
Abstract
Stroke is a leading cause of global mortality, making accurate health information vital. While TikTok is an influential source for health content, the quality of stroke-related information on the platform is unknown. This study evaluated the quality, reliability, and user engagement of the 100 most-liked stroke-related videos on TikTok. We conducted a cross-sectional analysis of videos from January 2025, assessing quality using validated instruments (e.g., GQS, mDISCERN) and categorizing creators. Healthcare professionals (HCPs) produced 34% of videos and achieved significantly higher quality scores (p < 0.001). Misinformation was present in 31% of videos, with significantly lower rates for HCPs (8.8%) compared to content creators (42.2%) and general users (42.9%). Only 23% of videos addressed stroke prevention. Importantly, we found no significant correlation between content quality and user engagement (r = −0.08, p = 0.43), revealing a concerning “engagement paradox”. The quality of stroke information on TikTok is highly variable and disconnected from user engagement, posing a risk of misinformation spread. These findings underscore the urgent need for enhanced content moderation and greater engagement from healthcare professionals to disseminate reliable health information on social media.
Similar content being viewed by others

Introduction
Stroke remains one of the leading causes of death and long-term disability globally, affecting approximately 15 million people annually worldwide1. The burden of stroke extends beyond individual health outcomes, imposing substantial economic and social costs on healthcare systems and communities. Early recognition of stroke symptoms and prompt medical intervention are critical factors that can significantly improve patient outcomes and reduce long-term disability2. Additionally, primary prevention through lifestyle modifications and risk factor management plays a crucial role in reducing stroke incidence, with estimates suggesting up to 80% of strokes are preventable3.
In the digital age, social media has become a primary source of health information, particularly for younger demographics4. Among these platforms, TikTok has emerged as a uniquely influential channel due to its short-form video format, a predominantly young user base exceeding one billion globally, and a powerful algorithm that drives engagement and shapes health perceptions5,6,7. This landscape presents a dual reality: while it offers an unprecedented opportunity for healthcare professionals to disseminate evidence-based information, the platform’s democratized nature also allows individuals without medical training to rapidly spread potentially harmful misinformation to a massive audience6,8.
This challenge of information quality is especially critical for stroke, a time-sensitive medical emergency where delays in care can lead to severe disability. TikTok’s format is particularly suited for disseminating simple, memorable symptom recognition tools like the FAST acronym, where its rapid, widespread reach could potentially shorten treatment-seeking times. Furthermore, the platform’s predominantly younger demographic presents a significant but underexplored opportunity for primary prevention. Effectively communicating risk factor management to this audience could foster long-term health behaviors, representing a crucial, proactive public health strategy.
Despite these distinct opportunities and risks, no comprehensive evaluation of stroke-related content quality on TikTok has been conducted to date. This gap is critically important to fill, as the platform’s unique features present a high-stakes public health challenge distinct from other media. Given these features, it is essential to understand whether the platform is effectively disseminating time-sensitive symptom information for an acute emergency like stroke or acting as a significant vector for harmful misinformation. Furthermore, it is unknown if the platform’s unparalleled potential for primary prevention messaging to this younger demographic is being realized. This study, therefore, aims to address this critical gap by providing the first systematic evaluation of stroke-related content on TikTok. We systematically evaluate content quality, examine the relationship between creator characteristics and information accuracy, and assess user engagement patterns to understand the platform’s actual impact on stroke-related health communication.
Methods
Study design and data collection
We conducted a cross-sectional analysis of TikTok videos related to stroke information. Data collection was performed between January 15–20, 2025, using a standardized protocol to ensure consistency and minimize algorithmic bias. To reduce the influence of personalized recommendation algorithms, we created a new TikTok account for data collection purposes. The account was configured as a 25-year-old user located in the United States with no prior viewing history or interactions.
