
Abstract
Background: The detection of pulmonary nodules is increasing every year, as well as the need for surgical treatment in more patients, which places a significant burden on surgeons. Surgeon fatigue not only increases surgical risk, but also poses a health hazard to the surgeons. How to reduce surgeon fatigue is an important issue that needs to be addressed urgently. Methods: We collected 917 patients who underwent thoracoscopic surgery between 2022 and 2023. They were categorized into thoracoscopy group, mechanical arm group and pneumatic arm group according to the procedure. Data related to the perioperative period (operative time, blood loss, serious adverse events, etc.) of different patients were retrospectively analyzed. The related scale of fatigue index was also designed to quantify and analyze the fatigue index of doctors. Results: There were 316, 302 and 299 patients in the thoracoscopic, mechanical and pneumatic arm groups, respectively. There was no statistically significant difference in operative time, bleeding, mean length of hospital stay, and serious adverse events among the three groups. Although there was no significant difference in overall surgical fatigue scores among the three groups, the use of robotic and pneumatic arms significantly reduced the fatigue of surgeons and assistants in complicated surgeries. Conclusion: Compared to traditional thoracoscopic surgery, the application of surgical assistance robotic arm does not increase perioperative risk. Moreover, in longer thoracoscopic procedures, it significantly reduces fatigue for both the surgeons and their assistants. However, current robotic arms still have certain limitations and require continuous improvements to better meet clinical demands.
Similar content being viewed by others
Introduction
In China, the detection rate of pulmonary nodules is gradually increasing, leading to a rising number of patients requiring lung surgery1. This trend has been further accelerated by the COVID-19 pandemic, as more people opt for chest computed tomography (CT) scans as a routine check-up measure2,3,4. Hundreds of thousands of lung surgeries are performed annually at various levels of hospitals. Minimally invasive lung surgery is now the mainstream approach for lung operations5,6,7. However, due to the high cost of the Da Vinci surgical robot, it is not yet widely adopted, and thoracoscopic minimally invasive surgery remains the predominant method8,9,10.
Traditional thoracoscopic surgery requires a lead surgeon and one to two assistants to complete the operation11. This is a significant physical challenge for the assistants, and any lack of coordination can affect the stability of the thoracoscope, thereby impacting the lead surgeon’s performance and the safety of the surgery12. Recent studies have shown that the fatigue level of surgeons significantly affects the quality of medical services and patient safety. Prolonged excessive fatigue severely impacts the physical and mental health of surgeons and poses a threat to patient safety13,14. Therefore, alleviating surgical fatigue for surgeons and their assistants is a pressing issue in modern healthcare.
Researchers have conducted numerous studies on how to address surgeon fatigue15,16,17. We used some assistive devices for use during surgery and developed a questionnaire to assess the fatigue levels of thoracic surgeons. We retrospectively analyzed the perioperative data of patients who underwent traditional thoracoscopic surgery and those who underwent surgery with the assistance of robotic arms over the past two years. This analysis aimed to address the physical and mental fatigue issues faced by surgeons during prolonged surgeries.
Methods
Patients
All patients were from the Thoracic Surgery Department of the First Affiliated Hospital of Zhejiang University School of Medicine. The surgeries took place between August 2022 and November 2023, with a total of 917patients participating in the study. The patients ranged in age from 16 to 82 years old, and all signed informed consent forms. This study was approved by the Ethics Committee of the First Affiliated Hospital of Zhejiang University. And all treatments were performed in accordance with relevant guidelines/regulations18,19,20.
Surgical methods
All patients underwent thoracoscopic surgery. The surgical approach utilized a single operation port technique. Depending on the location of the patient’s lesion, the observation port was typically placed at the seventh or eighth intercostal space along the mid-axillary line, while the operation port was positioned at the fourth or fifth intercostal space along the anterior axillary line.
Perioperative indicators
Perioperative data of the patient was collected, encompassing details such as the surgical procedure performed, duration of surgery, blood loss, length of hospital stay, and the occurrence of severe complications during hospitalization (e.g., major bleeding, conversion to thoracotomy, unplanned reoperation, pulmonary infection, or admission to the intensive care unit).
