
Abstract
HIV majorly contributes to the disease burden in South Africa. Depressive symptoms are common in people living with HIV (PLHIV). Few studies compared depressive symptoms between PLHIV and those without HIV. The aim of the study was to examine the association of HIV status and depressive symptoms. Moreover, the study aimed to explore the comparison between HIV-negative participants and the different HIV-positive sub-groups regarding their depressive symptoms. A cross-sectional analysis was conducted among PLHIV and HIV-negative participants in rural South Africa, using the baseline data of the Ndlovu Cohort study. Data was collected on demographics, socioeconomic status, and depressive symptoms using the PHQ-9 questionnaire. A score of 10 and above indicated depressive symptoms. Logistic regression analysis on the relationship between HIV status and depressive symptoms was used while adjusting for age, sex, level of education, employment status, income, and ever smoking. The study included 1,927 participants; 46% were PLHIV and 239 (12.5%) had depressive symptoms. PLHIV were more likely to have depressive symptoms than HIV-negative participants (OR 1.34, 95% CI 1.01–1.77). This association was not statistically significant after adjusting for confounders (OR 1.22, 95% CI 0.92–1.63). Compared to HIV-negative participants, ART (antiretroviral treatment) naïve participants had statistically significant higher odds of depressive symptoms (OR 1.84, 95% CI 1.20–2.78). This association remained after adjusting for confounders (OR 1.72, 95% CI 1.11–2.61). There was no statistically significant difference in depressive symptoms between HIV-negative participants and those on ART, regardless of treatment regimen. In general, higher odds of depressive symptoms in ART-naïve PLHIV could reflect poor coping with diagnosis of HIV. Future research to investigate the relation between ART regimen and depressive symptoms, to establish causality and to identify changes over time, is warranted.
Similar content being viewed by others

Introduction
In South Africa, HIV/AIDS (human immunodeficiency virus/acquired immunodeficiency syndrome) largely contributes to the burden of disease1. In 2022, there are approximately 8.45 million people living with HIV (PLHIV) in South Africa (13.9% of the population)1. The number of HIV/AIDS-related deaths has declined significantly in South Africa, with a reduction of 70% between 2010 (150,000) and 2022 (45,000)2, largely attributed to the increased use of antiretroviral therapy (ART)3. In South Africa, approximately 5.6 million PLHIV are on ART2. The increase in life expectancy of PLHIV leads to an increasing number of PLHIV with comorbidities, such as cardiovascular disease and neuropsychiatric diseases4. Depression is among the most common psychiatric comorbidities in PLHIV5,6,7,8. The estimated prevalence of depressive symptoms in PLHIV in South Africa was found to vary from 30 to 62%9,10,11,12. The occurrence of depressive symptoms is based on a screening instrument that uses a certain threshold score (e.g., Center for Epidemiologic Studies Depression Scale [CES-D], Patient Health Questionnaire-9 [PHQ-9]), whereas the diagnosis of a depressive disorder is based on the Diagnosis and Statistical Manual of Mental Disorders (DSM)12.
A meta-analysis, that investigated the relationship between depressive disorders and HIV, concluded that PLHIV are approximately two times more likely to have a depressive disorder compared to HIV-negative people13. However, this meta-analysis only included studies that were conducted in high income countries, which primarily included specific populations such as injecting drug users and men having sex with men13. A cross-sectional study in regional hospitals in KwaZulu Natal (South Africa), observed that the majority of women with significant depressive symptoms were PLHIV14. However, the prevalence of depressive symptoms did not differ significantly between PLHIV and HIV-negative participants14. Other factors could also influence the relationship between HIV status and depressive symptoms. Women, and those with a low level of education have been found to be more likely to have depressive symptoms15. A lower socioeconomic status (SES) has also been associated with an increased risk of having depressive symptoms and acquiring an HIV-infection6,16.
