
Abstract
We have reported that the FAN score, which consists of the fibrosis-4 (Fib-4) index, albumin–bilirubin (ALBI) score, and neutrophil–lymphocyte ratio (NLR), is a prognostic marker for patients receiving pembrolizumab for mUC. However, it remains unclear whether the FAN score is a prognostic factor for platinum-based first-line chemotherapy. We included 126 patients with mUC who received platinum-based first-line chemotherapy. The median PFS and overall survival (OS) were 6.3 months (95% confidence interval [CI] 4.5–8.0) and 14.0 months (95% CI 11.1–16.9), respectively. Multivariable analysis showed that Fib-4 index (HR 3.85, 95% CI 1.09–13.58, p = 0.036), ALBI score (HR 1.53, 95% CI 1.01–2.31, p = 0.045), and NLR (HR 1.76, 95% CI 1.14–2.71, p = 0.010) were independently associated with PFS. The FAN score was also associated with PFS (HR 2.56, 95% CI 1.62–4.05, p < 0.001). The median PFS for patients with low FAN score (≤ 1) and those with high FAN score (≥ 2) were 7.8 (95% CI 5.0–9.0) months and 3.0 (95% CI 1.6–5.8) months, respectively. In conclusion, the FAN score is a prognostic factor for mUC patients who are treated with platinum-based first-line chemotherapy.
Similar content being viewed by others
Introduction
Platinum-based chemotherapy has long been used as first line chemotherapy for metastatic urothelial carcinoma (mUC), with the efficacy of M-VAC (methotrexate, vinblastine, doxorubicin and cisplatin) therapy reported in 19981, and GC (gemcitabine and cisplatin) therapy in 20002. Based on the results of the EV-1013, EV-302/KEYNOTE-A394, and CheckMate 9015 trials, treatment regimens including immune checkpoint inhibitors(ICI) such as enfortumab vedotin (EV) plus pembrolizumab combination therapy or gemcitabine/cisplatin/nivolumab combination therapy will become the mainstream for first line therapy for metastatic urothelial carcinoma. The limited number of patients who are ineligible for EV or ICI will receive platinum-based chemotherapy without ICI as first-line therapy. Clinical trials of ICI and EV are being conducted as perioperative treatment for muscle-invasive bladder cancer6,7. If perioperative treatment shifts from platinum-based chemotherapy to ICIs and EVs in the future, platinum-based chemotherapy may be used as treatment for patients with recurrent disease after radical cystectomy. Thus, platinum-based chemotherapy is expected to continue to play a role in the treatment of patients with metastatic urothelial carcinoma, and predicting its efficacy and prognosis is clinically important.
We reported that the FAN score, consisting of the fibrosis-4 (Fib-4) index, albumin–bilirubin (ALBI) score, and neutrophil–lymphocyte ratio (NLR) is a prognostic marker for patients receiving pembrolizumab as second-line therapy for advanced urothelial carcinoma8. However, whether the FAN score and its component factors are prognostic factors for patients receiving platinum-based first-line chemotherapy remains unclear.
The aim of this study was to identify factors associated with prognosis in patients receiving first-line platinum-based chemotherapy for mUC and to determine if their prognosis is stratified by FAN score.
Patients and methods
Study design and patients
This is a single-center, retrospective study. Patients who received first line systemic chemotherapy including platinum agents for metastatic urothelial carcinoma from January 2006 to December 2022 at Osaka University Hospital were included.
Treatment
Gemcitabine plus cisplatin (GC) or gemcitabine plus nedaplatin (GN) were administered as first-line chemotherapy. GC is the standard treatment, but patients who were unfit for cisplatin due to renal insufficiency or other reasons were treated with GN. In case of patients with renal dysfunction (30≦eGFR < 50), GC with cisplatin reduced to 75% dose or full dose GN was given, with the choice left to the attending physician. The protocol for GC is as follows; gemcitabine 1,000 mg/m2 on days 1, 8 and cisplatin 70 mg/m2 on day 2 and the treatment cycle was repeated every 3 weeks. The protocol for GN is as follows; gemcitabine 1,000 mg/m2 on days 1, 8 and nedaplatin 70 mg/m2 on day 2 and the treatment cycle was repeated every 3 weeks.
