
Abstract
Distant metastases account for ~ 90% of cancer deaths and major responses with systemic therapy alone for metastatic cancers are so rare that the National Cancer Institute launched the Exceptional Responders Initiative. Comprehensive involved site radiotherapy (ISRT) is a promising treatment for oligometastases but the role of circulating tumor DNA to confirm durable molecular response following treatment remains unexplored. Among 597 consecutive patients with distant metastases treated with radiation therapy from 2014 to 2021, 133 (22%) were oligometastatic and 464 (78%) were polymetastatic. The 5-year overall survival was 38% for oligometastases vs. 3% for polymetastases (p < 0.001). At a median follow-up of 71 months for treated oligometastases, 37 (28%) exceptional responders (ER) remain alive and recurrence free at ≥ 2 year follow-up. Among ER, 49% underwent stereotactic radiotherapy (median 27 Gy in 3 fractions, EQD2 43 Gy), 65% underwent intensity-modulated radiation therapy (median 53 Gy in 24 fractions, EQD2 54 Gy), and 76% received additional systemic therapy. Although ctDNA testing was not possible in most ER due to patient refusal or tumor specimen quality, all 12 ER tested ctDNA-negative. Long-term complete responses, including molecular complete responses, are achievable with comprehensive ISRT in diverse clinical presentations.
Similar content being viewed by others

Introduction
Surgery and modern radiation therapy are often effective curative treatments for localized or regional stage I to III solid tumor malignancies1. Approximately 90% of cancer deaths are caused by distant metastases rather than the primary tumor2. Treating existing distant metastases and preventing new distant metastases are necessary components for an effective therapeutic strategy.
Despite ongoing progress, metastatic cancer remains largely incurable and recent analyses estimated that only 16% of all cancer patients respond to either genome-driven oncology or immunotherapy with varying durations of response2,3. Major responses with systemic therapy alone for metastatic cancers are so rare that the National Cancer Institute launched the Exceptional Responders Initiative4. Exceptional response is formally classified as superior response to treatment, expected to occur in less than 10% of patients and defined as greater than three times the duration of the published median response in a similar cohort4,5. There is tremendous enthusiasm for integrating cell-free circulating tumor DNA (ctDNA) testing into the management of patients with advanced cancer6,7,8. A commercially available bespoke ctDNA assay reported 98% sensitivity in patients with advanced solid tumors9. For patients with advanced malignancies, ctDNA clearance is associated with highly favorable survival outcomes9,10.
Metastasis-directed local therapy, generally in combination with systemic therapy, has been shown to improve progression-free survival and/or overall survival compared to systemic therapy alone in the majority of reported randomized trials studying oligometastases (Supplemental Table 1)2,11. In these randomized trials, stereotactic body radiotherapy was the most common local therapy administered. While the concept of oligometastasis as a distinct phenotype gains acceptance, critical gaps in knowledge remain2. Our objectives are to assess the clinical and treatment characteristics of patients who achieved durable radiologic and molecular complete responses following comprehensive involved site radiotherapy (ISRT) for oligometastases in the context of distant metastases treated with radiation therapy.
Patients and methods
Patient characteristics
The Good Samaritan University Hospital IRB approved study #16 − 011 with waiver of informed consent. All methods were performed in accordance with the Declaration of Helsinki. The study population consisted of 597 consecutive adult patients with metastatic solid tumor malignancy treated with radiation therapy by a single radiation oncologist from 1/1/14 to 12/31/21. Baseline data was captured using EPIC and ARIA electronic medical records. Prognostic factors associated with overall survival have been previously identified and based on those results, we collected age, gender, primary tumor site, Eastern Cooperative Oncology Group performance status, pre-treatment serum albumin (g/dl) metastasis site and metastasis extent12. Pre-specified categorical variable cutpoints for performance status (0–1 vs. 2 vs. 3–4) and albumin (≥ 3.4, 2.4 to 3.3 vs. <2.4) and primary tumor site (breast, prostate and kidney vs. other) were validated from the published literature13. Oligometastases were defined as up to 5 distant metastases with a consistent treatment philosophy where all sites of visible locoregional and distant disease were treated with comprehensive ISRT. For classification purposes, oligometastases could include both extracranial or cranial metastases. The EORTC oligometastasis classification system grouped patients into 9 groups but for analysis purposes was subdivided into synchronous vs. metachronous vs. other14,15. Polymetastases were defined as more than 5 distant metastases.
Treatment
Systemic therapy was administered at the discretion of the treating medical oncologist or urologist. For oligometastasis patients, type of adjuvant systemic therapy received was classified into none, chemotherapy, hormonal therapy, immunotherapy, biologically targeted therapy or combinations systemic therapy.
Radiation planning was performed on Varian Eclipse® or BrainLAB ® planning software. Radiation was administered on the Varian 21EX, TrueBeam or Edge linear accelerators. Radiation dose (Gy) and number of fractions was recorded for each site treated. Radiation dose intensity was quantified by converting radiation dose and number of fractions into biological equivalent dose in 2 Gy fractions (EQD2) using the linear quadratic cell survival formula with an alpha beta ratio of 10. For patients requiring radiation to multiple sites, individual EQD2 was calculated for each site and all treated sites and the mean EQD2 for all sites was reported. In general, oligometastasis patients were treated with highly conformal dose distributions on Varian TrueBeam® or Edge®linear accelerators with stereotactic capability equipped with cone beam CT and a 6-degree of freedom robotic couch. Treatment specific data collected included cumulative tumor volume in cm3(< 27.7 vs. ≥27.7), number of metastases treated (0 vs. 1 vs. 2 to 5), whether the primary tumor ± regional nodes were irradiated during this treatment course and radiation dose intensity (EQD2 < 62.5 Gy vs. ≥62.5 Gy)16.
