
Abstract
The aim of this study was to analyze the outcomes of arthroscopic subscapularis tendon repair combined with coracoplasty in the treatment. The study involved 80 patients (46 males, 34 females; aged 33 to 73 years), who underwent arthroscopic repair for subscapularis tears (type I, II, and III) presenting symptoms of anterior shoulder pain and tenderness. Subcoracoid impingement was defined as a coracohumeral distance of less than 6 mm on preoperative magnetic resonance imaging, with a follow-up of was at least two years. The patients were divided into two groups: Group A underwent coracoplasty, while Group B did not. The postoperative functional outcomes of the two groups were compared and analyzed using an independent sample t-test. The patients’ prognosis was assessed pre- and postoperatively using the University of California Los Angeles (UCLA) shoulder score, American Shoulder and Elbow Surgeons (ASES) shoulder score, and Visual Analog Scale (VAS)pain score. Postoperatively, primary wound healing was successful in all patients, with no systemic or localized shoulder joint infections or brachial plexus nerve injuries. Both groups showed improvements in overall functional outcomes after surgical intervention. At the 24-month follow-up, all evaluated parameters in both groups demonstrated improvements compared to preoperative values (P < 0.05). The functional scores significantly increased in both groups post-surgery compared to preoperative values (p < 0.01). When comparing the two groups using an independent sample t-test, the p-values for all indicators, except forward flexion range of motion, were below 0.01. The statistical analysis indicated that patients in Group A had better recovery outcomes than those in Group B, except for forward flexion. The results suggested that subcoracoid impingement syndrome could potentially be a significant precursor to subscapularis tendon injuries. It is noteworthy noting that the combined approach of subscapularis tendon repair and coracoplasty showed superior therapeutic efficacy compared to isolated subscapularis tendon repair when subscapularis tendon injuries were associated with subcoracoid impingement.
Similar content being viewed by others

Introduction
The subcoracoid impingement syndrome has gained attention as a research field in shoulder diseases1,2,3,4. It was first proposed by Professor Goldthwait in 19095. The clinical manifestations of this syndrome include anterior shoulder pain, as well as dysfunction in shoulder joint forward flexion or internal rotation. The pathogenesis involves the reduction of the distance between the coracoid process and the lesser tubercle of the humerus, which leads to long-term repeated friction between the coracoid process and the subscapularis tendon. This friction can result in edema and degeneration of the subscapularis tendon, potentially causing partial or complete tendon tear1,6. Lo and Burkhart7,8 introduced the concept of the “roller-wringer Effect” by dynamically observing the relationship between the coracoid process and the subscapularis tendon during shoulder arthroscopy. This term describes the repeated rolling impact of the subscapularis tendon between the lesser tubercle of the humerus and the coracoid process during internal rotation of the humerus. In patients with a narrowed subcoracoid space, this phenomenon may lead to subscapularis tendon injury due to subcoracoid impingement9.
While subacromial impingement has been extensively researched, there is limited literature on precursor lesions of subcoracoid impingement. There is ongoing debate on whether subcoracoid impingement contributes to subscapularis tendon injury10. Magnetic resonance imaging (MRI) or computed tomography (CT) are pivotal in diagnosing subcoracoid impingement. Coracohumeral distance (CHD), first introduced by Friedman and colleagues, is a frequently studied parameter in coracoid anatomy11. CHD denotes the smallest distance between the coracoidal tip and the nodal node in axial MRI scans. Subscapularis tendon injuries are commonly detected incidentally during arthroscopic evaluations for supraspinatus tendon injuries or adhesive capsulitis. The potential correlation between coracoid morphology and subscapularis tendon injury deserves more attention12,13. Although several classification systems for subscapularis tendon tears have been put forth, such as the Fox and Romeo classification14 and the Lafosse classification15, but there is a lack of consensus among orthopaedic surgeons regarding their use in diagnosis and treatment. Ghasemi and colleagues highlighted that the Lafosse classification is widely recognized and clinically applicable16.