Robotic arm assistance device
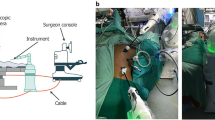
Both types of thoracoscopic assistance devices were produced by Hangzhou Kangsheng Medical Equipment Company. One device is a traditional mechanical arm, while the other is a pneumatic arm equipped with an air pump (Fig. 1A and B). Both devices were installed according to the manufacturer’s recommendations. During surgery, the devices were attached to the sliding rail on one side of the operating table, covered with a sterile protective cover, and the camera was fixed onto the corresponding device (Fig. 1C and D).

Design Diagrams of Different Robotic Arms. (A) Traditional mechanical arm; (B) Pneumatic arm. (C) The application of mechanical arm; (D) The application of Pneumatic arm.
Surgeon fatigue assessment scale
We designed a scale to evaluate surgeons’ post-operative fatigue and surgical satisfaction(Supplementary Table 1 ). The surgeons filled out the form immediately after completing the surgery. We used a quantitative scoring method to summarize the final data, lower scale scores indicate more surgeon fatigue. This scale was used to assess the surgeons’ fatigue levels and satisfaction with different types of surgeries.
Statistical analysis
All statistical analyses were conducted using SPSS 23.0 for windows (SPSS Inc., Chicago, USA) and GraphPad Prism (GraphPad Software Inc, USA). Data are presented as the means ± standard deviation. P values < 0.05 indicate statistical significance.
Result
Baseline data
All patients participating in the study underwent surgical treatment. According to the different surgical methods, they were divided into three groups: traditional thoracoscopic surgery group, mechanical arm group, and pneumatic arm group. All surgeries were performed under thoracoscopy, with 806 cases of lung cancer and the remaining cases involving benign lung lesions. Detailed information can be found in Table 1.
Impact of robotic arm application on perioperative safety
We collected perioperative data for the three groups, including surgery duration, intraoperative blood loss, hospital stay length, and major perioperative complications (e.g., major bleeding, conversion to thoracotomy, unplanned reoperation, pulmonary infection, or admission to the intensive care unit) in Table 2. The results showed that the average surgery durations for the different groups were 73.7 min, 73.9 min, and 69.2 min, respectively, with no significant differences observed. The average intraoperative blood loss was 28.5 ml, 24.7 ml, and 30.6 ml, respectively, with no significant statistical differences. The use of the mechanical arm did not result in perioperative adverse events. The average postoperative hospital stays were 4.7 days, 4.9 days, and 4.8 days, respectively, with no significant differences. There were 10, 8, and 9 cases of severe postoperative adverse events in each group, respectively, and no perioperative deaths occurred.
Reduction of surgeon fatigue with robotic arm in lung surgery
By analyzing and summarizing the evaluation scale, the results indicated that the use of the robotic arm did not significantly reduce surgeon fatigue in simple surgeries, such as lung wedge resection(Fig. 2A, C). However, in more complex surgeries (including those lasting over 100 min and complicated segmental lung resections), the robotic arm significantly alleviated surgeon fatigue, The scores for surgeons were 7.1(Thoracoscopic Surgery), 7.6(Mechanical Arm) and 7.9(Pneumatic Arm) respectively, while the scores of surgical assistants were 6.5(Thoracoscopic Surgery), 7.7(Mechanical Arm) and 7.9(Pneumatic Arm) (Fig. 2B, D).

Fatigue Scale Scores for Surgeons and Assistants. (A) In all surgeries, there were no significant differences in the fatigue scale scores of the surgeons; (B) In surgeries lasting more than 100 min, the use of mechanical and pneumatic arms significantly reduced the fatigue levels of the surgeons. (C) In all surgeries, there were no significant differences in the fatigue scale scores of the surgical assistant. (D) In surgeries lasting more than 100 min, the use of mechanical and pneumatic arms significantly reduced the fatigue levels of the surgical assistant. *P<0.05, **P<0.01, ****P<0.0001.
