
Abstract
Ventilation/perfusion (V/Q) matching represents a crucial indicator of lung function. The current for assessing V/Q in a clinical setting are inadequate for bedside monitoring purposes. They are characterised by invasiveness and an increased risk of infection. Accordingly, the present study was based on a high-performance electrical impedance tomography (EIT) system developed by our team, with the objective of exploring the feasibility of using it for non-invasive assessment of V/Q at the bedside. This was achieved by acquiring and imaging pulmonary blood flow pulsation signals and combining them with pulmonary ventilation impedance information. Continuous lung EIT imaging data were acquired at 40 fps through different body positions and breath-holding in anaesthetised domestic pigs (N = 8, 17.50 ± 1.51 kg). By analysing the blood flow pulsation impedance information, lung perfusion-related data were extracted and combined with lung ventilation impedance data to establish a pulsatility V/Q assessment method. Furthermore, the monitoring of pulmonary perfusion using hypertonic saline (5 ml of 10% NaCl) was employed as a control experiment. The results demonstrate that the V/Q results obtained through the utilisation of both methodologies exhibit a notable degree of variability in response to alterations in body position and the state of breath holding. The V/Q results obtained using the pulsatility method and the saline method were subjected to analysis using the Bland–Altman agreement test. During end-expiration breath-holding in the supine position, the results were as follows: 95% CI = 2.36% to 10.26%, bias = 6.309%. During end-inspiration breath-holding in the supine position, the results were as follows: 95% CI = 0.07% to 12.23%, bias = 6.150%. During end-expiration breath-holding in the prone position, the results were as follows: 95% CI = -0.40% to 14.43%, bias = 7.014%. During end-inspiration breath-holding in the prone position, the results were as follows: 95% CI = 1.92% to 11.17%, bias = 6.541%. Moreover, a Pearson correlation analysis revealed a significant correlation between the V/Q match% of the two methods (r = 0.7248; 95% CI = 0.50% to 0.86%; p < 0.0001). Consequently, EIT imaging based on the pulsatility method is capable of assessing V/Q alterations resulting from diverse body positions and changes during breath-holding. This approach offers a novel concept for bedside monitoring of patients.
Similar content being viewed by others
Introduction
The assessment of local lung ventilation/lung perfusion matching is of significant importance for the monitoring of patients with acute respiratory distress syndrome (ARDS), chronic obstructive pulmonary disease (COPD) and respiratory failure, as well as for monitoring patients with related lung diseases1. At present, the clinical imaging techniques employed for the assessment of lung ventilation/perfusion matching remain magnetic resonance imaging (MRI), computed tomography (CT), and single photon emission compensation tomography (SPECT)2,3,4. However, these existing techniques do not allow for bedside monitoring and have the disadvantages of inconvenient operation, high cost and high risk of transportation2,3,4. It is for this reason that a non-invasive, rapid, and continuous bedside monitoring system for lung ventilation and perfusion information has been developed in order to explore the potential demand for monitoring lung ventilation and lung perfusion in current clinical practice.
Electrical Impedance Tomography (EIT) is a functional imaging technique that offers high temporal resolution, high impedance sensitivity, and real-time dynamic non-invasive bedside monitoring5. The fundamental tenet of the measurement process is the periodic application of excitation signals to the object via the electrodes positioned on its surface6,7. The ensuing response signals are then detected at the measurement electrodes and combined with the appropriate reconstruction algorithms to yield an the image of the impedance changes occurring within the object7. EIT technology is currently employed in a diverse array of applications. At present, EIT technology is used in a multitude of applications, including the imaging of lung function, brain function, breast cancer detection, and abdominal organs6,7,8. Among these applications, pulmonary impedance technology is capable of detecting impedance changes resulting from pulmonary activity, and it can also discern the degree of matching between pulmonary ventilation and pulmonary perfusion9. A substantial body of evidence attests to the favourable prospects of EIT in the assessment of pulmonary ventilation5,6,9. This approach can enhance the patient’s pulmonary ventilation status through positional adjustments, thereby facilitating the clinician’s diagnosis and treatment, including positive end expiratory pressure (PEEP) titration, and pulmonary resuscitation9.