Video selection criteria
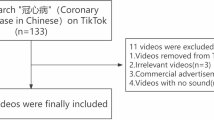
A systematic search of the TikTok platform was conducted to identify relevant videos for inclusion in the analysis. The search was performed using a comprehensive set of stroke-related hashtags, including #stroke, #strokeawareness, #strokeprevention, #strokesymptoms, and #strokerecovery. To capture content with the highest user engagement and visibility, results were filtered using the platform’s "most-liked" function. The video selection process is detailed in Fig. 1. Initially, 160 videos were identified through hashtag searches. After removing 20 duplicates, 140 unique videos underwent eligibility assessment. Forty videos were excluded: 15 (37.5%) were irrelevant to stroke medical information, 12 (30.0%) were personal narratives lacking educational content, 8 (20.0%) had durations outside the specified range, and 5 (12.5%) were in non-English languages. The final sample comprised 100 videos meeting all inclusion criteria. Inclusion criteria required that videos have a primary focus on stroke-related health information and a duration between 15 s and 10 min. Videos were excluded if they were duplicates, not in English, irrelevant to the medical context of stroke, or consisted of personal narratives lacking substantive educational value.The selection of the top 100 videos is consistent with the methodology of previous cross-sectional studies that have evaluated health information quality on social media platforms9. For each video in the final sample, a standardized data extraction form was used to collect quantitative video characteristics, including duration, upload date, and engagement metrics (likes, shares, comments). Creator-specific data were also recorded, including username, follower count, verification status, and any self-disclosed professional credentials. Finally, the thematic content was coded for the presence of key educational topics (stroke prevention, symptoms, treatment, and rehabilitation), and the use of visual elements such as graphics, medical imagery, or physical demonstrations was documented.

Flowchart of the video selection process.
User engagement
The primary dependent variable for this study was user engagement. This construct was operationally defined and measured using three publicly available metrics for each video: the total number of 'likes,' the total number of 'comments,' and the total number of 'shares.' These metrics were collected directly from the TikTok platform for each included video and were chosen as they are standard indicators of content reach and audience interaction.
Video analysis and coding
Two authors independently assessed the quality of the remaining stroke-related videos from January 8 to 18, 2025. A third arbitrator assigned the final score if the two raters’ scores were inconsistent. The inter-rater reliability for the video quality assessments was calculated using Cohen’s kappa (κ). The agreement was found to be substantial (κ = 0.78). The Patient Education Materials Assessment Tool (PEMAT), Video Information and Quality Index (VIQI), Global Quality Score (GQS), The Journal of the American Medical Association (JAMA) benchmark criteria and modified DISCERN (mDISCERN) were utilized to evaluate the video quality.
The PEMAT10 consists of 25 questions, with 21 representing the understandability of stroke-related health information and 4 evaluating the actionability of recommendations by videos. Each item is scored as "agree = 1, disagree = 0, N/A". The total score (PEMAT-T) and the score of understandability (PEMAT-U) and actionability section (PEMAT-A) are calculated as "Total Points/Total Possible Points × 100". Higher scores indicate better performance in delivering comprehensible and actionable stroke education.
The VIQI tool11 encompasses four dimensions: information flow (VIQI 1), information accuracy (VIQI 2), quality (videos including one point for each image, animation, interview, video captions, and summary) (VIQI 3), and precision (level of coherence between video title and stroke-related content) (VIQI 4). Each criterion is rated on a scale of 1–5, with higher scores indicating better quality of stroke educational content.
The JAMA benchmark criteria, a 4-point scale, were used to assess the credibility of the health information12.This tool evaluates four key components: authorship, attribution, currency, and disclosure, with higher scores indicating greater credibility.
The GQS13, a 5-point scale, assessed overall video quality of stroke-related content, ranging from poor (1) to excellent (5).
The mDISCERN was adapted from the DISCERN tool and is more suitable for assessing video material14. It consists of five questions related to the reliability of the stroke-related video content. Each question is scored 1 for “yes” and 0 for “no”. Higher scores correspond to more excellent reliability in stroke education materials.
Previous studies have validated the above tools, particularly in the context of social media platforms and neurological health content.
These five instruments were strategically selected to provide a comprehensive, multi-dimensional assessment of content quality. Collectively, they evaluate key aspects including overall quality and information flow (GQS, VIQI), reliability and credibility (mDISCERN, JAMA), and the practical utility for patients, such as understandability and actionability (PEMAT). The widespread use of these validated tools in prior social media health information research also allows for comparability with the existing literature.
Statistical analysis
Descriptive statistics were calculated for all variables. Due to non-normal distribution of engagement data, we used non-parametric tests (Mann–Whitney U test, Kruskal–Wallis test) for group comparisons. Spearman’s rank correlation coefficient assessed relationships between quality scores and engagement metrics. Statistical significance was set at p < 0.05. All analyses were performed using SPSS version 29.0.
