
Abstract
Primary central nervous system diffuse large B-cell lymphoma (PCNS-DLBCL) is a rare form of non-Hodgkin lymphoma with a notably poor prognosis. This study aimed to identify new prognostic factors for improved prognostic stratification in PCNS-DLBCL. A total of 85 PCNS-DLBCL cases from three hospitals were retrospectively analyzed. Disease progression within 24 months (POD24) and its risk factors were investigated, and a prognostic model for predicting POD24 was constructed. The median overall survival (mOS) and median progression-free survival (mPFS) for the entire cohort were 48.54 months and 39.09 months, respectively. Survival analysis indicated that age ≥ 65 years (HR = 4.05, P = 0.008), non-responsive disease (HR = 4.43, P = 0.004), and POD24 (HR = 25.22, P = 0.002) were independent poor prognostic factors for OS in PCNS-DLBCL. Further analysis revealed that independent risk factors for POD24 included elevated serum lactate dehydrogenase (LDH) levels (OR = 12.00, P = 0.03), elevated triglycerides (TG, OR = 4.88, P = 0.047), and non-responsive disease (OR = 9.39, P = 0.003). Subsequently, an “LDH-TG-Efficacy (LTE)” prognostic model for PCNS-DLBCL was constructed. The incidence of POD24 was significantly higher in the “LTE” high-risk group (≥ 1 point) compared to the low-risk group (0 points) (81.8% vs. 35%, P < 0.001). The receiver operating characteristic (ROC) curve determined that the area under the curve (AUC) for the “LTE” model was 0.828 (95% CI: 0.7282–0.927), with a sensitivity and specificity of 79.4% and 79.3%, respectively. Additionally, the prognosis of the “LTE” high-risk group was significantly worse. These findings demonstrated that POD24 might serve as an independent prognostic indicator for PCNS-DLBCL, and the “LTE” prognostic index may provide a reference for better identifying populations at risk for POD24.
Similar content being viewed by others


Introduction
Primary central nervous system lymphoma (PCNSL) is a rare subtype of non-Hodgkin lymphoma (NHL), it is usually confined to the brain, eyes, spinal cord or pia mater without other systemic infiltration. Diffuse large B-cell lymphoma (DLBCL) account for about 95% of PCNSL (also known as PCNS-DLBCL). The prognosis of PCNS - DLBCL is far worse than that of systemic DLBCL1. In the past few decades, intruduction of a series of treatment strategies, such as Whole Brain Radiation Therapy (WBRT), combination chemotherapy based on high dose methotrexate (HD-MTX), and autologous Hematopoietic Stem Cell Transplantation (ASCT), have significantly improved the survival of PCNS-DLBCL. However, relapse is common and long - term survival remains poor.
International Extranodal Lymphoma Study Group (IELSG) score2 and Memorial Sloan Kettering Cancer Center (MSKCC) score3 were routine prognostic models for PCNS-DLBCL in clinic. IELSG scoring system based on five factors: age, Eastern Cooperative Oncology Group Performance Status (ECOG) score, serum lactate dehydrogenase (LDH) level, the total protein concentration of cerebrospinal fluid (CSF), and involvement of deep brain structures. The MSKCC scoring system assessed outcomes of PCNS-DLBCL by age and the Karnofsky Performance Status (KPS) score. However, both the IELSG and MSKCC models had insufficient discriminative ability for either progression-free survival (PFS) or overall survival (OS) prognostic in asian population4. Some factors beyond these models were validated to affect survival, such as treatment patterns and response, should also be taken into account. Therefore, new risk stratification systems according to therapy changes over time are still needed to tailor therapeutic approaches in PCNS-DLBCL to date.
Disease progress within 24 months (POD24) is first proposed in follicular lymphoma (FL) and defined as primary - refractory disease (less than partial response), progression, transformation, or relapse within 24 months after diagnosis. Observational studies indicated that patients with FL who experience POD24 of front-line chemoimmunotherapy have unfavorable outcomes5. POD24 was subsequently shown to portend poor outcomes in marginal zone lymphoma (MZL)6. Except for indolent NHLs, early disease progression is also associated with dismal outcomes in aggressive lymphomas7. Previous studies showed event-free survival at 24 months (EFS24) predicted longer survival in DLBCL8. Above all, early disease progression is important prognostic factor in various subtype of NHLs, however, the specific role of POD24 in PCNS-DLBCL is still unclear.
Herein, based on retrospective analysis of PCNS-DLBCL cases from three chinese hospitals, we observed POD24 was a potent prognostic factor in predicting OS and PFS. In addition, we constructed a new prognostic model in order to identify high-risk POD24 population, it might help to optimize stratified treatment and improve long-term survival in the future.
