
Abstract
Medical tattoos after breast cancer surgery are a therapeutic approach to regain psychophysical integrity. The tattooing of the Nipple-Areola Complex (NAC) in the ARCADE clinic involves three sessions, 30–40 days apart, and specialized nurses perform it upon medical indication. This study aims to assess the feasibility of a NAC tattooing clinic for women who have undergone surgical treatment for breast cancer in the Comprehensive Cancer Center of Azienda USL–IRCCS di Reggio Emilia, in Italy. This project is guided by the Medical Research Council framework for the development and evaluation of complex interventions, focusing specifically on the feasibility phase. The objectives of this phase include assessing organisational sustainability through retrospective analysis of activity data (Endpoint 1); evaluating the NAC tattoos’ quality, by selecting a panel of experts that scored photographs’set, in a 1–5 Likert scale (Endpoint 2); exploring the professionals’ perceptions on their involvement in the clinic, through a qualitative study with semi-structured interviews (Endpoint 3). Endpoint 1: The activity had a standard character in timing and materials. 100% of the sample (N = 33) gained a satisfactory cosmetic result, without adverse events, or other complications like excessive color fading or pain (none or mild for 79%). Endpoint 2: 22 sets were retrospectively retrieved and included in the analysis. The tattooed NACs demonstrated excellent quality, achieving a medium score of 4.7 for color similarity and symmetry, and 4.8 for 3D effect. Endpoint 3: Five professionals (two nurses, one surgeon, two managers) were interviewed. The main macro-themes acknowledged considerations about the value of the clinic, the barriers and the facilitators encountered, and the related future needs. A nurse-led NAC tattooing clinic is a feasible, complex intervention for breast cancer care. The combination of the retrieved data analysis and those generated by the qualitative approach underlines how resource availability and personnel motivation are influential in determining goal achievement, as well as accountability promotion and competence development. The implementation of this service empowered a support network by engaging the community and professionals in collaborative efforts to provide this final step of care, which can be determinant for psychophysical recovery.
Similar content being viewed by others


Introduction
Breast cancer is the most frequently diagnosed tumor in women. The estimated net survival rate 5 years after diagnosis is 88%1. From initial diagnosis to subsequent follow-up, patients are guided through a structured clinical pathway involving multiple stages and healthcare professionals to ensure the delivery of comprehensive and coordinated care. The implementation of multidisciplinary approaches enhances the quality and consistency of treatment, which is often characterized by its extensive duration and complexity1. When surgical treatment is indicated, it may have long-term implications for quality of life. Women undergoing mastectomy often experience anxiety, stress, trauma, and depression2, which is associated with increased use of healthcare resources. Although rare, breast cancer occurs also in men and is frequently managed according to evidence generated in women. Nonetheless, male patients may experience considerable long-term physical and psychological sequelae3. Appropriate treatments may help reduce individual burden and strain on the healthcare system4. Reconstructive surgery often provides excellent results in terms of breast shape. However, Nipple-Areola Complex (NAC) tattooing is usually a neglected part of the breast reconstruction process5. Interest in NAC tattooing has grown extensively worldwide6. A growing body of empirical evidence indicates that the use of medical tattoos among women who have undergone mastectomy serves as a therapeutic intervention. This approach may facilitate the restoration of femininity, sexuality, and personal identity following disease and aggressive treatments7. It is regarded as the conclusion of a challenging process and signifies the completion of a treatment course by restoring both physical and psychological well-being8. The tattooing technique used for NAC reconstruction is medical dermopigmentation9: pigments are introduced into the superficial layer of the papillary dermis using an electric device and disposable needles to color the skin. A recent review concluded that NAC tattooing is a safe and well-tolerated technique that produces satisfactory aesthetic results10. However, further studies are needed to fill gaps about how this service can be provided. Although reducing health disparities is a priority, addressing their complexities remains challenging, particularly in breast cancer survivorship care11,12. Involving patients, their families, and communities in addressing this challenge is crucial13. Mahony et al. demonstrated that early contact with a specialist breast cancer nurse positively impacts patients, health services, and the healthcare system, leading to substantial net savings14. The organization of care services can influence the magnitude of these effects and should be optimized according to patients’ needs and the local healthcare context. This study seeks to evaluate the feasibility of establishing a NAC tattooing clinic for women who have previously undergone surgical treatment for breast cancer at the Comprehensive Cancer Center of Azienda USL–IRCCS in Reggio Emilia, Italy.
