
Abstract
The escalating conflict in Gaza since October 2023 has caused an unprecedented humanitarian crisis, widespread destruction, and mass displacement, profoundly impacting mental health. While depression is prevalent in war-affected regions, Gaza shows exceptionally high rates, with some studies reporting up to 99.5% prevalence. Crucially, comparative studies directly examining depression prevalence between Gaza war survivors who remained and those who fled have been notably absent. This cross-sectional study aimed to compare screened depression prevalence among Gaza war survivors, specifically differentiating between those who remained within Gaza and those who fled to outside Palestine, and to assess associated sociodemographic and war-related factors. Data were collected from 788 adult Palestinian participants, including 383 individuals who fled Palestine and 405 who remained in Gaza. Depression symptoms were assessed using the online self-administered Patient Health Questionnaire-9 (PHQ-9). Depression severity levels were classified according to standard cut-off scores, and logistic regression analyses were conducted to identify factors associated with depression. An alarmingly high overall prevalence of moderate-to-severe depression (82%) was found, with 37% experiencing severe depression. The fled group exhibited a significantly higher prevalence of moderate-to-severe depression (90.86%) compared to the non-fled group (72.59%), with nearly half (49.87%) of the fled group suffering from severe depression. Logistic regression analysis revealed that being in the fledgling group, younger age, and losing a family member significantly increased the odds of moderate-to-severe depression. Over 20% of respondents reported suicidal ideation nearly every day. Risk factors for depression appeared to operate similarly across both populations. This study highlights an exceptionally high prevalence of depression among Gaza war survivors, with those who fled experiencing significantly greater severity. The findings underscore the profound psychological burden of forced displacement and emphasize the urgent need for comprehensive, long-term mental health support for all war survivors.
Similar content being viewed by others
Introduction
The ongoing conflict in Gaza, which dramatically escalated in October 2023, has precipitated an unprecedented humanitarian crisis, characterized by intense hostilities, widespread destruction, and mass displacement1. The fragile infrastructure of the region has been further damaged by decades of military occupation, blockade, economic hardship, and political instability2. Reports indicate extensive damage to the housing sector and critical infrastructure, with over 84% of medical complexes damaged by January 2025, and many hospitals rendered inoperable3. This has forced approximately 1.9 million people, nearly 90% of Gaza’s population, into internal displacement, living in overcrowded shelters and makeshift camps with severe shortages of water, food, and other essential services4. Many families have endured multiple displacements and suffered profound losses, including homes and loved ones4.
Armed conflicts, particularly those marked by prolonged violence and forced displacement, exact a severe psychological toll on affected populations5,6,7. Common mental health issues observed in survivors include depression, anxiety, and post-traumatic stress disorder (PTSD)5. While meta-analyses of war-affected regions generally report prevalence rates for these disorders were 28.9%, 30.7%, and 23.5%, respectively8, the situation in Gaza is notably more severe.
Among the myriad psychological challenges, depression stands out as a significant mental health burden for Gaza war survivors3. Aldabbour et al. reported that 84.5% of internally displaced adults exhibited moderate-to-severe levels of depression3. In a more recent investigation, Albelbeis et al. documented an extraordinarily high prevalence of depressive symptomatology (99.5%) among internally displaced persons in southern Gaza during mid-2024, with approximately 70% classified within the extreme severity range9. Furthermore, Palestinian women migrants residing in a Gaza camp in Jordan reported 73% severe depression during the outbreak of the war10. These figures underscore the pervasive and severe nature of depression in this population.
Depression is highly prevalent among Gaza war survivors, both those who remain in the sector and those who fled, though the patterns differ. Residents face ongoing bombardment, famine, and repeated displacement, with rates exceeding 70–80% in 2023–20253, while many people who fled Gaza suffer from war injuries and severe psychological trauma, leading to a noticeable deterioration in the general health of the displaced population11. Inside Gaza, worsening living conditions and comorbid PTSD and anxiety accelerate mental health decline, whereas refugees experience chronic economic and political stressors that lead to prolonged hopelessness despite initial safety.
Therefore, this cross-sectional study aims to compare the screened prevalence of depression among Gaza war survivors who remained within Gaza versus those who fled and to assess the sociodemographic and war-related factors associated with their mental health outcomes.
Primary hypothesis:
Palestinians who fled Palestine will show different levels of depression severity compared to those who remained in Gaza.