Materials and methods
Study population and enrollment
In this retrospective study, we included cases with newly diagnosed PCNS-DLBCL admission from June 1, 2016 to September 30, 2023, in Huai’an First People’s Hospital, Yancheng No.1 People’s Hospital, and Affiliated Hospital of Xuzhou Medical University. The inclusion criteria were as follows: (1) The final histopathological and immunohistochemical (IHC) stain confirmed DLBCL. (2) Isolated central nervous system involvement, without systemic evidence of disease was confirmed by chest, abdominal and pelvic CT/MRI or systemic PET/CT and bone marrow tests (aspiration and biopsy). The exclusion criteria were as follows: (1) Confirmation of systemic DLBCL by imageological examinations or bone marrow tests. (2) With histories of immunodeficiency disorders (such as HIV infection) or organ transplantation. (3) Untreated cases. All the cases were divided into two groups based on whether they experienced disease progression within 24 months (POD24). 86 cases of central nervous system lymphoma (58 cases of PCNSL and 28 cases of secondary central nervous system lymphoma) from the MSK dataset of the cBioPortal database were used for validation. Informed consent was obtained from all subjects and/or their legal guardian(s). The use of data in this study has been approved by the ethics committee of Huai’an First People’s Hospital, and ethical approval has been obtained from all participating institutions. All methods we used were performed in accordance with the relevant guidelines and regulations.
Treatments and assessments
All the patients were treated with combination chemotherapy regimen based on high-dose methotrexate (HD-MTX). The response to therapies was evaluated by imaging examinations after 3 to 4 courses of induction therapy. IPCG criteria was used for efficacy evaluation. Achieving partial remission (PR) or better in the first-line treatment was defined as responsive disease (which includes PR and complete remission, abbreviated as CR), while the remainder was defined as non-responsive disease (which includes stable disease and progressive disease, abbreviated as SD and PD, respectively).
Prognostic model development
R software was employed to ascertain the weights of key prognostic factors for POD24, based on the results of the logistic regression model. A simplified model was formulated, incorporating the three identified factors. The discriminatory capacity of this simplified model was assessed using a receiver operating characteristic (ROC) curve. A nomogram was subsequently developed to quantify the prognostic value.
Statistical analyses
All patients were followed until January 10, 2024. Variables that adhered to a normal distribution were represented as mean ± standard deviation (x̄ ± s) and tested using the unpaired t-test, whereas non-normally distributed continuous data were represented as median (interquartile range) and tested using the Mann-Whitney U test. The chi-squared test or Fisher’s exact test were used to evaluate relationships between categorical variables. Kaplan-Meier curves (the log-rank test) and Cox proportional hazards regression were used for survival analysis. A binary logistic regression model was constructed to examine the predictors of POD24. The ROC curve was applied to assess the “LTE” prognostic index. SPSS (version 26.0) was used for data analysis. Statistical significance was defined as a P value of 0.05 or less.
Results
Baseline characteristics
In this study, we meticulously reviewed the medical records of 85 patients diagnosed with primary central nervous system diffuse large B-cell lymphoma (PCNS-DLBCL), of which 50.6% were male, with an average age of 58.00 years (interquartile range: 50.00 to 66.00 years). The baseline demographic and clinical features were delineated in Table 1. A preponderance of the patients exhibited a robust Ki-67 proliferation index, with 53.85% demonstrating a rate of 80% or greater. Additionally, 78.6% of patients presented with elevated protein concentrations in the cerebrospinal fluid (CSF). Only a minority of cases, 1.2%, 10.8%, and 17.6% respectively, were complicated by B symptoms, elevated β2-microglobulin (β2M), and elevated lactate dehydrogenase (LDH) levels. The GCB subtype was identified in 32.86% (42/78) of the cohort, while 12.9% were found to be infected with the hepatitis B virus (HBV). The median Karnofsky Performance Status (KPS) score for the entire patient population was 70. Risk stratification according to the Memorial Sloan Kettering Cancer Center (MSKCC) criteria allocated 17.6%, 58.8%, and 23.5% of patients to the low, intermediate, and high-risk categories, respectively. Despite the strong recommendation for stereotactic biopsy as a diagnostic gold standard, the majority of patients (81.2%) underwent surgical resection for diagnosis, with 70.6% exhibiting residual lymphoma within the central nervous system prior to induction therapies. As for the primary treatment approach, 30.86% of patients received Rituximab - containing regimens, For consolidation, 9/82 (10.98%) cases underwent WBRT, autologous hematopoietic stem cell transplantation (ASCT) was employed in 10.6% (9/85) of cases. Following induction therapy, 28.24% of the patients (24 out of 75) experienced refractory disease.
