
Abstract
Infant body size at birth has been suggested as a good marker of fetal development. However, in Vietnam, impacts of maternal TCDD exposure originating from Agent Orane on body size indices at birth have not been investigated in infants from birth cohorts around former US airbases. We investigated the effects of maternal TCDD exposure and TEQ levels of dioxin congeners other than TCDD (non-TCDD) on body size indices at birth among 504 infants from three Vietnamese birth cohorts in two contaminated areas and one unexposed area. The effects of two exposure factors, TEQ-PCDD and TEQ-PCDF in breast milk were also analyzed. Two-way analysis of covariance was used to investigate associations between body size markers and exposure factors, including interaction between exposure factors after adjusting for confounders. In girls, maternal TCDD exposure was associated with increased head circumference at birth, suggesting larger fetal brain size. TCDD exposure also showed a risk of increased abdominal fat accumulation, indicated by larger abdominal circumference in girls, whereas higher TEQ-PCDFs exposure decreased abdominal size in both sexes, suggesting potential antagonistic effects between PCDF congeners and TCDD. These findings suggest that, in Vietnam, TCDD may be a specific dioxin congener to influence fetal growth and development leading to atypical neurodevelopment and abdominal obesity in a later life.
Similar content being viewed by others

Da Nang and Bien Hoa airbases, located in central and southern Vietnam, are former United States airbases that were contaminated with dioxins from the use and disposal of so-called Rainbow herbicides from 1961 to 1972 during the Vietnam War. Agent Orange, one of the Rainbow herbicides, contains 2,4,5-trichlorophenoxy acetic acid contaminated with 2,3,7,8-tetrachlorodibenzo-p-dioxin (TCDD) at extremely high level. Since 2008, we have measured levels of dioxin congeners in the breast milk of mothers residing near Da Nang and Bien Hoa airbases and found these to be three to four times higher than levels in the breast milk of mothers living in unsprayed areas1,2,3. Owing to increased health risks among residents living in dioxin-contaminated areas, especially regarding physical growth and neurodevelopment among offspring, we conducted follow-up from age 4 or 6 months to age 9 years among infants and children living near Da Nang and Bien Hoa airbases. We found increased autistic traits in both sexes, as well as increased symptoms of attention-deficit/hyperactivity disorder (ADHD) related to dioxins among girls, which were associated with perinatal TCDD exposure in Da Nang and Bien Hoa, respectively4. We examined physical growth among infants from a Da Nang birth cohort and found that estimated marginal mean values for weight and body mass index (BMI) during the first 4 months of life, as well as neurodevelopmental scores, were significantly lower in boys with high perinatal dioxin exposure estimated according to high toxic equivalents of polychlorinated dibenzo-p-dioxins/furans (TEQ-PCDD/Fs) in the breast milk of their mothers5. However, impacts of maternal TCDD exposure, which is a specific and the most toxic dioxin congener originating from Agent Orange, on the body size at birth have not been investigated in infants from any birth cohorts in the exposed areas around former US airbases.
Infant body size at birth has been suggested as a useful marker of fetal development. Growth during the neonatal period is also affected by fetal condition. Studies in several European countries have reported lower birth weight and gestational weeks in infants exposed to dioxins and polychlorinated biphenyls (PCBs) during pregnancy6,7,8,9,10,11. Alteration of body length and head circumference at birth are also suggested to be affected by exposure to dioxins and dioxin-like compounds during the prenatal period12,13,14,15, although some reports suggest that the effects on infant body size might be directly associated with gestational age and modified according to smoking status during pregnancy.
In the present study, we included two birth cohorts in Da Nang and Bien Hoa comprising individuals who were exposed to dioxins originating from Agent Orange, and a reference birth cohort in Hanoi, an unexposed area that was not sprayed with herbicides during the Vietnam War. We aimed to investigate the impacts of dioxin exposure on body size at birth, particularly head circumference (indicating brain development during the fetal period) using a large sample size and wide range of dioxin exposure levels. We also performed data analysis using two-way analysis of covariance (ANCOVA) models with two exposure factors (TCDD levels and TEQ levels of dioxin congeners other than TCDD [non-TCDD]) as the main effects as well as their interaction; in our previous study, we analyzed the associations between infant body size and TCDD exposure without considering the interaction effects of other congeners5.