Secondary hypotheses:
Sociodemographic and contextual factors (e.g., gender, age, marital status, displacement status) will be associated with depression severity.
Interaction effects (e.g., displacement × gender, displacement × age) may further explain variation in depression severity.
Methods
Study design
This study employed a cross-sectional design to estimate and compare the prevalence of screened depression among Gaza war survivors. Data were collected over three months, from June 2024 to August 2024, using an online self-report survey. Conducting research during an active humanitarian crisis necessitated remote, technology-based data collection.
Participants
Participants were adult Palestinians aged 18 years and above who were either residing in Gaza during data collection or had been evacuated outside Gaza due to the ongoing genocide. The inclusion criteria required participants to be ≥ 18 years old, residing in Gaza or displaced abroad during the war, and able to provide informed consent. Individuals not meeting these criteria were excluded.
A total of 785 participants completed the survey. Despite the constraints of wartime conditions, the sample size exceeded the minimum required sample of 323, calculated using Cochran’s formula with a presumed prevalence of 30% from previous meta-analytic estimates.
Data collection and sampling
An online questionnaire was utilized to assess symptoms of depression. The survey link was disseminated through multiple channels, including social media platforms (e.g., WhatsApp, Facebook, and Telegram), community groups, and professional networks. It was shared in public posts, group chats, and via direct messages to reach individuals across different regions. Additionally, local community leaders and volunteers were asked to circulate the link within their networks to enhance reach among affected populations. Due to the ongoing humanitarian crisis and limited mobility in Gaza, an online survey was the most practical way to get participants safely. A convenience sampling approach has been utilized, and we used Cochran’s formula to calculate the required sample size based on a previous systematic review with an estimated prevalence of 30%12,13. With a 95% confidence level and a 5% margin of error, the minimal sample size was 323. Although convenience sampling was used due to wartime constraints, several steps were taken to reduce bias and improve representativeness. The survey link was widely distributed across multiple social media platforms and community networks, including public groups, university channels, professional forums, and local community leader networks. This broad dissemination helped reach participants with diverse demographic and displacement backgrounds, including both individuals inside Gaza and those evacuated abroad. Despite the limitations of non-probability sampling, these efforts enhanced the diversity of respondents and supported the adequacy of the sample for estimating the prevalence of depression in the affected population. Our study included 785 replies, which provided appropriate statistical power and representativeness.
Instrument
Depression symptoms were assessed using the Patient Health Questionnaire (PHQ-9), a validated screening instrument. Responses were self-reported, and no professional assessment or diagnostic confirmation was conducted. The use of a single standardized instrument to assess depression prevalence is scientifically justified on both methodological and pragmatic grounds. First, the PHQ-9 is one of the most widely validated screening tools for depressive symptomatology across diverse cultural, linguistic, and clinical contexts, demonstrating robust psychometric properties, including high internal consistency, test–retest reliability, and convergent validity with clinical diagnoses. Second, the PHQ-9 has been extensively used in population-based surveys and humanitarian settings, where its brevity, ease of administration, and minimal respondent burden are essential for feasibility, particularly under conditions of displacement, conflict, or crisis. Furthermore, reliance on a single, validated measure enhances comparability with existing epidemiological studies, thereby facilitating meta-analytic integration and cross-contextual benchmarking. While multi-method assessments may provide additional nuance, the PHQ-9 offers a scientifically rigorous, resource-efficient, and contextually appropriate means of estimating depression prevalence in large-scale field studies.
The Patient Health Questionnaire-9 (PHQ-9)14 is a self-administered tool consisting of 9 items designed to evaluate the severity of depressive symptoms experienced over the past two weeks. Respondents rate each item on a 4-point Likert scale from 0 (not at all) to 3 (nearly every day), resulting in a total score that can range from 0 to 27. Based on these total scores, the severity of depression was categorized into minimal-to-mild (less than 10 score) and moderate to severe (more than 10 score). It has been validated in Arabic15 and has demonstrated strong reliability and validity in previous studies conducted in conflict-affected populations. The PHQ-9 questionnaire includes items addressing issues such as “having little interest or pleasure in doing things,” “thoughts of being better off dead,” and “thoughts of self-harm.” The PHQ-9 has shown excellent internal consistency, with a reported Cronbach’s alpha of 0.90, reflecting strong reliability.