Results
Overview of key findings
Analysis of 100 TikTok stroke-related videos revealed three critical findings: only 23% addressed stroke prevention, 31% contained misinformation, and healthcare professionals (34% of creators) produced significantly higher quality content (GQS: 3.12 ± 0.68) compared to content creators (2.31 ± 0.84) and general users (1.95 ± 0.72, p < 0.001).
Video and creator characteristics
A total of 100 TikTok videos met inclusion criteria after systematic screening.The detailed video selection process is illustrated in Fig. 1. Table 1 presents comprehensive characteristics of analyzed videos, including creator demographics, video features, and engagement patterns. Healthcare professionals constituted 34% of video creators, content creators represented 45%, and general users comprised 21%. Despite having fewer followers (median: 23,400), healthcare professionals achieved higher profile verification rates (67.6%) compared to content creators (31.1%) and general users (19.0%, p < 0.001). Content creators demonstrated the highest engagement metrics with a median follower count of 185,600, receiving significantly more likes (median: 28,450 vs. 12,340 vs. 4230), comments, and shares compared to other creator categories (all p < 0.01).
Quality assessment scores
Quality scores varied significantly by creator type across all validated measures (Table 2). Healthcare professionals achieved the highest Global Quality Scores (3.12 ± 0.68), with 73.5% exceeding the quality threshold. Content creators scored lower (2.31 ± 0.84), while general users showed the poorest performance (1.95 ± 0.72).
The modified DISCERN scores showed similar patterns. Healthcare professionals demonstrated superior reliability (3.28 ± 0.71) compared to content creators (2.14 ± 0.93) and general users (1.81 ± 0.88). Video Information and Quality Index (VIQI) assessment reinforced these disparities. Healthcare professionals achieved the highest total scores (15.1 ± 2.8), significantly outperforming content creators (11.3 ± 2.9) and general users (9.2 ± 2.4). Healthcare professionals excelled particularly in information accuracy (3.9 ± 0.6 vs. 3.0 ± 0.7 vs. 2.4 ± 0.8) and information flow dimensions (3.8 ± 0.7 vs. 2.9 ± 0.8 vs. 2.3 ± 0.9).
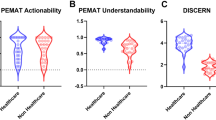
PEMAT understandability scores were relatively high across all groups (healthcare professionals: 82.4 ± 12.6%, content creators: 74.8 ± 15.3%, general users: 68.9 ± 18.2%, p = 0.006). However, actionability scores revealed greater disparities (76.3 ± 19.4% vs. 63.2 ± 23.1% vs. 54.7 ± 25.8%, p = 0.002), indicating non-professional creators struggled to provide practical guidance.
The JAMA benchmark criteria demonstrated the most striking differences. Healthcare professionals showed universal authorship identification (100.0%) compared to content creators (24.4%) and general users (9.5%, p < 0.001). Attribution of sources was similarly higher among healthcare professionals (58.8% vs. 13.3% vs. 4.8%, p < 0.001).
Content analysis
Content gaps were substantial (Table 3). Only 23% of videos addressed stroke prevention, with marked creator differences: healthcare professionals included prevention content in 44.1% of videos, compared to content creators (15.6%) and general users (9.5%, p = 0.002). Prevention strategies, when present, focused primarily on hypertension management (35.3% for healthcare professionals), exercise recommendations (23.5% for healthcare professionals), and dietary modifications (20.6% for healthcare professionals). Symptom recognition appeared in 67% of videos, with 82.4% of healthcare professional videos including symptom content compared to 64.4% of content creator videos and 47.6% of general user videos (p = 0.014). Healthcare professionals were significantly more likely to mention FAST criteria (61.8% vs. 26.7% vs. 14.3%, p < 0.001) and BE-FAST criteria (20.6% vs. 2.2% vs. 0%, p = 0.003). Treatment information appeared in 31% of videos, with healthcare professionals providing such content in 52.9% of their videos compared to 22.2% for content creators and 14.3% for general users (p = 0.002).
Misinformation analysis
Misinformation appeared in 31% of videos, with significant variation by creator type (Table 4). Healthcare professionals had the lowest rate (8.8%), while content creators (42.2%) and general users (42.9%) showed concerning levels (p < 0.001). The most problematic categories included: unproven treatments (12% of all videos, exclusively from non-professionals), incorrect symptom information (8%), and misleading prevention advice (7%). Healthcare professionals’ misinformation, when present, consisted primarily of oversimplified explanations rather than factually incorrect statements.
