
Abstract
While metabolic dysfunction-associated steatotic liver disease (MASLD) increasingly affects non-obese individuals, current screening approaches show poor performance in this population. We investigated whether the Clínica Universidad de Navarra-Body Adiposity Estimator (CUN-BAE) could better identify MASLD risk than traditional measures in non-obese adults, and examined how the triglyceride-glucose (TyG) index might mediate this relationship. Using data from the Dryad public database, we followed 16,173 Chinese non-obese adults (BMI < 25 kg/m²) without baseline MASLD for 5 years. MASLD diagnosis relied on abdominal ultrasonography. We applied multivariable logistic regression to assess cross-sectional associations and Cox models for incident disease risk. Restricted cubic splines revealed dose-response patterns in sex-stratified analyses, while structural equation modeling quantified TyG index mediation effects. Our cohort included 8,483 men and 7,690 women. After full adjustment, each standard deviation increased in CUN-BAE linked to 35% higher MASLD risk (HR = 1.35, 95% CI: 1.29–1.41, P < 0.001). Comparing top versus bottom tertiles showed 95% increased risk (HR = 1.95, 95% CI: 1.74–2.18, P < 0.001). Five-year cumulative incidence rose from 8.4% (lowest tertile) to 15.8% (middle) to 18.9% (highest tertile, Log-rank P < 0.0001). Cubic spline analysis uncovered sex differences: women showed a sharp risk increase above CUN-BAE 31.2, while men displayed more gradual, linear patterns. The TyG index accounted for 24.7% of the CUN-BAE-MASLD association (P < 0.001). CUN-BAE effectively predicts MASLD development in Chinese non-obese adults through clear dose-response relationships that differ by sex. Since TyG index only partially explains this association, insulin resistance appears important but insufficient to account for the full relationship. CUN-BAE could serve as a practical screening tool to identify high-risk individuals missed by conventional BMI-based approaches, enabling more precise risk stratification in non-obese populations.
Similar content being viewed by others

Introduction
Metabolic dysfunction-associated steatotic liver disease (MASLD), formerly called non-alcoholic fatty liver disease (NAFLD), has emerged as the leading cause of chronic liver disease worldwide, affecting roughly one-quarter to one-third of the global population and posing substantial challenges for healthcare systems1,2. Beyond its direct hepatic consequences including cirrhosis and hepatocellular carcinoma, MASLD intertwines with cardiovascular disease, type 2 diabetes, and chronic kidney disease, creating a web of comorbidities that elevate patient mortality while straining healthcare resources3,4.
While MASLD was historically viewed as a disease of obesity, growing evidence reveals that many patients maintain normal body mass index (BMI) values, with this phenomenon particularly pronounced in Asian populations where 7–20% of individuals develop MASLD despite normal weight status5,6,7. These non-obese patients present a clinical paradox: they typically show fewer traditional metabolic risk factors—including lower rates of diabetes, hypertension, and dyslipidemia—yet often develop more severe liver fibrosis and face higher cardiovascular mortality compared to their obese counterparts8,9. This counterintuitive pattern creates diagnostic challenges, as clinicians may dismiss MASLD risk in normal-weight individuals, potentially delaying critical interventions and missing early treatment windows10,11. MASLD diagnosis still depends heavily on imaging studies and liver biopsy, yet these approaches face practical barriers including high costs, limited availability, and variable reproducibility across different settings12,13. Simple, cost-effective screening tools would therefore fill a critical gap in early MASLD detection, especially among non-obese individuals where the need for accessible risk assessment has become increasingly urgent14.
The Clínica Universidad de Navarra-Body Adiposity Estimator (CUN-BAE) calculates body fat content using age, sex, and BMI parameters, with validation studies confirming its accuracy in Asian populations15. Unlike conventional BMI measurements, CUN-BAE captures individual variations in fat distribution and shows superior ability to detect “hidden obesity”—cases where normal BMI masks elevated body fat percentage16,17. These features make CUN-BAE particularly valuable for metabolic risk assessment in non-obese individuals, where traditional anthropometric measures often fall short. Growing research has established the triglyceride-glucose index (TyG) as a robust surrogate for insulin resistance, making it increasingly valuable in metabolic disease risk assessment18,19. Evidence suggests that TyG index correlates strongly with both MASLD development and progression, potentially bridging abnormal body fat distribution with hepatic steatosis20,21. Yet among non-obese individuals, the relationship between CUN-BAE and MASLD remains poorly understood, and TyG index mediating role in this population requires investigation.
Although studies have explored relationships between body fat assessment indicators and MASLD, existing research has significant limitations including predominantly cross-sectional designs that cannot establish causal relationships and focus mainly on obese populations with insufficient attention to non-obese individuals22,23. Moreover, there is a lack of large-sample, long-term longitudinal cohort studies to validate predictive efficacy in clinical practice. Prospective cohort designs offer the temporal framework needed to establish exposure-outcome sequences, strengthening causal inference beyond cross-sectional observations. Non-obese populations warrant dedicated investigation, as their MASLD risk profiles and progression trajectories may diverge substantially from patterns seen in obese cohorts.
