
Abstract
Previous studies have found that dyslipidemia is a risk factor for pancreatic cancer (PC), and that lipid-lowering drugs may reduce the risk of PC. However, it is not clear whether dyslipidemia causes PC. The Mendelian randomization (MR) study aimed to investigate the causal role of lipid traits in pancreatic cancer and to assess the potential impact of lipid-lowering drug targets on pancreatic cancer. Genetic variants associated with lipid traits and variants of genes encoding lipid-lowering drug targets were extracted from the Global Lipids Genetics Consortium genome-wide association study (GWAS). Summary statistics for PC were obtained from an independent GWAS datasets. Colocalization analyses were performed to validate the robustness of the results. No significant effect of lipid-lowering drug targets on PC risk was found. Genetic mimicry of lipoprotein lipase (LPL) was potentially associated with PC risks. Significant MR associations were observed in the discovery dataset (OR 1.64 [95% CI 1.24–2.16], p = 4.48*10–4) with PC in one dataset. However, the finding was not verified in the replication dataset. Our findings do not support dyslipidemia as a causal factor for PC. Among lipid-lowering drug targets, LPL is the potential drug target in PC.
Similar content being viewed by others


Introduction
Pancreatic cancer (PC) is one of the malignant tumors of digestive system with the worst prognosis. It has an insidious onset and rapid progression. The annual incidence is close to the annual mortality rate, and the 5-year survival rate is only 13%1. The high mortality rate is partly due to lack of effective treatments. Considering the poor survival with limited options for treatment of PC, early identification and modification of risk factors for PC in at-risk populations are warranted to lower the societal burden of this disease2.
Naudin S et al. conducted a prospective observational study and found that the prediagnostic serum lipid panel, including 43 lipids from 8 lipids and 5 fatty acids, was associated with PC. A total of 11 lipid species were positively associated with PC risk (ORs range: 1.16–1.21), while 32 lipid species were inversely associated (ORs range: 0.79–0.87)3. Previous study found that with lower total serum cholesterol, the short-term risk for PC would increase4. Despite these observational findings, epidemiological studies have methodological constraints and are subject to residual confounding. The causal relationship between dyslipidemia and the risk of PC has not been fully determined.
Considering that dyslipidemia is closely associated with PC development and severity, lipid-lowering drugs have been proposed as PC repurposing candidates (expanding the indication of approved drugs into other indications). Cai found that atorvastatin inhibits the proliferation, migration and invasion ability of human PC cells, and atorvastatin might exert the anti-tumor effect in PC via the inhibition of neurotrophins signaling pathway5. However, in 113,059 participants of two prospective cohort studies in the U.S, no difference was identified in pancreatic cancer risk for regular versus non-regular statin users6. Therefore, whether statins and other lipid-lowering drugs are effective for PC remains unclear.
Mendelian randomization (MR) is an epidemiological tool using data from genetic studies to estimate the non-confounded associations between exposures and outcomes. Important assumptions in instrumental variable analysis are that the chosen genetic variants are associated with the exposure of interest, they are not associated with any confounders, and they are not associated with the cancer outcome via any pathway other than through the exposure of interest (known as genetic pleiotropy)7. Genetic variants satisfying these three assumptions divide a study population into subgroups that are analogous to treatment arms in a randomized controlled trial, in that they differ systematically with respect to the exposure of interest, but not with respect to confounders. If all the instrumental variable assumptions are met, an association between the genetic variant and the outcome implies that the risk factor of interest has a causal effect on the outcome8.
Therefore, in this study, we conducted MR analyses to determine the effects of lipid traits on PC and to explore the potential effects of lipid-lowering drug targets on the treatment of PC.
Methods
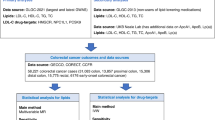
The association of lipid traits and lipid-lowering drugs with PC was examined in a population of European ancestry using MR. This study followed the Strengthening the Reporting of Observational Studies in Epidemiology-Mendelian Randomization reporting guidelines (Supplementary Table S1)9. Detailed information on the publicly available summary-level data from GWAS studies and expression quantitative trait loci (eQTL) study used in our study is summarized in Supplementary Table S2. An outline of the study design is shown in Fig. 1.

Outline of the study design. Abbreviations: LDL-C, low-density lipoprotein cholesterol; TG, triglyceride; TC, total cholesterol; PC, pancreatic cancer; SNP, single nucleotide polymorphism; MR, mendelian randomization; GWAS, genome-wide association study; ANGPTL3, angiopoietin-like 3; APOC3, Apolipoprotein C-III; LPL, lipoprotein lipase; PPARA, peroxisome proliferator activated receptor alpha; CETP, Cholesteryl ester transfer protein; LDLR, low density lipoprotein receptor; eqtl, expression quantitative trait locus.
Genetic variant selection
Independent genetic variants at genome-wide significance (p < 5e-08) associated with LDL-C, HDL-C, TG and TC (linkage disequilibrium [LD] clumping threshold of r2 < 0.001 with physical distance threshold 10,000 kb) were identified in a GWAS meta-analysis from the Global Lipids Genetics Consortium10.
