,27.
These mechanisms align with our finding that recent and prolonged TUD exposure are both linked to heightened cardiomyopathy risk. Chronic exposure likely exerts cumulative damage to myocardial tissue, explaining the dose-response relationship observed. Furthermore, nicotine’s impact on cardiac ion channels and oxidative stress may explain increased susceptibility to structural and functional abnormalities characteristic of cardiomyopathy28. These biological processes may underlie the association observed in our cohort.
Sex and age differences
Stratified analyses revealed that men with TUD had a higher risk of cardiomyopathy than women (AOR 1.440 vs. 1.251), consistent with prior literature suggesting male sex is associated with greater vulnerability to cardiovascular injury and inflammation in the context of smoking38,39,40,41. Experimental models have also shown sex-dependent differences in the severity of myocarditis and progression to dilated cardiomyopathy (DCM), with testosterone potentiating myocardial inflammation42,43,44,45,46.
Age-stratified results indicated higher risk in both middle-aged and older adults, mirroring general patterns of increased cardiomyopathy prevalence with age47,48,49,50,51. However, our data also showed elevated risk among younger individuals (20–49 years), suggesting that early-onset TUD may initiate subclinical myocardial damage, warranting earlier intervention and surveillance.
Socioeconomic disparities and cardiomyopathy risk
Although the cited Canadian data pertain to general heart disease rather than cardiomyopathy specifically52,53,54, the pattern of increased cardiovascular risk in low-income groups is reflected in our findings. We found that individuals from low-income households had significantly higher cardiomyopathy risk (AOR = 1.523), even after controlling for comorbidities and health care access.
This is consistent with social causation theory, which posits that structural inequalities—such as limited access to healthy food, stable housing, and medical care—contribute to adverse health outcomes54,55. In our cohort, low-income individuals may be more likely to experience chronic stress, greater TUD severity, and delayed diagnosis or treatment, all of which may accelerate cardiac pathology.
Metabolic and hemodynamic implications of smoking
Tobacco use is associated with metabolic dysregulation, including insulin resistance, hyperinsulinemia, and visceral fat accumulation-all of which contribute to the development of diabetes and cardiac dysfunction56,57,58,59,60,61. Our study adjusted for diabetes mellitus, yet TUD remained a significant independent risk factor, suggesting additive or synergistic effects beyond glycemic control.
In terms of blood pressure, acute nicotine exposure increases sympathetic tone, while chronic effects are less clear. Some studies report elevated systolic blood pressure among older smokers62, while others find no significant differences or even lower values63,64. Despite this inconsistency, the pro-hypertensive potential of nicotine may partially mediate the relationship between TUD and cardiomyopathy, especially among middle-aged men65,66,67,68.
Lipid abnormalities and renal comorbidity
Smoking has been associated with elevated LDL, triglycerides, and reduced HDL levels69. While one study paradoxically reported higher HDL in smokers, this contradicts most epidemiologic evidence and may reflect confounding factors or population-specific effects. Dyslipidemia promotes atherosclerosis, endothelial injury, and myocardial stress, which may contribute to cardiomyopathy, particularly in ischemic or mixed phenotypes70,71.
In addition, smoking has been linked to the onset and progression of CKD, which itself is a risk factor for cardiomyopathy72,73,74. Although our regression models adjusted for CKD, the persistence of TUD as an independent risk factor suggests direct cardiac toxicity from tobacco exposure or unmeasured renal-cardiac interactions. Some renal pathologies may be more susceptible to tobacco-induced vascular injury than others75.
Interpretation and implications
Our study reinforces previous findings regarding the cardiotoxic effects of tobacco use while contributing novel evidence of dose-response and temporal patterns specific to cardiomyopathy. The persistence of risk despite adjustment for conventional cardiovascular comorbidities indicates that tobacco exposure may play a more direct and independent role in myocardial pathology than previously appreciated. These findings support public health strategies aimed at early detection and cessation of TUD as a means to prevent not only coronary artery disease but also structural heart diseases such as cardiomyopathy.
