
Abstract
This investigation aimed to develop a radiographic 3D cephalometric index to grade severity of dentofacial deformity in patients with juvenile idiopathic arthritis (JIA), and to perform a validation against expert evaluations. Data were collected from a population-based Nordic JIA cohort of 240 patients that received a cone-beam computed tomography (CBCT) scan approximately 17 years after onset of JIA. The cohort was randomized into two groups: A baseline group for establishing the index (n = 210) and a test group (n = 30). The standardized index generation process led to the inclusion of six radiographic outcome measures, each representing different facets of dentofacial deformities. Specific severity scores were established for three domains; dentofacial asymmetry (0–8), vertical deviation (0–8), and sagittal deviation (0–8). An overall dentofacial deformity index score was computed by aggregating the scores from the six variables, with the total score ranging from 0 to 24. The validity of the index was assessed by comparing the index score with expert evaluations. Based on the generated index, 10 patients exhibited severe deformities. Reliable agreement between data-generated index scores and expert assessments was found. A 3D radiographic dentofacial deformity index was generated and tested. This index can support an objective assessment of the severity of dentofacial deformities related to JIA in a clinical setting and future research.
Similar content being viewed by others

Introduction
Juvenile idiopathic arthritis (JIA) is the most prevalent rheumatic chronic disease in children. It is characterized by onset before the age of 16 years and a minimum duration of six weeks with inflammation in one or more joints. The condition can also include additional findings, such as anterior uveitis, skin rash, and fever1.
JIA frequently affects the temporomandibular joint (TMJ), with 30–43% of patients experiencing TMJ involvement on one or both sides2,3,4. This condition can lead to mandibular growth impairment, TMJ degeneration and dysfunction, dentofacial deformity and malocclusion5,6. The dentofacial deformity may include mandibular retrognathism, convexity of the profile, clockwise rotation of the mandible, steep mandibular plane angle, anterior open bite, antegonial notching, and facial asymmetry7. The severity of these findings is influenced by age of onset, arthritis severity, and genetic factors. Consistent monitoring and timely initiation of treatment are essential for effective management8.
Failure to detect underlying dentofacial deformities can lead to poor treatment outcomes, necessitating surgical interventions. Tailored treatment decisions for JIA-related dentofacial deformities can be difficult and require a precise, quantitative method for assessing dentofacial deformity severity.
The aim of the present study was to develop and validate a radiographic 3D index to grade severity of dentofacial deformity in skeletally mature patients with JIA. Such an index would facilitate objective assessment for treatment decision-making, outcome evaluation, and research stratification.
Materials and methods
Population
This study utilizes a prospective, population-based, multicenter Nordic inception cohort. The cohort comprised consecutive patients diagnosed with JIA by pediatric rheumatologists from seven centers in Denmark, Finland, Norway, and Sweden between January 1, 1997, and June 30, 2000. The inclusion criterion was a diagnosis of JIA according to International League Against Rheumatism (ILAR) criteria9. Further details regarding the cohort characteristics are described in previous articles by Berntson et al.10 and Glerup et al.11.
Patients were invited for a 17-year follow-up examination regardless of the presence of JIA-related TMJ involvement. Enrolled subjects underwent a standardized clinical orofacial examination and a cone beam computed tomography scan (CBCT) examination11. CBCT examinations were standardized by ensuring: (1) teeth in habitual occlusion with no protrusion of the mandible, and (2) large field of view, at least 12 inches11.
CBCT examinations were conducted according to the manufacters description and the regulations of the health authorities in the specific country where the radiological examination was carried out. Ethical approval was granted by national research committees in all the countries (1-10-72-280-13, 2012/2051, Dnr 2014/413-31, 174/13/03/03/2014), and the participants provided informed consent11.
Randomization and grouping
Subjects were randomly divided into a JIA baseline group for establishing the index and a JIA test group for validation using the Microsoft Excel randomizer function, ensuring unbiased allocation. To maintain participant confidentiality, the dataset was anonymized by removing personal data and replacing names with study IDs.