Ethical considerations
Ethical approval for the study was obtained from the Research Ethics Committee at Al-Azhar University, and all procedures adhered to the Declaration of Helsinki16. Participants provided informed consent before voluntarily completing the questionnaire. To minimize distress, the survey included an introductory statement explaining its purpose and assuring participants that they could withdraw at any time. Strict confidentiality was maintained by collecting no identifying information, storing responses on a secure, encrypted platform, restricting access to authorized researchers only, and guaranteeing that data was not shared with any third parties.
Data analysis
Descriptive statistics were initially computed to provide a comprehensive characterization of the study sample using SPSS (version 26)17. Variables assessed included sociodemographic and war-related factors such as age, gender, marital status, educational attainment, displacement status, employment loss, and bereavement due to war-related fatalities. Comparative analyses were subsequently conducted between participants in the “fled group” (individuals who left Palestine) and the “non-fled group” (individuals who remained in Gaza). Group differences were evaluated using significance testing, with p-values reported to identify statistically meaningful distinctions across demographic and war-related characteristics.
To identify factors associated with moderate-to-severe depression, logistic regression analyses were employed, appropriate for the binary outcome and for estimating adjusted associations in the presence of multiple covariates. Analyses proceeded in two stages. First, univariate logistic regressions were fitted for each independent variable (fleeing status [fled vs. non-fled], age, gender, educational attainment, marital status, employment loss due to the war, forced displacement from one’s home, and bereavement due to a family member’s death in the war). Variables meeting p < 0.10 in univariate analyses, together with theory-driven covariates, were entered in a multivariable logistic model (Enter method) to adjust for confounding and estimate independent effects. For each predictor, crude and adjusted odds ratios (OR) with 95% confidence intervals (CI) and two-sided p-values were reported. Model adequacy was evaluated using the Hosmer–Lemeshow goodness-of-fit test, − 2 Log Likelihood, and Nagelkerke R². Multicollinearity was assessed via tolerance/VIF from an auxiliary OLS regression using the same predictor set. Linearity in the logit for continuous predictors was checked with Box–Tidwell transformations; no assumption violations were retained in the final model. Sample size sufficiency was verified against an events-per-variable (EPV) ≥ 10 criterion. Analyses were performed in SPSS v26. NO missing data were observed; therefore, no imputation or deletion procedures were required.
Results
The Completion rate was 95% as 5% refused to give consent for their data to be used. The total number of completed responses was 788, which includes 383 who fled Palestine (the fled group), and 405 who remain in Gaza (the non-fled group). The overall mean age of respondents was 38 years (SD = 14.57). The mean age of the non-fled group was 46.82 (SD = 11.50), and the fled group was 28.88 (SD = 11.48) (p = 0.00). Men made up more than half of the respondents (53.81%), and the percentage of men in the non-fled group was significantly greater (73.83%) (p = 0.00) than in the fled group (32.64%). The majority of participants (62.20%) were married, with the non-fled group having a considerably higher percentage of married people (87.65%) (p = 0.00) than the fled group (35.24%). A bachelor’s degree was held by the vast majority of participants (89.50%), with the non-fled group having a considerably higher proportion of bachelor’s degrees (92.10%) (p = 0.02) than the fled group (86.68%). The majority of respondents reported displacement within Gaza (84.52%), with a comparable proportion observed among the non-fled group (84.7%; p < 0.05). In addition, 48.6% of participants reported loss of employment as a direct consequence of the war, and 43.4% reported the death of a family member. Both outcomes showed no statistically significant differences between the groups. The sample characteristics are summarised in Table 1.
Depression symptomatology and severity
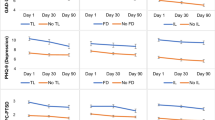
Based on the PHQ-9, a substantial proportion of participants reported experiencing depressive symptoms nearly every day: diminished interest or pleasure in activities (Q1) was reported by 46.3% of respondents; feelings of being down, depressed, or hopeless (Q2) by 49%; sleep disturbances (Q3) by 47.3%; fatigue or low energy (Q4) by 50.9%; appetite changes (Q5) by 38.2%; feelings of worthlessness or guilt (Q6) by 32%; concentration difficulties (Q7) by 39.7%; psychomotor agitation or retardation (Q8) by 23.9%; and suicidal ideation (Q9) by 20.7%. Figure 1 presents a comprehensive overview of the distribution of responses across PHQ-9 items.