Follow-Up, restaging and recurrence classification
Following radiotherapy, patients were followed with serial imaging, routine blood work, and regular clinical evaluations by the radiation oncology and medical oncology teams. Long-term disease response was defined as absence of clinical or radiological progression on whole body imaging including CT, PET, MRI or bone scan. When available tumor markers (PSA, CEA, CA27.29, CA-125, CA19-9) supplemented radiological imaging using the upper limit of normal to define biochemical control.
Overall survival was calculated as time from initial consultation to death or last follow-up by reviewing all available electronic medical records (EPIC including Care Everywhere, ARIA and scanned physician notes) and local obituaries. For patients with oligometastases, treatment failures were recorded. Progression-free survival is a composite endpoint where death or treatment failures are scored as events. Since patients with limited oligoprogression could be salvaged with further local ± systemic therapy, the TROG 13.01 SAFRON II trial developed a modified definition of progression free survival (mPFS)17. Using the TROG 13.01 SAFRON II mPFS, localized progression salvaged with local treatment such as radiation, thermal ablation or surgery were not counted as events. Additionally, patients with biopsy proven second cancers with a histology different than the index cancer were not counted as mPFS events. Cause of death was ascertained through thorough review of the medical records.
Exceptional responders
For patients treated with comprehensive involved site radiotherapy for oligometastases, exceptional responders were defined as alive and free of recurrence at more than 2 year follow-up (including successful salvage with local therapy for further oligometastases or second primary cancers) or alive with > 5 year overall survival with > 2 year progression free survival.
Circulating tumor DNA
A clinically validated, personalized, tumor-informed 16-plex mPCR-NGS assay (SignateraTM, Natera Inc.), was used to detect molecular residual disease (MRD) (Fig. 3). The Signatera assay is based on whole-exome sequencing of the tumor and a matched normal blood sample to detect and quantify ctDNA. Up to sixteen patient specific somatic single nucleotide variants, based on the tumor tissue, are targeted in patient plasma samples through the patient-specific ctDNA assay, as previously described9. A positive result is designated by greater or equal to 2 tumor-specific variants being detected. ctDNA concentration is reported as mean tumor molecules per ml of plasma (MTM/mL).
Statistical methods
Statistical analysis was performed on Stata 13.1. Treatment failures were classified as local for progression within or adjacent to the irradiated volume while unsalvageable distant metastases outside the irradiated volumes were classified as distant failures. All time-to-event endpoints were calculated from the date of radiation oncology consultation to date of event of interest. Differences in survival on univariable analysis were performed using the log rank test of 2 to 3 categorical variables. Variables with a p value of ≤ 0.1 on univariable analysis were entered into a Cox multivariable analysis. Actuarial survival curves were generated using the Kaplan Meier method. Patients lost to follow up were censored at the time of last verified contact. Differences between groups (oligometastatic versus polymetastatic; exceptional responders versus non-exceptional responders) were compared by Pearson’s chi-square for categorical variables and a 2-sided student’s t test for continuous variables with p values of < 0.05 considered statistically significant.
Results
Patient characteristics, radiation dose intensity and survival for patients with oligometastases and polymetastases
The median survival for all 597 patients with distant metastasis was 9.6 months with a 5-year overall survival of 11.5% (Fig. 1A). In terms of extent of metastases, 22% were oligometastatic and 78% were polymetastatic. Differences in patient characteristics between oligometastatic and polymetastatic patients were summarized in Table 1.
Between oligometastatic and polymetastatic groups, there were no significant differences in age or gender. The distributions of primary tumor sites were similar with the exception of more uterine cancers in the oligometastasis group (7.5% vs. 3.0%, p = 0.02). Patients with oligometastases were more likely to have better ECOG performance status (p < 0.001) and higher serum albumin (p < 0.001). Polymetastasis patients were more likely to have lung, bone, liver, adrenal and distant lymph node metastases (p < 0.02 for all) but the prevalence of brain metastases was similar (p = 0.28). Finally, patients with oligometastases tended to receive higher radiation doses with a median EQD2 of 54.4 Gy vs. 36.5 Gy (p < 0.001).
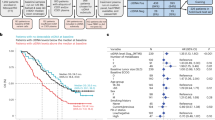
The median survival for patients with oligometastaes was 42.8 months vs. 6.1 months for patients with polymetastases (HR 4.1, p < 0.001). The 5-year overall survival was 38.2% oligometastases vs. 2.8% for polymetastasis (Fig. 1B).
Patterns of failure for patients with oligometastases
The median follow-up for surviving patients with oligometastases was 42.9 months with a 5-year overall survival 38.2% (IQR 28.7–47.6%) (Fig. 2A). The median modified progression-free survival (including successful salvage of further oligometastases) was 13.8 months with a 5-year modified progression-free survival (including successful salvage of further oligometastases) 29.0% (IQR 20.7–37.8%) (Fig. 2B). Median local progression-free survival has not been reached with a 5-year local progression free survival of 85.4% (IQR 75.5–91.6%) (Fig. 2C). Median distant progression-free survival (including successful salvage of further oliogmetastases) was 15.9 months and the 5-year distant progression-free survival was 34.8% (IQR 25.8–43.9%) (Fig. 2D).