Discussion
Fatigue is an inevitable effect of performing surgery, impairing both cognitive function and psychomotor performance. While surgical fatigue poses a significant threat to patient safety in the perioperative period. Fatigue can diminish concentration, slow reaction times, and impair decision-making, increasing the risk of complications such as incorrect incisions, improper suturing, or even overlooking critical steps in the surgery21,22. These errors can result in adverse outcomes for patients, including prolonged recovery times, additional surgeries, or in severe cases, life-threatening complications23,24. Moreover, the stress and mental exhaustion associated with surgical fatigue can lead to burnout among medical staff, further compromising the quality of care25. The cumulative effect of fatigue not only endangers the immediate safety of the patient on the operating table but also undermines the overall effectiveness of the healthcare system.
During surgery, surgeons are often in a state of mental tension and non-ergonomic positions, leading to muscle fatigue and mental fatigue26,27,28. Minimally invasive surgery requires a high level of concentration from the surgeons. Research have shown that prolonged high-pressure work and fatigue pose significant threats to the health of doctors, but also have led to adverse patient outcomes14,21,29,30. In China, the detection rate of pulmonary nodules is gradually increasing, leading to a rising number of patients requiring lung surgery1. This creates significant pressure on the healthcare system, particularly for thoracic surgeons. Addressing surgeon fatigue and ensuring safe and effective surgeries under heavy workloads is a major challenge30.
Similar to previous research, the surgical assistance robotic arm we designed is fixed to the side of the operating table, providing support for the thoracoscope31,32,33. This support is more stable than manual handling and allows convenient visual adjustments according to the lead surgeon’s needs33,34,35,36. Our clinical application revealed that the use of the robotic arm did not increase perioperative risk, with no perioperative deaths observed. Additionally, in complex lung surgeries, the robotic arm, especially the pneumatic arm, effectively reduced fatigue for both the surgeon and the assistant. Moreover, the use of robotic arms is highly convenient. After providing basic training to thoracic surgeons in local hospitals, they can quickly become proficient in using robotic arms during thoracoscopic surgeries. We also found that it is possible to perform unassisted thoracoscopic surgery through the use of a robotic arm thereby, which may provide new insights for future solo surgeon thoracoscopic surgery.
However, we also identified some drawbacks and limitations in its use. Although the robotic arm installation is relatively simple, it still requires about ten minutes for setup and sterilization. The traditional mechanical arm is prone to wear and deformation, while the pneumatic arm is bulky. These issues could be addressed in future research for further improvement and optimization.
Conclusion
Compared to traditional thoracoscopic surgery, the application of surgical assistance robotic arm does not increase perioperative risk. Moreover, in longer thoracoscopic procedures, it significantly reduces fatigue for both the surgeons and their assistants. However, current robotic arms still have certain limitations and require continuous improvements to better meet clinical demands.
Data availability
The datasets used and/or analysed during the current study available from the corresponding author on reasonable request.
References
Zheng, R. S. et al. Cancer incidence and mortality in China, 2022. Zhonghua Zhong Liu Za Zhi. 46 (3), 221–231 (2024).
Milanese, G. et al. Feasibility and safety of Lung Cancer Screening and Prevention Program during the COVID-19 pandemic . Chest 160 (1), e5–e7 (2021).
Mazzone, P. J. et al. Management of lung nodules and Lung Cancer Screening during the COVID-19 pandemic: CHEST Expert Panel Report. Chest 158 (1), 406–415 (2020).
Gysling, S. et al. The impact of COVID-19 on Lung Cancer incidence in England: analysis of the National Lung Cancer Audit 2019 and 2020 Rapid Cancer Registration datasets [J]. Chest 163 (6), 1599–1607 (2023).
Bendixen, M., Jorgensen, O. D., Kronborg, C., Andersen, C. & Licht, P. B. Postoperative pain and quality of life after lobectomy via video-assisted thoracoscopic surgery or anterolateral thoracotomy for early stage lung cancer: a randomised controlled trial . Lancet Oncol. 17 (6), 836–844 (2016).
