
Abstract
Type 2 diabetes (T2D) is the most common type of diabetes worldwide, accounting for over 90% of all cases. Micronutrient deficiencies (hidden hunger) are implicated in glycaemic control among T2D patients. This systematic review and meta-analysis aim to investigate the association between multiple micronutrient deficiencies and glycaemic control in patients with type 2 diabetes (T2D). The systematic review and meta-analysis followed the Cochrane Handbook and PRISMA 2020 standards. We searched various databases to identify relevant studies and used a pre-piloted data extraction sheet to gather information. Statistical analysis was conducted using R version 4.3.2 and specific packages. A weak but significant negative correlation was observed between overall micronutrient deficiencies and glycaemic control indices: Fasting Blood Glucose (FBG), Post Prandial Blood Glucose (PPBG), and Glycosylated haemoglobin (HbA1c). Vitamin D deficiency had a small but significant correlation with FBG [\(\:r=\)-0.0920, p-value = 0.0285], PPBG [\(\:r=\:\)-0.2416, p-value = 0.0175), and HbA1c, ( [\(\:r=\:\)-0.1975, p-value < 0.01]. However, there was no significant correlation with HOMA IR. Magnesium deficiency was moderately correlated with HbA1c[\(\:r=\:\)-0.3526, p-value < 0.01]and HOMA IR [\(\:r=\:\)-0.3427, p-value = 0.0016). Zinc had a negligible correlation with Hb1Ac, while iron and vitamin B12 had a low positive correlation. Study reported as statistically significant but weak negative correlation amongst micronutrient deficiency and glycaemic control among T2D patients. Only a small percentage of the variation in HbA1c, FBG, PPBG, and HOMA IR was attributable to micronutrient deficiencies. This study presents the limited explanatory power of micronutrient deficiencies alone on glycaemic control.
Systematic Review Registration: PROSPERO registration number- CRD42023439780. “https://www.crd.york.ac.uk/prospero/display_record.php?RecordID=439780”.
Similar content being viewed by others


Introduction
Diabetes mellitus (T2D – type 2 diabetes mellitus) is a silent epidemic1,2. It accounts for over 90% of diabetes globally. Since 2000, there has been a nearly threefold increase in the worldwide prevalence of diabetes among individuals aged 20 to 79, escalating from 4.6% to 10.5%. The prevalence is expected to increase to 11.3% and 12.2% by 2030 and 2045, respectively2,3,45. There is a shift in the prevalence of T2D, with a rise among the young population, including children1. Policymakers and researchers are actively engaged in addressing the rising disease burden due to T2D6.
T2D is associated with impaired glucose metabolism and glycaemic control. T2D arises from insufficient insulin production by pancreatic beta cells to fulfil metabolic demands. Also, T2D is primarily linked to unhealthy lifestyles and dietary behaviours. In addition, multiple factors influence glycaemic control, and micronutrients may also play a role7.
Poor glycaemic control leads to uncontrolled diabetes, resulting in various complications affecting quality of life, life expectancy, and healthcare costs8,9. Therefore, the key focus in managing T2D revolves around effective glycaemic control, promoting healthy dietary choices and lifestyles, incorporating a balanced diet, consistent physical activity, and maintaining optimal body weight. Furthermore, maintaining effective glycaemic control is crucial to prevent potential long-term complications10,11.
Glycaemic control refers to maintaining the optimal serum glucose levels in diabetes patients12. The glycaemic control is generally evaluated by measuring fasting blood glucose (FBG), postprandial blood glucose (PPBG), and glycosylated haemoglobin (HbA1c)12,13. The HbA1c is a gold standard when quality assurance measures are strict, assays meet international standards, and no conditions interfere with accurate measurement.
Micronutrients, such as vitamins A, B, C, D, and E, and minerals like calcium, folate, iron, and zinc, play pivotal roles in various physiological functions, including insulin production and its action14. Insufficient insulin or its resistance in the body is primarily responsible for developing T2D. Literature suggests micronutrient deficiencies affect insulin production and disrupt various physiological and biochemical processes, oxidative stress, pancreatic beta-cell dysfunction, deranged insulin signalling mechanism, and tyrosine kinase activity15,16. Literature also suggests that chromium, zinc, magnesium, manganese, copper, and vitamin B deficiencies are associated with glucose intolerance. Zinc, an antioxidant, influences insulin metabolism and enzyme activities, and chromium influences insulin’s effectiveness and improves glucose tolerance. Insufficient chromium levels are linked to raised serum cholesterol and triglycerides and impaired glucose tolerance17.
The nexus between hidden hunger or micronutrient deficiencies and T2D has been an underexplored domain in research, often overshadowed by more prominent factors influencing diabetes. Micronutrient deficiency, a subtle yet significant form of undernutrition, arises from insufficient intake or poor absorption of essential vitamins and minerals, often evading immediate clinical detection. A preliminary review by the authors identified varying rates of micronutrient deficiencies and conflicting evidence on the impact on serum glucose17. A study reported a negative correlation between vitamin D deficiency and HbA1c18. However, another study found no significant correlation between vitamin D and glycaemic control19. Studies on zinc showed contradictory evidence of a correlation between zinc and glycaemic control. Alvaro Perez found no significant correlation between zinc and blood glucose levels in a well-controlled T2D. Another study found an inverse significant correlation between zinc and various glycaemic parameters20,21. No significant correlation was found between B12 deficiency and HbA1c22, while a negative correlation was found between vitamin B12 and blood glucose levels23.
The present SRMA explored a research question - whether multiple micronutrient deficiencies affect glycaemic control in T2D. The review findings would make it possible to identify research gaps and provide physicians, public health professionals, program managers, and policy planners with the information they would need to decide whether to screen diabetes patients for micronutrient deficiencies and supplement diet as part of disease management.
Materials and methods
This review is the first to evaluate evidence on the effect of micronutrient deficiency on glycaemic control in individuals with T2D. This review includes studies on twenty-eight micronutrient (vitamins/minerals/electrolytes) deficiency and its effect on glycaemic control. The systematic review and meta-analysis followed the steps and procedures laid down in “The Cochrane Handbook of Systematic Reviews24 and Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines“25 (Supplementary file 6).
Study registration
The study protocol was registered in the “International Prospective Register of Systematic Reviews with registration number CRD42023439780” (https://www.crd.york.ac.uk/prospero/display_record.php?RecordID=439780)26 and was published in BMJ27.
Search strategy
The review included studies published in major databases, such as “PubMed, EMBASE, ProQuest, Cochrane Library, LILACS, and Scopus.” Keywords for the study were developed using various Emtree terms/Medical Subject Headings (MESH)/ Non-MESH terms, combining them with the Boolean operators (OR/ AND- as deemed appropriate) and thoroughly scrutinizing relevant studies and review articles. Additionally search engine like Google Scholar were also explored. SRMA focused on examining all publications that discussed the effect of micronutrient deficiencies on glycaemic control in patients with type 2 diabetes (T2D), regardless of language. Additionally, we have developed a specialized search strategy for accessing Grey Literature through databases like “ProQuest, Scopus, and Embase” as well as hand searches of institutional repositories such as the “International Diabetes Federation and other global organizations and associations dedicated to diabetes and micronutrients.” Primarily, the keywords were developed for the Embase database, which were later adapted to create keywords for other databases. Detailed keywords with search results are provided (Supplementary file 1). “PRESS Evidence-Based Checklist” was used to peer review the search strategy to assess adequacy28(Supplementary file-2). We conducted the initial search in July 2023 and repeated it on 1 January 2024.