(A) Overall Survival for Patients with Distant Metastases Treated with Radiotherapy. (B) Overall Survival for Patients with Distant Metastases Stratified by Oligometastases vs. Polymetastases.

Kaplan-Meier Survival Curves for 133 Consecutive Patients with Oligometastases. A) Overall Survival; B) Modified Progression-Free Survival; C) Local Control; D) Distant Control.
In terms of predictors of survival for patients with oligometastases, age, ECOG performance status, favorable primary tumor site (breast, prostate or kidney), liver metastases and serum albumin all had prognostic significance on univariable analysis (p < 0.02 for all) (Table 2). None of the analyzed treatment variables including cumulative tumor volume, number of metastases treated, treatment of the primary tumor, radiation dose intensity in EQD2 or adjuvant systemic therapy predicted survival (Table 2). On Cox multivariable analysis, age, ECOG performance status, baseline serum albumin and favorable tumor site (breast, prostate or kidney) independently predicted overall survival (Table 2).
Oligometastases with exceptional response
Among 133 patients with oligometastases, there are 37 exceptional responders described in detail in Supplemental Table 2. The median follow-up time for exceptional responders was 70.6 months. Exceptional responders had a median age of 65, 54% male, 35% lung primary, 84% ECOG 0–1, 81% normal albumin, 32% brain metastases, 30% bone metastases, 0% liver metastases, median tumor volume 40.6 cc, 67% 0 to 1 metastases treated, 46% primary tumor treated, median EQD2 radiation dose 51 Gy and adjuvant systemic therapy 76% (Table 3). Two (5.4%) exceptional responders had their primary tumor treated only with radiotherpay; metastatic sites were treated with other modalities. Comparing exceptional responders to non-exceptional responders, patient and treatment characteristics were similar except for more patients with normal albumin (81% vs. 60%, p = 0.05) and fewer patients with liver metastases (0% vs. 14%, p = 0.02) in the exceptional responder cohort (Table 3).
In terms of radiation regimen, 65% received IMRT with a median dose of 53 Gy in 24 fractions (EDQ 54 Gy) and 49% received stereotactic radiation with a median dose of 27 Gy in 3 fractions (EDQ2 43 Gy) (Supplemental Table 2). Five patients (14%) received both IMRT and stereotactic radiation. The exceptional responder cohort includes 5 patients requiring successful salvage radiation (median dose 50 Gy in 10 fractions, EQD2 63 Gy) and 2 patients with biopsy proven second malignancy (Fig. 3 and Supplemental Table 2). Systemic treatments received by exceptional responders include none (24%), hormonal therapy alone (19%), immunotherapy alone (14%), chemotherapy alone (11%), chemoimmunotherapy (11%), chemotherapy and biologically targeted therapy (11%), targeted therapy alone (8%) and hormonal therapy and biologically targeted therapy (3%). There were no obvious differences in systemic therapy received by exceptional responders (Table 4). There exceptional responders among all subgroups save for ECOG 3–4 performance status, albumin < 2.4 g/dl and liver metastases.

Swimmer plot of exceptional responders graphically depicting duration of follow-up after comprehensive involved site radiotherapy (blue bar), salvage radiation (green square) and ctDNA testing (black circle)
Pre-treatment and post-treatment circulating tumor DNA
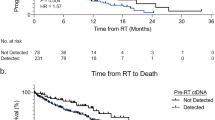
Clinical adoption of ctDNA testing at Good Samaritan University Hospital was not implemented until 2022. For patients with untreated oligometastases from 2022 to 2024, pretreatment ctDNA testing was performed in 10 patients with 1 to 5 distant metastases (4 lung primary, 3 ovarian primary 2 colorectal primary and 1 breast primary). Pre-treatment ctDNA was positive in 9 of 10 patients (90%) with the only false negative occurring in a patient with solitary brain metastases but no extracranial disease on PET/CT (Table 5).
The process for circulating tumor DNA testing is outlined in Fig. 4. Since all exceptional responders were treated prior to 2022, pre-treatment ctDNA was not available for these patients. Twenty of the 37 ER had ctDNA testing (Signatera) ordered; the remaining 17 patients declined testing. Among 20 tested patients, assay generation was not feasible in 8 patients due to bone decalcification or inadequate tumor tissue for whole exome sequencing. Among those who underwent assessment, remarkably all 12 specimens tested negative for ctDNA, signifying molecular complete remission. Further details of these patients, including specifics of radiation and systemic treatment, are available in Supplemental Table 3.

Overview of Circulating Tumor DNA Process. Exceptional responders were identified from consecutive oligometastatic patients treated between 2014 and 2021. A clinically validated, personalized, tumor-informed 16-plex mPCR-NGS assay (SignateraTM, Natera Inc), was used to detect molecular residual disease (MRD). The Signatera assay is based on whole-exome sequencing of the tumor and a matched normal blood sample to detect and quantify ctDNA. Created with BioRender.com.