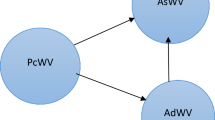
Overall, 82% of participants met criteria for moderate-to-severe depression, of whom 37% exhibited severe depressive symptoms. Stratification by fleeing status revealed that 72.6% of the non-fled group experienced moderate-to-severe depression, including 24.9% with severe depression. Conversely, 90.9% of the fled group met criteria for moderate-to-severe depression, with nearly half (49.9%) classified as severe (Fig. 2).
Logistic regression analysis
A binary logistic regression model was implemented to identify independent predictors of moderate-to-severe depression. Fleeing status emerged as a significant determinant: participants in the fled group were markedly more likely to experience moderate-to-severe depression relative to the non-fled group (crude OR 0.27; 95% CI 0.18–0.40, p < 0.001; adjusted OR 0.45; 95% CI 0.26–0.78, p = 0.004). Younger age was associated with increased odds of moderate-to-severe depression (crude OR 0.96; 95% CI 0.95–0.97, p < 0.001; adjusted OR 0.96; 95% CI 0.94–0.98, p < 0.001). Female participants demonstrated significantly higher crude odds of moderate-to-severe depression compared to males (crude OR 2.70; 95% CI 1.82–4.01, p = 0.001), though the association was not significant after adjustment.
Educational attainment showed a complex pattern: individuals with college-level education or above had lower crude odds of moderate-to-severe depression compared with secondary education (crude OR 0.38; 95% CI 0.16–0.89, p = 0.027), although the adjusted association was non-significant. Surprisingly, participants with only primary education also exhibited significantly reduced odds relative to secondary education (crude OR 0.16; 95% CI 0.04–0.70, p = 0.015; adjusted OR 0.16; 95% CI 0.03–0.78, p = 0.024).
Displacement status was a salient predictor: participants not displaced within Gaza exhibited lower crude odds of moderate-to-severe depression than those displaced internally (crude OR 0.56; 95% CI 0.31–1.001, p = 0.05). Conversely, participants displaced outside Palestine showed significantly higher crude odds relative to internal displacement (crude OR 3.20; 95% CI 1.14–8.10, p = 0.027); however, these associations were not significant in the adjusted model. Bereavement due to the loss of a family member was independently associated with increased odds of moderate-to-severe depression (crude OR 0.65; 95% CI 0.45–0.94, p = 0.02; adjusted OR 0.56; 95% CI 0.37–0.83, p = 0.004) (Table 2).
The model demonstrated adequate calibration and predictive ability: the Hosmer–Lemeshow goodness-of-fit test was non-significant (p = 0.64), percentage accuracy in classification (PAC) was 81.8%, and Nagelkerke R2 was 0.16. Interaction terms between fleeing status and all other predictors were tested individually; none achieved statistical significance, indicating no evidence of effect modification. Consequently, the identified risk factors for moderate-to-severe depression operate similarly across both fled and non-fled populations in this context.

(a) PHQ-9 answers of the non- fled group (N = 405). (b) PHQ-9 answers of the fled group (N = 383). PHQ-9: Patient Health Questionnaire-9. Q1:Little interest or pleasure in doing things. Q2:Feeling down, depressed, or hopeless. Q3:Trouble falling or staying asleep, or sleeping too much. Q4:Feeling tired or having little energy. Q5:Poor appetite or overeating. Q6: Feeling bad about yourself – or that you are a failure or have let yourself or your family down. Q7:Trouble concentrating on things, such as reading the newspaper or watching television. Q8:Moving or speaking so slowly that other people could have noticed? Or the opposite – being so fidgety or restless that you have been moving around a lot more than usual. Q9:Thoughts that you would be better off dead or of hurting yourself in some way.

(a) Severity of depression among the fled group (N = 383). (b) Severity of depression among the non-fled group (N = 405).
Discussion
This study provides critical insights into the psychological burden imposed by the ongoing conflict in Gaza, highlighting a stark contrast in depression prevalence between individuals who fled Palestine and those who remained. Overall, the findings reveal an alarmingly high prevalence of moderate-to-severe depression (82%) among participants, with the highest rates observed in the fled group (90.86%) compared to the non-fled group (72.59%). Notably, nearly half of the fled participants (49.87%) experience severe depression, emphasizing the profound psychological consequences of forced displacement and migration.