Assessment of dentofacial morphology
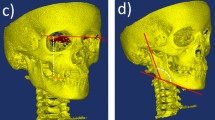
Each CBCT was assessed using a standardized and validated 3D radiographic assessment described by Stoustrup et al.12. The original radiographic evaluation consists of 21 unique outcome variables representing the different facets of JIA-related dentofacial deformity. For the present study, the following six variables, which were deemed of “high importance” by the original Stoustrup et al. study12, were used for calculation of a dentofacial deformity index: 1) total posterior mandibular height, 2) mandibular axial angle, 3) mandibular inclination, 4) posterior/anterior facial ratio, 5) mandibular sagittal position, 6) Wits appraisal13. Together, these variables describe the various aspects of JIA-related dentofacial deformities: facial asymmetry, vertical dentofacial deviation, and sagittal dentofacial deviation (Table 1, Fig. 1).

The six outcome variables in the dentofacial deformity index.
Outline of the index (data-generated index score)
The index was generated using a percentile-based grading system for each of the six outcome variables in the baseline group. Specifically, the values of the 25th percentile, the median, the 75th percentile, and 90th percentile were determined for each outcome measure. Severity scores were then assigned based on these percentiles as follows: ≤ 25th percentile = 0 points; 26th-50% percentile = 1 point; 50–75th percentile = 2 points; 76–90th percentile = 3 points; > 90th percentile = 4 points. The total dentofacial deformity index was obtained by summing all grading scores (points). An additive score of 0 indicates no dentofacial deformity, while a score of 24 represents most severe dentofacial deformity.
In addition, domain-specific severity scores for facial asymmetry, vertical deviation, and sagittal deviation were generated. The asymmetry index (range 0–8) was calculated by summing up the individual scores of the variables Total Mandibular Posterior Height and Mandibular Axial Angle. The vertical domain score (range 0–8) was captured by the variables Mandibular Inclination and Posterior/Anterior Face Ratio. The sagittal domain score (range 0–8) was captured by the variables Mandibular Sagittal Position and Wits Appraisal.
Expert assessment of dentofacial deformity (expert-index score)
An expert panel consisting of four orthodontists and two maxillofacial surgeons, with relevant clinical and research expertise, assessed the morphology of the JIA test group (n = 30). The experts conducted the assessments individually and were blinded to the measured values of the six outcome measures. CBCT-generated 3D images were presented as a 2D slide show showing the cranium in right, left, frontal, and inferior views. The expert panel was asked to address the following questions:
-
(1)
“How would you rate the degree of dentofacial deformity in this patient, in terms of asymmetry, the sagittal deviation, and the vertical deviation, on a scale from 0 (= normal) to 8 (= severe)?”
-
(2)
“How would you rate the overall dentofacial deformity of this patient on a scale from 0 (= normal) to 24 (= severe)?”
-
(3)
“How would you characterize the dentofacial deformity of this patient; normal, less severe, severe, or very severe?”
Comparing expert assessment and dentofacial deformity index
To assess the content validity of the index, the dentofacial deformity index was generated for each subject in the JIA test group and compared with expert assessment scores. In addition to the overall index score (range 0–24), the subdomain scores for asymmetry, sagittal deviation, and vertical deviation (0–8 for each) were compared with expert assessment for each subdomain.
Statistics
Dentofacial deformity index
Descriptive statistics were used to calculate the median value and 25th/75th/90th percentiles for each outcome variable. Box-plots were used to graphically display the spread of data.
Consistency of agreement
The dentofacial deformity index and the expert assessment for the test dataset was compared using a two-way mixed effects intra-class correlation coefficient (ICC) and graphical display from scatter plots. The consistency of agreement of the ICCs was assessed based on Cicchetti14: Less than 0.40: “Poor”; between 0.40 and 0.59: “Fair”; between 0.60 and 0.74: “Good”; between 0.75 and 1.00: “Excellent”.