The EIT technique is currently employed in the assessment of pulmonary ventilation, although its use in the assessment of pulmonary perfusion remains in the exploratory phase6,9. The assessment of pulmonary perfusion is primarily conducted through two main approaches. The first approach entails the generation of pulsatile alterations resulting from the cardiac rhythm and the subsequent pulmonary blood flow pulsation10. This process yields data that reflect pulmonary perfusion, a phenomenon known as the pulsatility method10. A review of the current status of the pulsatility method for monitoring pulmonary perfusion by Tan et al. revealed that the relatively weak changes in impedance of cardiac pulsatile blood flow make the pacing method extremely demanding on the accuracy of the EIT acquisition system10. Furthermore, the results of the pacing method for monitoring the pulmonary perfusion status may be affected by a variety of factors (e.g., changes in position and respiratory status), and the reliability of the results needs to be further improved10. Secondly, a central venous puncture and injection of a high-conductivity contrast agent (e.g., 10% NaCl solution) in the form of a “bullet” at under breath-hold is employed to enhance perfusion for a brief period11. This is employed to augment impedance alterations in the perfused region for a brief interval and to undertake EIT imaging. Studies have demonstrated a positive correlation between the results obtained by the hypertonic saline method in pulmonary perfusion function testing and those produced by PET and SPECT11,12. Furthermore, researcher has obtained preliminary clinical approval for measuring pulmonary blood flow perfusion using the hypertonic saline contrast technique13. Additionally, previous research has published consensus statements on the technique of pulmonary EIT14. However, the method is not without limitations, including invasiveness, inability to provide real-time data, and operational inconvenience. Consequently, it is not a viable option for bedside monitoring of local pulmonary ventilation/perfusion.
The team has a long-standing commitment to the research of key technologies associated with the acquisition and imaging of high-precision EIT data7,15 Recently, we have developed a high-performance imaging system with a measurement accuracy of better than 0.01‰7,15. On this basis, we conducted research on real-time non-invasive lung perfusion monitoring methods based on pulmonary blood flow pulsation, which were combined with lung ventilation to study the effects of different body positions (supine and prone) and different breath-holding states (end-expiratory breath-holding and end-inspiratory breath-holding) on alterations in pigs on the V/Q matching.
Methods
Objects and instruments
Experimental animals
The experimental subjects were eight anaesthetised Long White pigs of both sexes. The mean weight and mean chest circumference of the subjects were 17.50 ± 1.51 kg and 56.00 ± 2.33 cm, respectively. The subjects ranged in age from 2.0 to 2.5 months.The study was approved by the Animal Welfare and Ethics Committee of the Air Force Military Medical University (Licence No. IACUC-20241299). All experiments were conducted in accordance with the guidelines and regulations set forth by the Air Force Military Medical University.
EIT imaging instrumentation
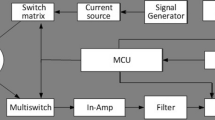
In this study, we employed the EC-100 pro high-performance EIT system, which was developed by the research group in collaboration with UTRON Technology Co., Ltd., Hangzhou, China7,15. The maximum acquisition speed of the system is up to 100 fps, and the data acquisition accuracy is superior to 0.01‰ within the range of 10 kHz to 250 kHz. The data acquisition is conducted through the working modes of opposite excitation and adjacent measurement. Each data acquisition parameter is set as follows: the number of electrodes is 16, the frame rate is 40 fps, the excitation current amplitude is 1.25 mA, and the frequency is 50 kHz.
Animal model experiments
Animal preparation
Prior to the commencement of the experiment, the animals were fasted and dehydrated for a period of 12 h. Their body temperature, respiration and heart rate were then confirmed to be within the normal range. The surgical protocol was as follows: anaesthesia was induced by intravenous injection of propofol (10 mg/kg) at the ear margin, followed by maintenance of anaesthesia with isoflurane gas. This was immediately followed by tracheal intubation and connection to a respiratory anaesthesia machine (Mindray WATO EX-65), with the respiratory rate set at 14 breaths/min, tidal volume of 310 ml, ventilation rate of 5.7 L/min, and an airway pressure of no more than 40 cm/H2O. Subsequently, a central venous catheter was introduced into the left internal jugular vein and sutured. Throughout the course of the experiments, an animal monitor (PHILIPS MX500) and an animal non-invasive sphygmomanometer (MINDRAY) were employed to monitor the experimental subjects (Fig. 1A). The ventilator parameters were adjusted during the surgical procedure based on physiological parameters, including electrocardiogram, blood pressure, heart rate, and oxygen saturation.

Experimental animals, instrument preparation and flowchart. (A) Experimental apparatus; (B) EIT acquisition system, electrode tape (white) and electrode wires (black); (C) Experimental animals; (D) Flowchart of the experiment in the supine position; (E) Flowchart of the experiment in the prone position.