Therefore, this study aimed to evaluate the association between body adiposity estimated by CUN‑BAE and the risk of metabolic dysfunction–associated steatotic liver disease (MASLD) in non‑obese Chinese adults, and to explore whether insulin resistance, estimated using the TyG index, mediates this association.
Methods
Study design and data sources
This study is a secondary analysis based on a public database, employing a longitudinal cohort design. The original data were sourced from the Dryad public database (repository at http://datadryad.org/ with the doi:https://doi.org/10.5061/dryad.1n6c424 in compliance with Dryad’s terms of service, with data freely available for researchers. The study population comprised 16,173 non-obese participants without MASLD at baseline, with a prospective 5-year follow-up period.
The original study protocol was approved by the Ethics Committee of Wenzhou People’s Hospital, and all participants provided informed consent. As a secondary analysis of a publicly available dataset, this study did not require additional ethical review.
Study population and inclusion/exclusion criteria
The study population consisted of non-obese Chinese adults. Baseline exclusion criteria were as follows: (1) incomplete clinical data or loss to follow-up; (2) current use of oral antihypertensive, lipid-lowering, or antidiabetic medications; (3) excessive alcohol consumption (> 140 g/week for men, > 70 g/week for women); (4) presence of MASLD, autoimmune hepatitis, viral hepatitis, or chronic liver disease of known etiology; (5) low-density lipoprotein cholesterol (LDL-C) > 3.12 mmol/L (According to the internal laboratory standard adopted in the database, values ≤ 3.12 mmol/L (120 mg/dL) were defined as within the normal range, which slightly differs from the national guideline upper limit (3.4 mmol/L). This classification was retained to ensure data consistency); (6) BMI ≥ 25 kg/m²(Fig. 1).

Flow chart. Abbreviations: MASLD-metabolic dysfunction-associated steatotic liver disease; LDL-C - Low-density lipoprotein cholesterol; BMI - Body mass index; n-number.
Data collection
Medical history and lifestyle habits were collected through questionnaire surveys conducted by trained physicians. Blood pressure measurements were obtained using automated sphygmomanometers in a quiet environment. Height and weight were measured with participants wearing light clothing and no shoes.
Fasting blood samples were collected in the early morning after overnight fasting to assess biochemical parameters, including alanine aminotransferase (ALT), aspartate aminotransferase (AST), total protein (TP), albumin (ALB), globulin (GLB), creatinine (Cr), blood urea nitrogen (BUN), fasting plasma glucose (FPG), uric acid (UA), total cholesterol (TC), triglycerides (TG), high-density lipoprotein cholesterol (HDL-C), and LDL-C levels.
Definitions and variable calculations
CUN-BAE Index = (0.00021 × BMI2 × age) - (0.005 × BMI2 × sex) - (0.02 × BMI × age) + (0.181 × BMI × sex) − (0.026 × BMI2) + (3.172 × BMI) + (10.689 × sex) + (0.503 × age) − 44.988; where sex is defined as male = 0, female = 125;
BMI (kg/m²) = weight (kg)/height² (m²);
TyG = Ln[FBG (mg/dL) ×TG (mg/dL)/2;
eGFR (mL/min/1.73 m²) = 186 × (Scr)⁻¹·¹⁵⁴ × (Age)⁻⁰·²⁰³ × (0.742 if female)26;
MASLD diagnostic criteria
MASLD was diagnosed by abdominal ultrasonography according to the standards recommended by the Chinese Society of Hepatology. All ultrasonographic examinations were performed using standardized procedures by experienced radiologists who had completed formal training in hepatic imaging. Each examination was independently interpreted by two radiologists who were blinded to all clinical and laboratory information of the participants, and any discrepancies were resolved by consensus. MASLD was defined as the presence of at least two of the following three abnormal ultrasound findings: (1) diffuse enhancement of liver near-field echoes (“bright liver”); (2) liver echogenicity greater than that of the kidney; and (3) vascular blurring and gradual attenuation of far-field echoes.
Statistical analysis
Missing data were handled by excluding variables with > 25% missing values and imputing those with ≤ 25% missing values using random forest methodology(Supplementary Table S2). Sensitivity analyses were conducted before and after imputation to ensure data stability (Supplementary Table S2). Participants were categorized into tertiles based on CUN-BAE values for descriptive analysis, with CUN-BAE standardized using Z-scores for regression analyses. Continuous variables are presented as mean ± standard deviation. Between-group comparisons were performed using one-way ANOVA or non-parametric tests for continuous variables.