Methods
Study design
To accomplish the overarching objective outlined above, the Medical Research Council (MRC) framework for the development and implementation of complex healthcare interventions was selected15. The four phases of the methodology are as follows: (1) development or identification of the intervention, (2) feasibility assessment, (3) evaluation, and (4) implementation. Further details regarding the initial phase are available in a prior publication16. This section delineates the second and third phases of the framework as applied to this project. Complex interventions comprise multiple interacting components and are commonly implemented within service delivery contexts across diverse fields, such as palliative care17, rehabilitation, and mental health18. The complexity of the intervention is determined by various factors, including the number of interactions and behaviors involved, the diversity and competencies of the professionals engaged, the types of instruments employed, the outcomes to be measured, organizational characteristics, logistical considerations, and the degree of flexibility inherent in the intervention15. It is crucial to understand the barriers and facilitators related not only to the characteristics of the intervention, but also to the individuals involved, in order to ensure successful implementation19.
The application of NAC tattooing within an oncological context exemplifies a complex intervention in healthcare, with its impacts evaluated across patient, professional, and organizational levels. To assess the feasibility of a nurse-led NAC tattooing clinic, we implemented the ARCADE_M study, an observational, single-centre, mixed-methods study. Its protocol was approved by the Area Vasta Emilia Nord ethic committee N° 2024/0133222, on 09/10/2024, and it is registered in Open Science Framework: https://osf.io/evrhc/?view_only=fe0aa5e7a9424def9177aa7376d8938c.
Specific outcomes
The feasibility of an intervention is determined by several elements, such as optimal delivery, adherence, costs, and the ability of professionals to provide it15. The ARCADE_M’s goals were: to assess the organisational sustainability of the nurse-led NAC tattooing clinic (Endpoint 1); to evaluate the cosmetic outcome of the NAC tattoo (Endpoint 2); to explore the professionals’ perceptions on their involvement in the NAC tattooing clinic (Endpoint 3); to explore the lived experiences of the tattooed women (Endpoint 4). The activities related to all the endpoints were conducted in parallel. This paper presents the results related to endpoints 1 to 3. Endpoint 4 will be discussed exhaustively in a separate report.
-
Endpoint 1: activity and process data of the ARCADE clinic were analysed retrospectively.
-
Endpoint 2: a panel of experts analysed the photographs of the tattooed NAC according to objective criteria (symmetry, colouring, 3D effect).
-
Endpoint 3: a qualitative study with semi-structured interviews was implemented to explore the perceptions of the healthcare professionals regarding their involvement in the ARCADE clinic.
Setting
The study’s setting is the Breast Surgery/Plastic Surgery Unit of the Azienda USL - IRCCS of Reggio Emilia, specifically the ARCADE nurse-led clinic of the plastic surgery service. Participants were interviewed at the Research, EBP, and IRCCS Unit, Health Professions Directorate of the Azienda USL - IRCCS of Reggio Emilia.
The NAC tattooing offered in ARCADE clinic: a brief overview
As fully described in Maselli et al.16, each NAC tattooing treatment involves, on average, three sessions 30–40 days apart. Up to three nurses specialized in NAC tattooing, using a local anesthetic, performed the treatments on medical indication with aseptic technique in a hospital surgical clinic. They have valuable experience and expertise in the management of cancer patients. The NAC reproduction is performed using a dermograph equipped with sterile disposable needles. The pigments used are bio-absorbable. Since color fading is normal over time, an annual follow-up session is recommended to maintain an optimal cosmetic result. The 3D technique was applied. NAC medical tattooing has been included in the Essential Levels of Care of the Italian National Healthcare System since 201920.
Study population
-
Endpoint 1: data regarding activities and processes where collected from January 2023 to August 2024, when 62 patients were treated with NAC tattooing at the Azienda USL – IRCCS di Reggio Emilia. Specifically, we collected retrospective data of patients that fulfilled the following criteria : (1) adult, (2) being able to speak and write in Italian; (3) willingness to participate in the study and sign written informed consent; (4) have undergone oncological breast surgery with removal of the NAC; (5) have received NAC tattooing.
-
Endpoint 2: starting from the cohort described above, we included patients who had completed the treatment at the date of study submission (6) and (7) agreed to contribute with the photographs of their NAC.