Methods
Study areas and participants
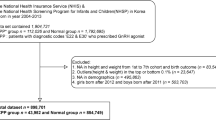
The study area comprised two areas near Da Nang and Bien Hoa airbases and a reference area in Hanoi, located in northern Vietnam. A total of 504 mother–infant pairs (87.5% of participant rate) were included in the present analysis from a Da Nang birth cohort recruited in 2008 and 2009, a Bien Hoa birth cohort recruited in 2012 and 2015, and a Hanoi birth cohort recruited in 20144. The characteristics of mother–infant pairs according to infant sex are shown in Table 1. No characteristics of mothers at birth including age and height were different between their infant sex groups. More than 97% of infants were full term at birth in both sexes. Low birth weight infants were included only in boys, although a number of infants was only 4. Characteristic differences of participants among birth cohorts in three areas were reported in our previous study16. From the factors with significant area difference, confounding factors were chosen in the present study.
Written informed consent was obtained from all participating mothers. The institutional ethics board for epidemiological studies at Kanazawa Medical University approved the study design (No. E-187). The Department of Health and Prevention of Diseases of the local government in each area reviewed and approved the informed consent process.
Exposure assessment
Dioxin measurement of maternal breast milk samples
In the present study, dioxins in breast milk at 1 month postpartum were used as indicators of prenatal dioxin exposure, because of good correlations of dioxin levels, particularly TCDD, between the paired samples of cord blood and breast milk collected from mother and infant pairs of the Bien Hoa birth cohort in Vietnam17. In each area, commune nurses visited all nursing mothers at home and collected breast milk samples from them at 4 to 5 weeks after delivery, when milk secretion was increased to be enough for donation, and frozen in the local health center or hospital. Samples were transported to Kanazawa Medical University in Japan for quantification of levels of 7 polychlorinated dibenzo-p-dioxin (PCDD) congeners and 10 polychlorinated dibenzofuran (PCDF) congeners. After extraction, purification, and fractionation using solvents, gas chromatography was performed (HP-6980; Hewlett-Packard, Palo Alto, CA, USA) with high-resolution mass spectrometry (HR-GC/MS; MSta-tion-JMS700, JEOL, Tokyo, Japan). The breast milk fat content was determined gravimetrically after extraction and purification and then used to calculate fat-based values. Levels of TEQ-PCDD/Fs were calculated by summing all values and multiplying each congener concentration by its toxicity equivalence factor, using World Health Organization 2005 toxicity equivalence factor values as reference18. Details regarding quality control of dioxin analysis such as the detection of limit and recovery rates have been reported in our previous study16.
Dioxin exposure categories
Levels of TEQ-PCDD/Fs in breast milk were stratified according to four levels (low, mild, moderate, and high), with three quantile values (8.5, 11.5, and 17.5 pg-TEQ/g lipid) as cut-off values. Their relationships with categories at two levels (≥ and < the 75th percentile value of each dioxin marker) for TCDD, TEQ-PCDD, TEQ-PCDF, and TEQ-non-TCDD are shown in Table 2, according to sex. The rate of higher TCDD levels with the cut-off of 2.5 (pg/g lipid), which is the upper range of TCDD in samples from a cohort in unsprayed Hanoi16, was increased with increased levels of TEQ-PCDD/Fs. However, rates of higher TEQ-PCDD (≥ 8.7 pg/g lipid), TEQ-PCDF (≥ 5.0 pg/g lipid), and TEQ-non-TCDD (≥ 9.2 pg/g lipid) levels were much lower with low and mild TEQ-PCDD/Fs levels (0% to 12%) than those with moderate and high levels (47% to 100%). Therefore, analysis of the associations between body size and TEQ-PCDD/Fs levels was performed for two levels, a group combining low and mild exposure and a group combining moderate and high exposure.