Materials and methods
Participants
This was a retrospective study of 80 patients (46 males, 34 females; age range 33 to 73 years old) who underwent shoulder arthroscopy for the management of subscapularis tears associated with subcoracoid impingement syndrome (from January 2018 to January 2022, the Department of Orthopedics at the Third Affiliated Hospital of Anhui Medical University treated 80 patients with subscapularis muscle injuries using shoulder arthroscopy as the primary treatment modality). Power analysis indicated that a total sample size of 80 patients (40 patients in each cohort) would provide a statistical power of 90% with a significance level of 0.05 to detect significant differences in VAS score, assuming an effect size of 0.50 (mean difference, 0.50; standard deviation, 0.69). This was based on the mean and standard deviation of VAS score observed in a pilot study. Among these cases, 40 individuals underwent combined subscapularis tendon repair and coracoplasty, while the remaining 40 patients received isolated subscapularis tendon repair. Comprehensive follow-up assessments were conducted for all participants. In this retrospective study, we presented a comprehensive synthesis of the outcomes observed in this cohort of 80 cases. The study was approved by the Ethics Committee of the Third Affiliated Hospital of Anhui Medical University (First People’s Hospital of Hefei, Hefei, China). The ethics approval number for this study is 2024-064-02, and the registration date is April 29, 2024.
Inclusion criteria
(1) Lack of significant improvement observed after 3–6 months of conservative treatment; (2) Presence of anterior shoulder tenderness accompanied by muscle weakness or impaired shoulder anterior flexion and external rotation; (3) MRI findings indicating partial or complete subscapularis tendon tear; (4) Coracohumeral distance less than 6 mm.
Exclusion criteria
(1) Follow-up duration less than 24 months; (2) Presence of shoulder instability (e.g., SLAP lesions, Bankart lesions); (3) Prior history of shoulder joint surgery; (4) Associated injuries to the suprascapular nerve; (5) Traumatic rotator cuff injuries; 6.The presence of systemic diseases precludes surgical and anesthetic tolerance.
Observation index
Physical examinations and imaging data were conducted during the preoperative assessment and the 24-month postoperative follow-up appointments. The measurements of range of motion, including internal rotation, external rotation, and forward flexion, along with the coracohumeral distance were recorded and analyzed. Additionally, the preoperative and postoperative evaluations comprised the University of California Los Angeles (UCLA) shoulder score, the American Shoulder and Elbow Surgeons (ASES) shoulder score, and the Visual Analog Scale (VAS) pain score.
Magnetic resonance imaging (MRI) examination
The coracohumeral distance was confirmed through preoperative and postoperative shoulder joint MRI examinations, measuring the minimal space between the minor tubercle of the humerus and the subcoracoid in the internal rotation position on MRI cross-sectional scans(Fig. 1).

Pre-operative and post-operative magnetic resonance imaging results. (A) Preoperative MRI revealed coracohumeral distance constriction of approximately 5.56 mm. (B) Patients who did not undergo coracoplasty exhibited no substantial alteration in CHD 24 months post-surgery. (C) Preoperative MRI demonstrated coracohumeral distance constriction of approximately 5.49 mm. (D) Patients who underwent coracoplasty experienced a notable increase in CHD 24 months after the operation.
Surgery
All patients underwent surgical procedures under general anesthesia, positioned in a beach chair posture. A standard posterior portal was established for visualization, followed by the creation of anterior superior lateral and more medial anterior portals. The management of the long head of the biceps tendon was determined based on its condition, including direct excision or preparatory fixation before excision.