According to recent guidelines for the management of dyslipidemia, common lipid-lowering drugs and novel therapeutics were selected11. Genes encoding pharmacologic targets of lipid-lowering drugs were identified using the DrugBank database (doi: go.drugbank.com/) and relevant reviews12,13. Based on the primary pharmacological action and the associations between PC and lipid traits, TG-lowering target genes and HDL-raising target genes were included in the study, that is: lipoprotein lipase (LPL), angiopoietin-like 3 (ANGPTL3), Apolipoprotein C-III (APOC3), peroxisome proliferator activated receptor alpha (PPARA) and Cholesteryl ester transfer protein (CETP) (Table 1).
Single nucleotide polymorphisms (SNPs) were identified within the corresponding genes (± 100 kb of the gene location) and were robustly associated with HDL-C or TG levels at genome-wide significance (p < 5*10–8) in a GWAS meta-analysis from the Global Lipids Genetics Consortium10.
For drug targets that reached significance for the risk of PC in the MR analysis, we used publicly available eQTLs data for blood tissues in which target genes were expressed from the eQTLGen consortium. EQTLs are genetic variants associated with expression levels of genes. SNPs, as genetic variants with a false discovery rate-corrected p value < 0.05, were selected and further clumped to an LD r2 threshold of 0.20.
Furthermore, considering that some genes encoding pharmacologic targets may affect PC risk in other ways instead of regulating lipid traits, eQTLs data for blood tissue of genes targeting lipid-lowering in eQTLGen database were collected as instrumental variables (IVs) to examine their associations with PC.
Outcome
For the outcome, summary genetic association data were extracted from a GWAS meta-analysis of PC with participants of 1196 European ancestry cases and 475,049 European ancestry controls14. For replication analyses, another PC GWAS dataset was obtained from the PanScanI (1788 cases and 1769 controls) consortia through the National Center for Biotechnology Information database of Genotypes and Phenotypes15.
Statistical analysis
The inverse-variance weighted (IVW) approach, MR-Egger regression, weighted–median method, Maximum likelihood and weighted mode were used for MR analysis. When the instrumental variables meet the three assumptions of MR and the sample size is sufficient, the IVW method can well explore the potential linear causal association between exposure and outcome. A statistically significant IVW result coupled with directionally consistent associations from all sensitivity analyses was considered sufficient evidence to claim a causal effect16,17. MR-PRESSO analysis can determine whether a single SNP has horizontal pleiotropy by calculating the distance from the fitting line calculated by removing the SNP, and comparing the results before and after removing these SNPs with horizontal pleiotropy. Thus, MR-PRESSO was used to test for horizontal pleiotropy and remove the relevant SNPs18. To test the relevance assumption, the strength of each genetic variant was assessed with F statistics analysis. Typically, an F statistic of at least 10 indicates no weak instrument bias.
In order to rule out the interaction between lipid traits, multivariate MR was further performed for lipid traits suspected to be associated with PC.
For a drug target that reached significance for risk of PC, colocalization analysis was performed for eQTLs data for blood tissue of drug targets and the corresponding regulated lipid trait GWAS to test the regulation of lipid trait by the drug target. It assessed the probability (PP.H4) that SNPs associated with the drug target and lipid traits are shared by the same causal variant at a given locus and the probability (PP.H3) that drug targets and lipid traits are affected by distinct causal variants that are in LD with each other. A posterior probability greater than 0.80 supported a tested configuration. Furthermore, to confirm that drug target genes and PC do not share genetic causal variants, colocalization analysis was performed for eQTLs data for blood tissue of drug targets and PC GWAS. It assessed the probability (PP.H2) that SNPs are only associated with the drug target in the genomic region. While SNPs in the genomic region are not associated with PC, drug targets that strongly colocalized with lipid traits (PP.H4 > 0.80) were considered to be potential target genes.
To determine whether the observed association between drug targets and PC was a direct association, the relationship between genetically proxied lipid-lowering therapies and risk factors for PC (Body Mass Index [BMI] and Type 2 diabetes [T2D]) was assessed.
The heterogeneity and pleiotropy between SNPs were evaluated by Cochran’s Q test and the MR-Egger intercept test. Bonferroni-corrected significance levels of p-value < 0.0125 (0.05/4) were used to adjust for multiple testing of four drug targets. For other analyses, an observed 2-sided p < 0.05 was considered statistically significant. All statistical analyses were conducted using the TwoSampleMR (version 0.6.4), coloc and MR-PRESSO (version 0.1.0) packages in R (version 4.4.1)19.