Experimental flow
The animal’s chest and back were shaved and subsequently treated with a combination of alcohol and abrasive cream. Subsequently, electrode tapes containing 16 electrodes (Fig. 1B) were placed horizontally around the porcine subject’s chest in a uniform configuration for one full circle, and the electrodes were secured by self-adhesive bandages. The electrodes were then connected to the EIT device, which was used for the acquisition of data and monitoring of the images. Simultaneously, the photoplethysmography (PPG) sensor finger cuff was secured to the edge of the animal’s ear (Fig. 1C), where the PPG was measured by the EIT device. The signal obtained not only the heart rate information of the animal, but also verified the cycle accuracy of the perfusion signal by comparing it with the EIT perfusion signal.
The EIT control monitoring experiment was divided into two principal phases, each comprising four subphases, as illustrated in Fig. 1D,E:
-
(1)
Supine position monitoring under pulsatility method vs. hypertonic saline
The EIT data were acquired continuously for a period of 30 min, during which time all of the animal’s physiological parameters remained stable. This allowed for the recording of impedance and image changes during pulmonary ventilation. The end-expiratory breath-holding was achieved by administering a small dose of propofol (2 mg/kg) and regulating the ventilator to obtain 20 cycles of blood flow pulsatile perfusion data and imaging. Subsequently, a hypertonic saline contrast agent (5 ml of 10% NaCl) was injected via a central venous catheter to continuously acquire and observe the impedance and image changes associated with the pulmonary perfusion process for 5–6 s. The entire end-expiratory pause state was maintained for approximately 45 s, after which autonomous respiration was resumed. Once the animal’s various physiological indexes had stabilised, the lung ventilation EIT data were collected continuously for 30 min. This was followed by end-inspiratory breath-holding, which was completed only by controlling the ventilator. The monitoring methods and processes were identical to those employed during the end-expiratory pause.
-
(2)
Prone position monitoring under pulsatility method vs. hypertonic saline
Following a change in the position of the animal and a period of observation to ensure stability of the animal’s physiological indexes, the EIT data were collected continuously for approximately 30 min to observe impedance and image changes associated with the pulmonary ventilation process. Subsequently, the impedance and image changes associated with the blood flow pulsatile perfusion and hypertonic saline perfusion process were monitored during the end-expiratory and end-inspiratory breath-holds, which were conducted in the same manner as in the supine position.
Following the completion of all experiments, the animals were euthanised with an overdose of anaesthetic (propofol, 50 mg/kg, administered intravenously at the ear margin).
A new method for extracting V/Q based on the pulsatility EIT technique
Once the raw data had been obtained, the effect of the blood flow beat signal was first removed during mechanical ventilation by means of frequency filtering, thus facilitating late lung ventilation imaging. Subsequently, the blood flow beat signal was extracted from the pulmonary blood flow booster impedance information during breath-hold for late lung perfusion imaging. This extraction was performed prior to the injection of hypertonic saline during breath-hold. Finally, cardiac information was extracted using the PPG signal, and the cardiac region of interest was removed for V/Q extraction in conjunction with imaging of lung ventilation and lung perfusion.
EIT data processing and image reconstruction
The data processing stage of this study concerns the processing of the boundary voltage signal, which reflects the distribution of conductivity within the lung. Subsequently, the signal was filtered using a band-pass filter with a cut-off frequency of 1Hz to 5Hz, resulting in the acquisition of the final measurement data, which reflected the lung information over time15. In this study, the mean value of the boundary voltage of a data frameis defined as the global boundary voltage (GBV), which is expressed as follows:
where N represents the number of channels, and the Vchn is the boundary voltage value of the nth measurement sequence.
The image reconstruction in this study is a dynamic differential reconstruction utilising a data-driven linear reconstruction algorithm that relies on a data-driven linear reconstruction algorithm, the Gratz consensus reconstruction algorithm for EIT, GREIT16. This algorithm was initially proposed and applied to lung impedance imaging by Adler’s group in 200916. The fundamental concept of the GREIT algorithm is designed to train a series of simulation data as a training target, with the objective of obtaining a reconstruction matrix R that minimises the error of the reconstructed image17. This matrix can then be used directly to obtain the impedance distribution when reconstructing other data17.
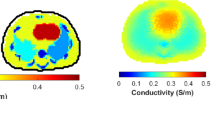
Ultimately, from the acquired and processed measurement data are used to reconstruct and visualise an internal lung tomographic image is reconstructed and visualised on the EIT acquisition platform, thereby obtaining information on the characteristics of the lung conductivity distribution18. The EIT acquisition platform is employed to obtain information about the distribution of conductivity in the lungs.