Although multiple studies have been conducted in sub-Saharan Africa, and particularly South Africa, to establish the prevalence of depressive symptoms in PLHIV, few studies included an HIV-negative comparison group. Most of the studies that included HIV-negative participants were conducted in specific populations, such as pregnant women, adolescents, or elderly. Moreover, many of these studies had a small sample size, which might have led to insufficient statistical power to make an adequate comparison between PLHIV and HIV-negative individuals.
Depressive symptoms are associated with medication non-adherence and sexual risk-taking in PLHIV17. Medication non-adherence negatively influences HIV-infection, resulting in increased risk of disease progression and mortality17. At the same time, depressive symptoms might increase sexual risk behavior, increasing the probability of contracting and transmitting HIV17,18. Therefore, the aim of this study was to investigate the association of HIV status and depressive symptoms in the Ndlovu Cohort study (NCS). Moreover, the study aimed to explore the comparison between HIV- participants and the different HIV + sub-groups regarding their depressive symptoms.
Methods
Study design and study population
The NCS was conducted in a rural township in the Moutse area, Elandsdoorn, Limpopo Province in South Africa19. The cohort was originally set up to investigate the risk of cardiovascular disease in PLHIV and HIV-negative participants in low/middle income setting19. The current study was a cross-sectional study, using the baseline data of the NCS. A detailed description of the methods of the NCS is provided by Vos et al.19.
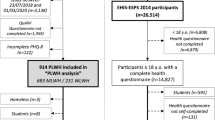
A community liaison officer and a team of counsellors at the Ndlovu Medical Center (NMC) HIV clinic were used to recruit participants at the NMC clinics, local events, in shopping areas and through community campaigns19. People eligible for inclusion were: (1) aged 18 years or older; (2) able to provide written, informed consent; and (3) committed to a long-term follow-up. Individuals were excluded for the study if, for any reason, they were unable to undergo the study procedures (e.g., not willing to undergo physical examination, HIV testing or blood sampling)19. The study included a total of 1,927 participants, of which 887 were PLHIV and 1,040 were HIV-negative, recruited between November 2014 and August 201719,20.
Measurements/data collection
Sociodemographics
Information on age, sex, education, employment status and income was collected. The highest level of education was measured by four different categories: no education, primary, secondary and matric (i.e., the final grade in secondary school), and college and university. The group that had no education was used as the reference category. Employment status and income position were measured by the National Income Dynamics Study (NIDS) Wave 3 2012 Adults Questionnaire21. Employment status was divided into three categories: employed, unemployed, and other (e.g., student, volunteer, elderly citizen). Participants that were unemployed or categorized as other were compared to those that were employed. For income position three categories were distinguished: less than 648 ZAR (South African Rands), between 648 and 992 ZAR, and more than 992 ZAR per person per month. This was based on the definitions for the lower and upper bound poverty lines in 2015, which were 648 and 992 ZAR per person per month22,23. In 2015 the average exchange rate for 100 ZAR was equivalent to 7.88 United States dollars (USD)24. The group with the lowest income was taken as the reference category.
Depressive symptoms (outcome)
Depressive symptoms were measured using the Patient Health Questionnaire-9 (PHQ-9), a validated screening tool for depression25,26,27. The questionnaire was administered by one of the trained counsellors of the NCS. The questionnaire consists of nine questions about how often the participant has been bothered by any of the mentioned problems in the last two weeks, which could all be answered with the following categories: “not at all” (0 points), “several days” (1 point), “more than half the days” (2 points), and “nearly every day” (3 points)26,27. A participant with a score of 10 or higher out of 27 was classified as having clinically significant depressive symptoms, while a participant with a score below 10 was classified as having no clinically significant depressive symptoms, further referred to as having no depressive symptoms in this paper28. This cut-off value was chosen as it is frequently used in other publications, making it possible to compare results across studies12. Moreover, studies in primary health care clinics in South Africa determined that the optimal cut-off score lies between 8 and 1128, and this cut-off value has a moderately high sensitivity and specificity29. To estimate internal consistency of the PHQ-9 questionnaire we estimated Cronbach’s alpha. Cronbach’s alpha was 0.82 for the study population with minor differences between HIV+ (0.82) and HIV- (0.81) study participants, indicating good internal consistency of PHQ9 items.