Results
Lipid traits and PC risk
Eighty independent SNPs associated with LDL-C, 89 SNPs associated with HDL-c, 55 SNPs associated with TG and 87 SNPs associated with TC were identified as IVs for lipid traits (Supplementary Table S3–S6). In the discovery dataset, increases in genetically proxied TG levels were associated with the decreased risk of PC (OR 0.69 [95% confidence interval (CI), 0.49–0.97]; p = 0.04) and increases in genetically proxied HDL-c levels were nominally associated with the decreased risk of PC (OR 0.82 [95% CI, 0.67–0.99]; p = 0.04) (Table 2). In the multivariate MR analysis, which included TG and HDL-C, increases in genetically proxied TG levels were nominally associated with the decreased risk of PC (OR 0.73 [95% CI, 0.55–0.96]; p = 0.02) (Supplementary Table S7). The finding was not verified in the replication dataset (TG: OR 1.05 [95% CI, 0.77–1.43], p = 0.74; HDL: OR 1.12 [95% CI, 0.81–1.53], p = 0.49) (Table 2).
Lipid-lowering drug targets and PC risk
We identified thirty-six SNPs as genetic instruments in CETP, 4 SNPs in ANGPTL3, 10 SNPs in APOC3 and 24 SNPs in LPL (Supplementary Table S8). The F statistics for the respective genetic instruments ranged from 24.2 to 2309.9, suggesting that instrument bias was unlikely to affect the analyses.
The associations of genetic proxies for the effects of four lipid-lowering drug classes on PC were shown in Fig. 2. In the discovery dataset, genetic mimicry of LPL enhancement equivalent to a 1-mmol/L (88.9 mg/dL) decrease in TG was significantly associated with higher PC risk (OR 1.64 [95% CI 1.24–2.16], p = 4.48*10–4). The genetic mimicry of APOC3 on the effect of PC risk also counted (OR 0.69 [95% CI 0.48–0.98], p = 0.04). However, this result was not statistically significant after correction by multiple tests (Bonferroni p < 0.0125). Other genetic mimicries of drug targets (CETP and ANGPTL3) were shown to have no effect on PC outcomes. In the replication dataset, this finding was close to null (OR 1.12 [95% CI 0.62–2.02], p = 0.71). But there was potential association found between CETP and PC (OR 0.61[95% CI 0.44–0.89], p = 0.004).

MR estimates of four lipid-lowering target genes on PC. (A) MR estimates of four lipid-lowering target genes on PC in the discovery dataset; (B) MR estimates of four lipid-lowering target genes on PC in the replication dataset. IVW (with 95% CI) from all the primary MR analyses are shown for the effects of LPL, APOC3, ANGPTL3, CETP. Red-filled symbols: IVW p < 0.0125. IVW, inverse variance-weighted method; LPL, lipoprotein lipase; ANGPTL3, angiopoietin-like 3; APOC3, Apolipoprotein C-III; CETP, Cholesteryl ester transfer protein.
The results of the alternative MR methods were generally consistent (Supplementary Table S9). The results of heterogeneity test also suggested no heterogeneity. MR-Egger intercept did not find evidence of pleiotropy, which improves causal inferences (Supplementary Table S10). Besides, these findings were robust in the leave-one-out sensitivity analysis (Supplementary Figure S1).
Gene expression and PC risk
Although the association was not verified in the replication dataset, LPL was found associated with PC in the discovery dataset. Also, CETP was found associated with PC in the replication dataset.
For further validation, genetic variants related to LPL expression in whole blood tissue were used as instrumental variables. Findings from the increase of LPL expression in blood tissue was associated with a higher risk of PC in the discovery dataset (blood tissue: OR 1.20 [95% CI, 1.10–1.30]; p = 9.85*10–6). In the replication dataset, there was no association found (blood tissue: OR 1.11 [95% CI, 0.95–1.30]; p = 0.19) (Table 3 & Supplementary Table S17). In addition, Findings from the increase of CETP expression in blood tissue was associated with a lower risk of PC in the replication dataset (blood tissue: OR 0.66 [95% CI, 0.45–0.98]; p = 0.04). In the discovery dataset, there was no association found (blood tissue: OR 1.17 [95% CI, 0.94–1.47]; p = 0.17) (Supplementary Table 3 & Table S17).
We further performed colocalization analyses to identify the probability that genetic variants associated with LPL expression in blood tissues and TG shared causal SNPs. LPL expression in blood tissue and TG shared a causal variant (PP.H4 = 0.916) (Supplementary Table S11). The causal variant (rs12678919) (SNP.PP.H4 > 0.95) was associated with both LPL expression in blood tissues and TG within the LPL locus (Supplementary Table S12 & Figure S2), providing evidence against the association driven by distinct SNPs that are in LD. In addition, the colocalization analyses between LPL eQTLs in blood tissue and PC showed that the genomic region was not associated with PC (PP.H2 = 0.91) (Supplementary Table S13 & Figure S3). Meanwhile, CETP expression in blood tissue and HDL shared were associated by the genomic region (PP.H4 = 0.982) (Supplementary Table S14). However, there is no causal variant (SNP.PP.H4 > 0.95) within the CETP loci (Supplementary Table S15 & Figure S4). The colocalization analyses between CETP eQTLs in blood tissue and PC showed that the genomic region was not associated with PC (PP.H2 = 0.943) (Supplementary Table S16 & Figure S5).