Data collection
Patient information, including laboratory examination results, was evaluated at the start of first-line platinum-based chemotherapy. Information on age, gender, Eastern Cooperative Oncology Group performance status (ECOG PS), primary site (bladder or upper urinary tract), metastatic site, chemotherapy regimen, hemoglobin level, serum albumin, serum bilirubin, serum aspartate aminotransferase (AST), serum alanine aminotransferase (ALT), estimated glomerular filtration rate (eGFR)9, neutrophil count, lymphocyte count, were collected from medical records. The albumin–bilirubin (ALBI) score is reported as a measure of liver function that can be easily calculated using the following formula: log10 (T-bil [mg/dL] × 17.1) × 0.66 + albumin [mg/dL] × 10(− 0.085)10. The fibrosis-4 (Fib-4) index has been reported as a indicator to predict liver fibrosis and is calculated by the following formula: age (years) × AST (U/L) / (platelet count [103/ μL] × (ALT [U/L]0.5)11. The neutrophil–lymphocyte ratio (NLR) was calculated using the formula: neutrophil count/ lymphocyte count. Cutoff values for the following parameters were determined based on previous reports: Fib-4 index > 3.512, ALBI score > − 2.610, and NLR > 5.013.
Progression-free survival (PFS) was calculated from the date of initiation of first line chemotherapy until radiological and clinical disease progression or last follow-up visit. Overall survival (OS) was calculated from the date of initiation of first line chemotherapy until death or last follow-up visit.
Ethical approval
This study was approved by the Institutional Review Board of Osaka University Hospital (Ethics review number: 13397–2) and conducted in accordance with the principles of the Declaration of Helsinki. Informed consent was obtained from all patients for data collection.
Statistical analysis
The PFS and OS rates were calculated using the Kaplan–Meier method and the log-rank test was used in survival analysis. A multivariable analysis was performed to determine factors associated with PFS and OS using Cox proportional hazard models. Sex, ECOG PS, primary site (bladder or upper urinary tract), hemoglobin level, eGFR, chemotherapy regimen, presence of visceral (lung, liver, bone) metastasis, Fib-4 index, ALBI score and NLR were included as variables. Age was not included as a variable in the multivariable analysis because it was included in the formula for calculating the ALBI score. In the multivariable analysis, the Fib-4 index, ALBI score, and NLR were included as variables respectively (Model 1), as well as in a model in which they were replaced by a FAN score consisting of these three variables (Model 2). All statistical analyses were performed using JMP Pro software, version 17.0 (SAS Institute Inc., Cary, NC) and p value < 0.05 was considered to indicate a statistically significant difference.
Results
Patient characteristics
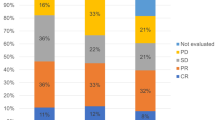
The characteristics of the 126 mUC patients included in this study are shown in Table 1. The median age was 70 (range 43–86). Ninety-one (72.2%) were male and 35 (27.8%) were female. Primary tumor sites were bladder (61 cases, 48.4%), upper urinary tract (61 cases, 49.2%) and both (3 cases, 2.4%). Seventy-seven (61.9%) were cases of recurrence or metastasis after radical surgery. Fifty-nine patients (46.8%) had visceral (lung, liver, or bone) metastases and 34 (27.0%) had only lymph node metastases. Fifty-nine patients (46.8%) had an eGFR of less than 50 ml/min/1.73 m2. Seventy-seven patients (61.1%) received gemcitabine/cisplatin and 49 (38.9%) received gemcitabine/nedaplatin as first-line chemotherapy. Patients with Fib-4 index > 3.5, ALBI score > − 2.6, and NLR > 5.0 were 4 (3.2%), 75 (59.5%), and 36 (28.6%), respectively. FAN score consisting of Fib-4 index, ALBI score and NLR was 0 in 41 cases (32.5%), 1 in 56 cases (44.4%), 2 in 28 cases (22.2%) and 3 in 1 case (0.8%). As post-treatment after first-line chemotherapy, 42 (33.3%) patients received immune checkpoint inhibitors, 5 (4.0%) patients received enfortumab vedotin, and 32 (25.4%) patients received other chemotherapy. The median observation period was 12.2 months (range 0.5–202.9 months).