Strengths and limitations
Strengths
This study possesses several notable methodological strengths that enhance the reliability and relevance of its findings. First, we utilized Taiwan’s NHIRD, which covers over 99% of the population, thereby ensuring near-complete national representation and minimizing selection bias. Second, the large sample size and long observation window (2000–2015) provided sufficient statistical power to detect meaningful associations between TUD and cardiomyopathy, even among subgroups. Third, the study employed a robust matching strategy (1:4 ratio) by age, sex, and index year, followed by conditional logistic regression to control for potential confounders. Fourth, we incorporated temporal elements of TUD exposure, including latency and cumulative duration, allowing us to evaluate not just the presence but also the timing and intensity of the exposure-risk relationship.
To our knowledge, this is the first nationwide, population-based study in an Asian setting to specifically evaluate the relationship between TUD and cardiomyopathy using longitudinal claims data. While our results align with previous studies on the cardiovascular risks of smoking, our analysis advances the field by providing empirical evidence on the dose-response and temporality of TUD exposure. Importantly, we ensured that all TUD exposures preceded the diagnosis of cardiomyopathy in our analysis, thereby reducing concerns of reverse causality and reinforcing the plausibility of a causal relationship.
Limitations
Several limitations of this study should be acknowledged. First, the identification of TUD relied on ICD-9-CM diagnostic codes from administrative claims data. Although widely used in population-based research, such codes may be subject to underreporting or misclassification, particularly for behavioral health conditions like TUD, which are often stigmatized or underdiagnosed. This may lead to nondifferential misclassification and potential attenuation of the observed associations.
Second, the retrospective case-control design precludes definitive causal inference. While temporal ordering was preserved by ensuring that TUD diagnoses preceded cardiomyopathy diagnoses, residual confounding and unmeasured variables—such as genetic predisposition, lifestyle factors (e.g., physical activity, diet), or environmental exposures-could influence the observed associations.
Third, selection and information biases may exist. Although the NHIRD provides comprehensive coverage of the Taiwanese population, certain subpopulations (e.g., undocumented individuals or those seeking alternative care) may be underrepresented. In addition, coding practices may vary across institutions and over time, further contributing to data variability.
Fourth, interaction effects between TUD and other covariates—such as age, sex, or comorbid conditions—were not formally assessed. Future studies may benefit from including such interaction analyzes to clarify differential risk patterns.
Fifth, the study period spanned from 2000 to 2015. While this long duration allowed us to assess long-term associations, changes in smoking patterns, diagnostic criteria, and treatment approaches since then may limit the generalizability of our findings to present-day populations.
Finally, exposure Classification Bias in Early Index-Year Cases. For patients diagnosed with cardiomyopathy in the year 2000, the time available to define prior TUD exposure may be insufficient due to the lack of lookback data before January 2000. Including these cases in the same exposure classification scheme as patients from later years could result in exposure misclassification and biased effect estimates. To address this concern, we conducted a sensitivity analysis excluding cardiomyopathy cases with an index date in 2000. The association between TUD and cardiomyopathy remained statistically significant (AOR = 1.264, 95% CI = 1.085–1.431, p = 0.001), supporting the robustness of the primary findings (Table S3).
Conclusion
In this large, nationwide, individually matched case-control study, TUD was associated with higher odds of cardiomyopathy. Conditional logistic regression analyses demonstrated that both recent and prolonged TUD exposures were linked to greater odds of cardiomyopathy, even after adjustment for demographic and clinical covariates.
A clear recency-related gradient in odds was observed: individuals with TUD exposure within one year before the index date had the highest adjusted odds (AOR = 2.990), followed by those with exposure one to five years prior (AOR = 1.401). In contrast, exposure beyond five years before the index date showed no statistically significant association after Bonferroni correction (AOR = 1.126, 95% CI = 0.835–1.464). Similarly, longer cumulative TUD exposure (> 5 years) was associated with higher odds of cardiomyopathy (AOR = 2.743), indicating that the odds increased with both recency and duration of TUD.