-
Endpoint 3: we included health professionals involved in the provision/evaluation of this service. They were specialists with experience in breast surgery or breast reconstruction, professionals with training and experience in the NAC tattooing, clinical coordinators or managers of health care facilities involved in the service development and management.
Data collection
Data collection was conducted by appropriately trained professionals and research nurses (DM, MT), and registered on the eCRF. Age, surgical NAC reconstruction, monolateral/bilateral tattoo, were patient-related variables collected. The main indicators concerning the Endpoint 1 included the number of tattoo treatments completed/not completed per person, the number of sessions required per person, adverse events, procedural pain, duration of sessions, not-standard adjustments to the procedure, pigments and needles used. For the Endpoint 2, the available photo sets were considered. Those that permitted comparisons (pre/post-treatment, or NAC comparisons), through at least one of the quality indicators (color similarity, symmetry, 3D effect), were included for the blind evaluation. The expert panel consisted of the nurse tattooists (TL, GF, SL) and two nurses PhD students (DM, MT), in order to allow for fairness and technical competence. For the Endpoint 3, the principal investigator (DM) contacted professionals who met the eligibility criteria by email, informing them about the study and proposing their participation. The interested professionals met the principal investigator and received a detailed description of the study. Those willing to participate were included by signing a consent form. Individual interviews were audio-recorded, transcribed verbatim and immediately deleted after transcription. Interview transcripts were stored in pseudo-anonymised form under the responsibility of the principal investigator. Two nurses PhD students (DM, MT) trained in qualitative research conducted the interviews that followed these key-points: first contact with the clinic and expectations; factors that acted as barriers and facilitators in the activities of the clinic; future challenges and opportunities; the role of the nurse in this treatment; the meaning of this clinic within a clinical pathway. The data saturation principle was followed, with enrolment stopping when no new significant themes emerged from the interviews21.
Data analysis
The Endpoint 1 involved the analyses of the frequencies and percentages for process and overall activity data, and by assessing procedural timeframes and costs. The Endpoint 2 involved the descriptive analyses of data regarding the quality of the cosmetic outcome expressed by the expert panel on a 5-points Likert scale. Qualitative findings related to Endpoint 3 were generated through a framework analysis based on the topics discussed in the interview22,23. Three independent researchers (DM, MT, VS) read and familiarized themselves with the interviews, generating initial codes. In a second phase, the codes were shared and discussed until an agreement was reached, after which the research team defined the codes and began generating initial themes. Using the constant comparison method, sub-themes and themes were identified. All analyses were performed in Italian, and the results were translated into English. Methodological rigor and fidelity to the data were pursued through various strategies. The thematic analysis was conducted according to the planned methods: the research team was familiar with qualitative analysis and cancer care. The COREQ criteria for reporting qualitative research have been followed24. Reflexivity was considered by engaging in ongoing researchers’ self-reflection, acknowledging their influence on data collection and interpretation25. The interpretation phase included data triangulation, whereby qualitative themes were compared with quantitative results to identify areas of convergence and divergence26. Integrating these findings strengthened the validity of the results and informed the study’s overall objective.
Results
Organizational sustainability
This paragraph presents the data regarding the activities and processes of the ARCADE clinic, whose activity volumes are illustrated in the table below (Table 1).
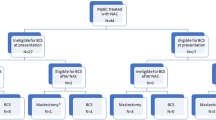
Thirty-three women were included in the retrospective analysis (Fig. 1). Table 2 describes the main characteristics of the cohort: monolateral treatments on previously reconstructed nipples were the most frequent.

Study participants and screening process.
Data presented in Table 3 show that 90% of the sample completed the treatment in 3 sessions, which is the standard of the procedure. Of the remaining 10%, two participants skipped the third tattoo session because the color was already fully and satisfactorily pigmented in the area, with less fading than expected. One participant was not tattooed at the first appointment because of a suspected allergy during the initial assessment, confirmed by the allergologist. The 100% of the sample gained a satisfactory cosmetic result following the correct post treatment care, without adverse events, or other complications like excessive color fading or shifts.
Session duration and the dressings used were standard. The pigments are labeled with numbers from one to nine. Table 4 shows that the color blend applied for the areola were mostly the same for every session type. The color blend used to pigment the nipple differs from the one used for the areola. All the procedures were performed using three needle types, that differed in size and function, defining details or shades. Procedural pain was measured with the numerical rating scale (NRS). 79% of the reported NRS scores ranged from 0 to 3.