Additional major responders
In addition to the 37 exceptional responders of 133 oligometastases, there were an additional 11 patients with sustained benefit defined as ≥ 5 year overall survival with death from metastatic cancer or ≥ 2 year progression-free survival with death unrelated to cancer (Supplemental Table 4). For these 11 patients, 4 patients developed widespread disease progression after a prolonged disease-free interval and ultimately failed salvage therapy leading to eventual death from cancer at 5.7 to 7.2 year follow-up. One breast cancer patient progressed at 2.9 years after treatment and was diagnosed with a PI3K mutation is currently receiving salvage systemic therapy at 3.2 year follow-up. Of the remaining 6 patients with clinically and radiographically controlled disease at 2.0 to 5.5 year follow-up, 1 died after complications following surgery for biopsy proven radionecrosis, 1 expired peacefully at home, 1 experienced cardiac arrest while fishing, 1 died of SARS-CoV-2, 1 died while on dialysis and 1 died of septic shock. Based on extensive review of medical records including recent restaging imaging, the cause of death did not appear to be related to cancer in any of these cases. Taken together, 48 of 133 (36%) oligometastasis patients, of various primary tumor types (Table 3), were either exceptional responders or derived sustained benefit and this corresponds nicely with the 5-year overall survival of 38%.
By contrast, only 6 of 464 patients with polymetastasis who were treated with primary systemic therapy and subtotal palliative radiotherapy were exceptional responders (Supplemental Table 5). With the exception of testicular seminoma, which is extremely sensitive to chemotherapy and low dose radiation therapy, the 5 remaining patients received radiation doses with a higher EQD2 > 40 Gy12. Consistent with the notion that immunotherapy responses can be durable, 4 of 6 exceptional responders to primary systemic therapy received immunotherapy.
Discussion
Prevalence of oligometastases
In a large general radiation oncology practice, 22% of patients with distant metastases treated with radiotherapy, including those with limited brain metastases, have oligometastases. In a cross sectional radiological study from University Hospital Zurich, approximately 50% of unique patients with distant metastases undergoing PET have less than 5 extracranial metastases on at least 1 scan18. While non-metastatic cancers are optimally treated with a multidisciplinary fashion often with tumor board input, metastatic disease has been historically managed primarily by the medical oncologist alone. This study demonstrates that oligometastases are not rare and could benefit from expanded adoption of a multidisciplinary approach.
Long-term survival for oligometastases treated with comprehensive ISRT
Patients with oligometastases and polymetastases are not directly comparable because oligometastasis patients have a lower disease burden resulting in better performance status and higher serum albumin (Table 1). The specific cause of improved long-term survival of patients with oligometastases vs. polymetastases cannot be determined from this retrospective study.
Prior multivariable analyzes consistently demonstrate that in addition to oligometastases treated with total metastatic ablation, better performance status, higher serum albumin and favorable primary tumor site (breast, prostate and kidney) independently contribute to improved prognosis12,19,20. Ultimately, randomized controlled trials are necessary to isolate the potential benefit of comprehensive involved site radiation to supplement systemic therapy alone.
A review of 19 published or presented randomized trials comparing systemic therapy alone ± supplemental local therapy in 1936 patients with extracranial oligometastases was performed (Supplemental Table 1)10,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38. Among these trials, 14 were positive including 6 trials that demonstrated improved overall survival with the remaining positive trials demonstrating improved progression-free survival or androgen deprivation therapy-free survival. These trials encompass a variety of cancer types including non-small cell lung cancer, prostate, breast, colorectal, esophageal, pancreatic and mixed histologies. While there remain skeptics, the preponderance of available data suggest that intensifying therapy by supplementing systemic therapy with metastasis directed therapy improves outcomes for oligometastases across a variety of tumor types although the effect size may be less robust or null for breast cancer patients or colorectal cancers that spread to lung rather than liver10,25,30. The interaction between radiotherapy and immunotherapy for non-small cell lung cancer is not well defined with conflicting results when considering the CURB and NRG LU-002 trials10,25. In the CURB trial, adding radiotherapy to systemic therapy improved progression free survival in patients with oligoprogressive non-small cell lung cancer where 77% received immunotherapy10. By contrast, in the NRG-LU002 trial, consolidative radiation failed to improve outcomes in patients treated with first-line systemic therapy including 90% receiving immunotherapy25. Consistent with the notion that immunotherapy may not necessarily augment comprehensive involved site radiation is the finding that only 25% of exceptional responders received immunotherapy. By contrast, 4 of 6 polymetastasis patients with exceptional response received immunotherapy.
Characteristics of oligometastases with exceptional response
When including successful salvage of further oligometastases, 37 of 133 patients (28%) treated for oligometastases were classified as exceptional responders with a median follow-up of 70.6 months. Compared to non-exceptional responders, exceptional responders had similar patient and treatment characteristics with the exception of higher serum albumin and lower prevalence of liver metastases. Specifics of systemic treatment received or radiation treatment dose intensity did not appear to impact outcome. Given the diversity of exceptional responders in terms of tumor type, location of metastases and type of systemic treatment received, it remains challenging to prospectively select patients more likely to benefit from curative-intent treatment for oligometastases. Importantly, this retrospective experience included oligometastasis patients typically excluded by the published randomized trials. Major subgroups historically underrepresented in oligometastasis trials include patients with brain metastases (30%), patients requiring treatment of the primary tumor and nodes (47%) and patients receiving IMRT rather than SBRT (65% of exceptional responders). There were no statistically significant differences in survival for oligometastases with brain metastases, requiring treatment to the primary tumor or with radiation dose intensity (Table 2). In terms of subgroups where comprehensive involved site radiation might be futile, patients with ECOG 3–4 performance status and albumin < 2.4 g/dl certainly fare worse without evidence of exceptional responders in this study.
Beyond clinical prognostic factors, using advanced methods such as pre-treatment genomic, transcriptomic and proteomic profiling may provide further insight into the biology of oligometastases and warrants further investigation39.