These findings suggest that recent and sustained tobacco use disorder are strongly associated with elevated odds of cardiomyopathy, emphasizing the importance of early cessation and sustained abstinence to mitigate adverse cardiac outcomes. However, because this study was case–control in design, causal inference cannot be established; the associations observed reflect statistical relationships in odds rather than direct causality.
Data availability
The data that supports the findings of this study are available from the corresponding author upon reasonable request.
References
Maron, B. J. et al. American heart association quality of care and outcomes research and functional genomics and translational biology interdisciplinary working groups. Circulation 113, 1807–1816. https://doi.org/10.1161/CIRCULATIONAHA.106.174287 (2006).
Arbustini, E. et al. The MOGE(S) classification of cardiomyopathy for clinicians. J. Am. Coll. Cardiol. 64, 304–318. https://doi.org/10.1016/j.jacc.2014.05.027 (2014).
Report of the WHO/ISFC task force on the definition and classification of cardiomyopathies. Br. Heart J. ;44:672. doi: https://doi.org/10.1136/hrt.44.6.672. (1980).
Richardson, P. et al. Report of the 1995 world health Organization/International society and federation of cardiology task force on the definition and classification of cardiomyopathies. Circulation 93, 841–842 (1996).
Basit, H. et al. Hypertrophic Cardiomyopathy. [Updated 2024 Jun 7]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025. Available from: https://www.ncbi.nlm.nih.gov/books/NBK430788/
Glavaški, M., Velicki, L. & Vučinić, N. Hypertrophic cardiomyopathy: genetic Foundations, Outcomes, Interconnections, and their modifiers. Med. (Kaunas). 59 (8), 1424. https://doi.org/10.3390/medicina59081424 (2023).
Brown, K. N. et al. Restrictive Cardiomyopathy. [Updated 2023 Jul 30]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025. Available from: https://www.ncbi.nlm.nih.gov/books/NBK537234/
Rapezzi, C. et al. Restrictive cardiomyopathy: definition and diagnosis. Eur. Heart J. 43 (45), 4679–4693. https://doi.org/10.1093/eurheartj/ehac543 (2022).
Varrenti, M. et al. Arrhythmogenic cardiomyopathy: Definition, classification and arrhythmic risk stratification. J. Clin. Med. 13 (2), 456. https://doi.org/10.3390/jcm13020456 (2024).
Spadotto, A. et al. The challenges of diagnosis and treatment of arrhythmogenic cardiomyopathy: are we there yet? Rev. Cardiovasc. Med. 23 (8), 283. https://doi.org/10.31083/j.rcm2308283 (2022).
Ahmad, S. A. et al. Takotsubo Cardiomyopathy. [Updated 2023 May 22]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025. Available from: https://www.ncbi.nlm.nih.gov/books/NBK430798/
Assad, J., Femia, G., Pender, P., Badie, T. & Rajaratnam, R. Takotsubo syndrome: A review of Presentation, diagnosis and management. Clin. Med. Insights Cardiol. 16, 11795468211065782. https://doi.org/10.1177/11795468211065782 (2022).
Sethi, Y. et al. Broken heart syndrome: evolving molecular mechanisms and principles of management. J. Clin. Med. 12 (1), 125. https://doi.org/10.3390/jcm12010125 (2022).
Singh, T. et al. Takotsubo Syndrome: Pathophysiology, Emerging Concepts, and Clinical Implications. Circulation. 145(13):1002–1019. (2022). https://doi.org/10.1161/CIRCULATIONAHA.121.055854. Epub 2022 Mar 28. Erratum in: Circulation. 2022;145(20):e1053. doi: 10.1161/CIR.0000000000001075.
Néstor, S. et al. AND DUAL DISORDERS joint statement by the Spanish psychiatry society and the Spanish dual disorders society. Actas Esp. Psiquiatr. 50 (Supplement), 77–138 (2022). Epub 2022 Jun 1.