Study eligibility
This review covered studies reporting the effect of multiple micronutrient deficiencies on glycaemic control. The micronutrients included in the review were -minerals/electrolytes “zinc, chromium, iron, copper, fluoride, selenium, iodine, manganese, calcium, phosphorus, molybdenum, potassium, Folic acid, magnesium, sodium, vitamins- Vitamin A, Vitamin B1, Vitamin B2, Vitamin B3, Vitamin B5, Vitamin B6, Vitamin B7, Vitamin B9, Vitamin B12, Vitamin C, Vitamin D, Vitamin E, Vitamin K among patients with type 2 diabetes”. The review included all studies published between 1998 and 2023, regardless of demography, nation, language, and ethnicity24. A grey literature search was also done for studies and reports. Studies fulfilling the eligibility criteria but not reporting the outcome of interest were excluded from the study.
Inclusion and exclusion criteria
“Inclusion criteria:
-
1.
T2D patients with or without complications, 18 years or older. Patients of all sexes and ethnicities.
-
2.
Exposure- Micronutrient deficiency and comparator - no deficiency.
-
3.
Analytical cross-sectional, Case-control, cohort, and randomized control trials (RCT).
Exclusion criteria:
-
1.
Patients with type 1 diabetes mellitus, gestational diabetes, and type 2 diabetes among persons less than 18 years.
-
2.
T2D patients on supplementation of micronutrients,
-
3.
Articles based on expert opinions, newspaper articles, reports, narrative reviews, editorials, conference abstracts, and posters.
Study selection
Two primary reviewers independently selected studies. Identified citations were exported and compiled in Rayyan software, and duplicates were removed. DG & NS independently conducted the title and abstract screening using PICOT criteria, and DKM was the arbitrator. Full texts of the selected articles were retrieved for review (NS & DKM, arbitrator- SDG) to ascertain conformity to inclusion criteria before data extraction. In case of disagreement between reviewers, both the reviewers documented the reasons for disagreement and sought advice from a third member, i.e., the arbitrator. The justification was given for excluding the studies from further analysis. Cross references were also checked (NS) before finalizing the list of articles for data extraction. Before data extraction, the two independent researchers reviewed the selected articles for risk of bias (ROB) assessment.
Data extraction
For data extraction, we used a pre-piloted Microsoft Excel data extraction sheet with information on study characteristics, micronutrient names and types, T2D, micronutrient deficiency diagnostic standards, associated cut-off values for deficiencies, and measures of glycaemic control. Details on data extraction are provided in Supplementary File 3. The data extraction was performed independently by two authors (NS and DG), and any disagreements were later discussed and addressed by the research team’s third member (DKM).
Data on outcome variables such as Risk Ratio, Odds Ratio, mean difference, or correlation of micronutrient deficiency with glycaemic control levels (HbA1c, fasting blood glucose (FBG), postprandial blood glucose (PPBG) and insulin sensitivity, estimated using HOMA IR, were recorded among patients with T2D having micronutrient deficiency compared with those without micronutrient deficiency.
Risk of bias assessment
The study quality was evaluated using the “Joanna Briggs Institute Critical Appraisal Checklist”29. This assessment tool encompasses eight for analytical cross-sectional studies, eleven for systematic reviews and meta-analyses, and eleven for cohort studies. Each query permitted responses of ‘yes,’ denoting higher quality; ‘no,’ indicating lower quality; ‘unclear’; or ‘not applicable.’ Two authors (NS and DKM) assessed the methodological quality of the selected articles. Any discrepancies in judgments regarding inclusion were resolved by the third author (SDG). We have generated the Risk of Bias plot using Excel. The result of the quality assessment was further utilized during sensitivity analysis. Criteria for scoring the Risk of Bias was adopted from previously published literature30,31,32. The detailed risk of bias results of all the included studies are attached in Supplementary File 4.
Statistical analysis
A Meta-analysis for understanding the effect of micronutrient deficiency on glycaemic control among T2D patients was performed utilizing extracted information from a pool of 101 studies. Nine micronutrients, namely Magnesium, zinc, Iron, vitamin B12, Vitamin D, Chromium, Copper, Vitamin C, and K2, were initially considered for the analysis. Later, we decided to perform a meta-analysis of those micronutrients with more than three studies or more than one thousand sample sizes33 (namely - Magnesium, zinc, Iron, vitamin B12, Vitamin D) to estimate the summary effect size. Different outcome variables like Odds Ratio (OR), Standardized Mean Differences (SMD), and Correlation Coefficient (\(\:r\)) were reported by the studies to quantify the association between micronutrient deficiency and glycaemic control. The most common outcome variable reported in the studies was the correlation coefficient. Hence, we chose it as a statistical measure for executing meta-analysis. We used the thumb rule for interpreting the strength of the correlation coefficient; a correlation coefficient’s value of 0.00 to 0.30 was interpreted as negligible correlation, 0.3–0.50 as low, 0.50–0.70 as moderate, 0.70–0.90 as high and 0.90-1.00 as extremely high correlation34. The other measures, like OR and SMD, were converted to correlation coefficients using a rapid effect size converter for meta-analysis35 to ensure a single measure of effect for meta-analysis.
We calculated the pooled effect size regarding the correlation coefficient between micronutrient deficiency and glycaemic control and HOMA IR using a random effects model, conservative thresholds of Q for the Q tests, or I2 > 75%. The entire analysis for this study was conducted using RStudio version 4.3.2 using various packages, namely {meta} and {metafor}. The findings from all studies were aggregated and presented as forest plots.
Subgroup analysis
Subgroup analysis was performed for five WHO regions, which are classified as “Region of Americas (AMR), European Region (EUR), Eastern Mediterranean Region (EMR), South-East Asian Region (SEAR), Western Pacific Region (WPR) and African Region (AFR).” Subgroup analysis was also performed to assess statistical heterogeneity for Vitamin D and Magnesium for studies reporting HbA1c as a measure of glycaemic control.
Publication bias
Egger’s test was employed to evaluate the potential for publication bias, with a significance level set at P < 0.05, indicating notable publication bias. We used Rücker and colleague’s (2011) model36 to do a limit meta-analysis to compute a bias-corrected estimate of the effect size termed adjusted effect size. In a limited meta-analysis, we consider that studies’ effect sizes and standard errors are not independent when there are small study effects. This is because publication bias affects small studies, and small studies will have a larger effect size than big ones.