Survival outcomes
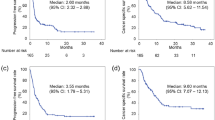
Median progression-free survival and overall survival after initiation of first-line chemotherapy in the overall cohort of 126 patients were 6.3 months (95% confidence interval [CI] 4.5–8.0) (Fig. 1A) and 14.0 months (95% CI 11.1–16.9) (Fig. 1B), respectively.

Probability estimates of the prognosis of the patients with metastatic urothelial carcinoma who were treated with platinum-based first-line chemotherapy. Probability estimates of progression-free survival (A) and overall survival (B). CI confidence interval.
Factors associated with progression-free survival
Figure 2 shows the PFS when patients are grouped by clinical factors. The GC group had a significantly better prognosis than the GN group (p = 0.046) (Fig. 2A). The eGFR ≥ 50 group tended to have a better prognosis than the eGFR < 50 group (p = 0.053) (Fig. 2B). When patients were divided into 4 groups according to both chemotherapy regimen and eGFR, the group of patients who received GC therapy with eGFR ≥ 50 had a significantly better prognosis than the other three groups, and there were no significant differences among the other three groups (Fig. 2C). The NLR ≥ 5 group had a significantly worse prognosis than the NLR < 5 group (p = 0.015) (Fig. 2D), and the ALBI ≥ -2.6 group had a significantly worse prognosis than the ALBI < -2.6 group (p = 0.027) (Fig. 2E). There were only 4 patients in the Fib-4 ≥ 3.5 group, but they tended to have a worse prognosis than those in the Fib-4 < 3.5 group (p = 0.058) (Fig. 2F). When patients were stratified into 4 groups (0, 1, 2, 3) by FAN score, there was a significant difference in prognosis except between the FAN score 0 group and the FAN score 1 group, with the group with the higher FAN score having a worse prognosis (Fig. 2G). Next, we divided patients into two groups (≤ 1, ≥ 2) by FAN score. The high FAN score (≥ 2) group had a significantly worse prognosis than the low FAN score (< 1) group (p = 0.0001), with a median PFS of 7.8 months (95% CI 5.0–9.0) and 3.0 (95% CI 1. 6–5.8) months, respectively (Fig. 2H). On the other hand, when patients were divided into two groups according to ECOG PS, presence of anemia (hemoglobin < 10 g/dl), and visceral metastasis, there was no significant difference in PFS (Supplementary Fig. 1).


Probability estimates of the progression-free survival rate by clinical factors. (A) Chemotherapy regimen, (B) eGFR, (C) Chemotherapy regimen and eGFR, (D) NLR, (E) ALBI score, (F) Fib-4 index, (G) FAN score, (H) FAN score groups. eGFR estimated Glomerular Filtration Rate, Fib-4 Fibrosis-4, ALBI albumin–bilirubin, NLR neutrophil–lymphocyte ratio.
COX regression analysis identified Fib-4 index (HR 3.85, 95% CI 1.09–13.58, p = 0.036), ALBI score (HR 1.53, 95% CI 1.01–2.31, p = 0.045) and NLR (HR 1.76, 95% CI 1.14–2.71, p = 0.010) as independent and significant factors associated with PFS (Table 2, Model 1). In a multivariable analysis including the FAN score, only the FAN score was an independent factor significantly associated with PFS (HR 2.56, 95% CI 1.62–4.05, p < 0.001) (Table 2, Model 2).