Lee, P. C. et al. Lobectomy for Non-small Cell Lung Cancer by Video-assisted thoracic surgery: effects of cumulative institutional experience on adequacy of lymphadenectomy . Ann. Thorac. Surg. 101 (3), 1116–1122 (2016).
Yang, C. J. et al. A minimally invasive Approach to Lobectomy after induction therapy does not compromise survival . Ann. Thorac. Surg. 109 (5), 1503–1511 (2020).
Pan, H. et al. Short-term outcomes of robot-assisted versus video-assisted thoracoscopic surgery for non-small cell lung cancer patients with neoadjuvant immunochemotherapy: a single-center retrospective study. Front. Immunol. 14, 1228451 (2023).
Upham, T. C. & Onaitis, M. W. Video-assisted thoracoscopic surgery versus robot-assisted thoracoscopic surgery versus thoracotomy for early-stage lung cancer . J. Thorac. Cardiovasc. Surg. 156 (1), 365–368 (2018).
Musgrove, K. A., Hayanga, J. A., Holmes, S. D., Leung, A. & Abbas, G. Robotic Versus Video-assisted thoracoscopic surgery pulmonary segmentectomy: a cost analysis. Innovations (Phila). 13 (5), 338–343 (2018).
Grossi, S., Cattoni, M., Rotolo, N. & Imperatori, A. Video-assisted thoracoscopic surgery simulation and training: a comprehensive literature review. BMC Med. Educ. 23 (1), 535 (2023).
Thurston, T. et al. Assessment of muscle activity and fatigue during laparoscopic surgery . Surg. Endosc. 36 (9), 6672–6678 (2022).
Asfour, L., Asfour, V., McCormack, D. & Attia, R. In surgeons performing cardiothoracic surgery is sleep deprivation significant in its impact on morbidity or mortality?. Interact. Cardiovasc. Thorac. Surg. 19 (3), 479–487 (2014).
Rothschild, J. M. et al. LANDRIGAN C P. risks of complications by attending physicians after performing nighttime procedures. JAMA 302 (14), 1565–1572 (2009).
Sakai, D. et al. Adolescent idiopathic scoliotic deformity correction surgery assisted by Smart glasses can enhance correction outcomes and accuracy and also improve surgeon fatigue. World Neurosurg. 178, e96–e103 (2023).
Wong, S. W. & Crowe, P. Visualisation ergonomics and robotic surgery. J. Robot Surg. 17 (5), 1873–1878 (2023).
Emam, T. A., Frank, T. G., Hanna, G. B. & Cuschieri, A. Influence of handle design on the surgeon’s upper limb movements, muscle recruitment, and fatigue during endoscopic suturing. Surg. Endosc. 15 (7), 667–672 (2001).
Saji, H. et al. West Japan Oncology G, Japan Clinical Oncology G. Segmentectomy versus lobectomy in small-sized peripheral non-small-cell lung cancer (JCOG0802/WJOG4607L): a multicentre, open-label, phase 3, randomised, controlled, non-inferiority trial. Lancet 399 (10335), 1607–1617 (2022).
Oncology Society of Chinese Medical & Chinese Medical Association Publishing, A. [Chinese Medical Association guideline for clinical diagnosis and treatment of lung cancer (2023 edition)]. Zhonghua Yi Xue Za Zhi. 103 (27), 2037–2074 (2023).
Aokage, K. et al. Japan Clinical Oncology G. Segmentectomy for ground-glass-dominant lung cancer with a tumour diameter of 3 cm or less including ground-glass opacity (JCOG1211): a multicentre, single-arm, confirmatory, phase 3 trial. Lancet Respir Med. 11 (6), 540–549 (2023).
Reijmerink, I. M., Van der Laan, M. J., Wietasch, J. K. G., Hooft, L. & Cnossen, F. Impact of fatigue in surgeons on performance and patient outcome: Systematic review. Br. J. Surg., 111(1). (2024).