Except for one patient whose PFS event could not be evaluated, the other 84 patients were divided into the POD24 group (n = 50) and the non-POD24 group (n = 34). Compared with the non-POD24 group, the proportion of patients with an elevated serum LDH level at baseline was significantly higher in the POD24 group (24.00% vs. 5.88%, P = 0.04), and the proportion of patients with residual parenchymal central nervous system lymphoma before systemic therapies was significantly higher (82.00% vs. 52.94%, P = 0.01). In the non-POD24 group, the proportion of patients receiving surgical resection was significantly higher (94.12% vs. 72.00%, P = 0.01), and the proportion of patients who failed first-line treatment was significantly lower (12.50% vs. 47.60%, P = 0.002). No statistical differences in other baseline variables between the two groups were observed.
Survival analysis
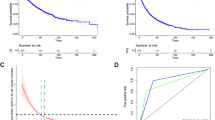
In our study, the median OS (mOS) and the median PFS (mPFS) for the entire cohort were 48.54 and 39.09 months, respectively. The 1-year, 3-year, and 5-year OS rates were 63.5%, 24.7%, and 15.3%, respectively. The 1-year, 3-year, and 5-year PFS rates were 49.4%, 16.5%, and 8.2%, respectively. There was no significant difference in OS among the three risk groups of PCNSL patients stratified by the MSKCC prognostic system. The PFS of patients in the intermediate-risk group was superior to that of patients in the low-risk group, while there was no statistically significant difference in PFS between the other groups (Fig. 1A-B). However, compared to patients who experienced POD24, those who did not (non-POD24) had both better OS in our cohort and the validation cohort (Fig. 1C-D, P < 0.001).

Survival of primary central nervous system diffuse large B-cell lymphoma (PCNS-DLBCL) patients stratified by the Memorial Sloan Kettering Cancer Center (MSKCC) prognostic system and by POD24 status. (A) and (B) Overall survival (OS) and Progression-free survival (PFS) curves for PCNSL patients stratified by the MSKCC prognostic system. (C) and (D) Comparison of OS between non-POD24 and POD24 groups within the study cohort and the validation dataset (the MSK dataset of the cBioPortal database).
To further analyze the effects of various factors on OS in PCNS-DLBCL, we included them in univariate analyses. The results indicated that the following were adverse prognostic factors for OS: triglycerides (TG) > 1.7 mmol/L, hepatitis B surface antigen (HbsAg) positive, non-responsive disease, POD24, and residual parenchymal central nervous system lymphoma before systemic therapies. Subsequently, age, sex, factors with a P value ≤ 0.1 in univariate analyses, elevated LDH levels (a significant difference was observed between the two groups at baseline), first-line therapies without Rituximab (RTX), and ASCT (although our results did not show statistical significance, previous study9 have observed benefits from upfront ASCT in PCNSL) were included in Cox proportional hazards regression analyses. The results revealed that age ≥ 65y (HR = 4.05, P = 0.008), non-responsive disease (HR = 4.43, P = 0.004) and POD24 (HR = 25.22, P = 0.002) were independent inferior prognostic factors for OS in PCNS-DLBCL (Table 2).
Analysis of risk factors for POD24
Since POD24 was a potent inferior prognostic factor for PCNS-DLBCL, further analyses were conducted to identify clinical predictors of early progression. Univariate analyses revealed that elevated LDH and TG at baseline, not undergoing excision of the intracranial tumor, residual parenchymal central nervous system lymphoma, and non-responsive diseases were risk factors for POD24. Gender, age, all significant factors identified by univariate analyses, KPS scores, regimens without RTX, and ASCT were further included in the multivariate analysis. The results revealed that elevated LDH (OR = 12.00, P = 0.03) and TG (OR = 4.88, P = 0.047) at baseline, and non-responsive diseases (OR = 9.39, P = 0.003) were independent risk factors for POD24 (as shown in Table 3).
Construction of POD24 risk prediction model
Furthermore, this study developed a risk prediction model named “LDH-TG-Efficacy” (“LTE” for short) for predicting the occurrence of POD24 in PCNSL patients, based on the aforementioned multivariate logistic regression model. The nomogram, illustrated in Fig. 2, encompasses three variables: LDH, TG, and Efficacy, each assigned corresponding weights (elevated TG assigned 64 points, elevated LDH assigned 100 points, and non-responsive disease assigned 90 points). By summing the scores of each variable, the total score for a patient can be obtained, which corresponds to the probability of POD24. The ROC curve analysis determined that the area under the curve (AUC) for the “LTE” model was 0.828 (95% CI: 0.7282–0.927, Fig. 3A), with a sensitivity and specificity of 79.4% and 79.3%, respectively, indicating its good predictive performance. The ROC curve identified the optimal cutoff value for the model as 0.436, and all patients were categorized into a low-risk group (LR, predicted probability < 0.436) and a high-risk group (HR, predicted probability ≥ 0.436) based on whether their values exceeded this cutoff. Patients in the HR group exhibited a significantly higher risk of POD24 compared to those in the LR group (81.8% vs. 23.3%, P < 0.001, Table 4). Additionally, the prognosis for the “LTE” high-risk group was significantly worse (P < 0.001, Fig. 3B-C).