Key risk factors associated with moderate-to-severe depression included younger age, female gender, lower educational attainment, forced migration, and bereavement. These results are striking when compared with global data: a meta-analysis of 57 studies encompassing 64,596 individuals from conflict zones worldwide reported an average depression prevalence of 25.6%8. The discrepancy underscores the extreme psychological toll of the Gaza conflict, particularly among displaced populations.
Logistic regression analyses confirmed that fleeing the conflict zone significantly increased the likelihood of developing moderate-to-severe depression, even after controlling for potential confounders. This finding aligns with extant literature indicating that forced displacement, exposure to unfamiliar environments, and disruption of social support systems are consistently associated with adverse mental health outcomes18,19,20. Interestingly, interaction analyses revealed no statistically significant effect modification between group status (fled vs. non-fled) and each predictor, suggesting that depression risk factors operate similarly across both populations.
The observation that individuals who fled Gaza reported higher levels of possible depression than those who remained challenges conventional assumptions that continuous exposure to conflict correlates with greater psychological distress. Several methodological factors may partially explain this pattern, including sampling bias, self-reported location, and unmeasured confounders such as socioeconomic status or prior mental health conditions. However, similar findings have been documented in displacement research, where relocation often introduces new stressors—loss of social networks, uncertainty about legal status, financial insecurity, and limited access to healthcare—that compound trauma rather than alleviate it19,20. Studies on refugees and internally displaced populations consistently show that post-displacement stressors can be as detrimental as direct exposure to violence, contributing to persistent depression and PTSD21,22. Furthermore, displacement disrupts cultural continuity and community support systems, which are critical for resilience in conflict settings19. These contextual factors suggest that fleeing a war zone does not guarantee psychological relief; instead, it may create a complex interplay of trauma and adaptation challenges. Future research should examine these dynamics using longitudinal designs and control for potential confounders to better understand the mental health trajectories of displaced populations.
The PHQ-9 data further reveal a deeply concerning mental health profile. Fatigue (Q4) and depressed mood (Q2) affected over 50% of respondents nearly every day, and 20.70% reported experiencing suicidal ideation (Q9) on a nearly daily basis. These figures are comparable to those observed in other conflict-affected populations: a 2022 study among internally displaced persons in Ethiopia reported a suicidal ideation prevalence of 22.4%, while a meta-analysis of refugees estimated a prevalence of approximately 20.5% (ranging from 10 to 32%)23,24. These similarities underscore the high psychological burden of the Gaza conflict and confirm that displaced and war-affected communities worldwide experience comparable levels of distress.
Age emerged as a significant predictor of depression, with younger individuals at higher risk. This finding aligns with developmental trauma theory, which posits that early-life exposure to stressors disrupts neurobiological and psychosocial development, increasing vulnerability to emotional disorders25. Younger individuals may face heightened risks due to disrupted education, interrupted socialization, limited coping resources, and exposure to violence. Evidence from war-affected youth in Uganda similarly demonstrates strong associations between exposure to violence, bereavement, sexual abuse, and heightened rates of depression and anxiety26, suggesting that early-life trauma has enduring effects on emotional and cognitive development.
Gender differences were observed, with females displaying higher crude odds of depression. Although the association lost significance after adjustment, these findings are consistent with research among Syrian refugees in Lebanon and Rohingya refugees in Bangladesh, where women are disproportionately affected by depression due to gender-based violence, caregiving burdens, and social instability27,28,29. In conflict and post-conflict contexts, women often assume primary responsibilities for maintaining family cohesion and managing household stability under extreme conditions30,31. These socially and culturally embedded roles contribute to psychological distress, though intersectional factors—such as education level and family structure—appear to mediate the impact of gender alone on mental health outcomes23,32. This highlights the need for interventions that are sensitive to the interplay between gender and other social determinants in shaping war-related psychological outcomes.
The relationship between education and depression was complex. While higher education was initially associated with lower crude odds of depression, this effect was not retained in adjusted models. This suggests that educational attainment alone may not suffice as a protective factor in high-trauma environments, where structural disruptions and emotional distress can outweigh individual resources30. Interestingly, individuals with only primary education exhibited lower odds of depression compared to those with secondary education, possibly reflecting differences in expectations, resilience, or social roles, a finding that warrants further investigation18.