Engagement-quality relationship
Correlation analysis revealed no significant associations between quality scores and engagement metrics: GQS vs. likes (r = −0.08, p = 0.43), mDISCERN vs. comments (r = 0.12, p = 0.23), PEMAT understandability vs. shares (r = 0.06, p = 0.57). This “engagement paradox” was consistent across all quality measures. Videos containing personal testimony were most common among general users (71.4% vs. 40.0% vs. 23.5%, p = 0.001), while achieving higher engagement than educational content. Videos with misinformation showed comparable engagement to accurate content (median engagement score: 2.3 vs. 2.1, p = 0.67), indicating that TikTok’s algorithm does not differentiate between evidence-based and misleading health information.
Visual presentation analysis revealed that healthcare professionals more frequently used medical imagery (52.9% vs. 26.7% vs. 19.0%, p = 0.010) and infographics/charts (38.2% vs. 15.6% vs. 9.5%, p = 0.015), while general users relied heavily on personal testimony and emotional appeal (47.6% vs. 42.2% vs. 20.6%, p = 0.027).
Discussion
Our analysis of stroke-related information on TikTok revealed three core findings: (1) a significant quality disparity exists, with healthcare professionals producing demonstrably more reliable content than other creators; (2) a concerning “engagement paradox” is present, where content quality does not correlate with user engagement metrics, meaning inaccurate content can achieve similar visibility to evidence-based videos; and (3) a critical content gap exists, with an overwhelming focus on symptom recognition over primary prevention. These findings have significant implications for public health communication in the digital age.
This study makes several novel contributions to the existing literature on health information quality in social media. First, to our knowledge, this is the first systematic evaluation specifically examining stroke-related content quality on TikTok, addressing a critical knowledge gap given the platform’s unique algorithmic structure and predominantly young user demographic. While previous studies have evaluated health information on YouTube and Instagram, TikTok’s short-form video format and powerful recommendation algorithm create a distinct information ecosystem that warrants separate investigation. Second, our identification and quantification of the “engagement paradox”—where content quality shows no correlation with user engagement (r = −0.08, p = 0.43)—represents a previously undocumented phenomenon in stroke health communication on social media. This finding challenges the assumption that accurate health information naturally achieves wider reach and has important implications for platform design and content moderation strategies. Third, we provide the first quantitative evidence of the severe underrepresentation of stroke prevention content (23%) on a platform whose user base is primarily under 40 years old, revealing a major missed opportunity for primary prevention messaging. Finally, our creator-stratified analysis offers new insights into the relationship between source credibility and misinformation rates, demonstrating that while healthcare professionals constitute only 34% of creators, their content is significantly more accurate (8.8% vs. 42.2–42.9% misinformation rate) yet does not achieve proportionally higher engagement. These findings extend beyond descriptive analysis to reveal fundamental challenges in the dissemination of evidence-based stroke information in algorithm-driven social media environments.
The superior performance of healthcare professionals across all quality metrics (GQS, mDISCERN, PEMAT A/V, and JAMA criteria) aligns with previous research examining health information quality on social media platforms15. Healthcare professionals demonstrated significantly better source attribution, balanced presentation of information, and adherence to evidence-based guidelines. These findings are consistent with studies evaluating health content on YouTube and Instagram, which similarly found that medical professionals produce more accurate and reliable health information16. The quality deficits observed among non-professional creators primarily stemmed from inadequate source citation, oversimplified medical explanations, and inclusion of unverified treatment recommendations. These patterns mirror findings from systematic reviews of health misinformation on social media, which consistently identify lack of medical expertise as a primary driver of inaccurate health content.
A particularly concerning finding is the absence of correlation between content quality and user engagement metrics. This “engagement paradox” suggests that TikTok’s algorithm may prioritize emotionally compelling content over medical accuracy, potentially amplifying misinformation while reducing the visibility of evidence-based health information17,18. This paradox likely reflects TikTok’s algorithm, which prioritizes emotionally resonant and narratively compelling content over factual accuracy. Personal anecdotes and dramatic storytelling, regardless of their medical validity, are often rewarded with higher engagement, posing a fundamental challenge to traditional, evidence-based health communication. Similar patterns have been documented across multiple social media platforms, indicating that this phenomenon extends beyond TikTok to represent a broader challenge in digital health communication19. The higher engagement rates observed for personal recovery narratives compared to educational content reflect the platform’s emphasis on storytelling and emotional connection. While personal experiences can be valuable for patient support and motivation, they may inadvertently overshadow critical educational content about stroke prevention and early recognition20.