Considering some drug target genes encoding may affect PC risk in other ways instead of regulating lipid traits, eQTLs in blood tissue of lipid-lowing drug target genes (APOC3, ANGPTL3, PPARA, PCSK9, LDLR, HMGCR, APOB, NPC1L1, ABCG5, ABCG8) were collected as IVs. Finally, eQTLs in blood tissue for PPARA and LDLR were found in the eqtlGen. No association with PC was found (Supplementary Table S17).
Median analysis
The MR estimates of LPL and CETP on risk factors (BMI and T2D) were presented in Supplementary Table S18. The results showed that the effects of LPL and CETP on the two risk factors were opposite to those on PC. Thus, BMI and T2D were not mediators in the associations of LPL and CETP with PC.
Discussion
In this study, considering the limited effect of current drug therapy for pancreatic cancer and the close association between PC and lipid metabolism, we conducted a comprehensive assessment of the potential causal effects of genetically influenced lipid-related traits and targets of lipid-lowering drugs on the susceptibility to PC in European populations. No significant effect of lipid traits or lipid-lowering drug targets on PC risk was found, which is validated by two dependent PC datasets. This suggests that no lipid-lowering drug could significantly affect pancreatic cancer by regulating lipid metabolism, which is in line with the existing lipid-lowering drugs and pancreatic cancer research conclusions6,20,21. Although Ji et.al have found that atorvastatin can inhibit the proliferation and spread of pancreatic cancer cells by inhibiting the neurotrophin pathway5, this effect may not be obvious for patients with pancreatic cancer as a whole, therefore, no consistent conclusions were obtained in observational studies or MR analysis in our study. This also reflects the current lipid-lowering drugs in the treatment of pancreatic cancer is not significantly effective, only as a chemotherapy regimen in the status of adjuvant drugs.
However, LPL was found associated with PC risk increase in the discovery dataset and CETP was found associated with PC risk decrease in the replication dataset. The finding was verified by different approaches of constructing genetic instruments (lipid trait GWAS and eQTL in blood tissue).
According to the MR estimates of lipid traits (LDL, HDL, TG, TC) on PC in two replication, TG and HDL were potentially associated with PC. Therefore, we combined the findings of some observational and basic studies to explore the association between lipid traits and PC.
Before, TG may not be recognized as a causal risk factor for PC with the available evidence. Although our results suggest that elevated blood triglyceride may reduce the risk of pancreatic cancer, which are consistent with the previous observational study by Naudin S3.
But not all methods in MR analysis supported this result. Furthermore, previous observational studies have shown that patients with pancreatic cancer have significantly higher blood triglyceride than the control group22 and TG might reduce CD8 + T lymphocyte infiltration into pancreatic cancer tissue, affecting antitumor immune functions and immunotherapy efficacy23. Mechanistically, triglyceride promotes the invasion and development of pancreatic cancer, which seems to contradict the conclusions of the study by Naudin S and our study.
Notably, an increase in serum diacylglycerols, in the study of Naudin S, was associated with an increased risk of pancreatic cancer3. Triglyceride hydrolysis produces glycerol and free fatty acids, and diglyceride is an intermediate product in the process of lipolysis24. Free fatty acids promote the migration of pancreatic cancer cells25. Lipid metabolic disorders and intracellular pathways, including cellular stress responses such as oxidative stress, endoplasmic reticulum stress, autophagy, and Ceramide formation, participated in lipotoxicity-induced cell death26. β-cell apoptosis is associated with type 2 diabetes, which is an independent risk factor for pancreatic cancer. This suggests that triglycerides promote pancreatic cancer by breaking down into free fatty acids. Because of lipolysis, the decrease in triglyceride leads to the increased risk of pancreatic cancer, consistent with the results in our study. Furthermore, Zhao RC et.al found that the exosomes of PC cells disrupt the lipid composition of adipocytes, particularly the TG species27. In setd2-deficient pancreatic tumors, there are lipid-rich stroma in the tumor microenvironment, including elevated intracellular TG, and adipogenic CAFs can promote the transfer of lipids from itself to tumor cells to supplement oxidative phosphorylation and provide energy for tumor cells, thereby promoting the development of pancreatic cancer28. Thus, the relationship between triglyceride and pancreatic cancer is extremely complex and could not be summarized by a simple linear relationship.
In addition, previous observational studies have found that high-density lipoprotein increases the risk of PC29. Our results also suggest the potential association with higher PC risk of lower HDL in the discovery dataset. The antioxidant and anti-inflammatory properties of HDL could inhibit cancer cell proliferation30. Stangl H et.al found that component-dependent interactions of HDL particles with SR-B1 and ABCA1 on cancer cells drive the apoptosis of PC cell31. In our study, CETP reduced the risk of pancreatic cancer by decreasing HDL. Therefore, although CETP was validated in the validation set and passed the colocalization analysis, it was not considered as the potential target genes. The more detailed explanation was given below.