Data collection and body size measurement
In all birth cohorts, infant weight, body length, as well as head and abdominal circumference at birth were measured by all nurses and doctors who were trained for measurement methods of the birth cohort study before starting recruitment. Measurements were carried out using the same scales, a baby scale (Yamato Scale Co., Ltd, Akashi, Japan) to measure weight, a mobile measuring mat (SECA-nihon Co., Chiba, Japan) to measure body length, and a measuring tape for infants and toddlers (SECA-nihon Co., Chiba, Japan) to measure head and abdominal circumference. Head circumference was measured above the eyebrows and ears, and abdominal circumference was measured at the level of the navel when infants sleep deeply without abdominal movement due to respiration. BMI was obtained using the formula weight (kg)/length (m2). The height and weight of mothers were measured before delivery in the hospital. Information about infants (i.e., gestational weeks at birth and sex) and details regarding complications during pregnancy and delivery were collected from obstetricians.
Statistical analysis
IBM SPSS version 22.0 software (IBM Corp., Armonk, NY, USA) was used for the statistical analyses. To clarify the associations between body size at birth among offspring and dioxin exposure, the means of body size indices were compared between higher and lower exposure levels of TEQ-PCDD/Fs using a general linear model, after adjusting for confounding factors (one-way ANCOVA) including maternal age, parity (primipara or multipara), higher education level (12 years or more), alcohol consumption during pregnancy (yes/no), family smoking (yes/no), monthly family income (Vietnam Done), gestational weeks at birth, and maternal height. At this time, maternal smoking was not included in confounding factors, because of no smoker among participated mothers. Also, no mother had occupational history of dioxin exposure. Moreover, the effects of two exposure factors and their interaction (such as TCDD and TEQ-non-TCDD or TEQ-PCDD and TEQ-PCDF) on body size indices were analyzed, after adjusting for confounding factors using two-way ANCOVA analysis. Results were considered significant with Bonferroni-corrected p-values for multiple comparisons.
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Institutional Review Boards of the Health Department of Da Nang City and the Kanazawa Medical University (No. E-187, September 2013).
Results
Effects of TEQ-PCDD/Fs exposure on body size indices at birth
Because we found no significant difference for any body size index among TEQ-PCDD/Fs exposure groups for either sex, we compared each index among higher and lower groups of PCDD/Fs (≥ and < 11.5 pg-TEQ/g lipid, respectively), after adjusting for confounding factors. The results according to sex are shown in Table 3. In boys, the length at birth was shorter in the group with higher TEQ-PCDD/Fs exposure compared with lower exposure group; however, difference between exposure groups was not significant (p = 0.021 > 0.01 for Bonferroni-correction). No significant difference was found for BMI and head and abdominal circumference between the groups with higher and lower PCDD/Fs exposure. In addition, differences were also significant in the analysis after excluding 4 boys with low birth weight. Similarly in girls, there were no significant differences for any body size index between groups with higher and lower exposure to PCDD/Fs.
Effects of TCDD and TEQ-non-TCDDs on body size indices
We analyzed the effects of two exposure factors (i.e., TCDD exposure and TEQ-non-TCDD exposure) on body size indices as main effects of a two-way ANCOVA model. We compared the mean body size indices between higher and lower TCDD levels (≥ and < 2.5 pg/g lipid; main effect of exposure 1) and between higher and lower TEQ-non-TCDD levels (≥ and < 10.5 pg-TEQ/g lipid; main effect of exposure 2), respectively, after adjusting the effect of the other exposure factor and confounding factors. The results with test results of interaction between two main effects (2 exposure factors) are presented in Table 4 for boys and Table 5 for girls.