The “LTE” POD24 predictive model for PCNS-DLBCL was constructed through a multivariate logistic regression analysis which included TG, LDH, and first-line efficacy.

(A) The ROC curve of the “LTE” POD24 predictive model. (B) and (C) Kaplan-Meier plot comparing OS and PFS between the “LTE” LR and HR groups.
Survival analysis of OS in POD12, POD12-24, and Non-POD groups
To further analyze whether there were differences in the prognosis of PCNSL patients who progressed within 12 months and those who progressed between 12 and 24 months, we further divided the patients into three groups: POD12, POD12-24, and Non-POD (no progression within 24 months). The median OS for these groups was 8.2 months, 33.77 months, and undefined, respectively. The OS of the Non-POD group was significantly better than that of the POD12-24 group, and the OS of the POD12-24 group was also better than that of the POD12 group, with P-values of 0.01 and 0.0007, respectively (Fig. 4A). In the cBioPortal validation dataset, the median OS for POD12, POD12-24, and Non-POD patients was 4.333 months, 18.48 months, and undefined, respectively. The OS of the Non-POD group was significantly better than that of the POD12-24 group and the POD12 group (both P-values < 0.0001). However, there was no statistically significant difference in OS between the POD12-24 group and the POD12 group (P = 0.44, Fig. 4B).

Comparison of OS among PCNS-DLBCL patients categorized into non-POD24 (Disease does not progress within 24 months), POD12-24 (Disease progression between 12 and 24 months), and POD12 (Disease progress within 12 months) groups using Kaplan-Meier analysis. (A) Our cohort. (B) The validation dataset (the MSK dataset of the cBioPortal database).
Discussion
In this collaborative retrospective study, conducted across three Chinese institutions, we elucidated that the median age for the diagnosis of PCNS-DLBCL was 58 years. Our findings revealed a male to female ratio akin to that observed in the SEER database, which encompasses over 5000 cases of PCNSL. However, our patient cohort was diagnosed at a younger age, contrasting with the SEER database median diagnosis age of 63.1 ± 14.9 years10. Consistent with prior research, the predominant subtype of PCNSL in our study was non-GCB, and baseline LDH levels were generally unremarkable11. Furthermore, In non-GCB subtype PCNSL patients, high Ki-67 index was an adverse independent prognostic marker12. Regarding the induction therapy, all patients in our cohort were administered HD-MTX, with 30.86% of the patients also receiving Rituximab. As one of the limited agents capable of traversing the blood-brain barrier (BBB), HD-MTX (3–8 mg/m²) and HD-MTX-based combination therapies have emerged as the standard induction protocols for patients newly diagnosed with PCNSL13. In the era of HD-MTX, the median survival for PCNSL in the United States has significantly improved, rising from 12.5 months in the 1970s to 26 months in the 2010s14. Consistent with prior reports15, our findings revealed a mPFS of 39.1 months and a mOS of 48.54 months, respectively, with a 12-month overall survival rate of 63.5%.
Although recent advancements in radiotherapy and chemotherapy have led to improved efficacy and survival rates for patients with PCNS-DLBCL compared to a decade ago, these improvements are often not sustained, with up to 50% of cases eventually recurring16. The prognosis for recurrent/refractory PCNSL is exceptionally poor, with a median survival time of approximately 2 months17. Therefore, effectively predicting lymphoma recurrence remains a critical challenge in the management of PCNS-DLBCL. The conventional Ann Arbor staging system is not applicable to PCNSL, and to date, no specific staging system for PCNSL has been established. Clinically, the prognostic assessment frameworks proposed by the IELSG and the MSKCC are predominantly utilized. Nevertheless, these pre-rituximab-era systems, which have been in use for two decades or more, exhibit considerable limitations in their clinical application. Previous studies have indicated that the traditional IELSG score has limited discriminatory value in stratifying PCNSL within the Chinese population4. In our cohort, the MSKCC scoring system also failed to effectively differentiate the prognostic outcomes for PCNSL patients, underscoring the necessity for a more instructive prognostic stratification system to guide the management of PCNSL in this new era of therapeutic advancements.