In Group A, the subcoracoid space was accessed to facilitate coracoplasty implementation. The anterior compartment of the subscapularis tendon was meticulously dissected until complete exposure to the base of the coracoid and the conjoint tendon. The Coracohumeral Distance (CHD) was measured in the internal shoulder joint position using a 4.0 mm shaver head as the standard gauge. The undersurface of the coracoid process was burred by trimming the distal portion of the curved base of the coracoid, including the spur up to 3 to 4 mm, to create a flat plane. Then, the lateral aspect was also burred by 4 to 5 mm to achieve a CHD ranging from 8 to 10 mm. In Group B, only debridement of the rotator interval was performed, without coracoplasty beneath the coracoid. Subsequently, the subscapularis tendon was thoroughly released until it provided adequate coverage over the lesser tuberosity. The minor tubercle of the humerus was burred using a 4.0 mm arthroscopy shaver head to promote bleeding. Depending on the condition of the subscapularis tendon, a 5.0 mm titanium or 4.5 mm PEEK anchor was used for suturing with a suture hook. This was securely fastened with a knot after traversing through the anchor. For specific Lafosse Type I patients, a simple PDS suture or anchor suture was used to ensure the stability of the subscapularis tendon(Fig. 2). Further interventions, including supraspinatus tendon repair on five patients, were performed based on the shoulder joint status of the individuals, with 3 cases in Group A, and 2 cases in Group B. The same departmental team performed the surgical interventions, and consistent postoperative pain management, rehabilitation, and nursing protocols were uniformly applied.

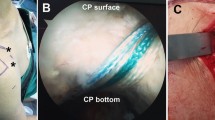
Subscapularis tendon suture combined with coracoplasty under arthroscopy observation. (A) Pre-subscapularis suture: complete tear of the upper third of the subscapularis (Lafosse type II). (B) Post-subscapularis suture: single-row fixation in a rotational neutral position following a double mattress suture of the subscapularis. (C) Prior to coracoplasty: bony hyperplasia was observed at the base and posterior coracoid process, leading to coracohumeral space constriction. (D) Following coracoplasty: The base and posterior of the coracoid process were meticulously smoothed and contoured until the bone surface achieved a sleek, even texture, consequently widening the coracohumeral distance.
The affected shoulder was immobilized in adduction and internal rotation positions for 4 weeks, with strict avoidance of shoulder elevation and excessive overhead activities. Grip exercises and gentle elbow flexion exercises were initiated from the first day post-surgery. Controlled passive external rotation and shoulder joint overhead activities were gradually initiated after the initial 4-week period. Normal muscle strength exercises and functional training were started at the 3-month postoperative mark.
Statistical analysis
Data analysis was conducted using IBM SPSS version 22.0 software (IBM Corp, Armonk, NY, USA). The independent samples t-test was employed for homogeneous and normally distributed continuous variables, while the Mann-Whitney U test was utilized for non-normally distributed or heterogeneous continuous variables. Pearson’s chi-square test was conducted for categorical variables. The statistical significance threshold was set at p < 0.05.
Results
The study involved a total of 80 patients, with 46 categorized as Lafosse15 Type I, 26 as Type II, and 8 as Type III. Among the participants, 46 were males, and 34 as females. It is worth noting that 42 cases were related to the left shoulder, while 38 cases were related to the right shoulder. The patients’ ages ranged from 33 to 73. Out of the 80 patients diagnosed with subscapularis tendon injury, a subset of 5 patients also showed signs of supraspinatus tendon injury. All participants underwent comprehensive follow-up assessments. The cohort comprised two groups, designated as Group A and Group B, each with 40 patients. Group A underwent subscapularis tendon repair along with coracoplasty, and Group B consisted of 40 patients who had isolated subscapularis tendon repair without acromion intervention. No significant differences were found in the demographic data, such as mean age, gender distribution, affected shoulder side, duration of symptoms, follow-up duration, Lafosse type classification, and Coracohumeral Distance (CHD), between Group A and Group B. Moreover, there were no significant differences in the preoperative functional motion evaluations and shoulder scores, as shown in Table 1.