In boys, the adjusted head circumference was larger in the higher-TCDD exposure group compared with that in the lower-exposure group after adjusting for the effects of TEQ-non-TCDD exposure and confounding factors; however, difference was not significant (p = 0.026 > 0.01 for Bonferroni-correction). TEQ-non-TCDD exposure showed no significant effects on head circumference (Table 4). In contrast, abdominal circumference was significantly smaller in the higher-TEQ-non-TCDD exposure group compared with that in the lower-exposure group (p = 0.006 < 0.05 for Bonferroni-correction); no significant effects associated with TCDD exposure were found for abdominal circumference (Table 4). Similarly, in girls, head circumference was significantly larger in the higher-TCDD exposure group (p = 0.002 < 0.05 for Bonferroni-correction); we found no effects of TEQ-non-TCDD on head circumference (Table 5). Also, abdominal circumference was significantly larger in the higher-TCDD exposure group (p = 0.001 < 0.01 for Bonferroni-correction) but significantly smaller in the group with higher TEQ-non-TCDD exposure (p = 0.001 < 0.01 for Bonferroni-correction) among girls (Table 5). These results suggest that TCDD exposure may increase head circumference in both sexes and abdominal circumference only in girls. However, TEQ-non-TCDD exposure may decrease abdominal circumference only in boys, although BMI—correlated with abdominal circumference in general—was not associated with either TCDD or TEQ-non-TCDD exposure. Additionally, no significant effects of TCDD and TEQ-non-TCDD exposure on weight and length were observed in either sex.
Effects of TEQ-polychlorinated dibenzo-p-dioxins (PCDD) and TEQ-polychlorinated dibenzofurans (PCDF) on body size indices
We investigated the effects of TEQ-PCDD and TEQ-PCDF exposure on body size indices, after adjusting for confounding factors; the results are shown in Table 6 for boys and Table 7 for girls. In both sexes, higher TEQ-PCDD exposure levels (≥ 8.7 pg-TEQ/g lipid) showed no significant effects on any body size index. Abdominal circumference was significantly smaller (p = 0.008 < 0.05 for Bonferroni-correction) in the group with higher TEQ-PCDF exposure (≥ 5.0 pg-TEQ/g lipid) (Table 6), suggesting only PCDF congeners may contribute to decrease abdominal circumference, although significant effect of non-TCDD congeners including PCDF congeners on abdominal circumference was observed in boys (Table 4). Similarly, abdominal circumference was significantly smaller with higher TEQ-PCDF exposure in girls (p = 0.004 < 0.05 for Bonferroni-correction), although the adjusted mean head circumference was similar between the higher- and lower-TEQ-PCDF groups (Table 7). However, no significant difference for BMI was found between groups with higher and lower TEQ-PCDF exposure levels in both sexes.
At the last, to indicate clinical impacts of dioxin exposure, we analyzed absolute differences of head and abdominal circumference with effect sizes (Cohen’s d) between exposed and unexposed groups and results were shown in Table 8. In boys, higher exposure groups to TEQ-nonTCDD and TEQ-PCDFs showed 0.73 and 0.85 (cm) smaller abdominal circumference than lower exposure groups, respectively. Their Cohen’s d values were 2.3 indicating huge impact on abdominal size. Even after boys with low birth weight were excluded, differences were 0.79 and 0.89 (cm), respectively, with 2.3 of Cohen’s d, suggesting huge impacts of TEQ-nonTCDD and TEQ-PCDFs to decrease abdominal size. In girls, head circumference was 0.91 (cm) larger in higher TCDD group compared with lower group with 1.6 of Cohen’s d, suggesting very large impact of higher TCDD on head circumference. For abdominal circumference, 1 (cm) larger size for higher TCDD group, but 0.63 and 0.71 (cm) smaller size for higher TEQ-nonTCDD and TEQ-PCDFs groups with 2.1 of Cohen’s d for all exposure markers were observed in girls, indicating clinically meaningful alteration of abdominal size at birth. In addition, scatter plots were created to exhibit dose-effect relationships between TCDD exposure and head and abdominal circumferences in girls (Figs. 1 and 2), and between TEQ-PCDDFs exposure and abdominal circumferences in girls (Fig. 2) and boys (Fig. 3). In girls, head and abdominal circumferences were increased with increasing TCDD levels, whereas abdominal circumference was decreased with increasing TEQ-PCDFs levels (Figs. 1 and 2). In boys, however, dose-effect relationship between TEQ-PCDFs and abdominal circumference was not so clear, suggesting a threshold effect, because of no cases with larger abdominal circumference more than 36 (cm) whose TEQ-PCDFs levels were more than 5.0 (pg-TEQ/g lipid) (Fig. 3).