Undetectable cell-free circulating tumor DNA (ctDNA) in exceptional responders
Oncologists and researchers have enthusiastically embraced ctDNA technology for early diagnosis, pre-treatment prognostication, response monitoring, detecting minimal residual disease and in surveillance to supplement standard imaging and laboratory testing40,41. At the minimum, ctDNA offers the possibility of detecting disease several months before radiological evidence of progression suggesting improved sensitivity. While there are significant differences in different published ctDNA technologies and methods, we utilized the commercially available tumor informed Signatera platform (Natera). While this tumor informed bespoke assay offers sensitivity rates as high as 98% for untreated metastatic cancer, there are specific pitfalls9,40. The requirement for adequate tumor DNA resulted in inability to test 8 of 20 exceptional responders. In contrast to patients undergoing surgery, patients diagnosed on prostate or lung needle biopsy often have only scarce archival tumor cells that may have been further depleted by prior immunohistochemical or genomic testing. For patients with bone metastases, widely utilized chemical decalcification protocols can damage tumor DNA. ctDNA will not rule out isolated brain or spinal cord metastases because tumor cells would have to cross the blood brain barrier to be detected. Finally, a tumor informed ctDNA assay can only detect the index cancer and not additional second primary tumors42. With these known limitations, clearing ctDNA at any point after treatment is associated with a superior outcome compared to patients with persistent ctDNA40,43.
In this context, we report that all 12 exceptional responders undergoing ctDNA testing at long-term follow-up were tested negative for ctDNA while 9 of 10 (90%) of untreated controls with oligometastases had detectable ctDNA. The novel observation of frequent ctDNA clearance in long-term survivors raises the possibility of molecular complete response for solid tumor metastases, a concept already well established in leukemia40. With further validation, ctDNA could develop into a surrogate endpoint for patients with oligometastases. In the recently published CURB study, the rate of clearing ctDNA with stereotactic body radiation for oligoprogressive non-small cell lung cancer at 8 weeks following radiation was approximately 50% vs. 10% with systemic therapy alone (p= 0.02)10. Within 4 months of chemoradiation for stage I-III non-small cell lung cancer, 53% of patients had detectable ctDNA and 3 year progression-free survival was 93% for undetectable ctDNA vs. 0% for detectable ctDNA (P< 0.001)44. Further analysis of ctDNA kinetics can identify the optimal time to establish molecular complete remission42. Since medical oncologists have historically been reluctant to administer adjuvant systemic therapy for metastatic cancer in the absence of measurable disease, persistence of ctDNA during surveillance could provide a future basis for earlier initiation of systemic therapy rather than waiting for overt metastatic relapse40.
In terms of cure of oligometastases, this retrospective study cannot provide definitive evidence for or against. It cannot be determined whether patients with negative ctDNA are truly cured, have low tumor burdens below the sensitivity of currently available ctDNA tests or instead have dormant disease that can reappear later2,40.
Research limitations
There are many limitations of this research. This is a single physician retrospective experience and may not be generalizable to other clinical settings. In real world practice, patients with distant metastases represent a highly heterogeneous population with a variety of tumor types and metastases sites with widely diverging tumor biology and natural history that limits generalizability (Tables 1 and 2). While patients were treated from 2014 to 2021, systemic therapies continue to advance rapidly, including the recent development of immunotherapy, antibody-drug conjugates, tyrosine kinase inhibitors and cyclin dependent kinase 4/6 inhibitors45. Some of these agents were not approved during the early years of this study and the impact of these new agents on the efficacy of metastasis-directed radiation is unknown.
Another limitation is that exceptional responders represent only 28% of patients and oligometastases represent only 22% of all patients with distant metastases requiring radiation therapy. Exceptional responders to comprehensive involved site radiation account for only 6% of all patients with metastatic cancer receiving radiotherapy. Even when successful, curative intent radiation for oligometastases can only reduce the public health burden of distant metastasis by a small percentage overall. As a community hospital program without resources to prospectively bank biological specimens, pretreatment plasma samples for ctDNA testing were not available for these patients who were treated from 2014 to 2021, limiting the robustness of our data. Additionally, we were only able to obtain ctDNA at a single timepoint at long-term follow-up and information on ctDNA kinetics is not available.
Future directions
Based on significantly improved prognosis and different treatment approaches compared to polymetastases, oligometastases are a clinically relevant phenotype. The field of medical oncology has enthusiastically embraced molecular testing to identify small subsets of patients treatable with targeted therapies. Genomic and molecular testing with immunohistochemistry, fluorescence in situ hybridization or genomics is an intuitively attractive concept that offers the advantage of objectivity46. Systemic therapy informed by molecular testing is well represented on current National Comprehensive Cancer Network (NCCN) guidelines. For example, tumor mismatch repair deficiency represents 2 to 4% of cancers and patients are routinely screened for this molecular phenotype47. By contrast, defining oligometastases on whole body imaging remains relatively poorly defined11. Current NCCN guidelines for colorectal, lung and prostate oligometastases discuss local therapy for certain clinical scenarios but are much less prescriptive than comparable guidelines for biologically targeted therapies or immunotherapy informed by molecular testing. Moving forward, rather than determining treatment protocols solely by tumor site, stage IV metastatic cancers as a whole could optimally be further divided into favorable or unfavorable cohorts with patients with oligometastases with good to excellent performance status ± normal albumin representing a distinct stage48.