Cumulative incidence of MASLD was estimated using the Kaplan-Meier method with log-rank tests comparing survival distributions between CUN-BAE tertiles. Cox proportional hazards regression models assessed associations between standardized CUN-BAE and incident MASLD using progressive adjustment: Model 1 adjusted for liver function markers (ALT, AST, TP, ALB, GLB); Model 2 additionally adjusted for renal function markers (BUN, CR, UA) based on Model 1; Model 3 further added lipid profiles (TC, TG, HDL-C, LDL-C) to Model 2; and Model 4 additionally incorporated metabolic parameters and blood pressure (FBG, SBP, DBP) to Model 3.
Restricted cubic spline regression was used to examine nonlinear dose–response relationships, with optimal knot placement determined by the Akaike Information Criterion. Sex‑stratified analyses were performed to explore potential effect modification. Further stratified analyses across demographic and clinical subgroups assessed heterogeneity using likelihood ratio tests. Mediation analysis was conducted to evaluate the TyG index as a potential mediator, applying a regression‑based causal mediation framework (generalized linear model with a probit link for MASLD and linear regression for TyG). Models were adjusted for age, sex, ALT, AST, TP, ALB, GLB, BUN, CR, UA, TC, HDL‑C, LDL‑C, SBP, and DBP. Nonparametric bootstrapping (1,000 resamples, percentile method) was applied to obtain 95% confidence intervals for the total, direct, and indirect effects and to calculate mediation proportions. Sensitivity analyses included comparison of complete case versus imputed data analyses, evaluation of association stability across adjustment models, and alternative CUN-BAE categorization approaches to assess result robustness. All analyses were performed using R software version 4.2.0 and EmpowerStats version 4.0, with two-sided P-values < 0.05 considered statistically significant. Given the exploratory nature of this analysis, P values were not adjusted for multiple comparisons, and the results should be interpreted with caution.
Results
Baseline characteristics of study population
This study included 16,173 participants, comprising 8,483 males and 7,690 females. Based on the presence of MASLD, participants were categorized into MASLD and non-MASLD groups. During the 5-year follow-up period, 1,294 males (15.25%) and 1,028 females (13.37%) were diagnosed with MASLD.As shown in Table 1, for both males and females, the MASLD group demonstrated significantly higher age, weight, height, BMI, systolic blood pressure (SBP), and diastolic blood pressure (DBP) compared to the non-MASLD group (all P < 0.001).
Regarding biochemical parameters, the MASLD group exhibited significantly elevated levels of ALT, AST, CR, UA, TC, TG, LDL-C, and FPG, while HDL-C and eGFR levels were significantly decreased (all P < 0.001). In males, CUN-BAE was significantly higher in the MASLD group (21.82 ± 3.14) compared to the non-MASLD group (18.36 ± 4.35, P < 0.001). In females, CUN-BAE was similarly elevated in the MASLD group (32.93 ± 2.82) versus the non-MASLD group (29.36 ± 3.97, P < 0.001). Additionally, the TyG index was significantly higher in the MASLD group (P < 0.001).
For both sexes, no statistically significant differences were observed between MASLD and non-MASLD groups for TP, ALB, GLB and BUN.
Association analysis between CUN-BAE and MASLD incident risk
To evaluate the association between CUN-BAE z-score and MASLD incident risk, we employed multivariable logistic regression analysis. The analysis was based on the entire study population and constructed four progressively adjusted regression models to examine result robustness: Model 1 adjusted for liver function markers (ALT, AST, TP, ALB, GLB); Model 2 added renal function markers (BUN, CR, UA); Model 3 added lipid profiles (TC, TG, HDL-C, LDL-C); and Model 4 added metabolic parameters and blood pressure (FPG, SBP, DBP). Results are presented in Table 2.
When CUN-BAE was included as a continuous variable, it demonstrated significant positive associations with MASLD risk across all models (all P < 0.001). In the unadjusted model, each one-unit increase in CUN-BAE z-score was associated with a 51% increased risk of MASLD (HR = 1.51, 95% CI: 1.45–1.57, P < 0.001). In the fully adjusted Model 4, this strong association persisted, with each one-unit increase in CUN-BAE z-score associated with a 35% increased risk of MASLD (HR = 1.35, 95% CI: 1.29–1.41, P < 0.001).
Subsequently, we conducted sensitivity analysis based on CUN-BAE z-score tertiles (Q1-Q3). In the fully adjusted Model 4, using the lowest CUN-BAE level (Q1) as reference, both Q2 and Q3 groups showed significantly elevated MASLD incident risk. The highest CUN-BAE group (Q3) demonstrated a 1.9-fold increased risk compared to Q1 (HR = 1.95, 95% CI: 1.74–2.18, P < 0.001). The trend test (P for trend) yielded P < 0.001, indicating a highly significant dose-response relationship between increasing CUN-BAE levels and MASLD incident risk.
To further explore the dose-response relationship between CUN-BAE and MASLD incident risk, we employed restricted cubic spline regression analysis, which can identify potential non-linear associations and provide more precise risk assessment. Overall population analysis (Fig. 2.A): Restricted cubic spline analysis revealed a significant non-linear dose-response relationship between CUN-BAE and MASLD risk, with increasing MASLD risk as CUN-BAE increased.