Tattoos’ quality evaluation
Experts independently evaluated the digital photo sets, scoring them using a checklist containing quality indicators and a Likert scale (1 = insufficient; 2 = poor; 3 = satisfactory; 4 = good; 5 = excellent). Thanks to continuous teamwork and training updates, all panel members were aligned on quality parameters, ensuring internal calibration. A set of photos was available for 30 patients. Eight sets were excluded because they did not permit comparisons (pre-/post-treatment, or NAC comparisons) through at least one of the quality indicators (color similarity, symmetry, 3D effect). Of the 22 sets included in the analysis (55 images in total), 47% were collected in the first tattoo session: 14 before the tattoo (T0) and 12 immediately after it (T1). In the second session, 28% of the photos were captured: 15 photos of 30-days tattoos (T2) and 13 taken immediately after the tattoo (T3). In the third session, 18% of the photos were collected: 5 photos of the 60-days tattoos (T4) and 13 taken immediately after the tattoo (T5). 7% of photos were captured in the annual follow-up: 2 photos of 1-year tattoo (T6) and 2 taken immediately after the tattoo (T7). As few photos were retrieved, we decided to analyze data anonymously, prioritizing the impartiality of the panel quality assessment over statistical correlations analysis. As evaluated by the experts and illustrated in more detail in Table 5, the cosmetic outcome of the reconstructed NACs showed very good quality, with 4,7 medium score for color similarity and symmetry, and 4,8 for 3D effect. All the photos’ sets allowed for evaluation of the 3D effect (Fig. 2), while five photo sets did not permit evaluation for color similarity and symmetry.

Tattooed NAC with reconstructed nipple. The tattoo at 30 days after the first session is shown in the top right, demonstrating appropriate colour absorption. The central image shows the same NAC immediately after the second session, with a more intense colour illustrating the features of the technique, with a focus on shading and the 3D effect.
Qualitative findings
Five professionals (two nurses, one surgeon, and two managers) involved in the ARCADE clinic were interviewed. Initial themes developed by the research team were discussed to reach their validation. Four thematic macro-areas were finalized: “The value of the clinic”, “Barriers to the service’s development”, “Facilitators”, and “Challenges and future needs”. More details and exemplary quotations are illustrated in Tables 6, 7, 8 and 9.
The value of the clinic
The NAC tattoo service was broadly acknowledged for aiding patients in restoring their self-image and social integration. Participants felt that, in addition to conventional medical treatments, it tackled the psychosocial aspects of cancer recovery. They believed the service offered a holistic and emotionally meaningful support for patients within the cancer care journey, which also motivated providers.
Barriers to the service’s development
Participants highlighted that limited resources, in terms of staffing and funding, constituted a fundamental constraint. They also acknowledged that lengthy logistics and informatics interventions initially delayed the implementation of the initiative. Regarding teamwork, although initial enthusiasm was observed, participants emphasized the subsequent need for increased collaborative efforts and improved coordination. Additionally, managerial changes during the implementation period contributed to the destabilization of the original vision.
Facilitators
According to the interviewees, the initiation of the service was facilitated by the team’s attitude, which was marked by strong dedication, motivation, and a shared commitment to the project’s goals. The service received support at multiple levels from various stakeholders. Notably, the formal recognition of NAC tattooing as a national essential level of care within the public health system was highlighted. Having basic education on sterility concepts, knowledge of the breast cancer care pathway, and the presence of a specialized nurse were key factors that allowed the service to begin. Additionally, ongoing support and recognition from healthcare facility management and local patient associations played crucial roles. Lastly, the patients’ strong confidence in the professionals provided essential support, and the team’s existing expertise was a significant advantage in making patients comfortable and earning their trust.
Challenges and future needs
Participants faced challenges, including developing a data-driven model for assessing workflows and quality standards and integrating the service into institutional pathways through formalization. Managing patient waiting lists and evaluating staff competencies are also crucial. Interviewees suggested that scientific validation and formal recognition of NAC tattooing training, currently offered by external companies without official status, would be helpful. For sustainability, managers should maintain a trained, motivated staff while balancing workforce size, skills, and the service’s specialized needs.