Li, Y., Cao, G. Y., Jing, W. Z., Liu, J. & Liu, M. Global trends and regional differences in incidence and mortality of cardiovascular disease, 1990–2019: findings from 2019 global burden of disease study. Eur. J. Prev. Cardiol. 30 (3), 276–286. https://doi.org/10.1093/eurjpc/zwac285 (2023).
McKee, A. & Morley, J. E. Obesity in the elderly. (eds Feingold, K. R. et al.) https://www.ncbi.nlm.nih.gov/books/NBK532533/ (Endotext. MDText.com,Inc., South Dartmouth, MA, 2018).
Sapna, F. et al. Advancements in heart failure management: A comprehensive narrative review of emerging therapies. Cureus 15 (10), e46486. https://doi.org/10.7759/cureus.46486 (2023).
Yoo, J. E. et al. Smoking behavior change and the risk of heart failure in patients with type 2 diabetes: nationwide retrospective cohort study. JMIR Public. Health Surveill. 10, e46450. https://doi.org/10.2196/46450 (2024).
Duncan, M. S. et al. Association of smoking cessation with subsequent risk of cardiovascular disease. JAMA 322 (7), 642–650. https://doi.org/10.1001/jama.2019.10298 (2019).
Singh, N., Wanjari, A. & Sinha, A. H. Effects of nicotine on the central nervous system and sleep quality in relation to other stimulants: A narrative review. Cureus 15 (11), e49162. https://doi.org/10.7759/cureus.49162 (2023).
Hamann, S. L. et al. Electronic cigarette harms: aggregate evidence shows damage to biological systems. Int. J. Environ. Res. Public. Health. 20 (19), 6808. https://doi.org/10.3390/ijerph20196808 (2023).
Łuczyk, R. J. et al. What increases smokers’ stress? Degree of nicotine dependence and motivation to quit smoking in people after myocardial infarction. J. Clin. Med. 14 (5), 1545. https://doi.org/10.3390/jcm14051545 (2025).
Aslam, S. P. et al. Nicotine Addiction and Smoking: Health Effects and Interventions (Nursing) [Updated 2024 Aug 8]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025. Available from: https://www.ncbi.nlm.nih.gov/books/NBK568714/
United States Public Health Service Office of the Surgeon General; National Center for Chronic Disease Prevention and Health Promotion (US) Office on Smoking and Health. Smoking Cessation: A Report of the Surgeon General [Internet]. Washington (DC): US Department of Health and Human Services. Chapter 6, Interventions for Smoking Cessation and Treatments for Nicotine Dependence. (2020). Available from: https://www.ncbi.nlm.nih.gov/books/NBK555596/
TaiwanData from Ministry of Health and Welfare. Taiwan Data from Ministry of Health and Welfare. Available online: (2019). https://www.mohw.gov.tw/lp-137-2.html (accessed on 22 January 2025).
Ministry of Health and Welfare. The Protection of Children and Youths Welfare and Rights Act. Available online: January (2025). https://law.moj.gov.tw/ENG/LawClass/LawAll.aspx?pcode=D0050001 (accessed on 22.
Charlson, M. E., Szatrowski, T. P., Peterson, J. & Gold, J. A. New method of classifying prognostic comorbidity in longitudinal studies: development and validation. J. Chronic Dis. 40, 373–383 (1987).
Khan, S. S. et al. Cigarette smoking and competing risks for fatal and nonfatal cardiovascular disease subtypes across the life course. J. Am. Heart Assoc. 10, e021751. https://doi.org/10.1161/JAHA.121.021751 (2021).
Wu, A. D. et al. Smoking cessation for secondary prevention of cardiovascular disease. Cochrane Database Syst. Rev. 8, CD014936 (2022).
Liu, M., Zheng, M. & He, S. Association between tobacco smoking and heart disease in older adults: a cross-sectional study based on the Chinese longitudinal healthy longevity survey. Ann. Transl Med. 11 (2), 63. https://doi.org/10.21037/atm-22-6344 (2023). Epub 2023 Jan 13.