Group A displayed significant enhancements in external rotation, internal rotation, and forward flexion range of motion at the 24-month postoperative assessment compared to preoperative values. Substantial improvements were also observed in CHD, UCLA score, ASE score, and VAS score. All associated p-values were below 0.01, indicating notable differences from the preoperative values. Similarly, in Group B, significant enhancements were noted in the range of motion for external rotation, internal rotation, and forward flexion at the 24-month postoperative review compared to preoperative values. Significant improvements were also detected in CHD, UCLA score, ASES score, and VAS score. The p-values for these measurements were less than 0.01, indicating significant variances from the preoperative values. Notably, the changes in CHD between preoperative and postoperative assessments were minimal due to the absence of coracoplasty (Table 2).
Both groups showed a substantial increase in functional scores postoperatively compared to preoperative values (p < 0.01). The p-values for all parameters, except for the forward flexion motion range, were less than 0.01 when comparing the two groups. A marked statistical difference was observed in the enhancements in external rotation range of motion, internal rotation range of motion, CHD, UCLA score, ASES score, and VAS score between the two groups (p < 0.01) (Table 3). Based on the statistical analysis, patients in Group A exhibited better recovery outcomes than those in Group B, except for the forward flexion range of motion.
Discussion
Shoulder impingement syndrome encompasses three specific types: subacromial impingement, subcoracoid impingement, and internal impingement12,17,18. However, clinical comprehension of shoulder impingement often remains limited, with these various impingement forms occasionally combined and treated as subacromial impingement. There is currently a growing body of research focusing on the pathology of subscapularis tendon tears and related risk factors. Friedman et al.11 originally introduced the concept of CHD, which denotes the minimal distance between the coracohumeral apex and the minor tubercle of the humerus measured by MRI in the internal rotation position of the shoulder joint. They noted that healthy individuals have an average CHD of about 10 mm, while patients exhibiting coracoid impingement symptoms have an average CHD of 5.5 mm. Richards et al.19 further emphasized the strong association between a narrowed subcoracoid space and subscapularis tendon injuries. Ting DS et al.20 found that the typical subcoracoid space ranges from 8 to 11 mm and established a relationship between subscapularis tendon injuries due to coracoid impingement and the decrease in CHD. Moreover, Dugarte et al.21 pointed out that the CHD decreases as the internal rotation angle of the shoulder joint increases, experiencing a significant drop when internal rotation exceeds 45°. Bone contact commonly occurs with internal rotation between 50° and 60°. The reduction in CHD significantly raises the risk of friction between the coracoid and the subscapularis tendon, leading to further damage, such as partial or full-thickness tears within the subscapularis tendon. Therefore, restoring an adequate subcoracoid space not only improves the surgical field but also protects the repaired subscapularis tendon, preventing re-tearing due to coracoid impingement and related abrasive influences22.
In this study, preoperative MRI measurements in Group A indicated a mean coracohumeral distance (CHD) range of 5.21 ± 0.48. Following coracoplasty, the coracohumeral distance showed a mean range of 9.41 ± 0.7 at the 24-month postoperative follow-up, which was statistically significant. However, the specific role of CHD as a research indicator for subcoracoid impingement still necessitates further discussion and research4. In Group A, all 40 patients underwent coracoplasty during the operation, enabling complete release of the anterior compartment of the subscapularis tendon down to the base of the coracoid process and the associated tendon. The assessment of the CHD was conducted with the shoulder joint in an internal rotation position, with measurements exceeding 8 mm from the base of the coracoid process to the target coracohumerus, utilizing a 4.0 mm grinding head as the reference scale. Moreover, the outcomes indicated that patients in Group A, who received subscapularis tendon repair combined with coracoplasty, demonstrated superior UCLA, ASES, and VAS scores at the 24-month postoperative assessment compared to Group B, which underwent isolated subscapularis tendon repair. Notably, no instances of re-tearing were noted in Group A during the follow-up period, while one incidence of re-tear was recorded in Group B. Nonetheless, attributing the re-tear definitively to the lack of the coracoplasty in Group B is challenging due to the relatively small sample size and brief follow-up duration. In terms of external rotation and internal rotation, both groups exhibited an increase in external rotation angle postoperatively compared to preoperative values, with no statistically significant differences at 1 month after the operation. This observation may be ascribed to the standard 4 weeks of postoperative immobilization. However, at the 24-month follow-up, the group that underwent subscapularis tendon repair combined with coracoplasty displayed a notable enhancement in external and internal rotation compared to the group that underwent isolated subscapularis tendon repair. Furthermore, there was no notable difference in the range of forward flexion motion between the two groups at the 24-month postoperative assessment. Overall, the functional scores displayed a remarkable improvement in both groups postoperatively compared to the preoperative values (p < 0.01). Based on the statistical analyses of each parameter, it appears that patients in Group A achieved better recovery outcomes than those in Group B, except for the forward flexion range of motion.