Sensitivity analysis
Sensitivity analysis was conducted to gauge the impact of individual studies on the pooled estimates and to determine whether one study disproportionately influenced the overall results. This analysis primarily involved excluding studies with a weight exceeding 10% to assess their impact on the pooled estimate, as substantial weight might unduly influence the overall estimate. Additionally, studies with a higher risk of bias were excluded to assess their effect on the pooled estimates. Leave-one-out sensitivity analysis was also performed, entailing the systematic removal of one study at a time from the included studies, followed by re-analysis to evaluate each study’s influence on the overall findings.
Overall quality of evidence
The quality of estimates was evaluated using the “Grading of Recommendations Assessment, Development and Evaluation Working Group (GRADE Working Group)”37. Analytical heads were taken from GradePro application and were later modified as per our study objectives, which helped assess the evidence based on study limitations, directness, consistency, precision, and reporting bias. The evidence was later determined as low, moderate, or high quality based on the overall scoring criteria.
Results
Included studies and characteristics
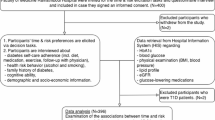
The initial literature search turned up a total of 5,581 records. A total of 2035 duplicates were removed. Following title and abstract screening, we excluded 3254 articles. Two hundred ninety-two full-text articles were assessed for eligibility, of which seventy-six were identified for analysis. A cross-referencing search turned up one paper, while another search for the study on the prevalence of multiple micronutrient deficiencies yielded an additional fifteen studies. Five studies were identified from an updated search undertaken on 1 January 2024. Thus, the total number of studies selected for the meta-analysis became ninety-seven. Three of the 97 studies reported data on more than one micronutrient; hence, we had 101 data sets (N = 30731) for the quantitative evidence synthesis in the subsequent meta-analysis. A grey literature search retrieved 1022 results; however, all studies were excluded as they were duplicated or irrelevant.
We included twenty-eight micronutrients for a search of research studies in our systematic review. We could only find relevant studies on nine of them. These micronutrients were magnesium, zinc, iron, copper, chromium, and vitamins B12, C, D, and K2. The PRISMA flow chart (24) shows the screening and review stages (Fig. 1).

The PRISMA flow chart (97 studies with 101 data sets were included for evidence synthesis).
Summary characteristics of studies
Most of the 101 study data sets deemed pertinent for the quantitative evidence synthesis were cross-sectional analytical studies (n = 57/N = 101). The English language studies were (n = 99/N = 101), and most were hospital-based (n = 95/N = 101). Most studies were conducted in South-East Asia (SEAR) (n = 34/N = 95). Six studies did not provide information about the WHO region, and three did not provide information on the study approach. Vitamin D was the most common micronutrient (n = 20/N = 101). Eight studies focused on zinc (n = 8/N = 101), while seven focused on vitamin B12 (n = 7/N = 101). Table 1 represents the overall characteristics of the included studies.
Risk of bias
The “Joanna Briggs Institute Critical Appraisal Checklist” was used to evaluate the quality of the studies25. There were sixty-eight analytical cross-sectional studies out of the ninety-seven selected studies; all employed appropriate statistical analysis and valid and reliable methods to measure outcomes. Fifty-one studies, or three-fourths of the total, did not address identifying confounding factors; conversely, 73.5% did not state strategies for dealing with such issues Additional critical appraisal questions revealed that most studies had low bias risk. Among eleven prevalence studies out of nineteen, sampling was not done appropriately. None of the studies explicitly discussed the sampling frame.
On the other hand, all the studies were categorized as having a minimal risk of bias for other questions. Three of the six case-control studies also did not address appropriately matching cases and controls, and four did not discuss identifying confounding factors or the strategies to address them. Two systematic reviews and meta-analyses with low bias risk and two cohort studies were identified, one with low bias risk and the other with medium risk38,39,40,41. Study-specific biases are presented in Supplementary File 4.
Meta-analysis
We estimated the pooled effect size of the correlation coefficient for all glycaemic indices and HOMA IR (Table 2). A weak negative correlation coefficient was observed for all glycaemic indices, and it was a statistically significant association. Analysis of 66 studies showed a weak negative correlation between HbA1c and overall micronutrient deficiency (r = -0.17, p-value- <0.0001). The highest estimated correlation coefficient was calculated for T2D patients for whom PPBG was considered as a measure for glycaemic control, indicating that deficiency of micronutrients results in poor glycaemic control more strongly when PPBG [\(\:r=\)-0.2564, p-value < 0.01] is taken as a reference for measuring glycaemic control followed by HOMA IR [\(\:r=\)-0.2081 p-value = 0.0643]. The computed coefficient of determination (\(\:{\:r}^{2})\) was highest for PPBG as an outcome measure, indicating 6.5% changes in PPBG blood sugar due to deficiency by any of the micronutrients, followed by \(\:{\:r}^{2}\) of 4.33% changes in HOMA IR values. We noted a high heterogeneity across analysis which indicates considerable variability across study populations, assessment methods, and contextual factors.

Forest plot for overall micronutrient deficiency and glycaemia control (HbA1c, FBG, PPBG, HOMA IR).
We present our findings as a forest plot (Fig. 2), which provides information on each of the studies included in the analysis and estimated coefficient of correlation, study weight, 95% Confidence interval, p-value, Coefficient of Determination (\(\:{\:r}^{2})\:\) and Cochrane Q test and I2 for heterogeneity. We have used the Random effects model to estimate the pooled correlation coefficient. We have examined the heterogeneity, which was more than 80%, for all glycaemic indices for outcome measures.
The pooled estimate of the correlation coefficient for all micronutrient deficiency is a crude measure as it is a weighted average of the correlation coefficients of the constituent micronutrients. Hence, comparing the pooled estimates for different regions is not appropriate. Therefore, we present the pooled estimates of correlation coefficients for individual micronutrients below:
Vitamin D
We pooled fifty-six studies for Vitamin D, which were tabulated for glycaemic control outcome variables, namely Hb1Ac, fasting blood sugar and postprandial blood sugar, and HOMA IR for insulin sensitivity for estimation and meta-analysis of the pooled correlation coefficient between Vitamin D deficiency and glycaemic control (Fig. 3). A low in magnitude but significant negative correlation coefficient at a 5% level was detected between deficiency of Vitamin D with HbA1c[\(\:r=\:\)-0.1975, p-value < 0.01], FBG [\(\:r=\)-0.0920, p-value = 0.0285] and PPBG [\(\:r=\:\)-0.2416, p-value = 0.0175]. A negative but nonsignificant correlation coefficient was detected between deficiency of vitamin D and levels of HOMA IR [\(\:r=\)-0.2181, p-value = 0.1242].


Forest plot for Vitamin D deficiency and glycaemia control (HbA1c, FBG, PPBG, HOMA IR).