Discussion
This study aimed to assess the feasibility of an NAC tattooing clinic for women who have undergone surgical treatment for breast cancer in Italy. While the central methodology employed complex intervention evaluation, specific goals were achieved to gain a clear picture of the intervention’s feasibility, including organizational sustainability, cosmetic outcome, and professionals’ experience. The relevance of this research lies in its rigorous and innovative approach to the topic, which gains solidity from previous phases16, maintaining coherence with its vision. Moreover, mixed methods enriched the evidence on the multi-level impact of NAC tattooing. Both quantitative and qualitative findings supported the feasibility of the project. The sustainability challenges were mitigated by the resilience of the professional team and the high therapeutic value of ARCADE. Furthermore, the crucial role of training in achieving the high-quality tattoos presented was emphasised, as was the demand for enhanced logistics and assessment. In the following paragraphs, we will discuss the main results of ARCADE_M’s three endpoints reported in this paper.
Endpoint 1 assessed the organizational sustainability: the activity has a standard character, with stable procedural times and predictable material usage. All participants achieved satisfactory results, demonstrating high tolerability and compliance without any complications. These data align with the overall workflow, where the number of 2024 sessions is more stable compared to 2023 (Table 1): organizational and procedural stability, as well as scheduling optimization, reflect the comparable number of treated women. Nevertheless, several factors contribute to the planning of activities. Three professionals were engaged in each intervention (due to training needs before reaching autonomy), working outside ordinary working hours (4 h). Human resources issues limited the flow of activities, as did the limited access to the clinic (only one day a week in the afternoon). In addition to these actionable barriers, the treatment structure, which requires at least three months to be considered complete, impacts the appointment schedule. Moreover, the number of annual follow-ups, which is regarded as replicable with no limits, will systematically grow, overlapping with new patients, if the organizational capacity remains unaltered. The number of new patients in 2024 (N = 28) is fewer than in 2023 (N = 44), as the 2024 touch-ups performed were 24. On the other hand, choosing to prioritize new patients’ interventions will increasingly delay the annual tattoos: in 2024, 16 planned annual tattoos were postponed in 2025. These data show how this trend can be initially balanced, but they also warn us about how these factors firmly influence the possibility of providing complete and timely care.
The experts’ panel evaluation of the treated NACs indicates high-quality scores for NAC similarity, symmetry, and 3D effect. In the absence of a specific and widely acknowledged instrument for quality evaluation in this field, a Likert scale was used. It was noted that symmetry was not always applicable in the evaluations, for example, when breasts with reconstructed NACs are already evidently asymmetrical. Alternatives like NAC shape similarity may be a helpful indicator. Regarding color, human evaluation cannot be as precise as AI comparison. While some inspiring experiences are reported27,28, questions about the everyday applicability, costs, and the absolute necessity for this measurement are to be considered. Although the cosmetic outcome must be evaluated for quality auditing and continuous improvement, an essential part of this is the woman’s perception, which is intimate and can change over time. In other words, pigment composition and its normal fading are worth measuring. However, personalization in every session and biological variables that can influence color uptake must be considered. Another issue is that the actual evaluation of the color fix can be done after 30 days, when the skin has healed and the excess color has faded. After the third session, the patient was unable to attend the clinic for the final evaluation. For a comprehensive assessment, this should be considered, but with consideration for patient burden. Easier contacts and access may be considered.
The themes we developed from the interviews, which are crucial for this field comprehension29, involved in the NAC tattooing, were very informative by integrating quantitative data in this research. Organizational limitations related to logistics and human resources were the primary barriers, as well as poor coordination within the team and uncertainties about the service’s vision and identity. Despite these issues, the resilience of the nurse tattooists in motivation and dedication was the main strength of the project’s progress. The support granted by medical and health professions management integrates that of the associations, research, and patients, who perceived the professionals’ competence and ongoing education within the practice. The value of the clinic emerged clearly from all the interviews: the intervention promotes self-image recovery and societal reintegration, providing a comprehensive and emotionally significant care pathway that addresses a health need. Its relevance is matched by its overall significance in benefiting breast cancer patients and survivors. Moreover, it is important that they can access the service without facing a heavy financial burden, within a healthcare framework that supports this equally. It represents a crucial point to be shared in the scientific and civic community.
The complex intervention methodology enables the identification of various actionable areas and both positive and negative aspects of healthcare services, as demonstrated by similar studies in the field of breast cancer30,31. This project confirms that a multi-stakeholder, mixed-methods research approach is appropriate for addressing complexities and gaps in evidence32.
We have identified seven intervention areas that represent the main challenges and future opportunities associated with ARCADE implementation:
-
1.
Dedicated and motivated personnel.
-
2.