HIV testing
To be eligible for enrollment as a PLHIV it was necessary that there was documentation of a positive HIV test result or proof of being on ART. In all other cases, participants were tested upon enrollment in the study19.
An antibody-based point-of-care test (ADVANCED QUALITY™ Rapid HIV Test [InTec Products, China]) was used to determine HIV status30. This test has a 98.8% sensitivity and a 100% specificity30. Participants with a positive test were retested with a second point-of-care test (ABON™ HIV HIV 1/2/O Tri-Line HIV Rapid Test Device [ABON Biopharm Hangzou, China]), which has a sensitivity of 100% and a specificity of 97.7%31. In order to clarify indeterminate results and to confirm positive results, an enzyme-linked immunosorbent assay was performed19.
ART regimen
ART use was self-reported20 and complemented with data from TIER.net, which is a national online electronic database that monitors treatment of HIV and tuberculosis32. ART naïve participants were defined as those who were not (yet) on treatment or initiated treatment at a maximum of eight weeks before enrollment20. Moreover, first- and second-line treatment regimens were distinguished. Participants on first-line ART primarily used tenofovir, emtricitabine, and efavirenz20. Most of the participants on second-line ART used ritonavir-boosted lopinavir20.
Substance use
A modified version of the World Health Organization (WHO) STEPS instrument was used to collect data on smoking and alcohol consumption19,33. In this study the information on ever and current smoking and alcohol consumption were used.
Data analysis
In the responses to the PHQ-9 test 16 missing values (0.8% of participants) were recorded, which were distributed over all nine questions. On income 103 values were missing (5.3% of the participants). One value was missing for having ever smoked (0.05%). There were no missing values for the other variables. Data was assumed to be missing at random.
The “mice” package of R was used to generate 20 imputed datasets for multiple imputation34. The available measurements on depressive symptoms, sex, and age were used for imputation. Furthermore, HIV status, education, employment, ever/current smoking and alcohol consumption, and income position were used to impute. Convergence of the MICE algorithm was confirmed with convergence plots. In each imputed dataset the parameters of interest were estimated separately. Then they were combined for analysis using Rubin’s rules35. A complete case analysis was conducted as well.
The prevalence of depressive symptoms was described and compared between PLHIV and HIV-negative participants. Continuous variables were summarized by means with standard deviations (sd) in normally distributed data, or medians and interquartile ranges (IQR) in non-normally distributed data. Categorical variables were expressed as frequency counts and percentages. These variables were compared between participants with and without depressive symptoms.
To investigate the association between HIV status and depressive symptoms logistic regression was used providing an odds ratio (OR) and 95% confidence interval (CI). Based on literature review, sex, age, level of education, income position, employment status, current/ever smoking and alcohol use were considered for statistical analysis. Univariable analysis was conducted and in case of a p-value < 0.2, variables were included in multivariable analysis. To explore the association between ART regimen and depressive symptoms the same procedure was used. All analyses were performed with the statistical software R version 3.6.136. Statistical significance was considered at a two-sided p-value below 0.05.
Results
The characteristics of the study population are presented in Table 1. This study included a total of 1,927 participants, of which 46.0% (n = 887) were PLHIV. Majority of participants were female (54.8%), had completed secondary and matric education (67.5%), were unemployed (67.8%), and had a reported income below 648 ZAR (62.7%). In the study population the median PHQ-9 score was 3 (IQR: 0–7). Most of the participants reported having ever used alcohol (70.5%). More than a quarter of the population was a current smoker (27.9%) or used alcohol in the past 30 days (33.8%).