The underrepresentation of stroke prevention content in only 23% of analyzed videos represents a significant missed opportunity for population-level health improvement. Primary prevention through lifestyle modification and risk factor management can reduce stroke incidence by up to 80%. Given TikTok’s predominantly younger user base, the platform represents an ideal venue for promoting stroke prevention strategies that could have decades-long health benefits. The predominant focus on symptom recognition, while important, reflects a reactive rather than proactive approach to stroke education. This pattern aligns with broader trends in health communication, where acute care messaging often overshadows prevention-focused content despite the greater population-level impact of preventive interventions21. This heavy focus on reactive symptom recognition over proactive prevention represents a major missed public health opportunity, especially on a platform dominated by younger users for whom primary prevention can yield decades of health benefits and significantly reduce the future societal burden of stroke. This heavy focus on reactive symptom recognition over proactive prevention represents a major missed public health opportunity, especially on a platform dominated by younger users for whom primary prevention can yield decades of health benefits and significantly reduce the future societal burden of stroke.
The presence of misinformation in 31% of analyzed videos raises serious public health concerns, particularly given the time-sensitive nature of stroke care. Misinformation about stroke symptoms could delay critical treatment, while inaccurate prevention advice might provide false reassurance or promote ineffective interventions22,23. The promotion of unproven treatments, observed exclusively among non-professional creators, poses particular risks by potentially deterring individuals from seeking appropriate medical care. The comparable engagement rates between accurate and inaccurate content suggest that users may not possess the health literacy skills necessary to differentiate between evidence-based and misleading information. This finding underscores the importance of digital health literacy initiatives and platform-level interventions to promote accurate health information24.
From the perspective of the Extended Parallel Process Model (EPPM), many analyzed videos effectively conveyed threat information about stroke severity but failed to provide adequate efficacy information, including clear prevention strategies and actionable response protocols. This imbalance can lead to fear-control responses rather than protective health behaviors, potentially reducing the effectiveness of stroke education efforts. Effective health communication requires balancing threat perception with self-efficacy and response efficacy to promote adaptive behavioral responses. The predominance of symptom-focused content without corresponding prevention information may inadvertently promote maladaptive coping strategies or health anxiety rather than constructive health behaviors.
Implications and actionable recommendations
Based on our findings, a multi-pronged approach is necessary, involving collaboration between platform developers, healthcare professionals, and public health organizations. For platform developers, the primary responsibility is to foster a safer information environment. This includes implementing a health information verification system that provides a visible badge or label for content from certified healthcare professionals and reputable health organizations. Furthermore, their content recommendation algorithms should be adjusted to incorporate quality indicators like source citation and factual accuracy, thereby preventing the amplification of low-quality or misleading health information. Platforms should also actively collaborate with public health bodies, such as the World Health Organization or the American Stroke Association, to promote and feature their evidence-based content, especially during awareness campaigns.
Concurrently, healthcare professionals and institutions must adapt their communication strategies for these new digital spaces. Medical schools and professional organizations should offer training on creating engaging, evidence-based short-form video content, emphasizing skills like effective storytelling and the use of visual aids without sacrificing accuracy. Professionals should adopt an engagement-oriented strategy rather than simply presenting facts, creating content that leverages platform trends like "myth-busting" videos to debunk misinformation or “duetting” inaccurate content to provide corrections. Given the platform’s young audience, there should also be a strong focus on prevention messaging, with creators prioritizing accessible and engaging content about primary stroke prevention framed around long-term wellness and healthy lifestyle choices.
Focus on Prevention Messaging: Given the platform’s young audience, healthcare creators should prioritize creating accessible and engaging content about primary stroke prevention, framing it around long-term wellness and healthy lifestyle choices.
Future research should examine the longitudinal effects of social media health information exposure on stroke knowledge, attitudes, and health behaviors. Intervention studies evaluating the effectiveness of evidence-based stroke education content on social media platforms could inform best practices for health communication in digital environments. Additional research is needed to understand user motivations for seeking health information on social media platforms and to identify effective strategies for promoting critical evaluation of health content 21. Cross-platform comparative studies could illuminate platform-specific factors that influence health information quality and user engagement patterns. Furthermore, future research should employ more advanced statistical methods to control for creator-level variables, such as follower count and average view rates, to better isolate the impact of content quality on user engagement patterns.