Bereavement emerged as a particularly salient risk factor. The loss of a family member due to war significantly increased depression risk, consistent with literature on trauma and prolonged grief. Bereavement disrupts social and familial structures, often resulting in prolonged grief, emotional instability, and increased vulnerability to depression8,33,34. In conflict-affected populations, sudden and violent loss is compounded by lack of closure and ongoing insecurity, intensifying psychological suffering. Research in Kosovo demonstrated that widowed lone mothers exhibited high rates of psychiatric disorders, including major depressive disorder (71%), PTSD (82%), and prolonged grief disorder (69%)35. The World Health Organization estimates that one in four Ukrainians is similarly at risk for war-related mental illnesses23. These findings emphasize the urgent need for targeted mental health interventions addressing trauma and grief in war survivors.
Despite the robust and theory-informed findings, this study has several limitations. Depression prevalence estimates are based solely on self-reported symptom screening using the PHQ-9, a validated screening instrument, without professional assessment or diagnostic confirmation. The cross-sectional design precludes causal inference, and self-report measures may be subject to recall and reporting biases. Additionally, respondents’ locations were based solely on self-report without independent verification, which introduces potential misclassification bias. The reliance on voluntary online participation likely attracted individuals who are more educated, digitally connected, and resilient than the general population, resulting in sampling bias and limiting the generalizability of the findings. While the PHQ-9 is widely validated, it may not fully capture culturally specific expressions of distress20. However, direct follow-up or referral for participants who screened positive was not feasible due to the study’s online and anonymous design. At the end of the questionnaire, participants were advised to seek psychological health support if they experienced severe distress or suicidal thoughts. Moreover, direct follow-up or referral for participants who screened positive was not feasible due to the study’s online and anonymous design. Future research should incorporate longitudinal designs and qualitative methods to better understand the lived experiences of war survivors, enabling the development of interventions that are both evidence-based and contextually relevant.
Conclusion
Overall, this study highlights a high prevalence of depression among Gaza war survivors, with significantly greater severity observed among those who fled the conflict zone. Key risk factors—such as younger age, female gender, forced displacement, lower educational attainment, and bereavement—were consistently associated with depression across both groups, underscoring the pervasive impact of war trauma. These findings reinforce theoretical models of trauma and displacement, which emphasize that exposure to violence, disruption of social and familial networks, and loss of stability have enduring psychological consequences21,22,25. Importantly, the similar mechanisms of risk across fled and non-fled individuals suggest that mental health interventions must address not only immediate exposure to conflict, but also the long-term ecological and social disruptions that perpetuate distress. From a global policy perspective, these results underscore the urgent need for comprehensive, inclusive, and sustained mental health support programs that target al.l war survivors, irrespective of their geographic location, and that are sensitive to age, gender, and sociocultural context. By combining evidence-based clinical strategies with community-informed interventions, policymakers and practitioners can better mitigate the enduring psychological impact of war and displacement on affected populations.
Data availability
The datasets generated during and/or analysed during the current study are available from the corresponding author on reasonable request.
References
Zughbur, M. R. et al. Prevalence and correlates of anxiety, depression, and symptoms of trauma among Palestinian adults in Gaza after a year of war: a cross-sectional study. Confl. Health. 19 (1), 43. https://doi.org/10.1186/s13031-025-00681-1 (2025).
OCHAOPT. Reported impact snapshot | Gaza strip (29 October 2024). (2024).
Aldabbour, B. et al. The psychological toll of war and forced displacement in gaza: A study on anxiety, PTSD, and depression. Chronic Stress (Thousand Oaks). 9, 24705470251334943. https://doi.org/10.1177/24705470251334943 (2025).
UNICEF. Children in Gaza need life-saving support: No safe place for children as humanitarian crisis deepens. New York: UNICEF; n.d. https://www.unicef.org/emergencies/children-gaza-need-lifesaving-support
Charlson, F. et al. New WHO prevalence estimates of mental disorders in conflict settings: a systematic review and meta-analysis. Lancet 394 (10194), 240–248. https://doi.org/10.1016/S0140-6736(19)30934-1 (2019).
Farajalla, F. et al. Prevalence of violence and quality of life among nursing students during the 7th of October war in Palestine. BMC Nurs. 24, 851. https://doi.org/10.1186/s12912-025-03544-5 (2025).
Qtait, M. et al. Impact of the October 7 Gaza war on post-traumatic stress symptoms and quality of life in Palestinian nursing. Sci. Rep. 15, 34575. https://doi.org/10.1038/s41598-025-18039-1 (2025).