Factors associated with overall survival
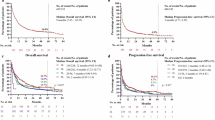
Figure 3 shows the OS when patients are grouped by clinical factors. The group with higher Fib-4 index (p < 0.0001), ALBI score (p = 0.015), and NLR (p = 0.041) had significantly shorter survival.


Probability estimates of the overall survival rate by clinical factors. (A) Chemotherapy regimen, (B) eGFR, (C) Chemotherapy regimen and eGFR, (D)NLR, (E)ALBI score, (F)Fib-4 index, (G)FAN score, (H)FAN score groups. eGFR estimated Glomerular Filtration Rate, Fib-4 Fibrosis-4, ALBI albumin–bilirubin, NLR neutrophil–lymphocyte ratio.
As with PFS, there was no significant difference in OS when patients were grouped by anemia, ECOG PS, and visceral metastases (Supplementary Fig. 2).
In multivariable analysis, Fib-4 index (HR 11.66 95% CI 3.13–43.39, p < 0.001), ALBI score (HR 1.75, 95% CI 1.15–2.68, p = 0.010), and NLR (HR 1.58, 95% CI 1.00–2.49, p = 0.049) were identified as independent factors associated with OS (Table 3, Model 1). In a model including FAN score, sex (HR 1.68, 95% CI 1.08–2.62, p = 0.023) and FAN score (HR 2.28, 95% CI 1.40–3.70, p = 0.001) was associated with OS (Table 3, Model 2).
Discussion
Various prognostic factors have been reported as predictors of outcome in patients with metastatic urothelial carcinoma receiving platinum-based chemotherapy. The most widely used model to date is the Memorial Sloan Kettering Cancer Center (MSKCC) risk score model, which is composed of two factors: Karnofsky performance status (KPS) and presence of visceral metastases14. Apolo AB et al.'s model, which consists of four factors: the two factors comprising the MSKCC risk score plus serum albumin and hemoglobin levels, predicted overall survival better than the MSKCC risk score15. Recently, Auvray M et al. reported that high NLR was associated with poor OS and poor PFS and predicted prognosis more easily and better than the MSK risk score16. Of these previously reported factors, only NLR was shown to be an independent factor associated with OS and PFS in this study cohort. Our cohort includes about half of the patients with upper tract urothelial carcinoma and is characterized by a high number of patients with chronic renal disease and cisplatin dose reduction or substitution with nedaplatin. These characteristics of the cohort may have been related to the differences from previous reports. Although previously reported NLR was an independent predictor of both PFS and OS in our study, the FAN score, which adds Fib-4 and ALBI to NLR, allowed for better prognostic stratification. The FAN score is considered very useful because it does not require special or invasive tests and can be calculated from common examination results.
Fib-4 index was developed as an indicator of liver fibrosis in patients with viral hepatitis11. The cutoff value of 3.5 used in this study is a previously reported level of cirrhosis12 and corresponds to the 90th percentile value in the group of patients treated with pembrolizumab in our previous study8. In the present cohort, only 4 patients (3.2%) had Fib-4 ≥ 3.5, but all of them died of cancer at an early stage and their prognosis is very poor. ALBI score was originally developed as an indicator of liver function in patients with hepatocellular carcinoma10. The cutoff value of − 2.6 is widely used17, and this value was also used for the FAN score.
In creating the FAN score, Fib-4, ALBI, and NLR were all used in line with previous reports, with no special cutoff values for prognostic prediction of platinum-based first-line chemotherapy for urothelial carcinoma. Furthermore, the FAN score is versatile and valuable because a common prognostic model can be used with pembrolizumab therapy as second-line treatment.
Among the components of the FAN score, NLR reflects systemic inflammation and has been reported to be prognostically relevant in various cancer types18. In a meta-analysis, pre-treated NLR was significantly associated with oncological outcome in TURBT for non-muscle invasive bladder cancer, radical cystectomy for muscle invasive bladder cancer, radical nephroureterectomy for UTUC, and chemotherapy for advanced urothelial carcinoma19. It has been reported that inflammation is associated with the development and progression of cancer and that there is a complex interaction between local immune responses of tumors and systemic inflammation20. Even in mUC patients receiving platinum-based chemotherapy, NLR reflects tumor-promoting inflammation and may be prognostically relevant.