Among participants with depressive symptoms, 53.6% were PLHIV, which were 45.0% among participants with no depressive symptoms. Details on the distribution of the total PHQ-9 score stratified by HIV status are presented in Supplementary Fig. 1. The prevalence of depressive symptoms was 14.5% among PLHIV and 10.8% among HIV-negative participants. The median age was higher in the participants with depressive symptoms (42 years, IQR 32-50.5) than in those without depressive symptoms (38 years, IQR 27–48). Among participants with depressive symptoms, 74.9% were unemployed, which was higher than among participants without depressive symptoms (66.7%). Among the participants with depressive symptoms 45.2% ever smoked, while 40.5% of those without depressive symptoms reported to have ever smoked. Current smoking was more common among those without depressive symptoms (28.3%) than those with depressive symptoms (26.8%). Alcohol use, ever and in the past 30 days, was also more frequent among the participants without depressive symptoms (70.5% and 34.2% respectively) compared to those with depressive symptoms (69.9% and 31.8% respectively).
Table 2 shows the results of the analyses of HIV status and ART regimen in relation to depressive symptoms. In univariable logistic regression analysis, the odds of having depressive symptoms were 1.34 times higher in PLHIV compared to HIV-negative participants (95% CI: 1.01–1.77). Adjustment for age and sex attenuated the association (OR = 1.21, 95% CI 0.91–1.60), that was slightly altered after further adjustment for education, employment status, income position, ever smoking (OR = 1.22, 95% CI: 0.92–1.63). Multivariable analysis for model 3 after multiple imputation provided similar results (See Supplementary Information, Supplementary Table 1).
Table 2 presents the association of ART regimen and depressive symptoms. Analysis showed that the odds of depressive symptoms of PLHIV on first- and second-line ART compared to HIV-negative participants did not differ significantly. For ART naïve participants the odds of having depressive symptoms were 1.85 times higher than for HIV-negative participants (95% CI: 1.20–2.78). The association between being ART naïve and depressive symptoms remained statistically significant after adjusting for age and sex (OR = 1.81, 95% CI 1.17–2.73), and further adjustment for education, employment status, income position, ever smoking (OR = 1.72, 95% CI 1.11–2.61). Adding time since HIV diagnosis to the models did not change the findings of a higher score in ART naïve individuals compared to PLHIV on first- or second-line ART (See Supplementary Information, Supplementary Table 2). The results for model 3 after multiple imputation were similar to those from the full case analysis (See Supplementary Information, Supplementary Table 1).
Discussion
The aim of the study was to assess the association between HIV status and depressive symptoms. The univariable analysis showed that PLHIV were more likely to have depressive symptoms than their HIV-negative peers, but this association was attenuated after adjusting for confounding. The analyses also showed that there was no significant difference between PLHIV on ART and HIV-negative controls, while ART naïve PLHIV were more likely to have depressive symptoms than the HIV-negative participants.
To date, few studies directly compared the risk of depressive symptoms or depression in PLHIV and HIV-negative participants. Similar to the current study, a couple of studies did not find a statistical association between HIV status and depressive symptoms. They attributed this lack of association to the importance of other determinants than HIV status, such as psychosocial factors and the availability of ART37,38. However, a systematic review concluded that PLHIV have more mental health problems than the HIV-negative population, which is contrary to the results of the current study7. There are several possible explanations as to why PLHIV might be more likely to suffer from depression. An important psychosocial factor is stigma regarding sexually transmitted disease and risk-behavior39. This might lead to isolation, lack of support, discrimination, and violence, which are associated with depressive episodes39,40,41. A biological theory suggests that neurobiological changes might occur due to persistent viral presence in the central nervous system8,39,42. It has also been hypothesized that pro-inflammatory cytokines could decrease the bioavailability by activating a tryptophan-degrading enzyme subsequently affecting the neurotransmission of serotonin, leading to depressive symptoms39,43,44.