Our univariate analysis revealed that TG > 1.7 mmol/L, HbsAg positivity, residual parenchymal central nervous system lymphoma, non-responsive disease, and POD24 were adverse prognostic factors for OS in patients with PCNSL. Multivariate analysis identified non-responsive disease, age, and POD24 as independent adverse prognostic factors for OS. In recent years, the incidence of PCNSL has increased among the elderly population, with patients over 60 years accounting for more than 50% of all PCNSL cases. Consistent with our findings, age has been established as an independent adverse prognostic factor for PCNSL, potentially due to the diminished organ function and reduced tolerance to chemotherapy in older patients compared to younger ones. Patients over 50 years with a KPS < 70 have the poorest prognosis, with a median survival of only 1.1 years18. Therefore, as a unique subgroup of PCNSL, elderly patients require more effective and less toxic treatment regimens.
In our cohort, 11 patients (12.9%) tested positive for HbsAg. A study from the affiliated cancer hospital of Fudan university, involving 199 PCNSL patients, reported an HBV infection prevalence of 16.1% in PCNSL, higher than that in a control group based on the national population19. A retrospective study found that 127 of systemic DLBCL patients (30.2%) were HbsAg positive, and HbsAg-positive DLBCL exhibited distinct clinicopathological features (such as more advanced disease). Additionally, in the context of antiviral prophylaxis, HBV infection was not an independent prognostic factor for OS in DLBCL20. In line with these findings, our univariate analysis suggested that HbsAg positivity might be an adverse prognostic factor for OS, however, it was not an independent prognostic factor in PCNS-DLBCL. In summary, although the prevalence of HBV infection is lower in PCNS-DLBCL than in systemic DLBCL, it remains higher than in the general population. The role of HBV infection in the pathogenesis of PCNS-DLBCL warrants further investigation.
In our PCNS-DLBCL cohort, a significant proportion of patients in the non-POD24 group underwent surgical resection. Although multivariate analysis showed that surgical resection and residual parenchymal central nervous system lymphoma were not independent prognostic factors for OS, univariate analysis indicated that residual parenchymal central nervous system lymphoma was an adverse prognostic factor for OS in PCNSL. Given that 44% of PCNSL cases are multifocal, most tumors cannot be completely resected surgically. Considering previous studies indicating that surgical resection offers no survival benefit for PCNSL and significantly increases the risk of postoperative neurological deficits and other complications, and that PCNSL is highly sensitive to chemotherapy and radiotherapy, surgical resection is not a standard treatment for PCNSL13,21,22. Current consensus recommends surgery only for emergency decompression of brain herniation or treatment of a single superficial tumor23,24. Despite the fact that stereotactic biopsy has largely replaced surgical resection for the diagnosis of PCNSL, a considerable proportion of patients still receive a diagnosis through surgical resection. In our study, 81.2% of patients underwent surgical resection, which, in addition to providing a diagnosis, also offered more rapid reduction of intracranial pressure. A retrospective study based on the SEER database showed that PCNSL patients who underwent surgical resection had better overall survival, especially those with complete resection, compared to those who did not undergo surgical resection10. Similarly, Schellekes et al. found that patients with a single lesion of PCNSL might benefit from resection in terms of survival compared to those who received only diagnostic biopsy23. Furthermore, with advancements in neurosurgical techniques, an increasing number of studies have shown that craniotomy is safe for patients25,26. These findings suggest that complete tumor resection might offer greater survival benefits for PCNSL if more neurological function can be preserved. Our results indicated that surgical tumor resection was not a favorable factor for OS, considering that 70.6% of patients had residual central nervous system lymphoma before systemic treatment. It is plausible that the lack of complete tumor resection limited the survival benefit after surgery. The therapeutic and prognostic significance of surgery in PCNSL requires further prospective studies to evaluate.