Lim, I. C. Z. Y. et al. Prevalence of depression, anxiety and post-traumatic stress in war- and conflict-afflicted areas: A meta-analysis. Front. Psychiatry. 13, 978703. https://doi.org/10.3389/fpsyt.2022.978703 (2022).
Albelbeisi, A. H., Hajizadeh, A., Al-Zeer, A. M., Saeidpour, J. & Kakemam, E. Prevalence and associated factors of mental health disorders among internally displaced persons in Gaza. East. Mediterr. Health J. 31 (2), 81–88. https://doi.org/10.26719/2025.31.2.81 (2025).
Gammoh, O. et al. The prevalence and correlates of Depression, Anxiety, and insomnia among camp residing Palestinian women migrants during the outbreak of the war on gaza: A Cross-Sectional study from Jordan. Med. (Kaunas). 60 (8), 1228. https://doi.org/10.3390/medicina60081228 (2024).
Tawfiles, D. & Zughbur, M. R. The invisible health crisis of gaza’s externally displaced. Lancet 406 (10502), 439–440. https://doi.org/10.1016/S0140-6736(25)01483-7 (2025).
Barron, I., McInnes, J. & Abdallah, G. Intergenerational trauma framework for programme efficacy studies: child trauma recovery in occupied Palestine. Crit. Radic Soc. Work. 4 (2), 217–230. https://doi.org/10.1332/204986016X14601003012367 (2016).
Ahmed, S. H. et al. Prevalence of post-traumatic stress disorder and depressive symptoms among civilians residing in armed conflict-affected regions: a systematic review and meta-analysis. Gen. Psychiatry. 37, e101438 (2024).
McLaughlin, K. A., Peverill, M., Gold, A. L., Alves, S. & Sheridan, M. A. Child maltreatment and neural systems underlying emotion regulation. J. Am. Acad. Child. Adolesc. Psychiatry. 54 (9), 753–762. https://doi.org/10.1016/j.jaac.2015.06.010 (2015).
Sawaya, H., Atoui, M., Hamadeh, A., Zeinoun, P. & Nahas, Z. Adaptation and initial validation of the patient health questionnaire-9 (PHQ-9) and the generalized anxiety disorder-7 questionnaire (GAD-7) in an Arabic speaking Lebanese psychiatric outpatient sample. Psychiatry Res. 239, 245–252. https://doi.org/10.1016/j.psychres.2016.03.030 (2016).
World Medical Association. World medical association declaration of helsinki: ethical principles for medical research involving human subjects. JAMA 310 (20), 2191–2194. https://doi.org/10.1001/jama.2013.281053 (2013).
IBM. How to cite IBM SPSS Statistics or earlier versions of SPSS. (2014). http://www-01.ibm.com/support/docview.wss?uid=swg21476197
Kim, D. J., Mitchell, D. & Wylie, G. Forced displacement and peacebuilding. In Peace and Conflict in a Changing World. https://doi.org/10.1007/978-3-031-66641-4_8 (Palgrave Macmillan, 2024).
Ehrkamp, P. Geographies of migration I. Prog. Hum. Geogr. 41 (6), 813–822. https://doi.org/10.1177/0309132516663061 (2016).
Ajele, K. W. & Idemudia, E. S. Charting the course of depression care: a meta-analysis of reliability generalization of the patient health questionnaire (PHQ-9) as the measure. Discov Ment Health. 5, 50. https://doi.org/10.1007/s44192-025-00181-x (2025).
Pinchuk, I., Yachnik, Y., Goto, R. & Skokauskas, N. Mental health services during the war in ukraine: 2-years follow up study. Int. J. Ment. Health Syst. 19 (1), 11. https://doi.org/10.1186/s13033-025-00667-9 (2025).
Amone-P’Olak, K., Ovuga, E., Croudace, T. J., Jones, P. B. & Abbott, R. The influence of different types of war experiences on depression and anxiety in a Ugandan cohort of war-affected youth: the WAYS study. Soc. Psychiatry Psychiatr. Epidemiol. 49 (11), 1783–1792. https://doi.org/10.1007/s00127-014-0873-5 (2014).
Haase, E., Schönfelder, A., Nesterko, Y. & Glaesmer, H. Prevalence of suicidal ideation and suicide attempts among refugees: a meta-analysis. BMC Public. Health. 22 (1), 635. https://doi.org/10.1186/s12889-022-13029-8 (2022).