The heterogeneity tests were found to be significant for all glycaemic indices HbA1c[\(\:{I}^{2}=99.7\%,\) p-value = 0], FBG [ \(\:{I}^{2}=75.3\%,\:\)p-value < 0.01], PPBG [\(\:{I}^{2}=87.6\%,\:\text{p}-\text{v}\text{a}\text{l}\text{u}\text{e}\:<\:0.01\)] and HOMA IR [98.7%, p-value < 0.01], indicating a high level of heterogeneity between studies. The coefficient of determination\(\:{\:r}^{2}\) for HbA1cwas \(\:0.039\), indicating that 3.9% of the variation in levels of HbA1cis due to Vitamin D deficiency. These 56 studies reported widely different values for the correlation coefficient between Vit D deficiency and Hb1Ac, ranging from – 0.10 to – 0.73. The estimates of heterogeneity confirm this observation. The values of \(\:{I}^{2}\) for HbA1cwas [\(\:{I}^{2}\)=99.7%, p-value = 0].
Magnesium
A meta-analysis evaluated twenty studies of magnesium divided into four glycaemic indices, indicating poor glycaemic control due to magnesium deficiency. The estimated pooled correlation coefficient was found to be significant and slightly higher in magnitude than Vitamin D. Negative correlation was found between deficiency of magnesium with levels of HbA1c[\(\:r=\:\)-0.3526, p-value < 0.01], FBG [\(\:r=\)-0.2162, p-value < 0.01], PPBG [\(\:r=\:\)-0.2602, p-value < 0.01] and HOMA IR [\(\:r=\:\)-0.3427, p-value = 0.0016] (Fig. 4).

Forest plot for Magnesium deficiency and glycaemia control (HbA1c, FBS, PPBS, HOMA IR).
The magnitude of heterogeneity for studies related to deficiency of magnesium was more than 75% for all glycaemic indices HbA1c[\(\:{I}^{2}=91.7\%,\) p-value = 0], FBG [ \(\:{I}^{2}=81.7\%,\:\)p-value < 0.01], PPBG [\(\:{I}^{2}=89.8\%\:,\:\text{p}\text{v}\text{a}\text{l}\text{u}\text{e}\:<\:0.01\)] and HOMA IR [\(\:{I}^{2}=\)98.7%, p-value < 0.01]. The coefficient of determination\(\:{\:\:r}^{2}\) for magnesium deficiency was \(\:0.1243,\:which\:explains\:\:12.43\text{\%}\:\:\text{v}\text{a}\text{r}\text{i}\text{a}\text{t}\text{i}\text{o}\text{n}\:\text{i}\text{n}\:\text{H}\text{b}\text{A}1\text{c}\text{l}\text{e}\text{v}\text{e}\text{l}\text{s}.\:\).
Zinc
Eight studies were compiled to estimate the pooled correlation coefficient between zinc deficiency and glycaemic indices. A significant pooled correlation coefficient was estimated for the meta-analysis of seven studies for zinc with HbA1cas glycaemic index [\(\:r=\:\)- 0.2162, p-value = 0.0093], and the pooled effect for the rest of the six studies was nonsignificant for FBG as glycaemic index [\(\:r=\:-0.1013\), p-value = 0.1795]. Statistical heterogeneity tests using a random-effects model resulted in significant effects for both HbA1c[\(\:{I}^{2}=83.8\%,\) p-value < 0.01] and FBG [\(\:{I}^{2}=74.8\%,\:\)p-value < 0.01]. The coefficient of determination is calculated as \(\:{\:r}^{2}=0.046\), indicating 4.6%, which is the only variation in levels of Hb1Ac, which a zinc deficiency can explain. For FBG \(\:{\:r}^{2\:}was\:0\:.01,\) indicating only 1% is the variation in levels of FBG, which a zinc deficiency can explain Supplementary File 5 (has supplementary Fig. 1–3).
Iron
Unlike zinc, meta-analysis for three studies of iron each for HbA1c[ \(\:r=\) 0.3347, p-value \(\:=\) 0.1214] and FBG \(\:[r=\) 0.2713, p-value 0.0546] demonstrated a positive pooled estimated correlation coefficient, which was nonsignificant at a 5% significance level. High statistical heterogeneity with \(\:{I}^{2}=98.6\%\:\:\)and \(\:96.5\%,\:\)each with p-value < 0.01, were identified for pooled iron studies for HbA1cand FBG as glycaemic indices, respectively. The coefficient of determination was computed as \(\:{\:r}^{2}=11.2\%,\:\)indicating that variation in levels of Hb1Ac, which a deficiency in iron can explain, is 11.2%, whereas variation in levels of FBG was \(\:{\:r}^{2}=\)7.3% due to iron deficiency Supplementary File 5.
Vitamin B12
The pooled estimate of the correlation coefficient for five studies for vitamin B12 exhibited a very weak positive and statistically nonsignificant correlation coefficient \(\:[r=\:\)0.0139, p-value = 0.8504], indicating no association between glycaemic control and vitamin B12 deficiency, as evidenced by the pool of available five studies. Significant statistical heterogeneity \(\:{I}^{2}=83.5\%\:\:\)with p-value < 0.01 was estimated. Since \(\:r\) is close to zero, the coefficient of determination will indicate that levels of HbA1cwill remain unaffected due to a deficiency of vitamin B12. The 95% CI for \(\:r\) [-0.1305; 0.1583] indicates the range of values, which can be both positive and negative if different samples of studies were taken. A study with a sample size of 932 T2D patients was the maximum among the five studies selected, which estimated a negative correlation coefficient of \(\:r=\:-\:\)0.09, p-value < 0.01, indicating a significant association between poor glycaemic control and vitamin B12 deficiency Supplementary File 5.
Subgroup
We performed subgroup analysis for five WHO regions, classified as “Region of Americas (AMR), European Region (EUR), Eastern Mediterranean Region (EMR), South-East Asian Region (SEAR), Western Pacific Region (WPR), and African Region (AFR)” for Vitamin D and Magnesium. (Table 3). A slightly larger negative correlation coefficient was found between Vitamin D deficiency and levels of HbA1cfor the South-East Asian Region [\(\:r=-0.2637;95\text{\%}\:\text{C}\text{I}\:\)(-0.4927; -0.0347)] followed by the West Pacific region [\(\:r=-0.2398\:;95\text{\%}\:\text{C}\text{I}\:(\)-0.3607; -0.1188)]. The r2 value was 6.97% for the South-East Asian Region, indicating that 6.9% of the variation in levels of HbA1cis due to Vitamin D deficiency. Similarly, Magnesium deficiency was found to have a negative statistically significant association with HbA1cin the South-East Asian Region [\(\:r=-0.3680\:;95\text{\%}\:\text{C}\text{I}\:\)(-0.5371; -0.1990)] followed by the European region [\(\:r=-0.3396;95\text{\%}\:\text{C}\text{I}\:\)(-0.4778; -0.2015)]. The r2 value was 13.54% for the South-East Asian Region, meaning magnesium deficiency accounts for 13.54% of the variation in HbA1clevels. These findings suggest that the correlation between Vit D and Magnesium deficiency and HbA1cvaries between WHO regions.
Sensitivity analysis
All studies were assessed for outliers. Studies with weight over 10% were removed, and the analysis was reiterated. The sensitivity analysis showed no significant change in the estimated pooled correlation coefficient for the micronutrients.