Technical advances in radiotherapy to facilitate radiation dose escalation including expanded use of high dose intensity stereotactic radiation, particle therapy, adaptive radiation, MR-linear accelerators, and PET-guided radiation could theoretically improve long-term local control or further reduce toxicity1. Since systemic therapy alone remains the mainstay of treatment for distant metastases, radiation dose intensity in this study was highly personalized to balance safety and efficacy. While judicious dose escalation for oligometastases should be investigated, the long-term efficacy (85% 5-year local control with only 1% isolated local failure) of relatively modest radiation doses raises the possibility of safely targeting more than 5 distant metastases. Recently published data suggest that the incidence of presenting with 6 to 10 metastatic lesions on whole-body imaging is 11% although the clinical benefit of metastasis-directed therapy for this patient population has not been established18. In the recent ARREST phase I trial, patients with > 10 distant metastases were comprehensively treated to 12 to 30 Gy in 3 to 5 fractions with a median survival of 13.8 months49. Finally, a provocative randomized phase II trial demonstrated that radiation to asymptomatic high-risk bone metastases improves overall survival50. These data raise the possibility that an expanded role of radiation for asymptomatic distant metastases could benefit carefully selected patients.
Patients with polymetastases treated with comparatively low doses of radiation to limited volumes only had a 2.8% 5 year overall survival despite the well documented advances in systemic therapy. Taken together, there is no compelling evidence that more comprehensive radiation to higher EQD2 doses compromises the efficacy of systemic therapy, particularly since systemic treatment is increasingly moving away from cytotoxic chemotherapy that requires an intact bone marrow.
Despite comprehensive involved site radiation, the majority of patients with oligometastases eventually progress with further widespread distant metastases contributing to the overwhelming majority of treatment failures. Reducing the incidence of widespread metastatic progression would be the most logical approach to increasing the frequency of exceptional responders. While achieving single agent activity is the most frequent path to achieving FDA approval, combining radiation with systemic therapy for oligometastases is relatively unexplored51. A specific approach that warrants further exploration is to view treated oligometastases as a form of minimal residual disease where adjuvant systemic therapy is utilized to prevent additional metastases2,52. One can speculate that patients with minimal residual disease would be responsive to treatment than patients with a higher burden of untreated disease. For instance, colorectal cancer patients with mismatch repair or microsatellite instability treated with immunotherapy alone has a clinical and radiological complete response rate approaching 100% for stage II-III rectal cancer compared to a more modest median progression-free survival of 16.5 months for stage IV colorectal cancer53,54.
While most researchers are pursuing tumor-specific studies (i.e., targeting tumor specific mutations, CAR-T/CRISPR/mRNA specific targeting), other researchers are studying broad technologies that address metastatic cancer across disease types48. Arguably, metastatic cancer is such a high priority area of research that both approaches should be vigorously pursued. The heterogeneity of oligometastasis makes studying systemic therapy in this population challenging, necessitating greater acceptance of molecular or phenotypic basket trials or single-subject (n of 1) clinical trials55. While the overall benefit of genomic testing remains limited, next-generation RNA transcriptome sequencing and targeting master regulators proteins offers promise56,57.
Conclusion
With all of the caveats associated with retrospective clinical research, we present data showing that patients with oligometastases can achieve long-term survival and even molecular complete remission following comprehensive involved site radiation in addition to standard of care systemic therapy. The role of systemic therapy in achieving molecular remission cannot be ruled out, as the majority of exceptional responders received varying types of systemic therapy in addition to radiotherapy. The potential of combined modality therapy to improve outcomes for selected patients with historically poor prognosis metastatic cancer is underappreciated. Further studies to reduce distant failure in patients with treated oligometastases represents a promising and underexplored avenue of research.
Data availability
Data is provided within the manuscript or supplementary information files.
Change history
31 March 2025
A Correction to this paper has been published: https://doi.org/10.1038/s41598-025-93866-w
References
Chandra, R. A., Keane, F. K., Voncken, F. E. M. & Thomas, C. R. Jr. Contemporary radiotherapy: present and future. Lancet 398, 171–184 (2021).
Gerstberger, S., Jiang, Q. & Ganesh, K. Metastasis Cell. ;186:1564–1579. (2023).
Haslam, A., Gill, J. & Prasad, V. Estimation of the percentage of US patients with Cancer who are eligible for Immune checkpoint inhibitor drugs. JAMA Netw. Open. 3, e200423 (2020).
Conley, B. A. et al. The exceptional responders Initiative: feasibility of a National Cancer Institute Pilot Study. J. Natl. Cancer Inst. 113, 27–37 (2021).
Nishikawa, G., Luo, J. & Prasad, V. A comprehensive review of exceptional responders to anticancer drugs in the biomedical literature. Eur. J. Cancer. 101, 143–151 (2018).
Attia, P. & Gifford, B. Outlive: The Science & art of Longevity. First Edition (Harmony, 2023).
Chabon, J. J. et al. Integrating genomic features for non-invasive early lung cancer detection. Nature 580, 245–251 (2020).
Tie, J. et al. Circulating tumor DNA analysis guiding adjuvant therapy in stage II Colon cancer. N Engl. J. Med. 386, 2261–2272 (2022).
Bratman, S. V. et al. Personalized circulating tumor DNA analysis as a predictive biomarker in solid tumor patients treated with pembrolizumab. Nat. Cancer. 1, 873–881 (2020).
Tsai, C. J. et al. Standard-of-care systemic therapy with or without stereotactic body radiotherapy in patients with oligoprogressive breast cancer or non-small-cell lung cancer (consolidative use of Radiotherapy to Block [CURB] oligoprogression): an open-label, randomised, controlled, phase 2 study. Lancet 403, 171–182 (2024).