This study reveals significant quality disparities in stroke-related information on TikTok, with healthcare professionals producing more reliable content that nonetheless fails to achieve higher user engagement. The prevalence of misinformation and underrepresentation of prevention-focused content highlight urgent needs for enhanced content moderation, increased healthcare professional engagement, and improved digital health literacy initiatives. Addressing these challenges requires coordinated efforts from healthcare professionals, platform developers, public health organizations, and educational institutions to harness social media’s potential for improving stroke prevention and outcomes while minimizing associated risks.
Limitations
The findings of this study should be interpreted in the context of several limitations.
First, the study’s scope was constrained. Our cross-sectional design captures a single point in time, the analysis was confined to English-language videos, and the findings are specific to TikTok. These factors may limit the generalizability of our results to other platforms, languages, or evolving content trends. Second, our focus on the 100 "most-liked" videos introduces a selection bias. While this method allowed us to analyze the most visible content, the findings may not be representative of all stroke-related videos on the platform, particularly those with lower engagement. Third, creator categorization relied on self-disclosed credentials, leading to a potential for misclassification. Healthcare professionals who did not list their qualifications in their profiles may have been incorrectly categorized as general users, potentially underestimating the prevalence of expert-created content. Finally, the use of platform engagement metrics as a proxy for content impact has several key limitations. These metrics can be heavily influenced by a creator’s existing follower count, independent of an individual video’s quality. Our cross-sectional analysis could not fully disentangle the effect of content quality from the creator’s pre-existing popularity, a factor known to significantly impact content visibility. Second, while these metrics indicate visibility and interaction, they do not necessarily correlate with actual behavior change.They are not a direct measure of the content’s influence on user knowledge, attitudes, or offline health behaviors.
Conclusions
Stroke-related information on TikTok varies significantly in quality, with healthcare professionals producing more reliable and evidence-based content compared to content creators and general users. The lack of correlation between content quality and user engagement suggests that inaccurate information may receive similar visibility to evidence-based content, posing potential risks to public health.
The predominance of symptom-focused over prevention-focused content represents a missed opportunity for population-level stroke risk reduction. The presence of misinformation in nearly one-third of videos highlights the need for enhanced content moderation and healthcare professional engagement on social media platforms. Healthcare institutions and professionals should consider strategic engagement with platforms like TikTok to improve the quality and reach of evidence-based stroke information. Platform developers should implement enhanced mechanisms for identifying and promoting high-quality health content while limiting the spread of misinformation. Ultimately, improving the quality of stroke-related health information on social media requires coordinated efforts from healthcare professionals, platform developers, public health organizations, and users themselves. Only through such collaborative approaches can we harness the potential of social media to improve stroke prevention, recognition, and outcomes while minimizing the risks associated with health misinformation.
Data availability
The original data used in this study were obtained from TikTok(https://www.douyin.com/) and are publicly available on the platform.
References
Li, X. et al. Global, regional, and national burden of ischemic stroke, 1990–2021: An analysis of data from the global burden of disease study 2021. Eclinicalmedicine. 75, 102758 (2024).
Powers, W. J. et al. Guidelines for the early management of patients with acute ischemic stroke: 2019 Update to the 2018 guidelines for the early management of acute ischemic stroke: A guideline for healthcare professionals from the American heart association/American stroke association. Stroke 50, e344–e418 (2019).
O’Donnell, M. J. et al. Global and regional effects of potentially modifiable risk factors associated with acute stroke in 32 countries (interstroke): A case-control study. Lancet 388, 761–775 (2016).
Colder Carras, M. et al. Prevention and health promotion interventions for young people in the context of digital well-being: Rapid systematic review. J. Med. Internet Res. 26, e59968 (2024).
Nickel, B. et al. Social media posts about medical tests with potential for overdiagnosis. Jama Netw. Open. 8, e2461940 (2025).
Basch, C. H. et al. Community mitigation of covid-19 and portrayal of testing on Tiktok: Descriptive study. Jmir Public Health Surveill. 7, e29528 (2021).
Rowdhwal, S. S. S. & El Boghdady, M. Exploring Tiktok’s influence on surgical patient education. Surg: J R Coll Surg Edinb Irel. 23, 265–276 (2025).