Tadesse, G., Gashaw, F., Zeleke, T. A., Fentahun, S. & Yitayih, S. Prevalence and factors associated with suicidal ideation and attempts among war-affected internally displaced people in Northwest Ethiopia, 2022. BJPsych Open. 10 (4), e132. https://doi.org/10.1192/bjo.2024.71 (2024).
McMullen, J. D., O’Callaghan, P. S., Richards, J. A., Eakin, J. G. & Rafferty, H. Screening for traumatic exposure and psychological distress among war-affected adolescents in post-conflict Northern Uganda. Soc. Psychiatry Psychiatr. Epidemiol. 47 (9), 1489–1498. https://doi.org/10.1007/s00127-011-0454-9 (2012).
Griffiths, M. Affect and displacement. In The Handbook of Displacement (eds Adey, P. et al.) https://doi.org/10.1007/978-3-030-47178-1_7 (Palgrave Macmillan, 2020).
Khan, S. & Haque, S. Trauma, mental health, and everyday functioning among Rohingya refugee people living in short- and long-term resettlements. Soc. Psychiatry Psychiatr. Epidemiol. 56, 497–512. https://doi.org/10.1007/s00127-020-01962-1 (2021).
Niolu, C., Bianciardi, E. & Siracusano, A. Gender inequality and women mental health: where do we stand?. In Social Determinants of Mental Health. Sustainable Development Goals Series (eds Fiorillo, A. & De Giorgi, S.) https://doi.org/10.1007/978-3-031-70165-8_7 (Springer, 2024).
Bürgin, D., Anagnostopoulos, D., Board and Policy Division of ESCAP. & et al. Impact of war and forced displacement on children’s mental health—multilevel, needs-oriented, and trauma-informed approaches. Eur. Child. Adolesc. Psychiatry. 31, 845–853. https://doi.org/10.1007/s00787-022-01974-z (2022).
Niaz, U. & Tariq, Q. Challenges in women’s mental health: care in conflict and Post-Conflict situations. In Mental Health and Illness of Women. Mental Health and Illness Worldwide (eds Chandra, P., Herrman, H., Fisher, J. & Riecher-Rössler, A.) https://doi.org/10.1007/978-981-10-2369-9_4 (Springer, 2020).
Leighton, C. & Martínez, C. Gender and depression: Women, transgender, and gender nonconforming depression. In Etiopathogenic Theories and Models in Depression. Depression and Personality (eds Jiménez, J. P., Botto, A. & Fonagy, P.) https://doi.org/10.1007/978-3-030-77329-8_15 (Springer, 2021).
Morina, N. & Emmelkamp, P. M. G. Mental health outcomes of widowed and married mothers after war. Br. J. Psychiatry. 200 (2), 158–159. https://doi.org/10.1192/bjp.bp.111.093609 (2011).
Rozanov, V. et al. Mental health consequences of war conflicts. In Advances in Psychiatry (eds Javed, A. & Fountoulakis, K.) https://doi.org/10.1007/978-3-319-70554-5_17 (Springer, 2019).
Santiago, P. N., Oravec, G. J. & Ursano, R. J. War sleep and PTSD war, and war-related trauma: an overview. In Sleep and Combat-Related Post Traumatic Stress Disorder (eds Vermetten, E., Germain, A. & Neylan, T.) https://doi.org/10.1007/978-1-4939-7148-0_1 (Springer, 2018).
Pinchuk, I. et al. Mental health services during the war in ukraine: 2-years follow up study. Int. J. Ment. Health Syst. 19, 11. https://doi.org/10.1186/s13033-025-00667-9 (2025).
Acknowledgements
We thank Mohammed W. Zimmo, Khaled Zaqout, Salam Alhabbash, and Abdallah AbuDraz for their contribution to data collection.
Funding
The authors did not receive support from any organization for the submitted work.
Author information
Authors and Affiliations
Contributions
Conceptualization and ideation: M.A., Y.H. Formal analysis: M.A. Review and supervision: G.V., M.A.A., and M.R.Z. All authors contribute to finalizing the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Consent to participate
Informed consent was obtained from all individual participants included in the study.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
AbuZarifa, M., Hamam, Y., Alnajjar, A.Z. et al. A cross-sectional study of screened depression prevalence among Gaza war survivors who fled versus those who remained. Sci Rep 16, 1345 (2026). https://doi.org/10.1038/s41598-025-31757-w
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-31757-w