The evaluation of subscapularis tendon injuries during arthroscopy commonly involves two prominent classification systems: the Fox and Romeo classification14 and the Lafosse classification15. The Fox and Romeo classification, established in 2003, categorizes subscapularis tendon injuries into four types based on tear severity: Type I signifies partial tears, Type II represents tears exceeding 25% full-thickness, Type III indicates tears exceeding 50% full-thickness, and Type IV denotes a complete tear of the subscapularis tendon. On the other hand, the Lafosse classification, introduced in 2007, characterizes subscapularis tendon injuries into five categories based on tear location and associated factors: Type I involves partial tears in the upper third of the tendon, Type II denotes a complete tear in the upper third of the tendon, Type III signifies a complete tear in the upper two-thirds of the tendon with no tear in the lower third and limited tendon retraction, Type IV indicates a complete tear of the tendon from the lesser tuberosity with fat infiltration grade 3 or lower and the humeral head remaining centered without touching the coracoid during external rotation. Finally, Type V represents a complete tendon tear with the humeral head displaced forward and upward, contacting the coracoid, along with fat infiltration grade 3 or higher. In this specific study, the Lafosse classification was applied, revealing 46 cases of Type I, 26 cases of Type II, and 8 cases of Type III. Further in-depth research is required for an effective analysis of these subtypes in future studies, given the primary focus on comparing the impact of coracoplasty on subscapularis tendon repair prognosis.
In 2002, Burkhart23 initially introduced arthroscopic subscapularis tendon repair surgery. This technique has garnered attention from arthroscopic surgeons for subscapularis tendon injuries. Currently, the dominant surgical techniques include single-row fixation, double-row fixation, and tendon transfers involving various muscles24. Lorbach et al.25 highlighted that the double-row fixation approach offers superior biomechanical properties and clinical outcomes compared to single-row fixation. However, there are dissenting viewpoints as well. Yoon et al.26 suggested that, for patients with good muscle quality, there is no significant difference in treatment outcomes between the two fixation methods. In this study, despite employing single-row fixation or simple suture repair and ligamentous fixation methods, only one case experienced re-tearing among all 80 patients during the follow-up period. Consequently, whether double-row fixation or tendon transfers yield better clinical outcomes for subscapularis tendon injuries remains inconclusive.
In conclusion, subcoracoid impingement syndrome could potentially play a significant role in the development of subscapularis tendon injuries. The combined approach of subscapularis tendon repair and coracoplasty demonstrates superior efficacy compared to isolated subscapularis tendon repair for cases of subscapularis tendon injuries caused by coracoid impingement. Nonetheless, it is crucial to acknowledge the limitations of this study, including a relatively small sample size and a short follow-up duration. These findings may serve as a fundamental reference for arthroscopic shoulder surgeons; however, further research in this field is warranted for broader clinical applicability.
Data availability
The datasets generated and analyzed during the current study are not publicly available due to ethical restrictions regarding patient data and anonymity, but may be available from the corresponding author upon reasonable request.