Liu, W., Bahig, H. & Palma, D. A. Oligometastases: emerging evidence. J. Clin. Oncol. 40, 4250–4260 (2022).
Kao, J. et al. Association of radiation dose intensity with overall survival in patients with distant metastases. Cancer Med. 10, 7934–7942 (2021).
Kao, J. et al. Clinical predictors of survival for patients with Stage IV Cancer referred to Radiation Oncology. PLoS One. 10, e0124329 (2015).
Templeton, A. J. et al. Prognostic role of neutrophil-to-lymphocyte ratio in solid tumors: a systematic review and meta-analysis. J. Natl. Cancer Inst. 106, dju124 (2014).
Baker, S. et al. Validation of the Prognostic Utility of ESTRO/EORTC Oligometastatic Disease classification: a secondary analysis from the Population-based phase II SABR-5 trial. Int. J. Radiat. Oncol. Biol. Phys. 114, 849–855 (2022).
Cao, Y. et al. Volumetric burden of metastatic lesions drives outcomes in patients with extracranial oligometastatic disease. Cancer Med. 10, 8091–8099 (2021).
Siva, S. et al. Long-term outcomes of TROG 13.01 SAFRON II Randomized Trial of single- Versus Multifraction Stereotactic Ablative Body Radiotherapy for Pulmonary oligometastases. J. Clin. Oncol. 41, 3493–3498 (2023).
Christ, S. M. et al. Imaging-based prevalence of Oligometastatic Disease: a single-center cross-sectional study. Int. J. Radiat. Oncol. Biol. Phys. 114, 596–602 (2022).
Zucker, A., Tsai, C. J., Loscalzo, J., Calves, P. & Kao, J. The NEAT predictive model for survival in patients with Advanced Cancer. Cancer Res. Treat. 50, 1433–1443 (2018).
Siva, S. et al. Impact of medical operability and total metastatic ablation on outcomes after SABR for oligometastases. Int. J. Radiat. Oncol. Biol. Phys. 114, 862–870 (2022).
Palma, D. A. et al. Stereotactic ablative radiotherapy for the Comprehensive Treatment of Oligometastatic Cancers: long-term results of the SABR-COMET phase II randomized trial. J. Clin. Oncol. 38, 2830–2838 (2020).
Gomez, D. R. et al. Local consolidative therapy Vs. maintenance Therapy or Observation for patients with Oligometastatic Non-small-cell Lung Cancer: long-term results of a multi-institutional, phase II, Randomized Study. J. Clin. Oncol. 37, 1558–1565 (2019).
Iyengar, P. et al. Consolidative Radiotherapy for Limited Metastatic Non-small-cell Lung Cancer: a phase 2 Randomized Clinical Trial. JAMA Oncol. 4, e173501 (2018).
Wang, X. S. et al. Randomized Trial of First-Line tyrosine kinase inhibitor with or without Radiotherapy for Synchronous Oligometastatic EGFR-Mutated Non-small Cell Lung Cancer. J. Natl. Cancer Inst. 115, 742–748 (2023).
Iyengar, P., Hu, C. & Gomez, D. R. al e. NRG-LU002: Randomized phase II/III trial of maintenance systemic therapy versus local consolidative therapy (LCT) plus maintenance systemic therapy for limited metastatic non-small cell lung cancer (NSCLC). J Clin Oncol ;42:8506. (2024).
Deek, M. P. et al. Long-term outcomes and genetic predictors of response to Metastasis-Directed Therapy Versus Observation in oligometastatic prostate Cancer: analysis of STOMP and ORIOLE trials. J. Clin. Oncol. 40, 3377–3382 (2022).
Tang, C. et al. Addition of Metastasis-Directed therapy to intermittent hormone therapy for oligometastatic prostate Cancer: the EXTEND phase 2 Randomized Clinical Trial. JAMA Oncol. 9, 825–834 (2023).
Francolini, G. et al. Stereotactic body Radiation Therapy and Abiraterone acetate for patients affected by Oligometastatic Castrate-resistant prostate Cancer: a Randomized Phase II Trial (ARTO). J. Clin. Oncol. 41, 5561–5568 (2023).
Ruers, T. et al. Local treatment of Unresectable Colorectal Liver metastases: results of a Randomized Phase II Trial. J. Natl. Cancer Inst. ;109. (2017).
Milosevic, M. et al. Pulmonary metastasectomy in Colorectal Cancer: updated analysis of 93 randomized patients - control survival is much better than previously assumed. Colorectal Dis. 22, 1314–1324 (2020).
Adam, R., Piedvache, C. & Chiche, L. al e. Chemotherapy and liver transplantation versus chemotherapy alone in patients with definitively unresectable colorectal liver metastases: A prospective multicentric randomized trial (TRANSMET). J Clin Oncol ;42:3500. (2024).
Chmura, S. J., Winter, K. A. & Woodward, W. A. al e. NRG-BR002: A phase IIR/III trial of standard of care systemic therapy with or without stereotactic body radiotherapy (SBRT) and/or surgical resection (SR) for newly oligometastatic breast cancer (NCT02364557). J Clin Oncol ;40:1007. (2022).
Khoo, V., Kirby, A., Ahmed, M. & al e. CORE - Standard of care +/- stereotactic body radiotherapy for oligometastases - primary results. Radiother Oncol. 182, S627 (2023).
Liu, Q. et al. Systemic therapy with or without local intervention for oligometastatic oesophageal squamous cell carcinoma (ESO-Shanghai 13): an open-label, randomised, phase 2 trial. Lancet Gastroenterol. Hepatol. 9, 45–55 (2024).