Accountability promotion and data-driven model for quality assessment.
-
3.
Formalize the service in the clinical pathway, enhancing team coordination.
-
4.
Efficient management of the requests.
-
5.
Competence maintenance and evaluation.
-
6.
Validation of the specific training.
-
7.
Concile long-term sustainability with high-level performances.
The integration and formalization of services, as well as the definition of the training pathway and resource requirements, were the main issues faced after this complex intervention evaluation. As Table 10 shows, the actions taken to overcome the detected barriers were building blocks that provided solidity and stability to the service, fundamental for its inclusion in the breast cancer clinical pathway of the healthcare facility.
Empowering people with training makes it possible to increase activities safely, manage waiting lists effectively, and distribute the workload more efficiently. Moreover, the electronic agenda for appointments marks the beginning of formal activities and the regional information flow. Nevertheless, these preliminary data were not sufficient to complete an exhaustive cost evaluation. We know that the cost of materials is around 50 euros for 3 tattoo sessions; the regional reimbursement provided for in the fee schedule is 16.80 euros for each session. Once space, time and human resources are defined and implemented, it will be possible to proceed with cost-effectiveness evaluations and others that consider the health benefits for patients. Notably, the tattoo-only technique can be used with patients who refuse another operation for NAC reconstruction, as well as with those who have potential risk factors for a poor outcome following surgical NAC reconstruction33. In addition, cost savings are suggested, but these still need to be examined in detail34. The organisational aspects of similar implementations are often poorly documented in the literature and lack cohesion in an international context6,16. This makes the research useful and relevant, but also makes it poorly comparable with similar studies, especially given its single-centre design. The small sample size considered for the retrospective analysis of data is another limitation to consider, as also the lack of patient-reported outcomes: due to the ongoing development of the intervention structure, data were not always available or were incomplete. For the same reason, cosmetic outcome evaluations need to be improved, and the new integrated electronic chart will be crucial to overcome these problems. Moreover, similar supportive interventions after breast cancer surgery should also consider the male population, as supported by recent literature3. On the other hand, patients ‘associations strengthened the whole research project, from the development to the results’ analysis: it permitted to continuously compare evaluations and actions to contextual appropriateness and receptivity. Community involvement is considered an integral part of the co-designed approach in oncology35 and will be important in the next implementation phases.
Implications for practice
The significance of the clinic extends beyond the execution of the tattoo, as it plays a crucial role in breast cancer survivorship, completing the care pathway. It is envisaged that the capacities of this service can be extended sustainably, providing space, for example, for research, therapeutic education, survivorship care, referral to local services, and training for dyads, citizens, and professionals. In this comprehensive vision the nurse is a central figure, like this quote remarks:“The nurse can really provide a response that goes beyond just the tattoo, but also in terms of support and guidance within our facilities, like the psychological support, if this need emerges during the reconstruction and tattooing process, and perhaps did not emerge in the previous stages of the journey” (P1). Future steps will be necessary, starting with professionals’ training and a more comprehensive cost evaluation.
Conclusion
A nurse-led NAC tattooing clinic represents a feasible and complex intervention within the context of breast cancer care. The treatments administered exhibited high levels of tolerability, personalization, and quality of cosmetic outcomes. Although subject to the influence of available resources, its sustainability—considering continuity and completeness—appears promising. The use of accountability instruments and competence development serves as protective factors. The implementation of this service has empowered a support network by engaging both community members and healthcare professionals in collaborative efforts, thereby providing a crucial final step in care that may significantly impact psychophysical recovery.
Data availability
The datasets generated and analysed during the current study are not publicly available for confidentiality reasons. However, they are available from the corresponding author upon reasonable request.
Abbreviations
- F:
-
Frequency
- NR:
-
Not reported
- NA:
-
Not applicable
- BL:
-
Bilateral
- ML:
-
Monolateral
References
Ministero della Salute. Il tumore al seno. https://www.salute.gov.it/portale/tumori/dettaglioContenutiTumori.jsp?lingua=italiano&id=5538&area=tumori&menu=vuoto#:~:text=La%20probabilit%C3%A0%20di%20vivere%20ulteriori,morte%20per%20tumore%20nelle%20donne. Last access on 02/07/2025.
Mishra, A., Nair, J. & Sharan, A. M. Coping in Post-Mastectomy breast cancer survivors and need for intervention: systematic review. Breast Cancer (Auckl). 17, 11782234231209126 (2023).