Abbreviations
- UCLA:
-
University of California Los Angeles
- ASES:
-
American shoulder and elbow surgeons
- VAS:
-
Visual analog scale
- CHD:
-
Coracohumeral distance
References
Lappin, M., Gallo, A., Krzyzek, M., Evans, K. & Chen, Y. T. Sonographic findings in Subcoracoid Impingement Syndrome: a Case Report and Literature Review. PM R: J. Injury Function Rehabilitation. 9, 204–209 (2017).
Tamborrini, G. & Müller, A. M. [CME Sonography 103: Subacromial Pain Syndrome (SAPS) and Subcoracoid Impingement (SCI)]. Praxis 111, 113–121 (2022).
Garofalo, R. et al. Subcoracoid impingement syndrome: a painful shoulder condition related to different pathologic factors. Musculoskelet. Surg. 95 (Suppl 1), S25–29 (2011).
Park, J. Y., Lhee, S. H., Oh, K. S., Kim, N. R. & Hwang, J. T. Is arthroscopic coracoplasty necessary in subcoracoid impingement syndrome? Arthroscopy: J. Arthroscopic Relat. Surg. : Official Publication Arthrosc. Association North. Am. Int. Arthrosc. Association. 28, 1766–1775 (2012).
Ayanoğlu, T. et al. Is routine coracoplasty necessary in isolated subscapularis tears? Eklem Hastaliklari ve Cerrahisi = Joint Dis. Relat. Surg. 30, 112–116 (2019).
El-Amin, S. F. 3rd et al. Coracoid impingement and morphology is Associated with fatty infiltration and rotator cuff tears. J. Clin. Med. 11 (2022).
Lo, I. K., Parten, P. M. & Burkhart, S. S. Combined subcoracoid and subacromial impingement in association with anterosuperior rotator cuff tears: an arthroscopic approach. Arthroscopy: J. Arthroscopic Relat. Surg. : Official Publication Arthrosc. Association North. Am. Int. Arthrosc. Association. 19, 1068–1078 (2003).
Stokes, D. A., Savoie, F. H., Field, L. D., Ramsey, J. R. & rd, & Arthroscopic repair of anterior glenohumeral instability and rotator interval lesions. Qld. Gov. Min. J. 34, 529–538 (2003).
Kucukciloglu, Y. & Aydın, D. Relationship between Radiological Measurement of Subcoracoid Impingement and Subscapularis Tendon Lesions. Clin. Orthop. Surg. 14, 441–449 (2022).
Cavaggion, C. et al. Reliability of coracohumeral distance and subcoracoid tendons in subacromial pain syndrome. Sci. Rep. 13, 2383 (2023).
Friedman, R. J., Bonutti, P. M. & Genez, B. Cine magnetic resonance imaging of the subcoracoid region. Orthopedics 21, 545–548 (1998).
Horowitz, E. H. & Aibinder, W. R. Shoulder impingement syndrome. Phys. Med. Rehabil. Clin. North Am. 34, 311–334 (2023).
Çetinkaya, M. et al. Is it the subcoracoid impingement or the subacromial impingement that tears the subscapularis tendon? A comparison of the MRI findings of the operated and healthy shoulders of the patients. Turk. J. Med. Sci. 53, 273–281 (2023).
Dyrna, F. et al. A superolaterally placed Anchor for Subscapularis leading-Edge Refixation: a Biomechanical Study. Arthroscopy-the J. Arthroscopic Relat. Surg. 35, 1306– (2019).
Lafosse, L. et al. Structural integrity and clinical outcomes after arthroscopic repair of isolated subscapularis tears. J. Bone Joint Surgery-American Volume. 89a, 1184–1193 (2007).
Ghasemi, S. A. et al. Subscapularis tear classification implications regarding treatment and outcomes: consensus decision-making. JSES Rev. Rep. Tech. 3, 201–208 (2023).
Sharma, S. et al. Progressive Resistance Exercises plus Manual Therapy Is Effective in Improving Isometric Strength in Overhead Athletes with Shoulder Impingement Syndrome: A Randomized Controlled Trial. BioMed Res. Int. 9945775 (2021).