Expert assessment of dentofacial deformity
A multi-rater two-way mixed-effects intra-class correlation coefficient model was implemented to assess the inter-rater consistency of agreement between the six experts. Descriptive statistics were used to summarize the overall severity assessment of the experts related to degree of asymmetry, vertical, and sagittal deviations, and total severity of dentofacial deformity for each case.
Results
Cohort characteristics
Of the 510 participants included in the baseline study, 420 were eligible for this study with access to CBCT at the 17-year follow-up, since 6 of 7 Swedish centers did not have CBCT available11. Of the 420 eligible participants, 155 (37%) were lost to follow-up11, and the remaining 265 (63%) were included in the present study. Of these, 240 received full-face CBCT examinations at the 17-year follow-up. The mean age of included subjects was 23.5 ± 4.2 years, and 186 (70.2%) were female. The mean duration from JIA onset to orofacial examination was 17.3 ± 1.3 years.
When comparing the included participants and those lost to follow-up, no differences were found in sex, JIA subtype, number of active joints, or baseline Juvenile Arthritis Disease Activity Score (JADAS) values. However, age at onset was lower in the included group (mean 6.0 ± 3.9 vs 6.2 ± 4.0. years in those lost to follow-up group; p = 0.003). Further descriptive characteristics can be found in Glerup et al.10.
Dentofacial deformity index calculation
Based on the the data distribution for the baseline group (n = 210) (Fig. 2) and the percentile-based values assigned (Table 2), patients were classified as follows: 0–6 points = normal; 7–12 points = minor deformity; 13–18 points = severe deformity; 19–24 points = very severe deformity (Table 3).

Distribution of data from the JIA index cohort (n = 210) for the six outcome variables included in the dentofacial deformity index. d) is the ratio between posterior and anterior face.
Expert assessment of dentofacial deformity
Inter-rater agreement between the experts based on the test dataset (n = 30) showed excellent results for all intra-correlation coefficients: Asymmetry: 0.95 (95%-CI 0.92–0.98), sagittal deviation: 0.89 (95%-CI 0.82–0.94), vertical deviation: 0.87 (95%-CI: 0.78–0.93), and total deformity index score: 0.91 (95%-CI 0.85–0.95) (Fig. S2a–c).
Consistency of agreement
ICC values for the different domains ranged between 0.63 and 0.83, corresponding to “good” or “excellent” agreement (Table 4; Fig. 3). 10 patients from the JIA test group displayed “severe” or “very severe” dentofacial deformities based on the generated index scores (Fig. 3d).

Consistency of agreement. Scatter plots depicting the agreement between the data-generated severity scores and the expert-generated severity scores in the JIA test group (n = 30) for each of the three domains (asymmetry, sagittal deviation, vertical deviation, scores 0–8) and total deformity score (0–24).
Discussion
The objective of the present study was to establish a validated dentofacial deformity index for patients with JIA. There is a need for reliable, standardized, and objective measurement of JIA-related dentofacial deformities in clinical settings and research, which the present study aims to provide.
Classification of dentofacial deformities can be difficult to standardize due to the multiple aspects in disease development and manifestation. Also, the distinction between an abnormal and a normal variance can be ambiguous. The results of the present study demonstrate that it is feasible to develop a score that reflects the severity of dentofacial deformities in patients with JIA and correlates with expert opinions.
Prior studies such as Leung and Leung have introduced a mandibular asymmetry classification using CBCT data from 65 healthy patients with mandibular asymmetry, focusing on specific anatomical regions15. Wink et al. utilized 3D-CT scans for hemifacial microsomia assessment and found only moderate inter-rater agreement16.