A dose-effect relationship between TCDD exposure and head circumference at birth in girls.

Dose-effect relationships between TCDD or TEQ-PCDFs exposure and abdominal circumference at birth in girls.

A dose-effect relationship between TEQ-PCDFs exposure and abdominal circumference at birth in boys.
Discussion
In the present study, increased prenatal dioxin exposure indicated by dioxins in breast milk, particularly higher TCDD exposure (≥ 2.5 pg/g lipid) originating from Agent Orange, was suggested to increase head circumference at birth indicating fetal brain size in girls. We also found that larger abdominal size was associated with higher TCDD exposure in girls, indicating a risk of central obesity later in life. In contrast, a smaller abdominal size was associated with higher TEQ-PCDF (≥ 5.0 pg-TEQ/g lipid) exposure in both sexes. Effect sizes of higher TCDD and TEQ-PCDFs exposure on head and abdominal circumferences were significant, suggesting that these alterations were clinically meaningful.
In previous studies, environmental factors during the fetal period, such as smoking19 and exposure to PCBs and heavy metals among mothers20 were reported to decrease infant head circumference at birth, leading to poor neurodevelopmental outcomes21,22 and a high prevalence of children with ADHD23. Tawara et al.13 reported inverse relationships between TCDD levels in maternal breast milk and infant head circumference at birth in a Japanese population exposed to TCDD, with a much lower mean concentration of TCDD (0.8 pg/g lipid) than that in the current study (1.5 pg/g lipid) and without samples with TCDD ≥ 5.5 pg/g lipid included in the present subjects. Long et al.15 reported that infants exposed to lipophilic persistent organic pollutants had a larger head circumference at birth, which was caused by the effect of persistent organic pollutants, which increased the gestational duration, resulting in a larger birth size. In the present study, no significant association was shown between head circumference and TEQ-nonTCDD levels, of which levels are much higher than that in general population. Taken together, these results suggest that only TCDD exposure originating from Agent Orange at high level, which significantly changed infant sex ratio at birth16, may induce enlargement effect on fetal brain.
We followed up infants from the Da Nang birth cohort, one of cohorts targeted to the current study and found mild language neurodevelopment deficits in boys and increased autistic traits in both sexes at 3 years of age exposed to high level of TCDD (≥ 3.5 pg/g lipid), as well as learning disabilities in boys and increased ADHD symptoms in girls at 8 years of age4. Also, among children from the Bien Hoa birth cohort, another cohort joined to the current study, living area around the most contaminated airbase to Agent Orange in Vietnam, we observed atypical gaze behavior (which is often found in children with autism spectrum disorder (ASD) at 2 years of age and increased autistic symptoms at 3 years of age, particularly in girls24. These results suggest that infants exposed to TCDD during pregnancy and with a larger head size at birth are at risk of neurodevelopmental disorders such as ASD in childhood, because macrocephaly has been suggested in studies of children with autism25,26. In future, we will combine data of neurodevelopmental scores examined by Bayley developmental scale, ver. 3 and autism spectrum rating scale (ASRS) scores at 3 years of age of all children enrolled to the present study and will analyze neurodevelopmental out-come of these children with TCDD > 2.5 (pg/g lipid) in their maternal breast milk and larger head size at birth.
In clinical medicine, the most important cause of macrocephaly is hydrocephalus, but infants with increased head size in the current study had no neurological symptoms during infancy, suggesting low possibility of hydrocephalus induced by TCDD exposure. In some animal studies, however, neuronal dendritic abnormalities (prolonged overgrowth) in developing brain induced by intrauterine TCDD exposure27,28, which might be the most possible mechanism for enlargement of head size observed in infants exposed to TCDD.