We observed ART naïve participants to have higher odds of depressive symptoms compared to HIV-negative participants. However, this finding needs to be interpreted with caution as this is based on a small group size that is ART naïve with depressive symptoms (n = 37, 1.9% of the total study population). To explore this finding, we adjusted the models for time since HIV diagnosis, as the majority (75%) of the ART naïve participants were recently diagnosed with HIV, explaining why they were not yet started on treatment. However, no association between time since HIV diagnosis and depressive symptoms was observed. Previous studies that examined the relationship between ART and depression in sub-Saharan Africa observed an association between depression and untreated HIV infection39,45,46,47,48,49. This association is considered to be bi-directional, i.e. being ART naïve being associated with having depressive symptoms and having depressive symptoms being associated with lower uptake of ART treatment and adherence. Several longitudinal studies found that being on ART has a protective effect on developing depression compared to being ART naïve39,45,46,47,48,49. A cohort study, conducted in rural Uganda, concluded that ART is associated with a reduction of internalized stigma, specifically during the first two years of treatment49. A biological mechanism that potentially explains the protective effect of ART is due a reduction in immune cell activation and cytokine levels39.
A major strength of this study was the large size of the study population including PLHIV and HIV-negative participants. Moreover, the general population was approached for inclusion, which adds to the literature that focused on more specific subgroups, such as elderly or pregnant women. Limitations relate to the cross-sectional analyses that do not allow to draw conclusions regarding causality. Another limitation is that part of the study participants was recruited before 2016, when the test and treat policy was incorporated in the HIV treatment guidelines in South Africa. Since then, there should be no groups of PLHIV but ART naïve participants as all needed to commence treatment as soon as possible.
Further studies are needed to conclude whether there is a difference in occurrence of depressive symptoms due to different ART regimens, as the current study was based on a small group of participants on second-line ART compared to those on first-line ART. Besides, the current first line ART includes integrase strand transfer inhibitors, which was not yet the case when this study was conducted. Longitudinal studies will allow to establish the causal relationship between HIV status and depressive symptoms and to identify changes in the prevalence of depressive symptoms and total PHQ-9 scores over time/upon initiation with ART.
To conclude, PLHIV did not report depressive symptoms more often compared to their HIV-negative peers. Higher odds of depressive symptoms in ART-naïve PLHIV could reflect poor coping with a new diagnosis of HIV. Following a new diagnosis of an HIV infection there should be awareness among healthcare providers that people might struggle with depressive symptoms. Future research is needed to further investigate the relation between ART regimen and depressive symptoms, to establish causality and to identify changes over time.
Data availability
Data is available from the corresponding author on reasonable request.
References
Statistics South Africa. Mid-year population estimates. Pretoria, South Africa: Statistics South Africa; 2022 July 28 2022. Report No.: P0302.
UNAIDS. UNAIDS data 2023 (UNAIDS, 2023).
UNAIDS. The Gap Report (UNAIDS, 2014).
Smit, M. et al. Future challenges for clinical care of an ageing population infected with HIV: A modelling study. Lancet Infect. Dis. 15 (7), 810–818. https://doi.org/10.1016/S1473-3099(15)00056-0 (2015).
Dubé, B., Benton, T., Cruess, D. G. & Evans, D. L. Neuropsychiatric manifestations of HIV infection and AIDS. J. Psychiatry Neurosci. 30 (4), 237–246 (2005).
Arseniou, S., Arvaniti, A. & Samakouri, M. HIV infection and depression. Psychiatry Clin. Neurosci. 68 (2), 96–109. https://doi.org/10.1111/pcn.12097 (2014).
Brandt, R. The mental health of people living with HIV/AIDS in Africa: A systematic review. Afr. J. AIDS Res. 8 (2), 123. https://doi.org/10.2989/ajar.2009.8.2.1.853 (2009).