Evidence regarding the beneficial effects of lipid-lowering drug targets on PC was not found in the present study. In contrast, we found LPL could increase the risk of PC. The association between TG-lowering genetic variants in APOC3 and ANGPTL3 with a lower PC risk was not validated, which suggested that the effect of LPL on pancreatic cancer might not be mediated by TG. As detailed in Schmidt et al., TG does not need to cause disease if LPL affects the risk of PC through alternative pathways32,33. However, the results of the mediation analysis showed that neither BMI nor T2D was a mediator of the association between LPL and PC.
LPL mediates intravascular hydrolysis of lipoprotein-coated triglycerides34. As previously mentioned, free fatty acids produced by triglyceride hydrolysis contribute to the migration of PC cells25. In addition, PC exosomes increased inflammatory factor IL-6 production which in turn promoted lipolysis in adipocytes and IL-6 level was found correlated with LPL27. Tumor exosomes have been demonstrated to transport cargos into target cells and then profoundly influence their phenotype and function, which played a critical role in tumor initiation and progression35. Furthermore, in the PC microenvironment, abnormal LPL activity may lead to lipid metabolism disorders. When LPL hydrolyzes TG to produce too much free fatty acids, the β-oxidation process in the mitochondria of these fatty acids may be disturbed, eventually generating reactive oxygen species (ROS). In addition, excess free fatty acids can activate nicotinamide adenine dinucleotide phosphate oxidase, a major ROS-producing enzyme36. High levels of ROS deplete intracellular antioxidants, exposing pancreatic cancer cells to long-term oxidative stress. At the same time, ROS can damage mitochondria, endoplasmic reticulum and other organelles in cells, further exacerbating oxidative stress. This environment of constant oxidative stress can promote the proliferation, migration, and invasion of PC cells37. Meanwhile, LPL-mediated aberration of lipid metabolism can activate inflammatory signaling pathways. When free fatty acids accumulate, they can bind to Toll-like receptors (TLR), especially TLR4. In pancreatic cancer cells and surrounding immune cells, TLR4 is activated through a series of signal transductions, activating nuclear factor—κB (NF—κB)38. NF-κB is an important transcription factor that promotes the transcription and release of a variety of inflammatory factors39. These inflammatory cytokines can recruit immune cells such as monocytes to the tumor site to form an inflammatory microenvironment. These monocytes can differentiate into tumor-associated macrophages (TAMs) in the tumor microenvironment and polarize towards the M2-polarized tumor-associated macrophages (M2 TAMs)40,41. M2 TAMs have the functions of promoting tumor growth, angiogenesis, and immunosuppression41. Therefore, in the treatment of pancreatic cancer, inhibition of LPL, thus reducing the production of free fatty acids, might reduce the migration of PC cells.
However, recent studies have shown that LPL activation is associated with insulin resistance42. Insulin resistance is associated with T2D and pancreatic fat accumulation and infiltration, two major risk factors for PC43,44,45. Therefore, the activation of LPL may be beneficial to the early prevention of PC in high-risk population. And the mechanism might affect its value as a therapeutic target to reduce the migration of PC cells. Thus, the potential therapeutic value of LPL remains to be further investigated due to the complex mechanisms between TG and PC.
The pharmacological properties of LPL regulation can be observed in various drugs, such as fibrates, omega-3 fatty acids and metformin, however, it is not the main mechanism of action of these drugs46. Therefore, new targeted drugs to regulate LPL remain to be developed. And more attention needs to be paid to the use of lipid-lowering drugs in the treatment of patients with pancreatic cancer who have other conditions that require lipid-lowering therapy like cardiovascular disease.
In the study, CETP was found appear to reduce the risk of pancreatic cancer. However, the association we found contradicts the current research supporting the protective effect of HDL on PC29,30,31. In our study, the association between CETP and PC was found in the replication dataset. However, the MR-egger analysis between HDL and PC in the replication dataset showed evidence of pleiotropy (egger_intercept = -0.033, p = 0.01), even though the MR-PRESSO did not test the pleiotropy of the results. Because of the pleiotropy, the result does not satisfy the INSIDE hypothesis, so that estimates from the MR-Egger method can be more biased and have greater Type 1 error rates47. In addition, this conclusion in the validation set could not be replicated in the discovery set. Furthermore, the results of the mediation analysis showed that neither BMI nor T2D was a mediator of the association between CETP and PC. Thus, combined with the results of other observational and basic studies, it was considered this as a false positive result.