Abdominal circumference is an index of internal obesity in adults. Mohd Efendy Goon et al.29 reported that dioxin exposure is weakly associated with metabolic syndrome, in which a main symptom is abdominal obesity, indicated by a larger waist size. It has been reported that abdominal obesity is associated with increased cardiometabolic risk in children and adolescents, leading to metabolic syndrome in adulthood. Recently, Villar et al.30 reported that fetal abdominal growth was associated with infant growth and adiposity up to age 2 years, suggesting that larger abdominal circumference at birth may be a good indicator of abdominal obesity in childhood. In the present study, we found larger abdominal size associated with higher TCDD exposure in girls, indicating a risk of abdominal obesity later in life. Whereas, smaller abdominal size was associated with higher TEQ-PCDF exposure in both sexes. These results suggest that infants exposed to higher levels of both of TEQ-PCDFs and TCDD (around 9% of all infants) may show smaller abdominal size in boys because of significant effects of PCDF exposure, but uncertain alteration of abdominal size in girls because of increasing effect of higher TCDD and decreasing effect of PCDF exposure at the same time. Then, we tried to analyze mean abdominal circumferences of 4 groups combined with TEQ-PCDFs and TCDD categories in girls and found the mean values were 31.8 (cm) for only higher TEQ-PCDFs, 33.8 (cm) for only higher TCDD group, 32.5 (cm) for both higher TEQ-PCDFs and TCDD group, and 32.5 (cm) for both lower TEQ-PCDFs and TCDD group. These results suggest that effects of PCDF congeners and TCDD on abdominal fat metabolism may be antagonistic, resulting no alteration of abdominal size at birth in girls with high TEQ-PCDFs and TCDD. However, within our knowledge, only additive effects among dioxin congeners have been reported, suggesting that more future studies to clarify interactions among dioxin congeners.
Liver damage, as indicated by increased serum γ-glutamyl transferase, is a characteristic clinical symptom among individuals exposed to dioxins and PCBs, such as patients with Yusho or so-called rice-bran oil disease31 and industrial workers32. These findings may indicate increased abdominal circumference due to fat accumulation or liver enlargement due to dioxin exposure. However, no studies have investigated the effects of dioxins on liver growth and fat accumulation during the fetal period and childhood. These health effects of dioxin exposure during fetal period remain to be investigated.
In Vietnam, a remediation project to decrease dioxin contamination in soil and sediment in the Da Nang airbase has been completed in 2018. Another project in the largest and heaviest contaminated Bien Hoa airbase, however, has just started in 2023, suggesting that infants around Bien Hoa airbase remain at a risk to altered head size and abdominal circumferences. However, infant head and abdominal size measurements at birth are not common in Vietnam. In the areas around Bien Hoa airbase, we will recommend body size measurement at birth by standardized methods to find infants with larger head size and abdominal circumference and following-up them for early detection of neurodevelopmental deficits and obesity.
In the present study, we couldn’t measure maternal dioxin levels in blood samples collected during pregnancy. Recently, however, fat-based biological equivalency (BEQ) levels measured using the DR-EcoScreen Bioassay have been reported to be useful dioxin exposure markers for exposure assessment in epidemiological studies33, because of small sample volume required for analysis, although bioassay can show only the levels of total dioxin-like toxicity. Therefore, in future studies in dioxin contaminated areas, two measures for exposure assessment; fat-based BEQ levels in blood samples during pregnancy and dioxin congener profiles in breast milk samples are recommended to estimate prenatal exposure levels.
Conclusion
In this study including a large sample size and conducted among infants from three birth cohorts in Da Nang, Bien Hoa, and a reference area in Vietnam, we found that TCDD exposure originating from Agent Orange before birth was suggested to increase fetal brain size in girls, as indicated by head circumference at birth. In girls, TCDD exposure was also associated with a risk of increased abdominal fat accumulation indicated by larger abdominal circumference at birth, whereas higher TEQ-PCDF exposure was associated with smaller abdominal circumference, as well as in boys, suggesting potential antagonistic effects between PCDF congeners and TCDD. These findings suggest that TCDD might be a specific dioxin congener to influence fetal brain development leading to atypical neurodevelopment in a later life. However, more future studies are necessary to clarify the effects of dioxin exposure during fetal period on abdominal obesity.