Furthermore, a comparison was conducted between the GBV and PPG changes during the experimental breath-hold, with the objective of obtaining the corresponding global boundary voltage over time curve (GBV-Time curve) and photoelectric volumetric tracings over time curve (PPG-Time curve). This was done in order to confirm the correlation between them. As illustrated in Fig. 2A, the EIT signal data obtained in the supine position were selected for analysis. It can be observed that the GBV changes during the breath-hold (red) are significantly correlated with the PPG changes at the corresponding moment (green). As illustrated in Fig. 2B, we randomly selected PPG and blood flow perfusion impedance GBV data for three consecutive cycles during end-expiratory breath-holds for analysis and image reconstruction. This was done to further illustration the changes in impedance of the heart and lung lobes due to the perfusion cycle, Fig. 2C depicts the alteration in the mean impedance of the region of interest (ROI)15.

EIT data acquisition in the supine position. (A) Corresponding change curves of global boundary voltage (GBV) and photoplethysmographic volumetric tracings (PPG) for lung ventilation and lung perfusion; (B) Changes in GBV, PPG during three consecutive heartbeat cycles at end-expiration during breath-hold; (C) Delineation of regions of interest, where red boxes indicate cardiac regions and blue boxes indicate pulmonary regions.
With regard to the delineation of regions of interest, given that EIT images are obtained from the chest, it is possible that they may also encompass heart and lung tissue. Consequently, in order to obtain the lung region of interest, it is first necessary to calculate the heart and lung region of interest, then to subtract the heart region of interest, and finally to obtain the lung region of interest. The heart–lung region of interest is typically indicative of the degree of correlation between the impedance change waveform of each pixel and the total impedance waveform, and it is obtained through the application of a linear regression method. The region of interest in the heart is obtained via PPG signals.
Calculation of lung ventilation/lung perfusion matching images
In order to identify the region of ventilation and perfusion, a threshold of 20% of the maximum pixel reconstruction value is applied to the ventilation and perfusion images, as illustrated in the blue box in Fig. 2. This threshold is then used to construct the V/Q matching image, which is created by combining the ventilated and perfused regions19. The specific construction process of the ventilation and perfusion regions is as follows:
The ventilation region was constructed by first acquiring the lung EIT data of each respiratory cycle. The end-expiratory moment (corresponding to the trough moment) was selected as the reference frame for EIT imaging of one respiratory cycle, allowing for the generation of a representative image of the lung ventilation at a given point in time. Subsequently, the impedance changes of five consecutive respiratory cycles were averaged, and the result was used as the pixel reconstruction value of the lung ventilation image, designated as \(\Delta Z_{V}\). This value enables the reconstruction of the global lung ventilation distribution image. The formula for \(\Delta Z_{V}\) is as follows:
Of these, the \(\Delta Z_{in,i}\) and \(\Delta Z_{ex,i}\) denote the relative impedance changes at the end-inspiratory and end-expiratory moments of the ith respiratory cycle, respectively, and MV denotes the number of respiratory cycles.
The perfusion region was constructed by first acquiring the lung EIT data during each breath-hold. The cardiac contraction moment, corresponding to the wave peak moment, was selected as the reference frame for one cardiac cycle of EIT imaging. Subsequently, the mean of the impedance changes observed over 10 consecutive cardiac cycles was calculated and used as the pixel reconstruction value of the lung perfusion image, \(\Delta Z_{Q}\). This value enables the reconstruction of a global lung perfusion distribution image. The formula for \(\Delta Z_{Q}\) is as follows:
Of these, the \(\Delta Z_{ca,i}\) and \(\Delta Z_{cd,i}\) denote the relative impedance changes at the moment of cardiac systole and the moment of cardiac diastole of the ith cardiac cycle, respectively, and MQ denotes the number of cardiac cycles.
The final division is based on the construction of the lung ventilation/perfusion area. The V/Q match area is represented by RV+P, which denotes the pixel overlay area of ventilation and perfusion20. The DeadSpace area is represented by RV, which denotes the pixel area of ventilation20. The Shunt area is represented by RP, which denotes the pixel area for perfusion20. The formula for calculating each area are as follows:
V/Q extraction based on hypertonic saline EIT technique
The hypertonic saline method is a method involves the injection of 5 ml of 10% NaCl solution into a central vein of a pig during a breath-hold, thereby obtaining lung perfusion-enhanced contrast imaging11,13. As illustrated in the black box in Fig. 2A, the initial point of saline entry into the animal was recorded as P0, which was the moment when the GBV-Time curve began to decline; the starting point of saline entry into the pulmonary vasculature was recorded as P1, occurring one second after the initial point; the endpoint of the first passage of saline through the pulmonary circulation was recorded as P2, occurring at the lowest point of global impedance. Ultimately, the V/Q data obtained from hypertonic saline method monitoring was extracted in accordance with the methodology proposed by He et al13.