Sex-stratified analysis (Fig. 2.B) revealed distinctly different association patterns between CUN-BAE and MASLD risk across sex groups (threshold effect analysis detailed in Supplementary Table 2): In the female population (red solid line), the risk curve demonstrated rapid escalation at lower CUN-BAE values (< 31.2), followed by a relatively moderate upward trend beyond the 31.2 threshold, creating a pronounced “inflection point” effect. In contrast, the male population (blue dashed line) exhibited a steeper and more consistently linear upward trend across the entire CUN-BAE range compared to their female counterparts.

Dose-response relationship between CUN-BAE and MASLD risk. (A) Non-linear association between CUN-BAE and log relative risk for MASLD in the overall population. (B) Sex-stratified analysis of the CUN-BAE-MASLD association (red line: female; cyan dashed line: male).
Cohort analysis of CUN-BAE predicting MASLD incidence risk
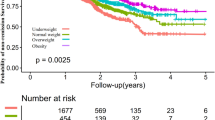
To validate the predictive value of CUN-BAE for incident MASLD cases, we conducted prospective cohort analysis among participants without MASLD at baseline. Study subjects were categorized into low, middle, and high groups based on CUN-BAE tertiles, with 5,391 participants in each group. Cumulative incidence was analyzed using the Kaplan-Meier method over 60 months of follow-up (Fig. 3).
Results demonstrated a significant dose-response relationship between CUN-BAE levels and incident MASLD risk (Log-rank test, P < 0.0001). At study completion, cumulative incidence rates for low, middle, and high CUN-BAE groups were approximately 8.4% (451 cases), 15.8% (853 cases), and 18.9% (1,018 cases), respectively.

Kaplan-Meier survival curves for MASLD incidence by CUN-BAE tertiles.
Stratified Analysis of CUN-BAE-MASLD Association
To evaluate the consistency of the CUN-BAE-MASLD association across different subgroups, we performed stratified analyses using standardized CUN-BAE z-scores (Table 3). All stratified groups showed CUN-BAE as a risk factor for MASLD (HR > 1). Age stratification revealed HRs of 1.45, 1.35, 1.29, and 1.21 for groups < 30, 30–45, 45–60, and ≥ 60 years, respectively, with no significant interaction (P interaction = 0.5852). In blood pressure stratification, diastolic blood pressure showed significant interaction (P interaction = 0.0340). Among metabolic parameters, uric acid (P interaction = 0.0007) and triglycerides (P interaction < 0.0001) demonstrated significant interactions.
Mediating Effect of TyG Index in the CUN-BAE-MASLD Association
To investigate whether the TyG index mediates the association between CUN-BAE and MASLD, we performed mediation analysis (Fig. 4). Results demonstrated that CUN-BAE had a significant positive predictive effect on the TyG index (β = 0.022, P < 0.001). The TyG index also showed significant association with MASLD (β = 0.022, P < 0.001). After controlling for the TyG index, CUN-BAE maintained a significant direct effect on MASLD (β = 0.068, P < 0.001). Mediation analysis revealed that the TyG index served as a partial mediator in the CUN-BAE-MASLD association, with a mediation proportion of 24.7%. Bootstrap testing confirmed the statistical significance of this mediation effect (P < 0.001).

Mediation analysis of the association between CUN-BAE and MASLD through TYG.
Discussion
In this prospective cohort study, higher CUN‑BAE was significantly associated with an increased risk of incident MASLD, and this association remained robust after multivariable adjustment. The results were consistent across demographic and clinical subgroups, suggesting the stability of the observed relationship. These findings indicate that CUN‑BAE, as an easily obtainable index of body fat content and distribution, may serve as a practical marker for identifying individuals at higher risk of MASLD in the general population.
These findings challenge the traditional paradigm that normal BMI equates to metabolic health, revealing the existence of subclinical metabolic dysfunction among apparently healthy individuals27,28. CUN-BAE, by integrating age, sex, and BMI information, provides a more refined assessment of body fat distribution, effectively identifying individuals who have normal BMI but relatively high fat content29. The observed dose-response relationship confirms the continuous nature of adiposity-related risk, suggesting that even modest increases in body fat within the non-obese range can trigger pathological processes leading to hepatic steatosis.