Bhardwaj, P. V., Gupta, S., Elyash, A. & Teplinsky, E. Male breast cancer: a review on Diagnosis, Treatment, and survivorship. Curr. Oncol. Rep. 26(1), 34–45 (2024).
Williams, J. T. W., Pearce, A. & Smith, A. A systematic review of fear of cancer recurrence related healthcare use and intervention cost-effectiveness. Psycho-Oncology Agosto. 30(8), 1185–1195 (2021).
DiCenso, D. & Fischer-Cartlidge, E. Nipple-Areola Tattoos: Making the right referral’. Oncol. Nurs. Forum. 42(6), E376–E381. https://doi.org/10.1188/15.ONF.E376-E381 (2015).
Ercegovac, M. & Serup, J. The sudden rise of cosmetic and medical tattoos on all continents. Curr. Probl. Dermatol. 56, 5–10 (2023).
Barone, M., Cogliandro, A., Salzillo, R., Tambone, V. & Persichetti, P. The role of appearance: definition of Appearance-Pain (App-Pain) and systematic review of Patient-Reported outcome measures used in literature. Aesthetic Plast. Surg. 42(5), 1399–1409. https://doi.org/10.1007/s00266-018-1158-2 (2018). Epub 2018 Jun 19. PMID: 29922843.
Caraccioli, P. G Psychological and psychosocial aspects of medical tattoos in women with breast cancer. Curr. Probl. Dermatol. 56, 181–186 (2023).
Santi, P. L. et al. To heal and take care: medical micropigmentation and its role in improving body image. Medicina Historica. 2023;7. https://www.scopus.com/inward/record.uri?eid=2-s2.0-85162087272&partnerID=40&md5=41dc3dce0018839fd0dcb330d7c8bbc2
Maselli, D. et al. Tattooing to reconstruct Nipple-Areola complex after oncological breast surgery: a scoping review. Support Care Cancer 32(3), 153 (2024).
Griffiths, M. J. S. et al. Primer on health equity research in health economics and outcomes research: an ISPOR special interest group report. Value Health Gennaio. 28(1), 16–24 (2025).
Lett, E. et al. Health equity tourism: ravaging the justice landscape. J. Med. Syst. 46, 1–6 (2022).
Pinho-Gomes, A. C. et al. Values, principles, strategies, and frameworks underlying patient and public involvement in health technology assessment and guideline development: a scoping review. Int. J. Technol. Assess. Health Care. 38(1), e46 (2022).
Mahony, J. et al. The impact of breast care nurses: an evaluation of the McGrath foundation’s breast care nurse initiative. Asia Pac. J. Oncol. Nurs. Marzo. 6(1), 28–34 (2019).
Skivington, K. et al. A new framework for developing and evaluating complex interventions: update of medical research Council guidance. BMJ 30, 2061 (2021).
Maselli, D., Torreggiani, M. & Guberti, M. A nurse-led multidisciplinary service for Nipple-Areola complex Tattooing after breast cancer: reporting on a complex intervention with tidier analysis. BMC Nurs. 25 Ottobre. 23(1), 785 (2024).
Remawi, B. N., Preston, N. & Gadoud, A. Development of a complex palliative care intervention for patients with heart failure and their family carers: a theory of change approach. BMC Palliat. Care 6 Maggio. 24(1), 129 (2025).
Connell, L., Ackerley, S. & Rycroft-Malone, J. Applying the updated MRC framework for developing and evaluating complex interventions with integrated implementation conceptual knowledge: an example using neurorehabilitation online. Front. Health Serv. 6 Maggio. 5, 1562627 (2025).
Damschroder, L. J. et al. Fostering implementation of health services research findings into practice: a consolidated framework for advancing implementation science. Implement. Sci. 4(1), 50 (2009).
Decreto del presidente del consiglio dei ministri 12 gennaio 2017. Definizione e aggiornamento dei livelli essenziali di assistenza, di cui all’articolo 1, comma 7, del decreto legislativo 30 dicembre 1992, n. 502. Gazzetta Ufficiale - Serie Generale n. 65, 18 marzo (2017).
Malterud, K., Siersma, V. D. & Guassora, A. D. Sample size in qualitative interview studies: guided by information power. Qual. Health Res. Novembre. 26(13), 1753–1760 (2016).
Braun, V. & Clarke, V. Using thematic analysis in psychology. Qualitative Res. Psychol. 3(2), 77–101. https://doi.org/10.1191/1478088706qp063oa (2006).