In our study, we utilized the Stoustrup et al. protocol for grading dentofacial deformities, assigning severity scores from 0 to –4 based on defined ranges. This method offers precision but also demands accurate measurements given the narrow grading ranges. Minor variation in the identification of landmarks can significantly impact the assigned grades. This is particularly true for measures related to the total posterior mandibular height and the mandibular axial angle where the smallest detectable differences are very small17. These limited ranges for smallest detectable differences mean that minor deviations can risk misclassification and require careful measurement during landmark detection.
Because no re-rating of the test group was performed, the intra-rater reliability was not calculated for the expert assessment. We were not able to perform a power calculation a priori due to a lack of preliminary data. Furthermore, the index does not consider if only one TMJ or both TMJs are involved. Moreover, the evaluators were presented with two-dimensional screenshots instead of complete 3D images for their assessment.
Notably, images are generated from the CBCTs of skeletally mature subjects. The applicability of the index for growing individuals remains unclear. Considering the significant changes in dentofacial morphology associated with rapid growth between ages 12–16 years, the index might require adjustments for these age groups. More specifically, due to the dynamic growth within this age range, the asymmetry scores to calculate the index might need to be adapted to the respective growth phase. Future studies could assess the applicability of the index in growing subjects18,19.
Important strengths of the present study are the large population-based cohort, the use of a standardized and validated radiological method to assess dentofacial deformity in JIA, and the inclusion of a validation process of the proposed index with expert assessment. Moreover, the index is based on 3D cephalometric measurements on CBCT images and therefore accounds for 3D data.
Future studies could refine the index by using a larger sample size and involving more experts and intra-rater assessments. Future research could also investigate whether a slight change in the score is due to a progression or normal variation. Additionally, an artificial intelligence approach could use the index as a basis to assess patients and outline individual treatment plans.
Conclusions
In the present project we present a novel 3D cephalometric index to objectively quantify dentofacial deformity in skeletally mature patients with JIA. The index integrates a series of key aspects of dentofacial deformity into a single score as well as sub-domain scores highlighting aspects of dentofacial deformity. Validated against expert evaluations, this index supports clinicians to accurately assess, classify, and track the severity of JIA-related dentofacial deformities. This standardized assessment contributes to simplified description of the severity of dentofacial deformity that may aid early diagnosis, monitoring and documentation of progression and treatment interventions, consistent clinical evaluation and comparable research results. Furthermore, future adaptation to treatment procedures can be individualized, based on cohort treatment outcome data.
Data availability
The data that support the findings of this study are not openly available due to reasons of sensitivity and are available from the corresponding author upon reasonable request.
References
Thatayatikom, A., Modica, R. & Leucio, A. De. Juvenile idiopathic arthritis. StatPearls. 2023. https://www.ncbi.nlm.nih.gov/books/NBK554605/. Accessed 14 Apr 2024.
Stoll, M. L. et al. Risk factors for temporomandibular joint arthritis in children with juvenile idiopathic arthritis. J. Rheumatol. 39(9), 1880–1887 (2012).
Glerup, M. et al. Incidence of orofacial manifestations of juvenile idiopathic arthritis from diagnosis to adult care transition: A population-based cohort study. Arthritis Rheumatol. 75(9), 1658–1667 (2023).
Cannizzaro, E., Schroeder, S., Müller, L. M., Kellenberger, C. J. & Saurenmann, R. K. Temporomandibular joint involvement in children with juvenile idiopathic arthritis. J. Rheumatol. 38(3), 510–515 (2011).
Rongo, R., Michelotti, A., Pedersen, T. K., Resnick, C. M. & Stoustrup, P. Management of temporomandibular joint arthritis in children and adolescents: An introduction for orthodontists. Orthod Craniofac. Res. 26(S1), 151–163. https://doi.org/10.1111/ocr.12676 (2023).
Murphy, M. K., MacBarb, R. F., Wong, M. E. & Athanasiou, K. A. Temporomandibular joint disorders: A review of etiology, clinical management, and tissue engineering strategies. Int. J. Oral Maxillofac Implant. 28(6), e393 (2013).