The most striking finding was the significant sex-specific patterns revealed by restricted cubic spline analysis. Women showed a distinct risk inflection point at CUN-BAE 31.2, while men exhibited a more linear dose-response relationship. This sex-specific pattern reflects complex biological mechanisms involving hormonal regulation, fat distribution patterns, and metabolic adaptation differences. These sex-specific differences may be largely attributed to hormonal and physiological variations that influence adipose tissue distribution and liver lipid metabolism. Estrogen enhances insulin sensitivity and promotes subcutaneous rather than visceral fat accumulation, reducing hepatic fat deposition and conferring protection against metabolic dysfunction–associated steatotic liver disease. In contrast, declining estrogen levels after menopause are associated with greater visceral adiposity and an increased metabolic risk, whereas low testosterone levels in men or androgen excess in women may exacerbate hepatic lipid accumulation30. Nevertheless, because hormone measurements such as estradiol or testosterone were not available in the current dataset, the proposed mechanistic explanations cannot be directly confirmed. Future studies incorporating detailed hormonal profiling are warranted to validate these pathways. The protective effects of estrogen on fat metabolism may effectively operate at lower adiposity levels by promoting subcutaneous fat distribution and improving insulin sensitivity31,32,33. However, once total adiposity reaches a critical threshold, this protective mechanism may become compromised, potentially contributing to ectopic fat deposition. The “threshold effect” observed in women may represent a critical tipping point where metabolic buffering capacity is exceeded, resulting in accelerated metabolic deterioration34,35.
Our mediation analysis revealed that TyG index mediated 24.7% of the CUN-BAE-MASLD association, indicating that insulin resistance represents an important but non-exclusive mechanistic pathway. The TyG index, as a well-validated surrogate marker of insulin resistance, provides crucial mechanistic insights into the CUN-BAE-MASLD relationship19,36. Insulin resistance represents a central pathophysiological mechanism linking excessive adiposity to hepatic steatosis through multiple pathways, including enhanced hepatic de novo lipogenesis, increased lipolysis from peripheral adipose tissue, and impaired hepatic fatty acid oxidation37. Therefore, our finding that TyG index partially mediates 24.7% of the CUN-BAE-MASLD association suggests that the increased MASLD risk observed in non-obese individuals with higher CUN-BAE values is, in part, attributable to insulin resistance-mediated metabolic dysfunction. This mechanistic understanding is particularly important in non-obese populations, where traditional obesity markers may fail to capture underlying metabolic abnormalities that predispose to hepatic steatosis.
This partial mediation suggests that while insulin resistance plays a central role in pathophysiology, other mechanisms also contribute significantly to this relationship38,39. The remaining 75.3% non-mediated effect may involve direct lipotoxic effects, gut-liver axis disruption, chronic low-grade inflammation, dysregulated adipokine secretion, and epigenetic modifications related to metabolic stress40,41. This mechanistic complexity emphasizes the multifactorial nature of MASLD pathogenesis in non-obese individuals.
Comparison with existing literature reveals both important consistencies and novel findings. The MASLD incidence rates observed in our study (8.4%−18.9%) are generally consistent with the 7–20% range reported in Western studies among lean populations8,10; however, our study demonstrated more definitive dose-response gradients and sex-specific patterns. This consistency supports the potential utility of CUN-BAE as a cross-ethnic risk assessment tool, while the refined risk stratification observed may reflect the application of more sensitive identification methods. Notably, Asian populations tend to exhibit higher body fat percentages and visceral fat proportions at equivalent BMI levels, along with relatively lower insulin secretory capacity, which may explain why significant risk differences can be identified in non-obese populations using the refined CUN-BAE indicator17,42. Our study extends previous research by specifically examining non-obese individuals using refined body composition indicators, revealing risk patterns and sex-specific characteristics that traditional anthropometric indices might overlook.
The clinical implications of these findings are substantial. Current clinical practice often underestimates MASLD risk in BMI-normal individuals, potentially leading to delayed diagnosis and missed prevention opportunities43,44. CUN-BAE, calculated simply from readily available clinical parameters, can serve as a practical screening tool for identifying high-risk non-obese individuals. The identified sex-specific risk patterns and dose-response relationships provide crucial guidance for individualized risk assessment strategies. The critical inflection point observed in women suggests that targeted screening for females approaching this threshold may be particularly beneficial. Furthermore, the partial mediating role of TyG index indicates that interventions targeting insulin resistance may effectively reduce MASLD risk, although multi-target approaches addressing non-mediated pathways may be necessary for optimal prevention45,46. From a public health perspective, the simplicity of CUN-BAE calculation makes it potentially applicable for widespread implementation in primary healthcare settings, facilitating early identification and stratified management of MASLD.