Currently, although the NCCN guidelines recommend HD-MTX +/- RTX as the first-line induction therapy for PCNSL, followed by ASCT consolidation, the clinical benefit of RTX remains uncertain. In a recent meta-analysis including 13 studies (2 randomized controlled trials and 11 retrospective cohort studies)27, the results showed that PCNSL patients receiving RTX treatment had significantly better objective response rate (ORR), complete response (CR) rate, and PFS than those who did not receive RTX. However, there was no statistically significant difference in OS (P = 0.06). The phase III large randomized controlled clinical trial HOVON 105/ALLG NHL 24 showed that the addition of RTX to the treatment regimen for newly diagnosed PCNSL did not improve efficacy28. Similarly, in this study, multivariate analysis showed that induction therapy without RTX was not an independent prognostic factor for survival. Furthermore, our study indicated that WBRT and ASCT were not independent predictors of OS in PCNSL, which might be due to the bias caused by the small number of patients who received ASCT or WBRT consolidation. A recent study reported an 8-year OS of 69% with the application of ASCT as a first-line consolidation regimen for newly diagnosed PCNSL, along with a significantly lower risk of relapse29. Two randomized controlled trials (IELSG32 study30 and ANOCEF-GOELAMS study31) compared the efficacy of WBRT or ASCT as consolidations in patients who achieved remission after induction therapy. The results showed that both therapies achieved good disease control, with the ANOCEF-GOELAMS study showing a certain advantage of PFS in the ASCT group. Both studies observed more pronounced long-term neurological adverse effects in the WBRT group. To mitigate the cognitive impairment associated with WBRT, recent studies have focused on reduced-dose WBRT (rdWBRT) as consolidation therapy for PCNSL, with results showing good PFS and OS rates. rdWBRT combined with HD-MTX showed no statistically significant difference in OS and PFS compared to high-dose WBRT and suggested that patients under 60 years might benefit from rdWBRT18. A recent study showed that 5 years of HD-MTX maintenance was not inferior to ASCT consolidation32. Additionally, the emergence of new drugs (such as BTK inhibitors, bispecific antibodies, CAR-T cells, and IMiDs) will further challenge the authoritative status of ASCT in PCNSL18.
Our results indicated that POD24 was an independent adverse prognostic factor for OS. Previous studies have shown that POD24 is not only an adverse prognostic factor for indolent NHLs (such as follicular lymphoma and marginal zone lymphoma)5,6 but also for aggressive NHLs7,8. Current guidelines recommend classifying relapsed/refractory systemic DLBCL into two categories: patients with progression within 12 months are advised to receive second-line CAR-T therapy, while those with relapse/progression after 12 months consider second-line salvage chemotherapy followed by ASCT consolidation. Therefore, the prognostic and therapeutic significance of POD12 in systemic DLBCL patients is well established. Previous studies have shown that EFS24 is an important prognostic factor for systemic DLBCL8. However, the prognostic and therapeutic significance of progression between 12 and 24 months (POD12-24) and beyond 24 months in systemic DLBCL and PCNSL remains unclear. Our results indicated that not only was POD24 an adverse prognostic factor for OS in PCNSL, but patients with POD12-24 might also differ from those with POD12 and beyond 24 months, warranting treatment as a unique subgroup in clinical practice. However, the results of the validation dataset differed from our study, showing no statistically significant difference in survival between the two subgroups of POD12 and POD12-24. This discrepancy might be due to the following two factors: (1) our patients received HD-MTX-based regimens, while patients in the validation dataset were treated with BTK inhibitor ibrutinib, which might overcome the adverse prognosis associated with short-term progression; (2) the validation dataset included a small number of patients with secondary central nervous system diffuse large B-cell lymphoma, which might have affected the results. However, POD24 was also an adverse prognostic factor for OS in the validation dataset. In summary, the prognostic significance of POD24 and POD12-24 in PCNSL needs to be further clarified by large-sample prospective clinical trials. Additionally, our results indicated that elevated LDH, elevated TG, and non-responsive disease were independent adverse prognostic factors for POD24. Previous studies have shown that lipid metabolism abnormalities exist in various tumors. In systemic DLBCL, univariate analysis showed that serum TG levels was associated with OS and PFS, and multivariate analysis confirmed the adverse effect of TG on PFS (P = 0.013)33. In our cohort, elevated TG was an adverse prognostic factor for OS in univariate analysis and was closely related to POD24. Moreover, a higher proportion of cases with elevated LDH was observed in the POD24 group. Previous studies have shown that serum LDH levels do not have a prognostic effect in PCNSL cases under 70 years34. Similarly, in our cohort, serum LDH levels were not an adverse prognostic factor for OS in PCNSL. It was reported that 10–15% of PCNSL were refractory to initial treatment18. Our results indicated that non-responsive disease was an independent adverse prognostic factor for OS in PCNS-DLBCL. This is consistent with previous studies, in PCNSL who treated with HD - MTX - based induction regimens, after a median follow-up of 27.5 months, there was no statistically significant difference in OS and PFS between patients with interim positive and negative diseases assessed by PET - CT. However, at the end of treatment, PET - CT - negative patients had significantly longer PFS than PET - CT - positive patients (P = 0.892)35. Moreover, multivariate analysis found that incomplete remission before high-dose therapy/ASCT was an independent adverse prognostic factor for OS18. Based on these above three factors, we constructed the POD24 prediction model “LTE”. The risk of POD24 was significantly higher in the high-risk “LTE” group compared to the low-risk group. The ROC curve determined the AUC for POD24 prediction to be 0.828, with a sensitivity and specificity of 79.4% and 79.3%, respectively. This model might helps to identify high-risk groups for POD24 early and may guide the adjustment of treatment strategies.