EIT data analysis and statistics
The EIT data acquisition and online image reconstruction were conducted using the EC-100 pro, while the offline data analysis and image reconstruction were performed using Matlab R2022b (Mathworks, Natick, Massachusetts, USA) based on EIDORS V3.1016,21. The imaging algorithm employed was the Gratz consensus reconstruction algorithm for EIT, GREIT algorithm16.
A total of 32 data sets were obtained in this study, comprising four sets of eight data points each, with the data from eight pigs included in the statistical analysis. The primary effects were the effects of varying body positions and end-expiratory/end-inspiratory pause modalities on V/Q data. These data were processed using SPSS 27.0 software and GraphPad software. The results were tested using analysis of variance (ANOVA), the V/Q results obtained by the two methods were compared using a Bland–Altman agreement analysis and a Pearson correlation analysis22,23. A value of P < 0.05 is deemed to be statistically significant.
Results
Pulsatility method to monitor the effect of on V/Q during different positions and breath-holds
As illustrated in Fig. 3A,C,E,G , our findings revealed that alterations in position and during breath-holding resulted in notable variations in pulmonary perfusion when employing the pulsatility method for monitoring pulmonary perfusion in different positions and breath-holding states. Figure 4 depicts the corresponding images of lung ventilation and lung perfusion obtained through the pulsatility method in different positions and breath-holding periods. The figures are designated as follows: I represents the supine end-expiratory breath-holding period, II represents the supine end-inspiratory breath-holding period, III represents the prone end-expiratory breath-holding period, and IV represents the prone end-inspiratory breath-holding period.

Sequence of EIT cycle images. (A) pulsatility method during end-expiratory breath-hold, (B) hypertonic saline method during end-expiratory breath-hold, (C) pulsatility method during end-inspiration breath-hold, (D) hypertonic saline method during end-inspiration breath-hold; (E) pulsatility method during end-expiratory breath-hold, (F) hypertonic saline method during end-expiratory breath-hold, (G) pulsatility method during end-inspiration breath-hold, (H) hypertonic saline method during end-inspiration breath-hold. V: corresponds to the actual Ventral side, R: corresponds to the actual Right side, D: corresponds to the actual Dorsal side, L: corresponds to the actual Left side.

V/Q-matched images. (A) Pulsatility method; (B) Hypertonic saline method; I. Supine position during end-expiratory breath-hold; II. Supine position during end-inspiratory breath-hold; III. Prone position during end-expiratory breath-hold, IV. Prone position during end-inspiratory breath-hold. V: corresponds to the actual Ventral side, R: corresponds to the actual Right side, D: corresponds to the actual Dorsal side, L: corresponds to the actual Left side.
As illustrated in Table 1, the V/Q results in the prone position represent a greater proportion than those observed in the supine position (65.79 ± 1.57 vs. 68.56 ± 3.61, 71.13 ± 1.61 vs. 73.56 ± 1.91). Furthermore, the V/Q result during end-expiratory breath-hold accounts for a smaller proportion than during end-inspiratory breath-hold (71.13 ± 1.61 vs. 65.79 ± 1.57, and 73.56 ± 1.91 vs 68.56 ± 3.61). Additionally, the percentage of DeadSpace scores was higher (21.29 ± 1.65 vs 25.31 ± 1.61, 22.54 ± 1.08 vs 26.79 ± 2.35). Subsequently, an analysis of variance was conducted on all data obtained using the pulsatility method, as illustrated in Table 1. The results demonstrated that the pulsatility method exhibited notable discrepancies in V/Q match%, Dead Space%, and Shunt% across diverse conditions (P < 0.001).
Hypertonic saline method to monitor the effect of on V/Q during different positions and breath-holds
As illustrated in Fig. 3B,D,F,H, we observed that alterations in body position and breath-holding duration resulted in notable variations in pulmonary perfusion as depicted on EIT imaging sequences. This was achieved by monitoring pulmonary perfusion across different body positions and breath-holding periods using the hypertonic saline method. Figure 4B presents matched images of pulmonary ventilation and lung perfusion obtained through the hypertonic saline method under varying body positions and breath-holding periods, exemplifying the hefficacy of this approach.