Braun, V. & Clarke, V. Conceptual and design thinking for thematic analysis. Qualitative Psychol. 9(1), 3–26. https://doi.org/10.1037/qup0000196 (2022).
Tong, A., Sainsbury, P. & Craig, J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int. J. Qual. Health Care. 19(6), 349–357. https://doi.org/10.1093/intqhc/mzm042 (2007).
Chan, Z. C., Fung, Y. & Chien, W. Bracketing in phenomenology: only undertaken in the data collection and analysis process. Qualitative Rep. 18(30), 1–9. https://doi.org/10.46743/2160-3715/2013.1486 (2013).
Creswell, J. W. & Creswell, J. D. Research Design: Qualitative, Quantitative, and Mixed Methods Approaches (SAGE, 2017).
Yamamoto, M. et al. Fading and color reproducibility of nipple areola tattoos in Asian patients. Arch Plast Surg. moriplas@tmd.ac.jp) Department of Plastic and Reconstructive Surgery, Graduate School of Medical and Dental Sciences, Tokyo Medical and Dental University, Tokyo, Japan) (2023). https://doi.org/10.1055/a-2309-2731
Levites, H. A. et al. Modeling fade patterns of nipple areola complex tattoos following breast reconstruction. Annals Plast. Surg. Dicembre. 73(Supplement 2), S153–S156 (2014).
Daly, A., Karl, J. & Dunne, S. Art is just something that makes people heal—a qualitative investigation of tattoo artists’ perspectives on cancer survivorship therapeutic tattoos. J. Cancer Survivorship (2024). https://www.scopus.com/inward/record.uri?eid=2-s2.0-85205032668&doi=10.1007%2fs11764-024-01682-4&partnerID=40&md5=91dbb2565cffdb187c9d3ded1923e40c
Olsson Möller, U. et al. Barriers and facilitators for individualized rehabilitation during breast cancer treatment – a focus group study exploring health care professionals’ experiences. BMC Health Serv. Res. 20(1), 252 (2020).
Richmond, H. et al. Development of an exercise intervention for the prevention of musculoskeletal shoulder problems after breast cancer treatment: the prevention of shoulder problems trial (UK PROSPER). BMC Health Serv. Res. 18(1), 463 (2018).
Saal, S. et al. Development of a complex intervention to improve participation of nursing home residents with joint contractures: a mixed-method study. BMC Geriatr. 18(1), 61 (2018).
Cha, H. G., Kwon, J. G., Kim, E. K. & Lee, H. J. Tattoo-only nipple-areola complex reconstruction: another option for plastic surgeons. J. Plast. Reconstr. Aesthetic Surg. Aprile. 73(4), 696–702 (2020).
Gava, A. et al. Dermopigmentation of the nipple-areola complex in a dedicated breast cancer centre, following the Treviso hospital (Italy) LILT model. Ann. Ist Super Sanita. 56(4), 444–451 (2020).
Pii, K. H., Schou, L. H., Piil, K. & Jarden, M. Current trends in patient and public involvement in cancer research: A systematic review. Health Expect. Febbraio. 22(1), 3–20 (2019).
Acknowledgements
This study was partially supported by Italian Ministry of Health - Ricerca Corrente Annual Program 2026. We also thank all of the participants for providing valuable contributions to this research, as also the local associations that support the ARCADE project, in particular the “Amiche del Core” group of Vittorio Lodini Association.
Funding
This work was partially supported by the Italian Ministry of Health – Ricerca Corrente Annual Program 2026.
Author information
Authors and Affiliations
Contributions
Conception/design: DM, SC, FC, LG; Data analysis: MT, VS, GF, DM, TL, SL; Data Interpretation of data: CC, DM, DB; Drafting and Revision: PF, SC, LG, DM. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval and consent to participate
The study protocol was approved by the Area Vasta Emilia Nord ethic committee N° 2024/0133222, on 09/10/2024. Consent to partecipate was collected for each participant.
Consent for publication
Consent for publication was collected for each participant.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Maselli, D., Torreggiani, M., Soffientini, V. et al. The feasibility of a complex intervention, a medical tattooing nurse-led clinic after breast cancer surgery: results from the ARCADE_M mixed-methods study. Sci Rep 16, 1877 (2026). https://doi.org/10.1038/s41598-025-31551-8
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-31551-8