In summary, we observed that POD24 was an independent adverse predictor for OS, and, elevated LDH, elevated TG, and non-responsive disease were independent adverse prognostic factors for POD24 in PCNS-DLBCL. The “LTE” prediction model, which included these above three factors, might serve as a strong predictor of POD24. Additionally, the “LTE” prediction model was an adverse prognostic indicator for OS and PFS in PCNS-DLBCL. Several limitations of our study should be noted. The modest sample size may affect the robustness of our conclusions. Furthermore, our prognostic model lacks contemporary molecular biomarkers, a significant oversight given their clinical relevance. The model’s predictive accuracy also remains untested in the context of novel therapies, such as BTK inhibitors and pomalidomide, which are changing the treatment paradigm for PCNSL. Therefore, large-scale prospective trials are essential to validate our findings and define the role of the “LTE” model in this new therapeutic era.
Data availability
The datasets analysed during the current study available from the corresponding author on reasonable request.
References
Chen, T. et al. Evidence-based expert consensus on the management of primary central nervous system lymphoma in China. J. Hematol. Oncol. 15, 136 (2022).
Ferreri, A. J. et al. Prognostic scoring system for primary CNS lymphomas: The international extranodal lymphoma study group experience. J. Clin. Oncol. 21, 266–272 (2003).
Abrey, L. E. et al. Primary central nervous system lymphoma: The memorial Sloan-Kettering cancer center prognostic model. J. Clin. Oncol. 24, 5711–5715 (2006).
Liu, C. J. et al. A new prognostic score for disease progression and mortality in patients with newly diagnosed primary CNS lymphoma. Cancer Med. 9, 2134–2145 (2020).
Casulo, C. et al. Early relapse of follicular lymphoma after rituximab plus Cyclophosphamide, Doxorubicin, Vincristine, and prednisone defines patients at high risk for death: An analysis from the National lymphocare study. J. Clin. Oncol. 33, 2516–2522 (2015).
Epperla, N. et al. Impact of early relapse within 24 months after first-line systemic therapy (POD24) on outcomes in patients with marginal zone lymphoma: A US multisite study. J. Hematol. Oncol. 16, 49 (2023).
Chen, H. et al. The prognostic significance of POD24 in peripheral T-cell lymphoma. Hematology 29, 2304483 (2024).
Maurer, M. J. et al. Event-free survival at 24 months is a robust end point for disease-related outcome in diffuse large B-cell lymphoma treated with immunochemotherapy. J. Clin. Oncol. 32, 1066–1073 (2014).
Yoon, S. E. et al. Role of upfront autologous stem cell transplantation in patients newly diagnosed with primary CNS lymphoma treated with R-MVP: Real-world data from a retrospective single-center analysis. Bone Marrow Transpl. 57, 641–648 (2022).
Tang, D. et al. Epidemiologic characteristics, prognostic Factors, and treatment outcomes in primary central nervous system lymphoma: A SEER-Based study. Front. Oncol. 12, 817043 (2022).
Camilleri-Broët, S. et al. A uniform activated B-cell-like immunophenotype might explain the poor prognosis of primary central nervous system lymphomas: Analysis of 83 cases. Blood 107, 190–196 (2006).
Cho, U., Oh, W. J., Hong, Y. K. & Lee, Y. S. Prognostic significance of high Ki-67 index and histogenetic subclassification in primary central nervous system lymphoma. Appl. Immunohistochem. Mol. Morphol. 26, 254–262 (2018).
Kobayashi, H. et al. Long-Term evaluation of combination treatment of single agent HD-MTX chemotherapy up to three cycles and moderate dose whole brain irradiation for primary CNS lymphoma. J. Chemother. 31, 35–41 (2019).
Mendez, J. S. et al. The elderly left behind-changes in survival trends of primary central nervous system lymphoma over the past 4 decades. Neuro Oncol. 20, 687–694 (2018).
Kaji, F. A. et al. Improved survival outcomes despite older age at diagnosis: An era-by-era analysis of patients with primary central nervous system lymphoma treated at a single referral centre in the united Kingdom. Br. J. Haematol. 195, 561–570 (2021).
Jahnke, K. et al. Relapse of primary central nervous system lymphoma: Clinical features, outcome and prognostic factors. J. Neurooncol. 80, 159–165 (2006).
Mendez, J. S. & Grommes, C. Treatment of primary central nervous system lymphoma: From chemotherapy to small molecules. Am. Soc. Clin. Oncol. Educ. Book. 38, 604–615 (2018).