Owe-Larsson, B., Sall, L., Salamon, E. & Allgulander, C. HIV infection and psychiatric illness. Afr. J. Psychiatry. 12 (2), 115. https://doi.org/10.4314/ajpsy.v12i2.43729 (2009).
Hughes, J., Jelsma, J., Maclean, E., Darder, M. & Tinise, X. The health-related quality of life of people living with HIV/AIDS. Disabil. Rehabil. 26 (6), 371–376. https://doi.org/10.1080/09638280410001662932 (2004).
Cholera, R. et al. Depression and engagement in care among newly diagnosed HIV-Infected adults in Johannesburg, South Africa. AIDS Behav. 21 (6), 1632–1640. https://doi.org/10.1007/s10461-016-1442-6 (2017).
Ramirez-Avila, L. et al. Depressive symptoms and their impact on health-seeking behaviors in newly-diagnosed HIV-infected patients in Durban, South Africa. AIDS Behav. 16 (8), 2226–2235. https://doi.org/10.1007/s10461-012-0160-y (2012).
Bernard, C., Dabis, F. & de Rekeneire, N. Prevalence and factors associated with depression in people living with HIV in sub-saharan Africa: A systematic review and meta-analysis. PLoS ONE. 12 (8), e0181960. https://doi.org/10.1371/journal.pone.0181960 (2017).
Ciesla, J. A. & Roberts, J. E. Meta-analysis of the relationship between HIV infection and risk for depressive disorders. Am. J. Psychiatry 158 (5), 725–. https://doi.org/10.1176/appi.ajp.158.5.725 (2001). 30.
Nydoo, P., Naicker, T. & Moodley, J. Depressive scores in newly diagnosed HIV-infected and HIV-uninfected pregnant women. S. Afr. J. Psychiatr. 23, 1085. https://doi.org/10.4102/sajpsychiatry.v23i0.1085 (2017).
Tomlinson, M., Grimsrud, A. T., Stein, D. J., Williams, D. R. & Myer, L. The epidemiology of major depression in South Africa: results from the South African stress and health study. S. Afr. Med. J. 99 (5 Pt 2), 367–373 (2009).
Probst, C. et al. Socioeconomic status and risk of HIV infections. AIDS Behav. 21 (7), 1926–1937. https://doi.org/10.1007/s10461-017-1758-x (2017).
Schuster, R., Bornovalova, M. & Hunt, E. The influence of depression on the progression of HIV: Direct and indirect effects. Behav. Modif. 36 (2), 123–. https://doi.org/10.1177/0145445511425231 (2012). 45.
Smit, J. et al. Mental health and sexual risk behaviours in a South African township: A community-based cross-sectional study. Public. Health. 120 (6), 534–. https://doi.org/10.1016/j.puhe.2006.01.009 (2006). 42.
Vos, A. et al. HIV and risk of cardiovascular disease in sub-saharan Africa: Rationale and design of the Ndlovu Cohort study. Eur. J. Prev. Cardiol. 24 (10), 1043–1050. https://doi.org/10.1177/2047487317702039 (2017).
Vos, A. G. et al. Cardiovascular Disease Burden in Rural Africa: Does HIV and Antiretroviral Treatment play a role? Baseline analysis of the Ndlovu Cohort study. J. Am. Heart Assoc. 9 (7), e013466. https://doi.org/10.1161/jaha.119.013466 (2020).
Southern Africa Labour and Development Research Unit. National income dynamics study wave 3: 2012 proxy questionnaire [Internet] [place unknown]: Southern Africa Labour and Development Research Unit; 2013 [updated 2021; cited 2022 Jan 15]. Available from: https://www.datafirst.uct.ac.za/dataportal/index.php/catalog/453/study-description
Statistics South Africa. National poverty lines. Pretoria, South Africa: Statistics South Africa. Report No.: P0310.1. (2018).