Data availability
The datasets generated and/or analyzed during the current study are not publicly available due to privacy or ethical restrictions but are available from the corresponding author on reasonable request.
References
Tai, P. T. et al. Dioxin concentrations in breast milk of Vietnamese nursing mothers: a survey four decades after the herbicide spraying. Environ. Sci. Technol. 45, 6625–6632 (2011).
Nghi, T. N. et al. Dioxins and non-Ortho PCBs in breast milk of Vietnamese mothers living in the largest hot spot of Dioxin contamination. Environ. Sci. Technol. 49, 5732–5742 (2015).
Nishijo, M. et al. Dioxin congener patterns in breast milk samples from areas sprayed with herbicide during the Vietnam war 40 years after the war ended. Toxics 10, 323 (2022).
Tran, N. N. et al. Neurodevelopmental effects of perinatal TCDD exposure differ from those of other PCDD/Fs in Vietnamese children living near the former US air base in Da Nang, Vietnam. Toxics 11, 103 (2023).
Nishijo, M. et al. Impact of perinatal Dioxin exposure on infant growth: a cross-sectional and longitudinal studies in Dioxin-contaminated areas in Vietnam. PLOS One. 7, e40273 (2012).
Patandin, S. et al. Effects of environmental exposure to polychlorinated biphenyls and Dioxins on birth size and growth in Dutch children. Pediatr. Res. 44, 538–545 (1998).
Vartiainen, T. et al. Birth weight and sex of children and the correlation to the body burden of PCDDs/PCDFs and PCBs of the mother. Environ. Health Perspect. 106, 61–66 (1998).
Papadopoulou, E. et al. Maternal diet, prenatal exposure to dioxin-like compounds and birth outcomes in a European prospective mother-child study (NewGeneris). Sci. Total Environ. 484, 121–128 (2014).
Vafeiadi, M. et al. In utero exposure to compounds with dioxin-like activity and birth outcomes. Epidemiology 25, 215–224 (2014).
Govarts, E. et al. Birth weight and prenatal exposure to polychlorinated biphenyls (PCBs) and Dichlorodiphenyldichloroethylene (DDE): a meta-analysis within 12 European birth cohorts. Environ. Health Perspect. 120, 162–170 (2012).
Govarts, E. et al. Combined effects of prenatal exposures to environmental chemicals on birth weight. Int. J. Environ. Res. Public. Health. 13, 495 (2016).
Fein, G. G. et al. Prenatal exposure to polychlorinated biphenyls: effects on birth size and gestational age. J. Pediatr. 105, 315–320 (1984).
Tawara, K. et al. Effects of maternal Dioxin exposure on newborn size at birth among Japanese mother-infant pairs. Environ. Health Prev. Med. 14, 88–95 (2009).
Long, M. et al. Dioxin-like activity in pregnant women and indices of fetal growth: the ACCEPT birth cohort. Toxics 10, 26 (2022).
Long, M. et al. Maternal serum dioxin-like activity and gestational age at birth and indices of foetal growth: the Aarhus birth cohort. Sci. Total Environ. 897, 165286 (2023).
Kaneko, N. et al. Altered sex ratio at birth with maternal exposure to Dioxins in Vietnamese infants. Toxics 12, 276 (2024).
Boda, H. et al. Prenatal Dioxin exposure estimated from Dioxins in breast milk and sex hormone levels in umbilical cord blood in Vietnamese newborn infants. Sci. Total Environ. 615, 1312–1318 (2018).
Van den Berg, M. et al. The 2005 world health organization Reevaluation of human and mammalian toxic equivalency factors for Dioxins and dioxin-like compounds. Toxicol. Sci. 93, 223–241 (2006).
Shiohama, T. et al. Decreased head circumference at birth associated with maternal tobacco smoke exposure during pregnancy on the Japanese prospective birth cohort study. Sci. Rep. 11, 18949 (2021).
Dallaire, R. et al. Growth in Inuit children exposed to polychlorinated biphenyls and lead during fetal development and childhood. Environ. Res. 134, 17–23 (2014).