Limitations
Some limitations should be considered when interpreting the results of this study. First, compared with the short-term effects of lipid-lowering drugs, genetic variants reflect the effect of lifelong changes in lipid levels on PC risk and the magnitude of the effects may not be comparable48. MR analysis can only confirm the direction of association, so that more quantitative studies are required. Second, the sample size of existing PC GWAS cohorts is limited and there might be population overlap between the exposure and outcome. There were pleiotropy issues in the MR analysis conducted using the validation datasets, and the conclusions of the validation dataset set and the discovery dataset were not consistent. In addition, reverse MR to test for causality was not possible because the GWAS cohort for pancreatic cancer lacked SNPs that satisfied the three assumptions of MR analysis. Our results would be more valuable if we had a larger updated PC GWAS as the replication dataset. As such, they may be biased toward the outcome-risk factor association, which caused the false positive result of CETP. Third, the causal relationship between lipid traits and pancreatic cancer was investigated to screen potential lipid-lowering drug targets. Although we screened out two lipid traits that were related. But the results of IVW method showed that they are not causally related to the PC, which further affects the therapeutic value of the potential positive targets we have identified, considering the results of colocalization analysis. A more detailed classification of lipids may be needed to investigate the causal relationship between lipid traits and PC. Fourth, to exclude certain drug target genes that do not affect PC through lipid traits, eQTL for target genes in blood tissue were screened but not included for drug target genes in other tissues. Fifth, although several methods (MR-PRESSO and MR-Egger) were used to rule out horizontal pleiotropy, there might still be undetected horizontal pleiotropy. Sixth, due to the limitations of the replication dataset, the potential therapeutic target (LPL) explored in this study have not been fully validated, so this study does not boldly explore the clinical application prospects of lipid traits and lipid-lowering drug targets. Last, our findings were limited to European population, so that these findings are not necessarily valid for other ethnic groups. Dunca D et.al demonstrated that genetically and environmentally-influenced genetic backgrounds lead to potential differences in CETP between European and East Asian populations49.
Conclusions
To summarize, no significant effect of lipid traits or lipid-lowering drug targets on PC risk was found. LPL might have potential therapeutic value in the migration of PC cells.
Data availability
Data is provided within the manuscript or supplementary information files.
Abbreviations
- PC:
-
Pancreatic cancer
- GWAS:
-
Genome-wide association study
- LPL:
-
Lipoprotein lipase
- MR:
-
Mendelian randomization
- eQTL:
-
Expression quantitative trait loci
- LD:
-
Linkage disequilibrium
- ANGPTL3:
-
Angiopoietin-like 3
- APOC3:
-
Apolipoprotein C-III
- PPARA:
-
Peroxisome proliferator activated receptor alpha
- CETP:
-
Cholesteryl ester transfer protein
- SNP:
-
Single nucleotide polymorphism
- IVW:
-
Inverse-variance weighted
- CI:
-
Confidence interval
References
Siegel, R. L., Giaquinto, A. N. & Jemal, A. Cancer statistics, 2024. CA A Cancer J. Clin. 74(1), 12–49. https://doi.org/10.3322/caac.21820 (2024).
Stoffel, E. M., Brand, R. E. & Goggins, M. Pancreatic cancer: Changing epidemiology and new approaches to risk assessment, early detection, and prevention. Gastroenterology 164(5), 752–765. https://doi.org/10.1053/j.gastro.2023.02.012 (2023).
Naudin, S. et al. Lipidomics and pancreatic cancer risk in two prospective studies. Eur. J. Epidemiol. 38(7), 783–793. https://doi.org/10.1007/s10654-023-01014-3 (2023).
Chen, W. C. et al. Total serum cholesterol and pancreatic cancer: A nested case-control study. Cancer Epidemiol. Biomark. Prev. A Publ. Am. Assoc. Cancer Res. Cosponsored Am. Soc. Prev. Oncol. 28(2), 363–369. https://doi.org/10.1158/1055-9965.Epi-18-0421 (2019).
Cai, S. et al. Atorvastatin inhibits pancreatic cancer cells proliferation and invasion likely by suppressing neurotrophin receptor signaling. Transl. Cancer Res. 9(3), 1439–1447. https://doi.org/10.21037/tcr.2020.01.27 (2020).
Hamada, T. et al. Statin use and pancreatic cancer risk in two prospective cohort studies. J. Gastroenterol. 53(8), 959–966. https://doi.org/10.1007/s00535-018-1430-x (2018).
Davey Smith, G. & Hemani, G. Mendelian randomization: genetic anchors for causal inference in epidemiological studies. Human Mol. Genet. 23(R1), R89-98. https://doi.org/10.1093/hmg/ddu328 (2014).
Burgess, S., Butterworth, A. S. & Thompson, J. R. Beyond Mendelian randomization: How to interpret evidence of shared genetic predictors. J. Clin. Epidemiol. 69, 208–216. https://doi.org/10.1016/j.jclinepi.2015.08.001 (2016).
Skrivankova, V. W. et al. Strengthening the reporting of observational studies in epidemiology using mendelian randomization: The STROBE-MR Statement. JAMA 326(16), 1614–1621. https://doi.org/10.1001/jama.2021.18236 (2021).
Willer, C. J. et al. Discovery and refinement of loci associated with lipid levels. Nat. Genet. 45(11), 1274–1283. https://doi.org/10.1038/ng.2797 (2013).