As illustrated in Table 2, the V/Q results in the prone position represent a greater proportion than those observed in the supine position (72.10 ± 2.42 vs. 75.57 ± 3.32, 77.28 ± 2.24 vs. 80.10 ± 1.79), and the V/Q result during end-expiratory breath-hold accounts for a smaller proportion than during end-inspiratory breath-hold (77.28 ± 2.24 vs. 72.10 ± 2.42, and 80.10 ± 1.79 vs 75.57 ± 3.32). Furthermore, the percentage of DeadSpace scores was higher (11.34 ± 1.18 vs 14.09 ± 1.60, 14.11 ± 1.31 vs 17.80 ± 1.49). Finally, the ANOVA was performed on all data obtained based on the hypertonic saline method, as shown in Table 2, and we found that the hypertonic saline method showed a significant difference in V/Q match%, DeadSpace% and Shunt% in different positions ( P < 0.001).
Bland–Altman analyses of pulsatility method and hypertonic saline methods for monitoring V/Q results
Figures 3 and 4 illustrate the alterations in pulmonary ventilation and pulmonary perfusion, in addition to V/Q matching, between the pulsatility method and the hypertonic saline method in diverse positions and during breath-holding, respectively. It was observed that both methods demonstrated effective visualization of pulmonary perfusion well on EIT imaging. Furthermore, the data presented in Tables 1 and 2 showed that the pulsatility method and the hypertonic saline method exhibited consistent alterations in the V/Q data across different conditions. This was demonstrated by a higher percentage of V/Q match% results in the prone position, a higher percentage of V/Q match% results during the end-expiratory breath-hold, and a lower percentage of DeadSpace% results for both methods.
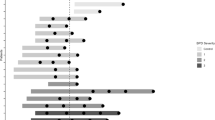
Furthermore, the V/Q results obtained by the two methods of pulsatility and hypertonic saline for monitoring different states were analysed using the Bland–Altman consistency test and Pearson correlation analysis24. Figure 5A illustrates the V/Q consistency results obtained by the pulsatility and hypertonic saline methods during end-expiratory breath-holding in the supine position, with a 95% CI of 2.36 to 10.26 and a bias of 6.309. Figure 5B depicts the V/Q concordance results obtained by the two methods during end-inspiratory breath-hold in the supine position, the 95% CI was 0.07 to 12.23, with a bias of 6.150. Figure 5C represents the V/Q concordance results obtained by the two methods during end-expiratory breath-hold in the prone position, with a 95% CI of -0.40 to 14.43, with a bias of 7.014. Figure 5D illustrates the V/Q concordance between the two methods during the prone end-inspiratory breath-hold. It can be observed that only one data point does not fall entirely within the 95% confidence interval, but the majority of the data points are within this interval, the 95% CI was 1.92 to 11.17, with a bias of 6.541. Finally, the Pearson correlation analysis and a residual analysis were conducted on the entirety of the data, the results of which are presented in Fig. 5E,F. The correlation coefficient for the two methods was found to be r = 0.7248, 95% CI = 0.50 to 0.86, p < 0.0001.

Bland–Altman plot of V/Q results. (A) Supine position during end-expiratory breath-hold; (B) Supine position during end-inspiratory breath-hold; (C) Prone position during end-expiratory breath-hold; (D) Prone position during end-inspiratory breath-hold; (E) Pearson correlation analysis; (F) Residual analysis.
Discussion
In clinical practice, alterations in body position and respiration are frequently efficacious methods of intervention for influencing or enhancing V/Q and reducing the prevalence of mechanical lung injury25. In this study, we proposed and established a pulsatility EIT-based imaging technique to assess the effect of V/Q, based on the high-speed and high-precision EIT imaging system recently established by our team. We investigated its use for the assessment of V/Q in different postures and breathing modes through experiments in animal models. This not only facilitates the early identification of patients who may benefit from postural and respiratory changes, but is also of paramount importance for guiding clinical treatment26.
Selection and establishment of animal models
In this study, healthy pigs were selected as experimental subjects, and the changes in lung EIT images and V/Q matching were observed based on the pulsatility method. This was done in order to control and verified the results using the hypertonic saline method. In selecting the body position, we controlled for both supine and prone positions. This was done for two reasons. First, prone ventilation is often used in clinical practice to improve V/Q matching in patients27. Second, the lungs are affected by gravity dependence27. Therefore, changes in supine and prone positions will also lead to changes in V/Q matching27. This study aimed to explore the feasibility of the pulsatility method for monitoring V/Q in different body positions. In the selection of breath-holding mode, end-expiratory/end-inspiratory breath-holding was used as a control, primarily because the contraction and diastole of respiratory muscles result in alterations in pulmonary blood flow, thus changes in breath-holding mode will also lead to changes in V/Q matching28. The objective was to explore the feasibility of using pulsatility method monitoring to assess V/Q during different breath-holding periods. This was done to account for the potential impact of respiratory muscle contraction and diastole on pulmonary blood flow28.