Moslehi, M., Letafatkar, A. & Miri, H. Feedback improves the scapular-focused treatment effects in patients with shoulder impingement syndrome. Knee Surg. Sports Traumatol. Arthroscopy: Official J. ESSKA. 29, 2281–2288 (2021).
Richards, D. P., Burkhart, S. S. & Campbell, S. E. Relation between narrowed coracohumeral distance and subscapularis tears. Arthroscopy: J. Arthroscopic Relat. Surg. : Official Publication Arthrosc. Association North. Am. Int. Arthrosc. Association. 21, 1223–1228 (2005).
Ting, D. S., Yang, J. L., Lin, K. H., Wang, T. G. & Lin, J. J. Alteration in coracohumeral ligament and distance in people with symptoms of subcoracoid impingement. BMC Musculoskelet. Disord. 24, 58 (2023).
Dugarte, A. J., Davis, R. J., Lynch, T. S., Schickendantz, M. S. & Farrow, L. D. Anatomic study of Subcoracoid morphology in 418 shoulders: potential implications for Subcoracoid Impingement. Orthop. J. Sports Med. 5, 2325967117731996 (2017).
Seo, J. B., Kim, S. J., Ham, H. J., Kwak, K. Y. & Yoo, J. New predictors for subscapularis tear: Coraco-lesser tuberosity angle, lesser tuberosity angle, and lesser tuberosity height. Orthop. Traumatol. Surg. Research: OTSR. 106, 45–51 (2020).
Burkhart, S. S. & Tehrany, A. M. Arthroscopic subscapularis tendon repair: technique and preliminary results. Arthroscopy: J. Arthroscopic Relat. Surg. : Official Publication Arthrosc. Association North. Am. Int. Arthrosc. Association. 18, 454–463 (2002).
Leite, M. J. et al. Coracoid morphology and humeral version as risk factors for subscapularis tears. J. Shoulder Elbow Surg. 29, 1804–1810 (2020).
Lorbach, O. et al. Reconstruction of 25 and 50% subscapularis tears: a single anchor with a double-mattress suture is sufficient for the reconstruction. Knee Surg. Sports Traumatol. Arthroscopy: Official J. ESSKA. 24, 3855–3862 (2016).
Yoon, J. S., Kim, S. J., Choi, Y. R., Kim, S. H. & Chun, Y. M. Arthroscopic repair of the isolated Subscapularis full-thickness tear: single- Versus double-row suture-bridge technique. Am. J. Sports Med. 47, 1427–1433 (2019).
Acknowledgements
The authors would like to thank all staff members in the participating departments.
Funding
This study was supported by Grants from the Anhui Key Clinical Speciality Construction Project, The Basic and Clinical Cooperative Research Promotion Program of the Third Affiliated Hospital of Anhui Medical University (2022sfy007), and The Key Research and Development Plan of Anhui Province (no. 202104j07020057).
Author information
Authors and Affiliations
Contributions
HLZ and RDN designed and conducted the study and wrote the manuscript. YLL, BZT and GC collected and analyzed the data. RDN reviewed and edited the manuscript. All authors read and approved the final version.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval and consent to participate
This study was conducted in accordance with the ethical standards set forth in the Declaration of Helsinki and its later amendments or comparable ethical standards. All procedures involving human participants were approved by the Ethics Committee of The Third Affiliated Hospital of Anhui Medical University. The ethics approval number for this study is 2024-064-02, and the registration date is April 29, 2024.In this retrospective study, written informed consent was obtained from all patients included.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Zheng, H., Liu, Y., Tu, B. et al. Analysis of the therapeutic efficacy of arthroscopic repair of the subscapularis tendon combined with coracoplasty. Sci Rep 15, 1563 (2025). https://doi.org/10.1038/s41598-025-85925-z
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-85925-z