Several limitations warrant acknowledgment. First, MASLD diagnosis was based on ultrasonographic rather than histological assessment, which may result in some degree of misclassification and inability to distinguish simple steatosis from steatohepatitis. Second, our study population consisted entirely of Chinese adults from a single geographic region, which may limit generalizability to other ethnic groups and populations with different genetic backgrounds, environmental exposures, and lifestyle patterns. Third, despite comprehensive adjustment for potential confounders, residual confounding from unmeasured factors such as genetic susceptibility, gut microbiome composition, sleep quality, and psychological stress cannot be completely excluded. Moreover, because age and sex were inherently included in the estimation of CUN‑BAE, these variables were not entered as separate exposures. However, information on other lifestyle factors, such as smoking status, physical activity, and dietary habits, was unavailable due to limitations of the original dataset, which might have led to residual confounding. In addition, several relevant metabolic and anthropometric parameters, including glycated hemoglobin (HbA1c), postprandial glucose, and waist circumference, were unavailable, limiting the ability to fully characterize glucose metabolism and central adiposity among participants. Fourth, while the 5‑year follow‑up period is adequate for epidemiological research, it may not capture long‑term disease progression patterns or account for dynamic changes in lifestyle behaviors (e.g., diet, physical activity, smoking) and body composition during follow‑up. These unmeasured time‑dependent variations could have influenced the observed associations and should be addressed in future longitudinal studies with repeated measurements. Future research should prioritize several key areas. Validation studies in diverse ethnic populations are crucial for establishing the generalizability of CUN-BAE as a MASLD predictor across different demographic groups. Multi-omics integration studies combining genomics, transcriptomics, metabolomics, and microbiomics data could provide deeper insights into the biological networks underlying the CUN-BAE-MASLD association47,48. Intervention studies examining whether CUN-BAE-guided lifestyle modifications can effectively reduce MASLD risk will provide critical evidence for clinical implementation. Additionally, development of artificial intelligence-driven risk prediction models integrating multiple risk factors could enhance precision medicine approaches. Longitudinal studies with extended follow-up periods and repeated measurements will better characterize disease trajectories and identify optimal intervention windows. Of particular interest, given our findings of sex-specific differences, future intervention studies should incorporate sex-specific prevention strategies, exploring intervention effect heterogeneity at different CUN-BAE thresholds.
These findings have important implications for clinical practice and public health policy. The paradigm shift from simple BMI-based classification toward sophisticated body composition assessment represents a critical advancement in precision medicine approaches for metabolic disease prevention. The identification of sex-specific risk thresholds provides actionable guidance for clinicians to implement targeted screening strategies, particularly in populations traditionally considered low-risk. Moreover, the partial mediating role of insulin resistance suggests that interventions targeting glucose-lipid metabolism may be effective, while the substantial non-mediated component indicates that comprehensive multi-pathway approaches will likely be necessary for optimal prevention outcomes.
Conclusions
This prospective cohort study establishes CUN-BAE as a robust predictor of MASLD risk in Chinese non-obese adults, demonstrating clear dose-response relationships and distinct sex-specific patterns. With TyG index serving as a partial mediator of this association, our findings reveal that insulin resistance represents an important but non-exclusive pathological mechanism. CUN-BAE offers a practical, clinically accessible tool for identifying high-risk individuals who may be overlooked by conventional BMI screening, supporting precision-based early detection and risk stratification in non-obese populations.
Data availability
The datasets analyzed during the current study were originally obtained from the Dryad Digital Repository (previously available at doi:10.5061/dryad.1n6c4). Due to technical issues with the original repository link, the complete dataset and analysis code are available from the corresponding author upon reasonable request and with appropriate data use agreements. All data handling and analysis procedures comply with relevant ethical guidelines and institutional policies, and data access will be provided in accordance with BMC’s data sharing policies.
Abbreviations
- ALB:
-
Albumin
- ALT :
-
Alanine aminotransferase
- AST :
-
Aspartate aminotransferase
- BMI :
-
Body mass index
- BUN :
-
Blood urea nitrogen
- CI:
-
Confidence interval
- CR:
-
Creatinine
- DBP:
-
Diastolic blood pressure
- FPG:
-
Fasting plasma glucose
- GLB:
-
Globulin
- HDL-C:
-
High-density lipoprotein cholesterol
- HR:
-
Hazard ratio
- LDL-C:
-
Low-density lipoprotein cholesterol
- NAFLD:
-
Non-alcoholic fatty liver disease
- SBP:
-
Systolic blood pressure
- TC:
-
Total cholesterol
- TG:
-
Triglycerides
- TP:
-
Total protein
- TyG:
-
Triglyceride-glucose index
- UA:
-
Uric acid
- CUN-BAE :
-
Clínica Universidad de Navarra-Body Adiposity Estimator
- MASLD:
-
Metabolic dysfunction-associated steatotic liver disease
References
Riazi, K. et al. The prevalence and incidence of NAFLD worldwide: a systematic review and meta-analysis. Lancet Gastroenterol. Hepatol. 7 (9), 851–861 (2022).
Younossi, Z. M. et al. The global epidemiology of nonalcoholic fatty liver disease (NAFLD) and nonalcoholic steatohepatitis (NASH): a systematic review. Hepatology 77 (4), 1335–1347 (2023).
Powell, E. E., Wong, V. W. & Rinella, M. Non-alcoholic fatty liver disease. Lancet 397 (10290), 2212–2224 (2021).
Mantovani, A. et al. Non-alcoholic fatty liver disease and risk of fatal and non-fatal cardiovascular events: an updated systematic review and meta-analysis. Lancet Gastroenterol. Hepatol. 6 (11), 903–913 (2021).
Eslam, M. et al. A new definition for metabolic dysfunction-associated fatty liver disease: an international expert consensus statement. J. Hepatol. 73 (1), 202–209 (2020).