Publication bias
The assessment of publication bias investigated through Eggers’s Regression indicated the presence of bias for overall micronutrients, Vitamin D, and Magnesium for almost all the outcome measures for glycaemic indices Hb1Ac, FBG, PPBG, and HOMA IR. Bias-corrected estimates are present as adjusted estimates for all glycaemic indices in Table 4. Adjusted pooled estimates show an increase in the magnitude of the estimated pool correlation coefficient for almost all glycaemic indices and micronutrients, indicating that deficiency of micronutrients results in poorer glycaemic control, as shown by raised adjusted correlation coefficients in Table 4.
Overall quality of evidence
The GRADE summary (Table 5) evaluates the certainty of evidence for the outcome of interest. Despite a large effect size, micronutrients exhibit low certainty due to serious inconsistency and publication bias. The micronutrients revealed high certainty in the evidence using the PPBG measuring indicator. On the other hand, zinc also exhibited a high level of certainty in the evidence when using the FBG measuring indicator. The result reveals that inconsistencies and, in some cases, imprecision or publication bias limit the overall evidence. This summary underscores the need for more robust and consistent research to strengthen the evidence on the role of micronutrients in T2D management.
-
Risk of bias: Studies were assessed for risk of bias, as explained in the methods section. The rating was done after the studies were examined in each criterion.
-
Inconsistency: Pooled results were assessed to see if they were consistent across studies. This was analysed using the I2 value – if more than 75% is considered serious, if less, then not serious.
-
Indirectness: Assess if the evidence directly answers the research question.
-
Imprecision: Assess if the results are precise enough using the Confidence interval.
-
Publication bias: Checked using the Eggers test, p-value < 0.05 is considered the presence of publication bias.
-
Large effect: Assessed if the effect was large or very large.
-
Plausible confounding: Plausible residual confounding was assessed.
Discussion
This systematic review and meta-analysis (SRMA) is the first of its kind that included ninety-seven studies on T2D covering twenty-eight micronutrients to explore the relationship between glycaemic control and deficiency of micronutrients (hidden hunger). We estimated the pooled effect size of the correlation coefficient for all micronutrients and nine individual micronutrient deficiencies and the indices for glycaemic control viz. FBG, PPBG, HbA1c, and insulin sensitivity in T2D patients. In the earlier SRMA42, the authors revealed a high pooled prevalence of micronutrient deficiencies, 45.30% (95% CI: 40·35% – 50·30%) in T2D Patients. It would be worth exploring whether T2D causes micronutrient deficiency or, conversely, micronutrient deficiency is associated with poor glycaemic control.
We found a weak negative pooled correlation between all micronutrient deficiency and glycaemic control (FBG, PPBG, Hb1Ac), and insulin sensitivity (HOMA IR), the correlation being statistically significant. Glycaemic control measured by PPBG had the higher estimated correlation coefficient. [r= -0.2564, p-value < 0.01], suggesting that micronutrient deficiencies lead to poor glycaemic control more strongly in this group of patients, followed by HOMA IR [r=-0.2081 p-value = 0.0643].
We also examined each micronutrient separately because the pooled correlation coefficient between micronutrient deficiency and glycaemic control is a crude estimate inappropriate for comparing the deficiency of specific micronutrients. Several studies have reported on the effect of specific micronutrient deficiencies on glycaemic control. However, the evidence was inconsistent; some studies reported an association, while others found none17. The present meta-analysis clarifies conflicting reports on the association.
Vitamin D is the most researched micronutrient in the context of glycaemic control in T2D patients. The present meta-analysis based on 56 studies revealed that Vitamin D deficiency has a negligible but significant negative correlation coefficient with HbA1c[r=-0.1975, p-value < 0.01], FBG [r=-0.0920, p-value = 0.0285], and PPBG [r= -0.2416, p-value = 0.0175]. At the same time, there is a negligible nonsignificant negative correlation [r=-0.2181, p-value = 0.1242] between vitamin D deficiency and HOMA IR. We measured the coefficient of determination, \(\:{\:r}^{2}\), to estimate the contribution of vitamin D in poor levels of glycaemic control. The \(\:{\:r}^{2}\)=3.9% for Hb1Ac, 0.85% for FBG, and 5.8% for PPBG, indicating that vitamin D deficiency contributes 6% to 1% to poor glycaemic control measured as PPBG, Hb1Ac, and FBG, respectively.
The findings reported in these fifty-six studies varied widely, as confirmed by heterogeneity estimates. The values of \(\:{\:I}^{2}\)for glycaemic indices were found to be significant for all indices of glycaemic control. Vitamin D deficiency had a significant impact on all these indices, the highest being 5.8% in FBG \(\:\left({\:r}^{2}\right).\:\)Some studies reported a significant and more substantial correlation. A study by Havilah Polur et al. titled ‘Study of vitamin D: A risk factor of type 2 diabetes mellitus’ reported a strong negative correlation between vitamin D and HbA1c [r= -0.993, p-value = < 0.0001]”43. The pooled estimates of the correlation coefficient in our SMRA do not support these findings.
Despite the observation that Vit D has a negligible negative correlation with glycaemic control, Vit D deficiency is quite common among T2D patients. Our recent SRMA reported the highest prevalence of Vitamin D at 60.45% (CI: 55% − 65%) (k = 66). Patients with Type 2 diabetes mellitus need to understand the high frequency of vitamin D deficiency and how it negatively affects bone health and glycaemic control. Several investigations have demonstrated the involvement of vitamin D in blood glucose regulation and target tissue uptake. Several investigations conducted on humans and animals have proven the involvement of vitamin D in insulin production and secretion from β cells. The onset and advancement of type 2 diabetes are brought on by insulin resistance and glucose intolerance. These studies suggest sufficient vitamin D supplementation can help prevent diabetes to some extent, particularly in high-risk populations.
Additionally, some studies on vitamin D have demonstrated postponing complications among chronic T2D patients44. Thus, all pre-diabetics and diabetic patients may be screened for Vitamin D deficiency. Vitamin D supplementation may be considered for inclusion in standard treatment protocol to prevent the harmful effects of Vitamin D deficiency and the progression of diabetes. Zaleha Md Isa et al.45 conducted a comprehensive analysis that revealed the potential impacts of vitamin D deficiency and insufficiency on various aspects such as mental health, complications related to type 2 diabetes (T2D), metabolic syndrome, obesity risk, blood pressure, dyslipidaemia, glycaemic control, nerve-related disease, musculoskeletal complications, and quality of life. However, our research findings do not align with these perspectives, as our combined correlation coefficient estimate suggests a weak negative correlation, primarily derived from observational studies. It is challenging to determine whether vitamin D deficiency is a cause or a consequence of poor glycaemic control.
Based on our most recent SRMA, the prevalence of magnesium deficiency among T2D patients was the second highest at 41·95% (CI 27% − 56%)27. The present analysis of twenty studies for magnesium revealed that it had a significant and slightly higher pooled correlation coefficient than Vitamin D. Magnesium deficiency had a low negative statistically significant correlation with HbA1c[r= -0.3526, p-value < 0.01] and HOMA IR [r= -0.3427, p-value = 0.0016] and a negligible statistically significant correlation with FBG [r= -0.2162, p-value < 0.01], PPBG [r= -0.2602, p-value < 0.01], and levels.