The Fib-4 index and ALBI score, indicators of liver function, have been reported to be associated with prognosis in patients receiving immunotherapy and molecular targeted therapy in hepatocellular and colorectal cancer21,22. The Albumin-bilirubin score is also associated with cancer-related cachexia in colorectal cancer patients23 and is presumed to reflect cachexia in patients with mUC. Cancer-associated cachexia is caused by upregulation of systemic inflammation and catabolism, including in adipose and liver tissue, resulting in inhibition of protein synthesis. The Fib-4 index, and ALBI score reflect cancer-related cachexia, which is presumably associated with poor physical function and intolerance to chemotherapy and was a poor prognostic factor.
Nedaplatin was used as an alternative for patients with cisplatin unfit in this study. Nedaplatin is a cisplatin analog developed in Japan to reduce cisplatin toxicity24,25. In advanced urothelial carcinoma, its efficacy has been reported in combination with gemcitabine and paclitaxel/ifosfamide26,27,28, and it has been shown to cause less renal dysfunction than cisplatin29. However, there are no reports of sufficient numbers of cases of GN therapy as first-line treatment for advanced urothelial carcinoma. The median PFS and OS of the 49 patients who received GN therapy in this study were 4.9 and 11.1 months, respectively, worse than those who received GC therapy. However, in multivariable analysis nedaplatin use was not an independent prognostic factor for both PFS and OS. Based on these results, GN therapy may be a promising first-line treatment option for cisplatin-unfit patients.
There are several limitations in this study. First, it is a retrospective study with a limited number of cases. Since the choice of reduced-dose cisplatin or nedaplatin was left to the attending physician in patients with chronic renal disease, it is possible that factors other than those collected in this study may have influenced the choice of drug and thus the prognosis. Second, in this study, nedaplatin, rather than the widely used carboplatin, was used as an alternative platinum agent for patients with cisplatin unfit. Further studies are needed to determine whether the FAN score is a predictor of prognosis in patients receiving gemcitabine plus carboplatin therapy as well. Furthermore, since most cases are from the era before the availability of immune checkpoint inhibitors and EV as post-treatment, only a few patients have received these therapies. Therefore, factors related to overall survival may not be applicable to patients receiving current therapy. However, the FAN score was originally found as a prognostic factor for patients receiving pembrolizumab as second-line therapy, and it is at least useful for predicting prognosis up to and including first-line platinum-based therapy and second-line ICI therapy. It remains to be elucidated whether the FAN score or its components are related to the prognosis of patients receiving EV plus pembrolizumab as a novel first-line therapy or EV as a third-line therapy.
Conclusion
The FAN score consisting of fibrosis-4 index, albumin-bilirubin score and neutrophil–lymphocyte ratio, predicts prognosis of mUC patients who are treated with platinum-based first-line chemotherapy.
Data availability
Detailed data were generated at Osaka University. Derived data supporting the results of this study are available upon request from the corresponding author.
References
Sternberg, C. N. et al. Preliminary results of M-VAC (methotrexate, vinblastine, doxorubicin and cisplatin) for transitional cell carcinoma of the urothelium. J. Urol. 133, 403–407. https://doi.org/10.1016/s0022-5347(17)48996-8 (1985).
von der Maase, H. et al. Gemcitabine and cisplatin versus methotrexate, vinblastine, doxorubicin, and cisplatin in advanced or metastatic bladder cancer: Results of a large, randomized, multinational, multicenter, phase III study. J. Clin. Oncol. 18, 3068–3077. https://doi.org/10.1200/JCO.2000.18.17.3068 (2000).