Rinella, M. E. et al. A multisociety Delphi consensus statement on new fatty liver disease nomenclature. Ann. Hepatol. 29 (1), 101133 (2024).
Dao, A. D., Nguyen, V. H., Ito, T., Cheung, R. & Nguyen, M. H. Prevalence, characteristics, and mortality outcomes of obese and Nonobese MAFLD in the united States. Hepatol. Int. 17 (1), 225–236 (2023).
Ye, Q. et al. Global prevalence, incidence, and outcomes of non-obese or lean non-alcoholic fatty liver disease: a systematic review and meta-analysis. Lancet Gastroenterol. Hepatol. 5 (8), 739–752 (2020).
Xu, R., Pan, J., Zhou, W., Ji, G. & Dang, Y. Recent advances in lean NAFLD. Biomed. Pharmacother. 153, 113331 (2022).
Young, S. et al. Prevalence and profile of nonalcoholic fatty liver disease in lean adults: systematic review and Meta-Analysis. Hepatol. Commun. 4 (7), 953–972 (2020).
Hagstrom, H. et al. Risk for development of severe liver disease in lean patients with nonalcoholic fatty liver disease: A long-term follow-up study. Hepatol. Commun. 2 (1), 48–57 (2018).
Sanyal, A. J., Castera, L. & Wong, V. W. Noninvasive assessment of liver fibrosis in NAFLD. Clin. Gastroenterol. Hepatol. 21 (8), 2026–2039 (2023).
Rinella, M. E. et al. AASLD practice guidance on the clinical assessment and management of nonalcoholic fatty liver disease. Hepatology 77 (5), 1797–1835 (2023).
European Association for the Study of the L. EASL clinical practice guidelines on non-invasive tests for evaluation of liver disease severity and prognosis – 2021 update. J. Hepatol. 75 (3), 659–689 (2021).
Peng, Q. et al. The relationship between the CUN-BAE body fatness index and incident diabetes: a longitudinal retrospective study. Lipids Health Dis. 22 (1), 21 (2023).
Chen, X. et al. Association of the CUN-BAE body adiposity estimator and other obesity indicators with cardiometabolic multimorbidity: a cross-sectional study. Sci. Rep. 14 (1), 10557 (2024).
Costa, A. et al. CUN-BAE index as a screening tool to identify increased metabolic risk in apparently healthy Normal-Weight adults and those with obesity. J. Nutr. 151 (8), 2215–2225 (2021).
Hong, J. et al. Comparison of triglyceride glucose index and modified triglyceride glucose indices in predicting cardiovascular diseases incidence among populations with cardiovascular-kidney-metabolic syndrome stages 0–3: a nationwide prospective cohort study. Cardiovasc. Diabetol. 24 (1), 98 (2025).
Ramdas Nayak, V. K., Satheesh, P., Shenoy, M. T. & Kalra, S. Triglyceride glucose (TyG) index: A surrogate biomarker of insulin resistance. J. Pak Med. Assoc. 72 (5), 986–988 (2022).
Zou, H., Xie, J., Ma, X. & Xie, Y. The Value of TyG-Related Indices in Evaluating MASLD and Significant Liver Fibrosis in MASLD. Can J Gastroenterol Hepatol 2025: 5871321. (2025).
Priego-Parra, B. A. et al. Diagnostic performance of sixteen biomarkers for MASLD: A study in a Mexican cohort. Clin. Res. Hepatol. Gastroenterol. 48 (7), 102400 (2024).
Wang, C. et al. The clinica Universidad de Navarra-Body adiposity estimator index is a reliable tool for screening metabolic dysfunction-associated steatotic liver disease: an analysis from a gender perspective. Lipids Health Dis. 23 (1), 311 (2024).
Dominguez, L. J. et al. Increased adiposity appraised with CUN-BAE is highly predictive of incident Hypertension. The SUN project. Nutrients 13(10),3309. (2021).
Sun, D. Q. et al. Association of low-density lipoprotein cholesterol within the normal range and NAFLD in the non-obese Chinese population: a cross-sectional and longitudinal study. BMJ Open. 6 (12), e013781 (2016).
Gomez-Ambrosi, J. et al. Clinical usefulness of a new equation for estimating body fat. Diabetes Care. 35 (2), 383–388 (2012).
Kidney Disease. Improving global outcomes CKDWG: KDIGO 2024 clinical practice guideline for the evaluation and management of chronic kidney disease. Kidney Int. 105 (4S), S117–S314 (2024).
Stefan, N. Causes, consequences, and treatment of metabolically unhealthy fat distribution. Lancet Diabetes Endocrinol. 8 (7), 616–627 (2020).
Bluher, M. Metabolically healthy obesity. Endocr Rev 41(3), bnaa004 (2020).
Gomez-Ambrosi, J. et al. Body mass index classification misses subjects with increased cardiometabolic risk factors related to elevated adiposity. Int. J. Obes. (Lond). 36 (2), 286–294 (2012).