ESC/EAS guidelines for the management of dyslipidaemias. Lipid modification to reduce cardiovascular risk. Atherosclerosis 290, 140–205. https://doi.org/10.1016/j.atherosclerosis.2019.08.014 (2019).
Borén, J. et al. Metabolism of triglyceride-rich lipoproteins in health and dyslipidaemia. Nat. Rev. Cardiol. 19(9), 577–592. https://doi.org/10.1038/s41569-022-00676-y (2022).
Tosheska Trajkovska, K. & Topuzovska, S. High-density lipoprotein metabolism and reverse cholesterol transport: Strategies for raising HDL cholesterol. Anatolian J. Cardiol. 18(2), 149–154. https://doi.org/10.14744/AnatolJCardiol.2017.7608 (2017).
Sakaue, S. et al. A cross-population atlas of genetic associations for 220 human phenotypes. Nat. Genet. 53(10), 1415–1424. https://doi.org/10.1038/s41588-021-00931-x (2021).
Amundadottir, L. et al. Genome-wide association study identifies variants in the ABO locus associated with susceptibility to pancreatic cancer. Nat. Genet. 41(9), 986–990. https://doi.org/10.1038/ng.429 (2009).
Minelli, C. et al. The use of two-sample methods for Mendelian randomization analyses on single large datasets. Int. J. Epidemiol. 50(5), 1651–1659. https://doi.org/10.1093/ije/dyab084 (2021).
Mounier, N. & Kutalik, Z. Bias correction for inverse variance weighting Mendelian randomization. Genetic Epidemiol. 47(4), 314–331. https://doi.org/10.1002/gepi.22522 (2023).
Verbanck, M. et al. Detection of widespread horizontal pleiotropy in causal relationships inferred from Mendelian randomization between complex traits and diseases. Nat. Genet. 50(5), 693–698. https://doi.org/10.1038/s41588-018-0099-7 (2018).
Hemani, G. et al. The MR-Base platform supports systematic causal inference across the human phenome. eLife https://doi.org/10.7554/eLife.34408 (2018).
Kirkegård, J. et al. Statins and pancreatic cancer risk in patients with chronic pancreatitis: A Danish nationwide population-based cohort study. Int. J. Cancer 146(3), 610–616. https://doi.org/10.1002/ijc.32264 (2020).
Wang, W. et al. The causal relationship between PCSK9 inhibitors and malignant tumors: A Mendelian randomization study based on drug targeting. Genes 15(1), 132. https://doi.org/10.3390/genes15010132 (2024).
Qin, L. et al. High-fat mouse model to explore the relationship between abnormal lipid metabolism and enolase in pancreatic cancer. Mediators Inflamm. 2023, 4965223. https://doi.org/10.1155/2023/4965223 (2023).
Wu, B. et al. Plasma lipid levels are associated with the CD8+ T-cell infiltration and prognosis of patients with pancreatic cancer. Cancer Med. 12(13), 14138–14148. https://doi.org/10.1002/cam4.6080 (2023).
Zechner, R. et al. FAT SIGNALS–lipases and lipolysis in lipid metabolism and signaling. Cell Metab. 15(3), 279–291. https://doi.org/10.1016/j.cmet.2011.12.018 (2012).
Takai, M. et al. FFAR-mediated signaling drives migration of pancreatic cancer cells in hypoxic fibroblast co-cultures. Biochem. Biophys. Res. Commun. 727, 150322. https://doi.org/10.1016/j.bbrc.2024.150322 (2024).
Oh, Y. S. et al. Fatty acid-induced lipotoxicity in pancreatic beta-cells during development of type 2 diabetes. Front Endocrinol. (Lausanne) 9, 384. https://doi.org/10.3389/fendo.2018.00384 (2018).
Wang, S. et al. Pancreatic cancer cell exosomes induce lipidomics changes in adipocytes. Adipocyte 11(1), 346–355. https://doi.org/10.1080/21623945.2022.2084900 (2022).
Niu, N. et al. Tumor cell-intrinsic epigenetic dysregulation shapes cancer-associated fibroblasts heterogeneity to metabolically support pancreatic cancer. Cancer Cell 42(5), 869–84.e9. https://doi.org/10.1016/j.ccell.2024.03.005 (2024).
Zhong, L. et al. Correlation between pancreatic cancer and metabolic syndrome: A systematic review and meta-analysis. Front Endocrinol. (Lausanne) 14, 1116582. https://doi.org/10.3389/fendo.2023.1116582 (2023).
Revilla, G. et al. LDL, HDL and endocrine-related cancer: From pathogenic mechanisms to therapies. Seminars Cancer Biol. 73, 134–157. https://doi.org/10.1016/j.semcancer.2020.11.012 (2021).
Oberle, R. et al. The HDL particle composition determines its antitumor activity in pancreatic cancer. Life Sci. Alliance 5(9), e202101317. https://doi.org/10.26508/lsa.202101317 (2022).