O’Donnell, P. H. et al. Enfortumab vedotin with or without pembrolizumab in cisplatin-ineligible patients with previously untreated locally advanced or metastatic urothelial cancer. J. Clin. Oncol. 41, 4107–4117. https://doi.org/10.1200/JCO.22.02887 (2023).
Powles, T. et al. Enfortumab vedotin and pembrolizumab in untreated advanced urothelial cancer. N. Engl. J. Med. 390, 875–888. https://doi.org/10.1056/NEJMoa2312117 (2024).
van der Heijden, M. S. et al. Nivolumab plus gemcitabine-cisplatin in advanced urothelial carcinoma. N. Engl. J. Med. 389, 1778–1789. https://doi.org/10.1056/NEJMoa2309863 (2023).
Powles, T. et al. Perioperative durvalumab with neoadjuvant chemotherapy in operable bladder cancer. N. Engl. J. Med. 391, 1773–1786. https://doi.org/10.1056/NEJMoa2408154 (2024).
Galsky, M. D. et al. Perioperative pembrolizumab therapy in muscle-invasive bladder cancer: Phase III KEYNOTE-866 and KEYNOTE-905/EV-303. Future Oncol. 17, 3137–3150. https://doi.org/10.2217/fon-2021-0273 (2021).
Kawashima, A. et al. FAN score comprising fibrosis-4 index, albumin-bilirubin score and neutrophil–lymphocyte ratio is a prognostic marker of urothelial carcinoma patients treated with pembrolizumab. Sci. Rep. 11, 21199. https://doi.org/10.1038/s41598-021-00509-x (2021).
Matsuo, S. et al. Revised equations for estimated GFR from serum creatinine in Japan. Am. J. Kidney Dis. 53, 982–992. https://doi.org/10.1053/j.ajkd.2008.12.034 (2009).
Johnson, P. J. et al. Assessment of liver function in patients with hepatocellular carcinoma: A new evidence-based approach-the ALBI grade. J. Clin. Oncol. 33, 550–558. https://doi.org/10.1200/JCO.2014.57.9151 (2015).
Sterling, R. K. et al. Development of a simple noninvasive index to predict significant fibrosis in patients with HIV/HCV coinfection. Hepatology 43, 1317–1325. https://doi.org/10.1002/hep.21178 (2006).
Butt, A. A. et al. Liver fibrosis progression in hepatitis C virus infection after seroconversion. JAMA Intern. Med. 175, 178–185. https://doi.org/10.1001/jamainternmed.2014.6502 (2015).
Khaki, A. R. et al. A new prognostic model in patients with advanced urothelial carcinoma treated with first-line immune checkpoint inhibitors. Eur. Urol. Oncol. 4, 464–472. https://doi.org/10.1016/j.euo.2020.12.006 (2021).
Bajorin, D. F. et al. Long-term survival in metastatic transitional-cell carcinoma and prognostic factors predicting outcome of therapy. J. Clin. Oncol. 17, 3173–3181. https://doi.org/10.1200/JCO.1999.17.10.3173 (1999).
Apolo, A. B. et al. Prognostic model for predicting survival of patients with metastatic urothelial cancer treated with cisplatin-based chemotherapy. J. Natl. Cancer Inst. 105, 499–503. https://doi.org/10.1093/jnci/djt015 (2013).
Auvray, M. et al. Prognostic value of baseline neutrophil-to-lymphocyte ratio in metastatic urothelial carcinoma patients treated with first-line chemotherapy: A large multicenter study. Clin. Genitourin. Cancer 15, e469–e476. https://doi.org/10.1016/j.clgc.2016.10.013 (2017).
Hiraoka, A. et al. Validation and potential of albumin-bilirubin grade and prognostication in a nationwide survey of 46,681 hepatocellular carcinoma patients in Japan: The need for a more detailed evaluation of hepatic function. Liver Cancer 6, 325–336. https://doi.org/10.1159/000479984 (2017).
Templeton, A. J. et al. Prognostic role of neutrophil-to-lymphocyte ratio in solid tumors: A systematic review and meta-analysis. J. Natl. Cancer Inst 106, dju124, https://doi.org/10.1093/jnci/dju124 (2014).