Zhang, M. et al. Trends in low-density lipoprotein cholesterol level among Chinese young adults hospitalized with first acute myocardial infarction. Ann. Transl Med. 9, 1536. https://doi.org/10.21037/atm-21-4480 (2021).
Kaplan, A. et al. Sex differences in cardiac remodeling post myocardial infarction with acute cigarette smoking. Biol. Sex. Differ. 13, 36. https://doi.org/10.1186/s13293-022-00446-y (2022).
Caliri, A. W., Tommasi, S. & Besaratinia, A. Relationships among smoking, oxidative stress, inflammation, macromolecular damage, and cancer. Mutat. Res. Rev. Mutat. Res. 787, 108365. https://doi.org/10.1016/j.mrrev.2021.108365 (2021).
Oshunbade, A. A. et al. Cigarette Smoking, incident coronary heart Disease, and coronary artery calcification in black adults: the Jackson heart study. J. Am. Heart Assoc. 10, e017320. https://doi.org/10.1161/JAHA.120.017320 (2021).
Lin, G. M. et al. Muscular strength and carotid Intima-Media thickness in physically fit young adults: the CHIEF atherosclerosis study. J. Clin. Med. 11, 5462. https://doi.org/10.3390/jcm11185462 (2022).
Farra, Y. M. et al. Structural and functional remodeling of the female Apoe(-/-) mouse aorta due to chronic cigarette smoke exposure. Am. J. Physiol. Heart Circ. Physiol. 320, H2270–H2282. https://doi.org/10.1152/ajpheart.00893.2020 (2021).
Lee, L. V. & Foody, J. M. Women and heart disease. Cardiol. Clin. 29, 35–45 (2011).
McNamara, D. M. et al. Clinical and demographic predictors of outcomes in recent onset dilated cardiomyopathy: results of the IMAC (Intervention in myocarditis and acute Cardiomyopathy)-2 study. J. Am. Coll. Cardiol. 58, 1112–1118. https://doi.org/10.1016/j.jacc.2011.05.033 (2011).
Regitz-Zagrosek, V. & Seeland, U. Sex and gender differences in myocardial hypertrophy and heart failure. Wien Med. Wochenschr. 161, 109–116. https://doi.org/10.1007/s10354-011-0892-8 (2011).
Roger, V. L. et al. Executive summary: heart disease and stroke statistics–2012 update: a report from the American heart association. Circulation 125, 188–197. https://doi.org/10.1161/CIR.0b013e3182456d46 (2012).
Woodruff, J. F. Viral myocarditis. A review. Am. J. Pathol. 101, 425–484 (1980).
Cocker, M. S., Abdel-Aty, H., Strohm, O. & Friedrich, M. G. Age and gender effects on the extent of myocardial involvement in acute myocarditis: a cardiovascular magnetic resonance study. Heart 95, 1925–1930. https://doi.org/10.1136/hrt.2008.164061 (2009).
Cooper, L. T. et al. Myocardial recovery in peripartum cardiomyopathy: prospective comparison with recent onset cardiomyopathy in men and nonperipartum women. J. Card Fail. 18, 28–33. https://doi.org/10.1016/j.cardfail.2011.09.009 (2012).
Lyden, D. C., Olszewski, J., Feran, M., Job, L. P. & Huber, S. A. Coxsackievirus B-3-induced myocarditis effect of sex steroids on viremia and infectivity of cardiocytes. Am. J. Pathol. 126, 432–438 (1987).
Fairweather, D., Cooper, L. T. Jr & Blauwet, L. A. Sex and gender differences in myocarditis and dilated cardiomyopathy. Curr. Probl. Cardiol. 38 (1), 7–46. https://doi.org/10.1016/j.cpcardiol.2012.07.003 (2013).
Heron, M. & Deaths Leading Causes for 2019. National Vital Statistics Reports Vol. 709 (National Center for Health Statistics, 2021).