Schmidt, A. F. et al. Genetic drug target validation using Mendelian randomisation. Nat. Commun. 11(1), 3255. https://doi.org/10.1038/s41467-020-16969-0 (2020).
Schmidt, A. F., Hingorani, A. D. & Finan, C. Human Genomics and Drug Development. Cold Spring Harbor Perspect. Med. 12(2), a039230. https://doi.org/10.1101/cshperspect.a039230 (2022).
Wu, S. A., Kersten, S. & Qi, L. Lipoprotein lipase and its regulators: An unfolding story. Trends Endocrinol. Metab. TEM 32(1), 48–61. https://doi.org/10.1016/j.tem.2020.11.005 (2021).
Wortzel, I. et al. Exosome-mediated metastasis: Communication from a distance. Dev. Cell 49(3), 347–360. https://doi.org/10.1016/j.devcel.2019.04.011 (2019).
Ackerman, D. & Simon, M. C. Hypoxia, lipids, and cancer: Surviving the harsh tumor microenvironment. Trends Cell Biol. 24(8), 472–478. https://doi.org/10.1016/j.tcb.2014.06.001 (2014).
Glorieux, C. et al. Targeting ROS in cancer: rationale and strategies. Nat. Rev. Drug Discov. 23(8), 583–606. https://doi.org/10.1038/s41573-024-00979-4 (2024).
Shi, H. et al. TLR4 links innate immunity and fatty acid-induced insulin resistance. J. Clin. Investig. 116(11), 3015–3025. https://doi.org/10.1172/jci28898 (2006).
Silke J, O'Rreilly L A. NF-κB and Pancreatic Cancer; Chapter and Verse. Cancers, 2021, 13(18), https://doi.org/10.3390/cancers13184510.
Sweeney, P. L. et al. Mechanisms of tyrosine kinase inhibitor resistance in renal cell carcinoma. Cancer drug resistance (Alhambra, Calif) 6(4), 858–873. https://doi.org/10.20517/cdr.2023.89 (2023).
Zhou, J. et al. A novel role of TGFBI in macrophage polarization and macrophage-induced pancreatic cancer growth and therapeutic resistance. Cancer Lett. 578, 216457. https://doi.org/10.1016/j.canlet.2023.216457 (2023).
Li, Y. X. et al. Insulin resistance caused by lipotoxicity is related to oxidative stress and endoplasmic reticulum stress in LPL gene knockout heterozygous mice. Atherosclerosis 239(1), 276–282. https://doi.org/10.1016/j.atherosclerosis.2015.01.020 (2015).
Guglielmi, V. & Sbraccia, P. Type 2 diabetes: Does pancreatic fat really matter?. Diabetes/Metabol. Res. Rev. 34(2), 1. https://doi.org/10.1002/dmrr.2955 (2018).
Alempijevic, T. et al. Non-alcoholic fatty pancreas disease. Postgrad. Med. J. 93(1098), 226–230. https://doi.org/10.1136/postgradmedj-2016-134546 (2017).
Kim, D. S. & Scherer, P. E. Obesity, diabetes, and increased cancer progression. Diabetes Metab. J. 45(6), 799–812. https://doi.org/10.4093/dmj.2021.0077 (2021).
Geldenhuys, W. J. et al. Emerging strategies of targeting lipoprotein lipase for metabolic and cardiovascular diseases. Drug Discov. Today 22(2), 352–365. https://doi.org/10.1016/j.drudis.2016.10.007 (2017).
Burgess, S. & Thompson, S. G. Interpreting findings from Mendelian randomization using the MR-Egger method. Eur. J. Epidemiol. 32(5), 377–389. https://doi.org/10.1007/s10654-017-0255-x (2017).
Holmes, M. V. et al. Integrating genomics with biomarkers and therapeutic targets to invigorate cardiovascular drug development. Nat. Rev. Cardiol. 18(6), 435–453. https://doi.org/10.1038/s41569-020-00493-1 (2021).
Dunca, D. et al. Comparing the effects of CETP in East Asian and European ancestries: A Mendelian randomization study. Nat. Commun. 15(1), 5302. https://doi.org/10.1038/s41467-024-49109-z (2024).
Acknowledgements
Not applicable.
Funding
National Natural Science Foundation of China (81972274); Shandong Provincial Natural Science Foundation (ZR2021LSW004); Taishan Scholars Program for Young Experts of Shangdong Province (tsqn202103172); Clinical Research Foundation of Shandong University (2020SDUCRCC016).
Author information
Authors and Affiliations
Contributions
B.S. and Z.F. contributed to the study conception and design. Material preparation, data collection and analysis were performed by B.S. and J.W. The first draft of the manuscript was written by B.S. and Z.F. commented on previous versions of the manuscript. Furthermore, H.Z. was response for funding acquisition, project administration and supervision. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Su, B., Fan, Z., Wu, J. et al. Genetic association of lipid-lowering drug target genes with pancreatic cancer: a Mendelian randomization study. Sci Rep 15, 3282 (2025). https://doi.org/10.1038/s41598-025-87490-x
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-87490-x