Weiskirchen, R. & Lonardo, A. Sex hormones and metabolic Dysfunction-Associated steatotic liver disease. Int J. Mol. Sci 26(19), 9594 (2025).
Tramunt, B. et al. Sex differences in metabolic regulation and diabetes susceptibility. Diabetologia 63 (3), 453–461 (2020).
Gado, M., Tsaousidou, E., Bornstein, S. R. & Perakakis, N. Sex-based differences in insulin resistance. J Endocrinol 261(1),e230245 (2024).
Palmer, B. F. & Clegg, D. J. The sexual dimorphism of obesity. Mol. Cell. Endocrinol. 402, 113–119 (2015).
Karastergiou, K., Smith, S. R., Greenberg, A. S. & Fried, S. K. Sex differences in human adipose tissues - the biology of Pear shape. Biol. Sex. Differ. 3 (1), 13 (2012).
Meloni, A. et al. Gender differences and cardiometabolic risk: the importance of the risk factors. Int J. Mol. Sci 24(2), 1588 (2023).
Tahapary, D. L. et al. Challenges in the diagnosis of insulin resistance: focusing on the role of HOMA-IR and Tryglyceride/glucose index. Diabetes Metab. Syndr. 16 (8), 102581 (2022).
Xu, S. et al. Does diabetes status modify the association between the triglyceride-glucose index and major adverse cardiovascular events in patients with coronary heart disease? A systematic review and meta-analysis of longitudinal cohort studies. Cardiovasc. Diabetol. 24 (1), 317 (2025).
Grander, C., Grabherr, F. & Tilg, H. Non-alcoholic fatty liver disease: pathophysiological concepts and treatment options. Cardiovasc. Res. 119 (9), 1787–1798 (2023).
Muzurovic, E., Mikhailidis, D. P. & Mantzoros, C. Non-alcoholic fatty liver disease, insulin resistance, metabolic syndrome and their association with vascular risk. Metabolism 119, 154770 (2021).
Tilg, H., Adolph, T. E., Dudek, M. & Knolle, P. Non-alcoholic fatty liver disease: the interplay between metabolism, microbes and immunity. Nat. Metab. 3 (12), 1596–1607 (2021).
Samuel, V. T. & Shulman, G. I. The pathogenesis of insulin resistance: integrating signaling pathways and substrate flux. J. Clin. Invest. 126 (1), 12–22 (2016).
Fan, J. G., Kim, S. U. & Wong, V. W. New trends on obesity and NAFLD in Asia. J. Hepatol. 67 (4), 862–873 (2017).
Zhang, W. et al. Long-term outcomes following hepatectomy in patients with lean non-alcoholic fatty liver disease-associated hepatocellular carcinoma versus overweight and obese counterparts: A multicenter analysis. Asian J. Surg. 48(1), 150–158 (2025).
Wongtrakul, W., Charatcharoenwitthaya, N. & Charatcharoenwitthaya, P. Lean non-alcoholic fatty liver disease and the risk of all-cause mortality: an updated meta-analysis. Ann. Hepatol. 29 (3), 101288 (2024).
Cusi, K. et al. American association of clinical endocrinology clinical practice guideline for the diagnosis and management of nonalcoholic fatty liver disease in primary care and endocrinology clinical settings: Co-Sponsored by the American association for the study of liver diseases (AASLD). Endocr. Pract. 28 (5), 528–562 (2022).
Francque, S. M. et al. Non-alcoholic fatty liver disease: A patient guideline. JHEP Rep. 3 (5), 100322 (2021).
Hu, C. & Jia, W. Multi-omics profiling: the way towards precision medicine in metabolic diseases. J. Mol. Cell. Biol. 13 (8), 576–593 (2021).
Friedman, S. L. & Sanyal, A. J. The future of hepatology. Hepatology 78 (2), 637–648 (2023).
Acknowledgements
We acknowledge the contributions of all investigators involved in the original study.
Funding
This research was financially supported by the Science and Technology Department of Hunan Province under Grant No. 2023SK4090. The funding agency played no role in the study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Author information
Authors and Affiliations
Contributions
The study’s conceptual framework and design were developed by Jian Luo. Data analysis and result interpretation were undertaken by Xueyan Wu and Shenglian Gan. The initial manuscript draft was collaboratively prepared by Xueyan Wu, Fang Yu and Rong Zhang. Data verification procedures were conducted by Haifeng Zhou. The manuscript underwent comprehensive review and revision by all authors, who collectively approved the final submitted version. Jian Luo takes overall responsibility for the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.

Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Wu, X., Zhang, R., Gan, S. et al. CUN‑BAE predicts risk of metabolic dysfunction–associated steatotic liver disease: A prospective cohort study in non‑obese Chinese adults. Sci Rep 16, 1063 (2026). https://doi.org/10.1038/s41598-025-30646-6
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-30646-6

{kind=link}