Ketelaar, E. J. et al. Ideal cardiovascular health index and its determinants in a rural South African population. Glob Heart. 15 (1), 76. https://doi.org/10.5334/gh.801 (2020).
Exchange Rates, U. K. Available from: https://www.exchangerates.org.uk/ZAR-USD-spot-exchange-rates-history-2015.html
Spitzer, R. L., Kroenke, K., Williams, J. B. W. & Group atPHQPCS. Validation and utility of a self-report version of PRIME-MD the PHQ primary care study. JAMA 282 (18), 1737–1744. https://doi.org/10.1001/jama.282.18.1737 (1999).
Kroenke, K., Spitzer, R. L. & Williams, J. B. The PHQ-9: Validity of a brief depression severity measure. J. Gen. Intern. Med. 16 (9), 606–613. https://doi.org/10.1046/j.1525-1497.2001.016009606.x (2001).
Pfizer Inc. Patient Health Questionnaire (PHQ-9). (Pfizer Inc., 1999).
Bhana, A., Rathod, S. D., Selohilwe, O., Kathree, T. & Petersen, I. The validity of the Patient Health Questionnaire for screening depression in chronic care patients in primary health care in South Africa. BMC Psychiatry. 15 (1), 118. https://doi.org/10.1186/s12888-015-0503-0 (2015).
Cholera, R. et al. Validity of the Patient Health Questionnaire-9 to screen for depression in a high-HIV burden primary healthcare clinic in Johannesburg, South Africa. J. Affect. Disord. 167, 160–166. https://doi.org/10.1016/j.jad.2014.06.003 (2014).
World Health Organization. HIV Assays: Operational Characteristics (Phase I) (World Health Organization, 2002). Report No. 12
World Health Organization. Prequalification of Diagnostic Programme Geneva (World Health Organization, 2014).
Osler, M. et al. A three-tier framework for monitoring antiretroviral therapy in high HIV burden settings. J. Int. AIDS Soc. 17 (1), 18908. https://doi.org/10.7448/ias.17.1.18908 (2014).
World Health Organization. STEPwise approach to NCD risk factor surveillance (STEPS) [Internet] Geneva: World Health Organization; Available from: https://www.who.int/teams/noncommunicable-diseases/surveillance/systems-tools/steps
van Buuren, S. & Groothuis-Oudshoorn, K. Mice: Multivariate imputation by chained equations in R. J. Stat. Softw. 45 (3), 1–67. https://doi.org/10.18637/jss.v045.i03 (2011).
Rubin, D. B. Inference and missing data. Biometrika 63 (3), 581. https://doi.org/10.1093/biomet/63.3.581 (1976).
R Core Team. R: A Language and Environment for Statistical Computing (R Foundation for Statistical Computing, 2020).
Geldsetzer, P. et al. Depressive symptoms and their relation to age and chronic diseases among middle-aged and older adults in rural South Africa. J. Gerontol. Biol. Sci. Med. Sci. 74 (6), 957–963. https://doi.org/10.1093/gerona/gly145 (2019).
Mwangala, P. N., Nasambu, C., Wagner, R. G., Newton, C. R. & Abubakar, A. Prevalence and factors associated with mild depressive and anxiety symptoms in older adults living with HIV from the Kenyan coast. J. Int. AIDS Soc. 25 (Suppl 4), e25977. https://doi.org/10.1002/jia2.25977 (2022).
Nanni, M. G., Caruso, R., Mitchell, A. J., Meggiolaro, E. & Grassi, L. Depression in HIV infected patients: A review. Curr. Psychiatry Rep. 17 (1), 530. https://doi.org/10.1007/s11920-014-0530-4 (2015).
Schuster, R. M. & Gonzalez, R. Substance abuse, hepatitis C, and aging in HIV: Common cofactors that contribute to neurobehavioral disturbances. Neurobehav. HIV Med. 2012 (4), 15–34. https://doi.org/10.2147/nbhiv.S17408 (2012).