Furthermore, a breath-holding model of approximately 45 s was established during the breath-holding process. This was done to ensure that the data acquisition of the pulsatility method and the hypertonic saline method were in the same breath-holding period, thus avoiding errors. At the same time, pulsatility data prior to the injection of hypertonic saline was chosen, which helped to minimise errors due to the potential change in cardiac output resulting from the injection of hypertonic saline. To minimise this error, a period of 30 min was allowed for recovery in different positions and different breath-holds. This allowed the pigs to return to a normal physiological state.
In particular, a small quantity of propofol was administered during the end-expiratory pause, with the ventilator employed to regulate this phase. This is due to the fact that the end-expiratory carbon dioxide waveform (as displayed on the ventilator) does not fully dissipate when the end-expiratory pause is solely regulated by the ventilator. The administration of a small dose of propofol effectively suppresses respiration until the end-expiratory carbon dioxide waveform has fully dissipated, thereby ensuring that the acquired lung perfusion data are not confounded by respiration. This process is relatively unaffected by respiratory mechanics due to the rapid metabolism of propofol29. It is also necessary to confirm the respiratory and hemodynamic effects of anesthesia, which may be present simultaneously.
Feasibility and applicability of dynamic EIT techniques for monitoring V/Q
In 1999, Gazzolo and colleagues proposed the blood flow pulsation EIT technique, which is based on the acquisition of pulmonary blood flow signals derived from cardiac pulsation30. However, they found that these signals lacked sufficient information content for meaningful extraction30. The underlying reason for this result was the accuracy of the EIT system. To ascertain the accuracy of the EIT system, a comparison was made between existing commercially available EIT devices, including the Goe-MF II EIT system (CareFusion, Höchberg, Germany), the PulmoVista500 (Dräger Medical, Höchberg, Germany), and the Swisstom Pioneer EIT system (Manufacturer, Swisstom)31,32. It was found that the EC-100 pro system demonstrates distinctive advantages in addressing the challenges of high precision and wide bandwidth (5kHz to 1.17MHz), which adopts the high-precision calibration technology to address inter-channel discrepancies inherent to parallelised systems, achieving a precision of 0.01‰, the average signal-to-noise ratio exceeds 90dB, and the reciprocal error is 0.125%, establishing a robust hardware platform for the present study7,15,33.
Furthermore, the existing literature has indicated that EIT is a reliable method for monitoring alterations in perfusion resulting from changes in disease severity and PEEP34. However, it has been demonstrated to be less precise in assessing changes in body position34. This is due to the fact that in a healthy model, hypoventilation may occur as a result of a reduction in pulmonary blood flow, which is caused by conditions such as pulmonary embolism (complications), which also affects the V/Q results35. The impact of hypoventilation on V/Q can be enhanced by modifying various PEEP levels35. It is also pertinent to highlight that this study should establish a disease-control animal model to more accurately validate some of the observed differences with lung disease, which was considered in the subsequent study.
In this study, we explored the changes of V/Q in healthy pigs during different positions and different breath-holding periods by the pulsatility method. The findings revealed that the pulsatility method can initially monitored the effects of varying positions and breath-holding states on V/Q. The data yielded significant results when assessing the impact of different conditions on V/Q using the pulsatility method (P < 0.001) (Table 1). Subsequently, the hypertonic saline method was employed as a control, yielding results that were consistent with those obtained using the pulsatility method (Table 2). Furthermore, certain assumptions have been made regarding the outcomes of the data. This may be attributed to two reasons: Firstly, the V/Q obtained by the pulsatility method is to some extent more dependent on vascular compliance than on blood flow. However, the pulsatility method may contain useful information about local blood flow and local pulmonary vasculature dynamics, which requires further investigation10. Secondly, because the V/Q obtained by the hypertonic saline method in the end-expiratory breath-holding period is more dependent on blood flow than on vascular compliance, further study is needed. Furthermore, the small quantity of propofol administered during end-expiratory breath-holding precludes the possibility of determining whether this results in a reduction in cardiac output (CO)36. It is important to note that the EIT method of monitoring V/Q, as employed in this study, can only provide information about the relative spatial distribution of ventilation and perfusion37. Consequently, calibration of the EIT results using cardiac output (CO) and ventilation per minute (MV) would yield a closer approximation to the true value of V/Q. However, this requires further experimentation37.