Liu, Y., Yao, Q. & Zhang, F. Diagnosis, prognosis and treatment of primary central nervous system lymphoma in the elderly population (Review). Int. J. Oncol. 58, 371–387 (2021).
Meng, Y. et al. High prevalence of hepatitis B virus infection in primary central nervous system lymphoma. Int. J. Clin. Exp. Med. 8, 9937–9942 (2015).
Chen, D. G. et al. Clinicopathological and prognostic features of hepatitis B virus-associated diffuse large B-cell lymphoma: A single-center retrospective study in China. Infect. Agent Cancer. 16, 57 (2021).
Wu, S. et al. The role of surgical resection in primary central nervous system lymphoma: A single-center retrospective analysis of 70 patients. BMC Neurol. 21, 190 (2021).
Thomas, A. et al. Radiotherapy for newly diagnosed primary central nervous system lymphoma: Role and perspective. Rep. Pract. Oncol. Radiother. 28, 271–285 (2023).
Schellekes, N. et al. Resection of primary central nervous system lymphoma: Impact of patient selection on overall survival. J. Neurosurg. 135, 1016–1025 (2021).
Labak, C. M. et al. Surgical resection for primary central nervous system lymphoma: A systematic review. World Neurosurg. 126, e1436–e1448 (2019).
Cloney, M. B. et al. The safety of resection for primary central nervous system lymphoma: A single institution retrospective analysis. J. Neurooncol. 132, 189–197 (2017).
Yun, J. et al. Assessing the safety of craniotomy for resection of primary central nervous system lymphoma: A nationwide inpatient sample analysis. Front. Neurol. 8, 478 (2017).
Van Dijck, R., Doorduijn, J. K. & Bromberg, J. The role of rituximab in the treatment of primary central nervous system lymphoma. Cancers (Basel) 13, (2021).
Bromberg, J. et al. Survival, neurocognitive function, and health-related quality of life outcomes after rituximab-methotrexate, BCNU, teniposide, and prednisolone for primary CNS lymphoma: Final results of the HOVON 105/ALLG NHL 24 study. Neuro Oncol. 26, 724–734 (2024).
Houillier, C. et al. Radiotherapy or autologous Stem-Cell transplantation for primary CNS lymphoma in patients age 60 years and younger: Long-Term results of the randomized phase II PRECIS study. J. Clin. Oncol. 40, 3692–3698 (2022).
Ferreri, A. et al. Whole-brain radiotherapy or autologous stem-cell transplantation as consolidation strategies after high-dose methotrexate-based chemoimmunotherapy in patients with primary CNS lymphoma: Results of the second randomisation of the international extranodal lymphoma study Group-32 phase 2 trial. Lancet Haematol. 4, e510–e523 (2017).
Houillier, C. et al. Radiotherapy or autologous stem-cell transplantation for primary CNS lymphoma in patients 60 years of age and younger: Results of the intergroup ANOCEF-GOELAMS randomized phase II PRECIS study. J. Clin. Oncol. 37, 823–833 (2019).
Hwang, S. R. et al. Comparison of outcomes in postinduction strategies for primary central nervous system lymphoma: A Mayo clinic experience. Blood Adv. 9, 924–932 (2025).
Wang, F. et al. Altered serum lipid levels are associated with prognosis of diffuse large B cell lymphoma and influenced by utility of rituximab. Ann. Hematol. 102, 393–402 (2023).
van der Meulen, M. et al. MMSE is an independent prognostic factor for survival in primary central nervous system lymphoma. J. Neurooncol. 152, 357–362 (2021).
Jo, J. C. et al. Interim (18)F-FGD PET/CT May not predict the outcome in primary central nervous system lymphoma patients treated with sequential treatment with methotrexate and cytarabine. Ann. Hematol. 96, 1509–1515 (2017).
Funding
The authors declare that no specific grant was received from any funding agency in the public, commercial, or not-for-profit sectors to support this work. The authors declare no conflict of interest.
Author information
Authors and Affiliations
Contributions
Yuye Shi, Chunling Wang, and Yuqing Miao were primarily responsible for the conception and writing of the article. Yuye Shi was in charge of providing financial support. Yunjie Li, Xiaohu Xu, and Jingjing Ma was responsible for data organization and chart preparation. Yuan Deng, Tingting Ji, Zhengyuan Liu and Hong Tao were involved in data organization. The authors declare that they have no conflict of interest.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Shi, Y., Li, Y., Xu, X. et al. Prognostic significance of POD24 in primary central nervous system diffuse large B-cell lymphoma: a retrospective study. Sci Rep 16, 5443 (2026). https://doi.org/10.1038/s41598-025-34772-z
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-34772-z