Magnesium is crucial for insulin secretion, binding, and activity, and it serves as a vital cofactor for numerous enzymes involved in carbohydrate metabolism42. Various factors, including disrupted insulin metabolism, poor glycaemic control, and osmotic diuresis, likely cause a decline in serum magnesium levels in individuals with T2D. Magnesium deficiency has been associated with diabetes, insulin resistance, and metabolic syndrome. Studies have shown that inducing magnesium deficiency reduces insulin sensitivity in people without diabetes while supplementing magnesium for four weeks has been found to enhance glucose regulation in elderly individuals without diabetes46. Several authors have indicated that low magnesium levels may be a potential risk factor for the onset and progression of diabetic retinopathy. Our systematic review and meta-analysis on the effect of micronutrient deficiency reveal a moderate negative correlation with glycaemic control and a 12.43% coefficient of determination in T2D patients.
Analysis of three studies on iron revealed a low nonsignificant positive correlation [ \(\:r=\) 0.3347, p-value \(\:=\) 0.1214] of iron for with HbA1cand negligible correlation with FBG \(\:[r=\) 0.2713, p-value 0.0546]. A high level of statistical heterogeneity (\(\:{\:I}^{2}\) >90%, p-value <0.01) was found for pooled iron studies. Contrary to this, a study by Achuthan et al. showed that iron had a statistically significant positive association with HbA1c [r = 0.59, p- value = < 0.001] and FBG [r = 0.43, p value = < 0.001]47.
We found no correlation between glycaemic control and vitamin B12 deficiency, the pooled estimate of five available studies being \(\:r=\:\)0.0139 ( p-value = 0.8504). There was a significant statistical heterogeneity \(\:{(I}^{2}=83.5\%\:\:\)with p-value < 0.01). It seems HbA1cwould remain unaffected due to a deficiency of vitamin B12. However, a study among these five studies with a sample size of 932 T2D patients showed a weak negative but significant correlation coefficient (\(\:r=-\:\)0.09, p-value < 0.01). The pooled correlation coefficient estimate does not support the finding of a significant relation.
Analysis of eight studies of zinc revealed a negligible and nonsignificant correlation (r=-0.2622, p-value = 0.0093) with HbA1c and FBG (r=-0.1013, p-value = 0.1795). The coefficient of determination, \(\:{\:r}^{2}=0.046\)indicates that only a fraction of HbA1clevels can be attributed to a zinc deficiency. However, Farooq et al. reported “a statistically significant negative correlation of zinc with HbA1c [r= -0.472, p- value = < 0.001] and FBG [r= -0.223, p- value= 0.001]”48. Due to its antioxidant properties, zinc may assist in lowering blood sugar levels. Additionally, when T2D patients’ zinc levels are restored, it may mitigate the negative effects of oxidative stress and avert complications from diabetes. According to several studies, middle-aged people with type 2 diabetes who have low serum zinc levels are at independent risk for cardiovascular death and fatal or nonfatal myocardial infarction. Research49 also revealed that daily zinc supplementation reduces glycated haemoglobin levels and enhances impaired fasting glucose. Our research showed that those with poorly managed diabetes had low levels of magnesium and zinc. Earlier studies have suggested that numerous health problems associated with diabetes are linked to low serum levels of magnesium and zinc, and supplementation could be tried to avoid such consequences. Nevertheless, additional general population-based studies are required to clearly understand Magnesium and Zinc supplementation’s role in glycaemic control.
Limitations
The present SRMA was comprehensive and exhaustive and searched seven databases for studies of various micronutrient deficiencies in T2D patients with no language restrictions; the possibility remains for missing some relevant pieces of evidence on micronutrient deficiency and glycaemic control. Further, most studies included in the systematic review and meta-analysis were cross-sectional and hospital-based; it may not be appropriate to conclude a causal association between the observed effect size of glycaemic control and levels of micronutrient deficiency. None of the studies was designed to establish cause and effect relationship. The correlation coefficient cannot and should not be used to interpret causality. Most studies focused on descriptive analysis and did not evaluate the effects of confounding factors on the outcome measurement- the glycaemic control. In addition, the studies included in SRMA were highly heterogeneous.
Conclusions
Based on the systematic review and meta-analysis findings, we may safely conclude that overall micronutrient deficiency and deficiency of individual micronutrients such as Vit D, B 12, Magnesium, and Zinc have a week negative and statistically significant correlation with glycaemic control measured in terms of FBG, PPBG and HbA1c, and insulin resistance (HOMA IR). Although the correlation is weak, the coefficient of determination explained a small fraction of poor glycaemic control. Yet, it may not be pertinent to conclude that it is causal because the results are primarily based on observational studies.
Most studies (97%) were hospital-based. Hence, well-designed community-based studies would be needed. The review also indicated a need for analytical case control, cohort studies, and randomised control trials with the clear and specific research question (s) to establish the conclusive role of micronutrient deficiency in glycaemic control in diabetic patients.
The present SRMA provides weak evidence of a relationship between micronutrient deficiency and glycaemic control, precluding strong recommendations for micronutrient supplementation in diabetic patients. American Diabetic Association’s standard of care in diabetes (2024) does not support supplementation with vitamins, minerals such as chromium and vitamin D, herbs, or spices such as cinnamon or aloe vera for glycaemic control due to lack of solid evidence. Moderate prevalence of overall micronutrient deficiency (45.30%) and high prevalence of Vitamin D (60.45%), followed in order by Magnesium (41.95%), and its statistically significant negative correlation with most indices of glycaemic control may prompt to suggest routine screening and managing micronutrient deficiencies in patients with T2D. However, considering the lack of sufficient evidence, we recommend more community-based research to understand the role of micronutrient deficiencies in glycaemic control and insulin resistance.
Data availability
The datasets used and/or analysed during the current study available from the corresponding author on reasonable request.
References
Salman, R. A., AlSayyad, A. S. & Ludwig, C. Type 2 diabetes and healthcare resource utilisation in the Kingdom of Bahrain. BMC Health Serv Res [Internet]. ;19(1):939. Available from: https://bmchealthservres.biomedcentral.com/articles/ (2019). https://doi.org/10.1186/s12913-019-4795-5
Vos, T. et al. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019. The Lancet [Internet]. ;396(10258):1204–22. (2020). Available from: https://linkinghub.elsevier.com/retrieve/pii/S0140673620309259
IDF Diabetes Atlas. 10th edition 2021 [Internet]. [cited 2023 Nov 28]. Available from: https://diabetesatlas.org/atlas/tenth-edition/
Stein, A. D., Obrutu, O. E., Behere, R. V. & Yajnik, C. S. Developmental undernutrition, offspring obesity and type 2 diabetes. Diabetologia [Internet]. ;62(10):1773–8. Available from: http://link.springer.com/ (2019). https://doi.org/10.1007/s00125-019-4930-1
World Health Organization. World Health Organization (Diabetes - World Health Organization, 2022).