Aagaard, K. et al. Head circumference at birth and childhood developmental disorders in a nationwide cohort in Denmark. Paediatr. Perinat. Epidemiol. 32, 458–466 (2018).
Aagaard, K. et al. Head circumference at birth and intellectual disability: a nationwide cohort study. Pediatr. Res. 87, 595–601 (2020).
Boucher, O. et al. Prenatal methylmercury, postnatal lead exposure, and evidence of attention deficit/hyperactivity disorder among Inuit children in Arctic Québec. Environ. Health Perspect. 120, 1456–1461 (2012).
Pham, T. N. et al. Effect of perinatal Dioxin exposure originating from agent orange on gaze behavior in 3-year-old children living in the most Dioxin-contaminated areas in Vietnam. Toxics 10, 150 (2022).
Gillberg, C. et al. Head circumference in autism, asperger syndrome, and ADHD: a comparative study. Dev. Med. Child. Neurol. 44, 296–300 (2002).
Lainhart, J. E. et al. Head circumference and height in autism: a study by the collaborative program of excellence in autism. Am. J. Med. Genet. A. 140, 2257–2274 (2006).
Kimura, E. et al. Developmental origin of abnormal dendritic growth in the mouse brain induced by in utero disruption of Aryl hydrocarbon receptor signaling. Neurotoxicol Teratol. 52 (Pt A), 42–50 (2015).
Gileadi, T. E. et al. Effects of Low-Dose gestational TCDD exposure on behavior and on hippocampal neuron morphology and gene expression in mice. Environ. Health Perspect. 129, 57002 (2021).
Mohd Efendy Goon, M. D. et al. Association between polychlorinated biphenyl (PCB) and Dioxin with metabolic syndrome (METS): a systematic review and meta-analysis. Sci. Rep. 14, 17941 (2024).
Villar, J. et al. Association between fetal abdominal growth trajectories, maternal metabolite signatures early in pregnancy, and childhood growth and adiposity: prospective observational multinational INTERBIO-21st fetal study. Lancet Diabetes Endocrinol. 10, 710–719 (2022).
Kanagawa, Y. et al. Association of clinical findings in Yusho patients with serum concentrations of polychlorinated biphenyls, polychlorinated quarterphenyls and 2,3,4,7,8-pentachlorodibenzofuran more than 30 years after the poisoning event. Environ. Health. 7, 47 (2008).
Pond, S. M. Effects on the liver of chemicals encountered in the workplace. West. J. Med. 137, 506–514 (1982).
Nakamura, M. et al. Bioassay using the DR-EcoScreen system to measure Dioxin related compounds in serum samples from individuals exposed to Dioxins originating from agent orange in Vietnam. Toxics 13, 513 (2025).
Acknowledgements
We are grateful to all medical staffs in local Health Centers in Bien Hoa, Da Nang, and Hanoi in Vietnam for their collaboration.
Funding
This work was partly supported by the Ministry of Education, Science, Sports and Culture, Japan with a Grant-in-Aid for Scientific Research (17H04665). The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, or in the decision to publish the results.
Author information
Authors and Affiliations
Contributions
Conceptualization, Y.T., N.K., and M.N.; methodology, T.P.-T., T.T. and Y.N.; investigation, T.P-T., T.T-T.L., T.N.P., N.N.T. and H.T.V.; data curation, Y.T., T.T.; writing—original draft preparation, Y.T. and M.N.; writing—review and editing, M.N. and H.T.V.; funding acquisition, M.N., Y.N. All authors have reviewed the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethical approval
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Institutional Review Boards of the Health Department of Da Nang City and the Kanazawa Medical University (No. E-187, September 2013).
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Takahashi, Y., Nishijo, M., Vu, H.T. et al. Altered head size at birth is associated with maternal 2,3,7,8-tetrachlorodibenzo-p-dioxin (TCDD) exposure in Vietnamese infants. Sci Rep 16, 1256 (2026). https://doi.org/10.1038/s41598-025-30939-w
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-30939-w