Hu, Z., Yang, Z., Li, Q. & Zhang, A. The covid-19 infodemic: Infodemiology study analyzing stigmatizing search terms. J. Med. Internet Res. 22, e22639 (2020).
Xia, L., Bao, J., Yao, K., Zhang, J. & Yu, W. Evaluation of the quality and reliability of Chinese content about orthognathic surgery on Bilibili and Tiktok: A cross-sectional study. Sci. Rep. 15, 28967 (2025).
Shoemaker, S. J., Wolf, M. S. & Brach, C. Development of the patient education materials assessment tool (Pemat): A new measure of understandability and actionability for print and audiovisual patient information. Patient Educ. Couns. 96, 395–403 (2014).
Nagpal, S. J. S., Karimianpour, A., Mukhija, D., Mohan, D. & Brateanu, A. Youtube videos as a source of medical information during the ebola hemorrhagic fever epidemic. Springerplus 4, 457 (2015).
Silberg, W. M., Lundberg, G. D. & Musacchio, R. A. Assessing, controlling, and assuring the quality of medical information on the internet: Caveant lector Et viewor-let the reader and viewer beware. JAMA 277, 1244–1245 (1997).
Bernard, A. et al. A systematic review of patient inflammatory bowel disease information resources on the World Wide Web. Am. J. Gastroenterol. 102, 2070–2077 (2007).
Singh, A. G., Singh, S. & Singh, P. P. Youtube for information on rheumatoid arthritis: A wakeup call?. J. Rheumatol. 39, 899–903 (2012).
Gabarron, E., Oyeyemi, S. O. & Wynn, R. Covid-19-related misinformation on social media: A systematic review. Bull. World. Health. Organ. 99, 455–463 (2021).
Madathil, K. C., Rivera-Rodriguez, A. J., Greenstein, J. S. & Gramopadhye, A. K. Healthcare information on Youtube: A systematic review. Health Inform. J. 21, 173–194 (2015).
Rathore, F. A. & Farooq, F. Information overload and infodemic in the covid-19 pandemic. Jpma. J Pak Med Assoc. 70(3), 62–65 (2020).
Ahmed, W., Vidal-Alaball, J., Downing, J. & López Seguí, F. Covid-19 and the 5G conspiracy theory: Social network analysis of twitter data. J. Med. Internet Res. 22, e19458 (2020).
Schmidt, A. L., Zollo, F., Scala, A., Betsch, C. & Quattrociocchi, W. Polarization of the vaccination debate on facebook. Vaccine. 36, 3606–3612 (2018).
Moorhead, S. A. et al. A new dimension of health care: Systematic review of the uses, benefits, and limitations of social media for health communication. J. Med. Internet Res. 15, e85 (2013).
Glasgow, R. E., Phillips, S. M. & Sanchez, M. A. Implementation science approaches for integrating Ehealth research into practice and policy. Int. J. Med. Inform. 83, e1–e11 (2014).
Hou, S., Charlery, S. R. & Roberson, K. Systematic literature review of internet interventions across health behaviors. Health Psychol. Behav. Med. 2, 455–481 (2014).
Diviani, N., van den Putte, B., Meppelink, C. S. & van Weert, J. C. M. Exploring the role of health literacy in the evaluation of online health information: Insights from a mixed-methods study. Patient Educ. Couns. 99, 1017–1025 (2016).
Norman, C. D. & Skinner, H. A. Ehealth literacy: Essential skills for consumer health in a networked world. J. Med. Internet Res. 8, e9 (2006).
Funding
The authors did not receive support from any organization for the submitted work.
Author information
Authors and Affiliations
Contributions
Zhaowei Wang and Chengwu Hu are co-first authors. Zhaowei Wang and Chengwu Hu were responsible for the study design, data collection, analysis, and the drafting of the manuscript. Bo Zhou contributed to the interpretation of data and critical revision of the manuscript for important intellectual content. Meiping Wan was responsible for the conception of the study, supervision, and critical revision of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethical approval
This study was based on the analysis of publicly available data from the social media platform TikTok. As the research did not involve human participants, clinical data, or personal privacy information, ethical review and approval were not required for this study.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Wang, Z., Hu, C., Zhou, B. et al. Quality evaluation of stroke-related information on TikTok: a cross-sectional study. Sci Rep 16, 1843 (2026). https://doi.org/10.1038/s41598-025-31464-6
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-31464-6