Khan, M. A. B. et al. Epidemiology of Type 2 Diabetes – Global Burden of Disease and Forecasted Trends. J Epidemiol Glob Health [Internet]. ;10(1):107. (2019). Available from: https://www.atlantis-press.com/article/125921499
ADA. American Standards of Medical Care in Diabetes American STANDARDS OF MEDICAL CARE IN DIABETES American Diabetes Association—. The Journal of Clinical and Applied Research and Education. 2023;46(Supplement 1):1–298. (2023).
Azzam, M. M., Ibrahim, A. A. & Abd El-Ghany, M. I. Factors affecting glycemic control among Egyptian people with diabetes attending primary health care facilities in Mansoura District. Egypt J Intern Med [Internet]. ;33(1):33. Available from: https://ejim.springeropen.com/articles/ (2021). https://doi.org/10.1186/s43162-021-00065-w
LeRoith, D. & Smith, D. O. Monitoring glycemic control: The cornerstone ofdiabetes care. Clin Ther [Internet]. ;27(10):1489–99. (2005). Available from: https://linkinghub.elsevier.com/retrieve/pii/S0149291805001980
Neuenschwander, M. et al. Role of diet in type 2 diabetes incidence: umbrella review of meta-analyses of prospective observational studies. BMJ [Internet]. ;l2368. Available from: https://www.bmj.com/lookup/doi/ (2019). https://doi.org/10.1136/bmj.l2368
Sami, W., Ansari, T., Butt, N. S. & Hamid, M. R. A. Effect of diet on type 2 diabetes mellitus: A review. Int J Health Sci (Qassim) [Internet]. ;11(2):65–71. (2017). Available from: http://www.ncbi.nlm.nih.gov/pubmed/28539866
Bin Rakhis, S. A., AlDuwayhis, N. M., Aleid, N., AlBarrak, A. N. & Aloraini, A. A. Glycemic Control for Type 2 Diabetes Mellitus Patients: A Systematic Review. Cureus [Internet]. ; (2022). Available from: https://www.cureus.com/articles/92743-glycemic-control-for-type-2-diabetes-mellitus-patients-a-systematic-review
Monnier, L. & Colette, C. Target for Glycemic Control. Diabetes Care [Internet]. ;32(suppl_2):S199–204. (2009). Available from: https://diabetesjournals.org/care/article/32/suppl_2/S199/26598/Target-for-Glycemic-ControlConcentrating-on
Younes, S. The role of micronutrients on the treatment of diabetes. Hum. Nutr. Metab. 35, 200238. https://doi.org/10.1016/j.hnm.2023.200238 (2024).
Walker, A. F. Potential micronutrient deficiency lacks recognition in diabetes. Br J Gen Pract [Internet]. ;57(534):3–4. (2007). Available from: http://www.ncbi.nlm.nih.gov/pubmed/17244416
Christopher Edet, E. Micronutrient deficiency, a novel nutritional risk factor for insulin resistance and syndrom X. Archives Food Nutritional Sci. 2 (1), 016–30 (2018).
Mangal, D. K. et al. Hidden hunger in patients with type 2 diabetes (T2D) and its effect on glycaemic control: a protocol for systematic review and meta-analysis. BMJ Open 14(3):e078688. https://doi.org/10.1136/bmjopen-2023-078688 (2024).
Iqbal, K., Islam, N., Mehboobali, N., Asghar, A. & Iqbal, M. P. Association of vitamin D deficiency with poor glycaemic control in diabetic patients. J Pak Med Assoc [Internet]. ;66(12):1562–5. (2016). Available from: http://www.ncbi.nlm.nih.gov/pubmed/28179690
Olt, S. Relationship between vitamin D and glycemic control in patients with type 2 diabetes mellitus. Int J Clin Exp Med [Internet]. ;8(10):19180–3. (2015). Available from: http://www.ncbi.nlm.nih.gov/pubmed/26770553
Sudan, H. & Asaad, R. Evaluation of Serum Zinc Levels and Its Relationship to Glycemic Control and:ipd Profile in Type (2) Diabetes Mellitus. Bulletin of Pharmaceutical Sciences Assiut [Internet]. ;45(2):1051–61. (2022). Available from: https://bpsa.journals.ekb.eg/article_271791.html
Perez, A. et al. Association between zinc nutritional status and glycemic control in individuals with well-controlled type-2 diabetes. Journal of Trace Elements in Medicine and Biology [Internet]. ;50:560–5. (2018). Available from: https://linkinghub.elsevier.com/retrieve/pii/S0946672X17308660
Abubakr, G. O., Hasan, K. M., Al-Rawy, H. & Hamid, S. F. Prevalence of B12 deficiency among patients with type 2 diabetes mellitus using Metformin in Sulaimani governorate /Kurdistan region of Iraq. Advanced Medical Journal [Internet]. ;6(1):28–33. (2020). Available from: https://amj.khcms.edu.krd/index.php/main/article/view/275
Lee, Y. J., Wang, M. Y., Lin, M. C. & Lin, P. T. Associations between Vitamin B-12 Status and Oxidative Stress and Inflammation in Diabetic Vegetarians and Omnivores. Nutrients [Internet]. ;8(3):118. (2016). Available from: http://www.mdpi.com/2072-6643/8/3/118
Higgins, J. P. T. et al. Cochrane handbook for systematic reviews of interventions [Internet]. Cochrane Handbook for Systematic Reviews of Interventions. wiley; 2019 [cited 2024 Feb 14]. 1–694 p. Available from: https://onlinelibrary.wiley.com/doi/book/https://doi.org/10.1002/9781119536604
Page, M. J. et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ [Internet]. ;n71. Available from: https://www.bmj.com/lookup/doi/ (2021). https://doi.org/10.1136/bmj.n71
PROSPERO [Internet]. [cited 2024 May 21]. Available from: https://www.crd.york.ac.uk/prospero/display_record.php?RecordID=439780
Mangal, D. K. et al. Burden of micronutrient deficiency among patients with type 2 diabetes (T2D): A systematic review and Meta-analysis. BMJ Nutrition, Prevention & HealthUnpublished e000950. https://doi.org/10.1136/bmjnph-2024-000950 (2025).