Hu, Y., Billiau, A. D., Verdonck, A., Wouters, C. & Carels, C. Variation in dentofacial morphology and occlusion in juvenile idiopathic arthritis subjects: A case–control study. Eur. J. Orthod. 31(1), 51–58. https://doi.org/10.1093/ejo/cjn085 (2009).
Stoustrup, P. et al. Management of orofacial manifestations of juvenile idiopathic arthritis: Interdisciplinary consensus-based recommendations. Arthritis Rheumatol. 75(1), 4–14 (2023).
Petty, R. E., Southwood, T. R., Manners, P., Baum, J., Glass, D. N., Goldenberg, J. [UNIFESP] et al. International league of associations for rheumatology classification of juvenile idiopathic arthritis: Second revision, Edmonton, 2001. J. Rheumatol. Publ. Co 2004. http://repositorio.unifesp.br/11600/44671
Berntson, L. et al. Incidence of juvenile idiopathic arthritis in the Nordic countries. A population based study with special reference to the validity of the ILAR and EULAR criteria. J. Rheumatol. 30(10), 2275–2282 (2003).
Glerup, M. et al. Longterm outcomes of temporomandibular joints in juvenile idiopathic arthritis: 17 Years of followup of a nordic juvenile idiopathic arthritis cohort. J. Rheumatol. 47(5), 730–738 (2020).
Stoustrup, P., Iversen, C. K., Kristensen, K. D., Resnick, C. M., Verna, C., Nørholt, S. E., et al. Assessment of dentofacial growth deviation in juvenile idiopathic arthritis: Reliability and validity of three-dimensional morphometric measures. PLoS One 13(3). https://pubmed.ncbi.nlm.nih.gov/29534095/. (2018)
Jacobson, A. The, “Wits” appraisal of jaw disharmony. Am. J. Orthod. 67(2), 125–138 (1975).
Cicchetti, D. V., Shoinralter, D., Tyrer, P. J. The effect of number of rating scale categories on levels of interrater reliability : A Monte Carlo investigation. 9(1):31–36. https://doi.org/10.1177/014662168500900103. (1985).
Leung, M. Y. & Leung, Y. Y. Three-dimensional evaluation of mandibular asymmetry: A new classification and three-dimensional cephalometric analysis. Int. J. Oral Maxillofac. Surg. 47(8), 1043–1051 (2018).
Wink, J. D. et al. Maxillary involvement in hemifacial microsomia: An objective three-dimensional analysis of the craniofacial skeleton. J. Craniofac. Surg. 25(4), 1236–1240 (2014).
Stoustrup, P. et al. Smallest detectable differences in clinical functional temporomandibular joint examination variables in juvenile idiopathic arthritis. Orthod Craniofac Res. 16(3), 137–145. https://doi.org/10.1111/ocr.12008 (2013).
Arvidsson, L. Z. et al. Craniofacial growth disturbance is related to temporomandibular joint abnormality in patients with juvenile idiopathic arthritis, but normal facial profile was also found at the 27-year follow-up. Scand J. Rheumatol. 39(5), 373–379 (2010).
Fjeld, M. G. et al. Average craniofacial development from 6 to 35 years of age in a mixed group of patients with juvenile idiopathic arthritis. Acta Odontol Scand. 67(3), 153–160 (2009).
Author information
Authors and Affiliations
Contributions
S.V. wrote the paper and contributed to data analysis. I.T. collected the data and contributed to data analysis. M.G., T.P., P.S., S.N., C.R., C.V. , T.H., C.M. , L.B. , E.N. , M.R., K.A. , A.K. conceived and designed the analysis. All authors reviewed the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Vassis, S., Glerup, M., Tambjerg, I. et al. Development of a 3D cephalometric index to grade severity of dentofacial deformity in patients with juvenile idiopathic arthritis. Sci Rep 15, 2625 (2025). https://doi.org/10.1038/s41598-025-86410-3
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-86410-3