Centers for Disease Control and Prevention. About heart disease. Available from: https://www.cdc.gov/heartdisease/about.htm
Ford, E. S. et al. Explaining the decrease in U.S. Deaths from coronary disease, 1980–2000. N Engl. J. Med. 356 (23), 2388–2398 (2007).
Heron, M. & Anderson, R. N. Changes in the Leading Cause of Death: Recent Patterns in Heart Disease and Cancer mortality. NCHS Data Brief, No 254 (National Center for Health Statistics, 2016).
Sanchis-Gomar, F., Perez-Quilis, C., Leischik, R. & Lucia, A. Epidemiology of coronary heart disease and acute coronary syndrome. Ann. Transl Med. 4 (13), 256 (2016).
Lee, D. S. et al. Trends in risk factors for cardiovascular disease in canada: temporal, socio-demographic and geographic factors. CMAJ 181 (3–4), E55–66. https://doi.org/10.1503/cmaj.081629 (2009). Epub 2009 Jul 20.
Butler-Jones, D. Report on the state of public health in Canada. Addressing health inequalities. Ottawa, ON: Public Health Agency of Canada; (2008). Available from: www.phac-aspc.gc.ca/cphorsphc-respcacsp/2008/fr-rc/pdf/CPHO-Report-e.pdf. Accessed 2014 Jul 24.
Eaton, W. W. & Muntaner, C. Socioeconomic stratification and mental disorder. In A Handbook for the Study of Mental health. Social contexts, Theories and Systems (eds Horwitz, A. V. & Scheid, T. L.) 259–283 (Cambridge University Press, 1999).
Lemstra, M., Rogers, M. & Moraros, J. Income and heart disease: neglected risk factor. Can. Fam Physician. 61 (8), 698–704 (2015).
Public Health Agency of Canada [website] Tracking heart disease and stroke in Canada. Ottawa, ON: Public Health Agency of Canada. (2009). Available from: www.phac-aspc.gc.ca/publicat/2009/cvd-avc/index-eng.php. Accessed 2013 Apr 3.
Public Health Agency of Canada [website] Cardiovascular disease—economic burden of illness. Ottawa, ON: Public Health Agency of Canada. (2012). Available from: www.phac-aspc.gc.ca/cd-mc/cvd-mcv/cvd_ebic-mcv_femc-eng.php. Accessed 2013 Apr 3.
Heart and Stroke Foundation of Canada [website] Statistics. Ottawa, ON: Heart and Stroke Foundation of Canada. (2013). Available from: www.heartandstroke.com/site/?c=ikIQLcMWJtE&b=3483991. Accessed 2013 Apr 3.
Facchini, F. S., Hollenbeck, C. B., Jeppesen, J., Chen, Y. D. & Reaven, G. M. Insulin resistance and cigarette smoking. Lancet 339 (8802), 1128–1130 (1992).
Eliasson, B. Cigarette smoking and diabetes. Prog. Cardiovasc. Dis. 45 (5), 405–413 (2003).
Chiolero, A., Faeh, D., Paccaud, F. & Cornuz, J. Consequences of smoking for body Weight, body fat Distribution, and insulin resistance. Am. J. Clin. Nutr. 87 (4), 801–809 (2008).
Primatesta, P., Falaschetti, E., Gupta, S., Marmot, M. G. & Poulter, N. R. Association between smoking and blood pressure: evidence from the health survey for England. Hypertension 37 (2), 187–193 (2001).
Green, M. S., Jucha, E. & Luz, Y. Blood pressure in smokers and nonsmokers: epidemiologic findings. Am. Heart J. 111, 932–940. https://doi.org/10.1016/0002-8703(86)90645-9 (1986).
Luehrs, R. E. et al. Cigarette smoking and longitudinal associations with blood pressure: the CARDIA study. J. Am. Heart Assoc. 10, e019566. https://doi.org/10.1161/JAHA.120.019566 (2021).