McGowan, J. et al. PRESS Peer Review of Electronic Search Strategies: 2015 Guideline Statement. J Clin Epidemiol [Internet]. ;75:40–6. (2016). Available from: https://linkinghub.elsevier.com/retrieve/pii/S0895435616000585
JBI -The University of Adelaide [Internet]. JBI Critical Appraisal Tools. Available from: https://jbi.global/critical-appraisal-tools
Manosroi, W., Phudphong, P., Atthakomol, P. & Phimphilai, M. The differences of serum lipid profiles between primary aldosteronism and essential hypertension: a meta-analysis and systematic review. BMC Endocr Disord [Internet]. ;22(1):217. Available from: https://bmcendocrdisord.biomedcentral.com/articles/ (2022). https://doi.org/10.1186/s12902-022-01135-y
Nalbant, G., Hassanein, Z. M., Lewis, S., Chattopadhyay, K. & Content Structure, and Delivery Characteristics of Yoga Interventions for Managing Hypertension: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Front Public Health [Internet]. ;10. Available from: https://www.frontiersin.org/articles/ (2022). https://doi.org/10.3389/fpubh.2022.846231/full
Singh, T., Tripathy, B., Pandey, A. K., Gautam, D. & Mishra, S. S. Examining birth preparedness and complication readiness: a systematic review and meta-analysis of pregnant and recently delivered women in India. BMC Womens Health [Internet]. ;24(1):119. Available from: https://bmcwomenshealth.biomedcentral.com/articles/ (2024). https://doi.org/10.1186/s12905-024-02932-4
Pandey, A. K., Gautam, D., Tolani, H. & Neogi, S. B. Clinical outcome post treatment of anemia in pregnancy with intravenous versus oral iron therapy: a systematic review and meta-analysis. Sci Rep [Internet]. ;14(1):179. (2024). Available from: https://www.nature.com/articles/s41598-023-50234-w
Mukaka, M. M. Statistics corner: A guide to appropriate use of correlation coefficient in medical research. Malawi Med J [Internet]. ;24(3):69–71. (2012). Available from: http://www.ncbi.nlm.nih.gov/pubmed/23638278
rESCMA, V. H. & Kenner [Internet]. [cited 2024 May 21]. (2020). Available from: https://www.rescma.com/
Sterne, J. A., Egger, M., Moher, D. & Boutron, I. Addressing reporting biases editors: In: (eds Higgins, J. P. T., Churchill, R. & Chandler, J.) CM, Cochrane Handbook for Systematic Reviews of Interventions. Cochrane; 241–245. (2017).
Migliavaca, C. B., Stein, C., Colpani, V., Munn, Z. & Falavigna, M. Quality assessment of prevalence studies: a systematic review. J Clin Epidemiol [Internet]. ;127:59–68. (2020). Available from: https://linkinghub.elsevier.com/retrieve/pii/S0895435619308194
Taderegew, M. M. et al. Vitamin D deficiency and its associated factors among patients with type 2 diabetes mellitus: a systematic review and meta-analysis. BMJ Open [Internet]. ;13(10):e075607. Available from: https://bmjopen.bmj.com/lookup/doi/ (2023). https://doi.org/10.1136/bmjopen-2023-075607
Lei, X. et al. Serum and supplemental vitamin D levels and insulin resistance in T2DM populations: a meta-analysis and systematic review. Sci Rep [Internet]. ;13(1):12343. (2023). Available from: https://www.nature.com/articles/s41598-023-39469-9
Rashad Mostafa, N., Ali, A. A. M. & Marzo, R. R. The effect of vitamin D deficiency on glycemic control in patients with type 2 diabetes mellitus. Healthc Low Resour Settings [Internet]. ;11(s2). (2023). Available from: https://www.pagepressjournals.org/index.php/hls/article/view/11340
Abubaker, S. et al. Association Between Vitamin D Levels and Glycemic Control Among Adult Diabetic Patients in Riyadh, Saudi Arabia. Cureus [Internet]. ; (2022). Available from: https://www.cureus.com/articles/100791-association-between-vitamin-d-levels-and-glycemic-control-among-adult-diabetic-patients-in-riyadh-saudi-arabia
Sinha, S. & Sen, S. Status of zinc and magnesium levels in type 2 diabetes mellitus and its relationship with glycemic status. Int J Diabetes Dev Ctries [Internet]. ;34(4):220–3. Available from: http://link.springer.com/ (2014). https://doi.org/10.1007/s13410-014-0196-9
Polur, H., Kedam, D., kumar, K. R. & Vinodh, P. Study of vitamin D: A risk factor of type2 diabetes mellitus. J. Pharm. Sci. Res. 5 (1), 5–7 (2013).
Gulseth, H. L., Wium, C., Angel, K., Eriksen, E. F. & Birkeland, K. I. Effects of Vitamin D Supplementation on Insulin Sensitivity and Insulin Secretion in Subjects With Type 2 Diabetes and Vitamin D Deficiency: A Randomized Controlled Trial. Diabetes Care [Internet]. ;40(7):872–8. (2017). Available from: https://diabetesjournals.org/care/article/40/7/872/30123/Effects-of-Vitamin-D-Supplementation-on-Insulin
Md Isa, Z., Amsah, N. & Ahmad, N. The Impact of Vitamin D Deficiency and Insufficiency on the Outcome of Type 2 Diabetes Mellitus Patients: A Systematic Review. Nutrients [Internet]. ;15(10):2310. (2023). Available from: https://www.mdpi.com/2072-6643/15/10/2310
Tosiello, L. Hypomagnesemia and diabetes mellitus. A review of clinical implications. Arch Intern Med [Internet]. ;156(11):1143–8. (1996). Available from: http://www.ncbi.nlm.nih.gov/pubmed/8639008
Achuthan, A. & Mageswari, U. Correlation between serum free iron, glycated hemoglobin and insulin resistance in uncontrolled type-2 diabetic patients. Natl J Physiol Pharm Pharmacol [Internet]. ;7(6):1. (2017). Available from: http://www.scopemed.org/fulltextpdf.php?mno=252240
Farooq, D., Alamri, A., Alwhahabi, B., Metwally, A. & Kareem, K. The status of zinc in type 2 diabetic patients and its association with glycemic control. J Family Community Med [Internet]. ;27(1):29. Available from: https://journals.lww.com/ (2020). https://doi.org/10.4103/jfcm.JFCM_113_19
Singh, R. B. et al. Current Zinc Intake and Risk of Diabetes and Coronary Artery Disease and Factors Associated with Insulin Resistance in Rural and Urban Populations of North India. J Am Coll Nutr [Internet]. ;17(6):564–70. Available from: http://www.tandfonline.com/doi/abs/ (1998). https://doi.org/10.1080/07315724.1998.10718804
Acknowledgements
None.
Funding
Abbott Nutrition Research and Development. Grant Number- RA40.
Author information
Authors and Affiliations
Contributions
DKM, SDG, and FA conceptualized the research question and objectives. DKM, NS, DG, AKP, and HT have contributed substantially to the article’s concept and design. RT provided project management support for the research study. DKM, AKP, NS, and DG drafted the article. HT, AKP, DKM and DG conceptualised the statistical analysis of the data for meta-analysis. It was critically reviewed for the proper intellectual content after inputs by DKM, SDG, RT, NS, DG, AKP, HT, and FA They have accessed and verified the underlying data reported in the manuscript. DKM, NS, DG, AKP, KCS, and JP prepared the search strategy for the study. DKM, SDG, SK, RT, NS, DG, AKP, and FA critically reviewed and approved the version for submission.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Mangal, D.K., Shaikh, N., Tolani, H. et al. A systematic review and meta-analysis to assess the effect of hidden hunger on glycaemic control in patients with type 2 diabetes. Sci Rep 16, 1936 (2026). https://doi.org/10.1038/s41598-025-31681-z
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-31681-z