Kahol, K. et al. Effect of fatigue on psychomotor and cognitive skills. Am. J. Surg. 195 (2), 195–204 (2008).
Gawande, A. A., Zinner, M. J., Studdert, D. M. & Brennan, T. A. Analysis of errors reported by surgeons at three teaching hospitals. Surgery 133 (6), 614–621 (2003).
Gerdes, J., Kahol, K., Smith, M., Leyba, M. J. & Ferrara, J. J. Jack Barney award: the effect of fatigue on cognitive and psychomotor skills of trauma residents and attending surgeons. Am J Surg, 196(6): 813-9; discussion 9–20. (2008).
Mccormick, F. et al. Surgeon fatigue: a prospective analysis of the incidence, risk, and intervals of predicted fatigue-related impairment in residents. Arch. Surg. 147 (5), 430–435 (2012).
Cohen-Gadol, A. A. Surgeon’s philosophy and ergonomic operating position: advancing efficiency and minimizing fatigue during microsurgery. World Neurosurg. 141, 580–582 (2020).
Yang, L. et al. Impact of Procedure Type, Case Duration, and Adjunctive Equipment on Surgeon Intraoperative Musculoskeletal discomfort. J. Am. Coll. Surg. 230 (4), 554–560 (2020).
Yang, L. et al. ND, Intraoperative musculoskeletal discomfort and risk for surgeons during open and laparoscopic surgery. Surg Endosc, 35(11): 6335-43. (2021).
Olasky, J. et al. Effects of sleep hours and fatigue on performance in laparoscopic surgery simulators. Surg. Endosc. 28 (9), 2564–2568 (2014).
Sun, E. C. et al. Assessment of Perioperative outcomes among surgeons who operated the night before. JAMA Intern. Med. 182 (7), 720–728 (2022).
Partin, A. W., Adams, J. B., Moore, R. G. & Kavoussi, L. R. Complete robot-assisted laparoscopic urologic surgery: a preliminary report. J. Am. Coll. Surg. 181 (6), 552–557 (1995).
Mittal, R., Sbaih, M., Motson, R. W. & Arulampalam, T. Use of a robotic camera holder (FreeHand((R))) for laparoscopic appendicectomy. Minim. Invasive Ther. Allied Technol. 29 (1), 56–60 (2020).
Chung, D. G. et al. Bed-mounted laparoscopic surgical robot system with novel positioning arm mechanism. Int. J. Med. Robot. 18 (4), e2402 (2022).
Gonzalez-Rivas, D. Unisurgeon’ uniportal video-assisted thoracoscopic surgery lobectomy. J. Vis. Surg. 3, 163 (2017).
Migliore, M. Uniportal video-assisted thoracic surgery, and the uni-surgeon: new words for the contemporary world. J. Vis. Surg. 4, 45 (2018).
Migliore, M. Will the widespread use of uniportal surgery influence the need of surgeons?. Postgrad. Med. J. 92 (1086), 240 (2016).
Acknowledgements
We all authors appreciate Stryker Corporation (USA) and Hangzhou Kangsheng Medical Equipment Company for their technical support.
Funding
This work was supported by the Key R&D Program of Zhejiang (grant number: 2022C04030) and the Natural Science Foundation of Zhejiang Province (grant number: Q234020022).
Author information
Authors and Affiliations
Contributions
Qingyi Zhang, Honghai Ma and Lei Ke wrote the main manuscript text and Zhehao He, Chunlin Zhou completed data Collection, Wang Lv, Jian Hu and Luming Wang completed data analysis. Luming Wang managed the project.All authors reviewed the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Supplementary Material 2
Supplementary Material 3
Supplementary Material 4
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Zhang, Q., Ma, H., Ke, L. et al. Application and exploration of surgical assistive arms in thoracoscopic surgery: a single-center retrospective study. Sci Rep 15, 5606 (2025). https://doi.org/10.1038/s41598-025-89897-y
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-89897-y
Keywords
This article is cited by
-
Prescribed-time trajectory tracking control for manipulators based on disturbance observers
Nonlinear Dynamics (2025)