Grassi, L. et al. Illness behavior, emotional stress and psychosocial factors among asymptomatic HIV-infected patients. Psychother. Psychosom. 68 (1), 31–38. https://doi.org/10.1159/000012308 (1999).
Del Guerra, F. B., Fonseca, J. L., Figueiredo, V. M., Ziff, E. B. & Konkiewitz, E. C. Human immunodeficiency virus-associated depression: Contributions of immuno-inflammatory, monoaminergic, neurodegenerative, and neurotrophic pathways. J. Neurovirol. 19 (4), 314–. https://doi.org/10.1007/s13365-013-0177-7 (2013). 27.
Dantzer, R., O’Connor, J. C., Freund, G. G., Johnson, R. W. & Kelley, K. W. From inflammation to sickness and depression: When the immune system subjugates the brain. Nat. Rev. Neurosci. 9 (1), 46–56. https://doi.org/10.1038/nrn2297 (2008).
Dantzer, R., O’Connor, J. C., Lawson, M. A. & Kelley, K. W. Inflammation-associated depression: From serotonin to kynurenine. Psychoneuroendocrinology 36 (3), 426–. https://doi.org/10.1016/j.psyneuen.2010.09.012 (2011). 36.
Martinez, P. et al. Reversal of the Kynurenine pathway of tryptophan catabolism may improve depression in ART-treated HIV-infected ugandans. J. Acquir. Immune Defic. Syndr. 65 (4), 456–. https://doi.org/10.1097/qai.0000000000000062 (2014). 62.
Gutiérrez, F. et al. Risk of clinically significant depression in HIV-infected patients: Effect of antiretroviral drugs. HIV Med. 15 (4), 213–223. https://doi.org/10.1111/hiv.12104 (2014).
Nakasujja, N. et al. Improvement in depressive symptoms after antiretroviral therapy initiation in people with HIV in Rakai, Uganda. J. Neurovirol. 27 (4), 519. https://doi.org/10.1007/s13365-020-00920-6 (2021). 30.
Wagner, G. J., Ghosh-Dastidar, B., Garnett, J., Kityo, C. & Mugyenyi, P. Impact of HIV antiretroviral therapy on depression and mental health among clients with HIV in Uganda. Psychosom. Med. 74 (9). https://doi.org/10.1097/PSY.0b013e31826629db (2012).
Tsai, A. C. et al. How does antiretroviral treatment attenuate the stigma of HIV? Evidence from a cohort study in rural Uganda. AIDS Behav. 17 (8), 2725–2731. https://doi.org/10.1007/s10461-013-0503-3 (2013).
Acknowledgements
We would like to acknowledge the Ndlovu Cohort study research team for collecting all the data. We would also like to thank all the study participants without whom this work would not be possible.
Funding
This work was supported by a grant from the Dutch AIDS Foundation, Dioraphte Foundation, De Grote Onderneming, Hofstee Stichting, and the University Medical Center Utrecht.
Author information
Authors and Affiliations
Contributions
LXYdB, KS, AGV, and KKG contributed to the study conception and design. Data analysis, and interpretation of data for the work was performed by LXYdB, KS, AGV, and KKG. The first draft of the manuscript was written by LXYdB. All authors critically commented the article and read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval
The study was conducted in accordance with the Declaration of Helsinki and was approved by the Human Research Ethics Committee at the University of Pretoria, Pretoria, South Africa, and the Limpopo Department of Health Ethics Committee (ethics reference number: 227/2014). Written informed consent was obtained from all participants prior to study participation.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
den Boer, L.X.Y., Scheuermaier, K., Tempelman, H.A. et al. The association of HIV status and depressive symptoms in the Ndlovu Cohort study. Sci Rep 15, 4539 (2025). https://doi.org/10.1038/s41598-025-85830-5
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-85830-5