Ludmir, E. B. et al. Addition of Metastasis-Directed therapy to systemic therapy for Oligometastatic Pancreatic Ductal Adenocarcinoma (EXTEND): a Multicenter, Randomized Phase II Trial. J. Clin. Oncol. :JCO2400081. (2024).
Schellenberg, D., Gabos, Z. & D’uimering, A. al e. Stereotactic Ablative Radiotherapy for Oligo-Progressive Cancers: Results of the Randomized Phase II STOP Trial. Int J Radiat Oncol Biol Phys ;117:S58. (2023).
Ost, P. et al. Surveillance or Metastasis-Directed therapy for oligometastatic prostate Cancer recurrence: a prospective, randomized, Multicenter Phase II Trial. J. Clin. Oncol. 36, 446–453 (2018).
Phillips, R. et al. Outcomes of Observation vs Stereotactic Ablative Radiation for oligometastatic prostate Cancer: the ORIOLE phase 2 Randomized Clinical Trial. JAMA Oncol. 6, 650–659 (2020).
Pitroda, S. P. et al. Integrated molecular subtyping defines a curable oligometastatic state in colorectal liver metastasis. Nat. Commun. 9, 1793 (2018).
Moding, E. J., Nabet, B. Y., Alizadeh, A. A. & Diehn, M. Detecting liquid remnants of solid tumors: circulating Tumor DNA minimal residual disease. Cancer Discov. 11, 2968–2986 (2021).
Corcoran, R. B. & Chabner, B. A. Application of cell-free DNA analysis to Cancer Treatment. N Engl. J. Med. 379, 1754–1765 (2018).
Abbosh, C. et al. Tracking early lung cancer metastatic dissemination in TRACERx using ctDNA. Nature 616, 553–562 (2023).
Pellini, B. & Chaudhuri, A. A. Circulating tumor DNA minimal residual disease detection of non-small-cell lung Cancer treated with curative intent. J. Clin. Oncol. 40, 567–575 (2022).
Chaudhuri, A. A. et al. Early detection of molecular residual disease in localized Lung Cancer by circulating Tumor DNA profiling. Cancer Discov. 7, 1394–1403 (2017).
DeVita, V. T., Lawrence, T. S. & Rosenberg, S. A. Devita, Hellman, and Rosenberg’s cancer: principles and practice of oncology. Twelfth edition (Wolters Kluwer, 2023).
Tannock, I. F. & Hickman, J. A. Limits to Personalized Cancer Medicine. N Engl. J. Med. 375, 1289–1294 (2016).
Maio, M. et al. Pembrolizumab in microsatellite instability high or mismatch repair deficient cancers: updated analysis from the phase II KEYNOTE-158 study. Ann. Oncol. 33, 929–938 (2022).
Andre, F., Rassy, E., Marabelle, A., Michiels, S. & Besse, B. Forget lung, breast or prostate cancer: why tumour naming needs to change. Nature 626, 26–29 (2024).
Nguyen, T. K. et al. Ablative Radiation Therapy to restrain everything safely treatable (ARREST): a phase 1 study of Stereotactic Ablative Radiation Therapy for Polymetastatic Disease. Int. J. Radiat. Oncol. Biol. Phys. (2024).
Gillespie, E. F. et al. Prophylactic Radiation Therapy Versus Standard of Care for patients with high-risk asymptomatic bone metastases: a Multicenter, Randomized Phase II Clinical Trial. J. Clin. Oncol. 42, 38–46 (2024).
Kao, J. et al. Concurrent sunitinib and stereotactic body radiotherapy for patients with oligometastases: final report of a prospective clinical trial. Target. Oncol. 9, 145–153 (2014).
Kao, J. K. Progress in Cancer Research. New. York Times 2023;July. 2, 11 (2023).
Andre, T. et al. Pembrolizumab in microsatellite-instability-high Advanced Colorectal Cancer. N Engl. J. Med. 383, 2207–2218 (2020).
Cercek, A. et al. PD-1 blockade in Mismatch Repair-Deficient, locally advanced rectal Cancer. N Engl. J. Med. 386, 2363–2376 (2022).
Mundi, P. S. et al. A transcriptome-based Precision Oncology platform for patient-therapy alignment in a Diverse Set of Treatment-resistant malignancies. Cancer Discov. 13, 1386–1407 (2023).
Paull, E. O. et al. A modular master regulator landscape controls cancer transcriptional identity. Cell 184, 334–351 (2021). e20.
Perspective, P. V. The precision-oncology illusion. Nature 537, S63 (2016).
Author information
Authors and Affiliations
Contributions
RR, VG, LA, SM, JH, AS, JK acquired data. RR, MK, ML, JH, MM, JK wrote the main manuscript text. RR, CK, and JK prepared tables and figures. All authors reviewed the manuscript.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
The original online version of this Article was revised: The original version of this Article contained errors in the figures. In Figure 1, panel B was omitted. The figure legend was correct at the time of publication. In Figure 2, panels B, C and D were omitted. As the result, Figure 2 legend now reads: “Kaplan-Meier Survival Curves for 133 Consecutive Patients with Oligometastases. A) Overall Survival; B) Modified Progression-Free Survival; C) Local Control; D) Distant Control.”
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Radigan, R., Kao, C.S., Krainock, M. et al. Long-term survival and undetectable circulating tumor DNA following comprehensive involved site radiotherapy for oligometastases. Sci Rep 15, 6126 (2025). https://doi.org/10.1038/s41598-025-88266-z
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-88266-z