Rhee, M. Y., Na, S. H., Kim, Y. K., Lee, M. M. & Kim, H. Y. Acute effects of cigarette smoking on arterial stiffness and blood pressure in male smokers with hypertension. Am. J. Hypertens. 20, 637–641. https://doi.org/10.1016/j.amjhyper.2006.12.017 (2007).
Au Bich, T. et al. The association between smoking and hypertension in a population-based sample of Vietnamese men. J. Hypertens. 28, 245–250. https://doi.org/10.1097/HJH.0b013e32833310e0 (2010).
Al-Safi, S. A. Does smoking affect blood pressure and heart rate? Eur. J. Cardiovasc. Nurs. 4, 286–289. https://doi.org/10.1016/j.ejcnurse.2005.03.004 (2005).
Primatesta, P., Falaschetti, E., Gupta, S., Marmot, M. G. & Poulter, N. R. J. H. Association between smoking and blood pressure: evidence from the health survey for England. Hypertension 37, 187–193. https://doi.org/10.1161/01.hyp.37.2.187 (2001).
Craig, W. Y., Palomaki, G. E. & Haddow, J. E. Cigarette smoking and serum lipid and lipoprotein concentrations: an analysis of published data. BMJ 298 (6676), 784–788 (1989).
Yang, H., Negishi, K., Otahal, P. & Marwick, T. H. Clinical prediction of incident heart failure risk: A systematic review and Meta-Analysis. Open. Heart. 2 (1), e000222 (2015).
Wilhelmsen, L., Rosengren, A., Eriksson, H. & Lappas, G. Heart failure in the general population of men: Morbidity, risk Factors, and prognosis. J. Intern. Med. 249 (3), 253–261 (2008).
Bleyer, A. J. et al. Tobacco, hypertension, and vascular disease: risk factors for renal functional decline in an older population. Kidney Int. 57 (5), 2072–2079. https://doi.org/10.1046/j.1523-1755.2000.00056.x (2000).
Yamagata, K. et al. Risk factors for chronic kidney disease in a community-based population: a 10-year follow-up study. Kidney Int. 71 (2), 159–166. https://doi.org/10.1038/sj.ki.5002017 (2007).
Ejerblad, E. et al. Association between smoking and chronic renal failure in a nationwide population-based case-control study. J. Am. Soc. Nephrol. 15 (8), 2178–2185. https://doi.org/10.1097/01.ASN.0000135048.35659.10 (2004).
Yacoub, R. et al. Association between smoking and chronic kidney disease: a case control study. BMC Public. Health. 10, 731. https://doi.org/10.1186/1471-2458-10-731 (2010).
Acknowledgements
We appreciate the support from the Tri-Service General Hospital Research Foundation and the Medical Affairs Bureau, Ministry of Defense, Taiwan, ROC. We also appreciate the database provided by the Health and Welfare Data Science Center, Ministry of Health and Welfare (HWDC, MOHW).
Funding
This study was funded by the Tri-Service General Hospital, grant numbers: TSGH-A-114,010, TSGH-B-114,022, TSGH-D-114,196, and the sponsor has no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Author information
Authors and Affiliations
Contributions
P.-Y.Y.,T.-H.W., Y.-C.H., L.-Y. F., C.-H.C., and W.-C.C.: conception and design, analysis and interpretation of the data, critical review, and approval of the final version submitted for publication. P.-C.Y., S.-H.H., B.-L.W., H.-T.H., C.-T.T., and Y.-C.H.: statistical analysis, critical review, and approval of the final version submitted for publication. P.-C.Y., S.-H.H., R.-J.C., B.-L.W., H.-T.H., P.-Y.Y., T.-H.W., Y.-C.H., L.-Y. F., C.-H.C., and W.-C.C.: drafting of the paper, critical review, and approval of the final version submitted for publication. All authors have read and agreed to the published version of the manuscript.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Yu, PY., Hsin, HT., Yu, PC. et al. Tobacco use disorder is associated with increased risk of cardiomyopathy in a population-based study from Taiwan. Sci Rep 16, 708 (2026). https://doi.org/10.1038/s41598-025-30328-3
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-30328-3