Suh, J. et al. Clinical significance of pre-treated neutrophil-lymphocyte ratio in the management of urothelial carcinoma: A systemic review and meta-analysis. Front. Oncol. 9, 1365. https://doi.org/10.3389/fonc.2019.01365 (2019).
Diakos, C. I., Charles, K. A., McMillan, D. C. & Clarke, S. J. Cancer-related inflammation and treatment effectiveness. Lancet Oncol. 15, e493-503. https://doi.org/10.1016/S1470-2045(14)70263-3 (2014).
Watanabe, D. et al. Association of albumin-bilirubin score in patients with colorectal cancer receiving later-line chemotherapy with regorafenib. Int. J. Clin. Oncol. 26, 1257–1263. https://doi.org/10.1007/s10147-021-01910-2 (2021).
Lee, P. C. et al. Predictors of response and survival in immune checkpoint inhibitor-treated unresectable hepatocellular carcinoma. Cancers (Basel). https://doi.org/10.3390/cancers12010182 (2020).
Koh, H. H. & Kang, J. ASO Author Reflections: Albumin–Bilirubin grade and myosteatosis as potential cancer cachexia-related indicators in patients with colorectal cancer. Ann. Surg. Oncol. 29, 3877–3878. https://doi.org/10.1245/s10434-022-11489-1 (2022).
Kameyama, Y. et al. Nephrotoxicity of a new platinum compound, 254-S, evaluated with rat kidney cortical slices. Toxicol. Lett. 52, 15–24. https://doi.org/10.1016/0378-4274(90)90161-e (1990).
Niioka, T. et al. Pharmacokinetics of low-dose nedaplatin and validation of AUC prediction in patients with non-small-cell lung carcinoma. Cancer Chemother. Pharmacol. 59, 575–580. https://doi.org/10.1007/s00280-006-0298-2 (2007).
Kitamura, H. et al. Paclitaxel, ifosfamide, and nedaplatin as second-line treatment for patients with metastatic urothelial carcinoma: A phase II study of the SUOC group. Cancer Sci. 102, 1171–1175. https://doi.org/10.1111/j.1349-7006.2011.01909.x (2011).
Matsumoto, K. et al. Gemcitabine plus nedaplatin as salvage therapy is a favorable option for patients with progressive metastatic urothelial carcinoma after two lines of chemotherapy. Asian Pac. J. Cancer Prev. 16, 2483–2487. https://doi.org/10.7314/apjcp.2015.16.6.2483 (2015).
Kobayashi, K. et al. Clinical significance of a second-line chemotherapy regimen with paclitaxel, ifosfamide and nedaplatin for metastatic urothelial carcinoma after failure of cisplatin-based chemotherapy. Jpn. J. Clin. Oncol. 46, 775–780. https://doi.org/10.1093/jjco/hyw071 (2016).
Nagasawa, M. et al. Changes in renal function following nedaplatin-containing chemotherapy in patients with urothelial carcinoma unfit for cisplatin. Oncol. Lett. 17, 2551–2556. https://doi.org/10.3892/ol.2018.9859 (2019).
Author information
Authors and Affiliations
Contributions
Y.I. contributed to data collection and analysis, table and figure preparation, reference collection, and manuscript writing. Y.I. and A.K. contributed to the data collection and analysis and supervised all activities. Y.H., A.Y., M.T., A.Y., L.Y., S.N., T.O., Y.O., T.U., G.Y., T.H., Y.Y., T.K., K.H., and N.N. supervised all the activities. The first draft of the manuscript was prepared by Y.I. and A.K. All authors have read and approved the published version of the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Ishizuya, Y., Kawashima, A., Horibe, Y. et al. FAN score predicts prognosis after platinum-based first-line chemotherapy in patients with metastatic urothelial carcinoma. Sci Rep 15, 4640 (2025). https://doi.org/10.1038/s41598-025-86212-7
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-86212-7