Finally, the V/Q match%, Dead Space% and Shunt% obtained by the two methods were evaluated using the Bland–Altman agreement test and the Pearson correlation analysis. The results demonstrated that the two methods exhibited consistent outcomes, with correlation coefficients of r = 0.7248, p < 0.0001; r = 0.6719, p < 0.0001; r = 0.7521, p < 0.0001 (see Attachment 2). It is also pertinent to consider that the different V/Q mechanisms obtained by the pulsatility method and the hypertonic saline method of monitoring. The latter is more reliant on the short-term enhancement of imaging with the contrast agent. The aforementioned results validate the pulsatility EIT technique as a means of assessing V/Q results in different positions and in the breath-hold state. Furthermore, there are currently no devices or techniques available in the clinic that can continuously monitor V/Q. Indeed, the pulsatility method demonstrates its potential for assessing V/Q compared to the invasiveness of the hypertonic saline method. This is because the pulsatility method achieves true non-invasiveness, which means that the pulsatility method may have a higher degree of generalisability.
Limitations
It should be noted that this study is not without limitations. (1) The model established in healthy pigs in this study, although the feasibility of the pulsatility method for monitoring V/Q was initially obtained, the practical application for clinical patients has yet to be explored; (2) The purpose of this study, which was controlled by hypertonic saline, was to initially explore the feasibility of the pulsatility method (non-invasive) as an alternative to the hypertonic saline method (invasive). The subsequent phase will entail the utilisation of computed tomography (CT) and other imaging modalities to substantiate and enhance the precision of the pulsatility method. This will facilitate the corroboration of the efficacy and reliability of the pulsatility technique through the analysis of a more substantial data set; (3) The sample size of this study is relatively limited, necessitating the acquisition of a considerably larger data set to ascertain the viability of the pulsatility approach as a clinical tool for real-time patient monitoring; (4) This study employed PPG to obtain heart signals, the subsequent phase will employ a more precise ECG to ascertain cardiac data, thereby enhancing the precision of lung ventilation.
Conclusions
In the present study, given the current absence of non-invasive, real-time technical means to assess V/Q in clinical settings, a high-performance EIT imaging system was employed to capture information on impedance changes resulting from pulmonary blood flow pulsatility and to extract V/Q in conjunction with pulmonary ventilation data. The results of the animal experiments demonstrated that the established EIT method was capable of monitoring the effects of different body positions and different breath-holding periods on V/Q. This entirely non-invasive image monitoring method offers a novel approach to bedside patient monitoring, enabling the real-time observation and assessment of V/Q at the bedside.
Data availability
The datasets used and analysed during the current study available from the corresponding author on reasonable request.
Abbreviations
- ARDS:
-
Acute respiratory distress syndrome
- COPD:
-
Chronic obstructive pulmonary disease
- EIT:
-
Electrical impedance tomography
- MRI:
-
Magnetic resonance imaging
- SPECT:
-
Single photon emission computed tomography
- PET:
-
Positron emission tomography
- GBV:
-
Global boundary voltage
- PPG:
-
Photoplethysmographic
References
Uwagboe, I., Adcock, I. M., Lo Bello, F., Caramori, G. & Mumby, S. New drugs under development for COPD. Minerva Med. 113, 471–496 (2022).
Meijer, F. J. & Goraj, B. Brain MRI in Parkinson’s disease. Front. Biosci. (Elite Ed) 6, 360–369. https://doi.org/10.2741/e711 (2014).
Currie, G. M. & Bailey, D. L. V/Q SPECT and SPECT/CT in pulmonary embolism. J. Nucl. Med. Technol. 51, 9–15. https://doi.org/10.2967/jnmt.122.264880 (2023).
Leblanc, M. & Paul, N. V/Q SPECT and computed tomographic pulmonary angiography. Semin. Nucl. Med. 40, 426–441. https://doi.org/10.1053/j.semnuclmed.2010.08.001 (2010).
Jimenez, J. V. et al. Electric impedance tomography-guided PEEP titration reduces mechanical power in ARDS: A randomized crossover pilot trial. Crit. Care 27, 21. https://doi.org/10.1186/s13054-023-04315-x (2023).
Sella, N. et al. Electrical impedance tomography: A compass for the safe route to optimal PEEP. Respir. Med. 187, 106555. https://doi.org/10.1016/j.rmed.2021.106555 (2021).
Yan, X. H. et al. A preliminary study on the application of electrical impedance tomography based on cerebral perfusion monitoring to intracranial pressure changes. Front. Neurosci. https://doi.org/10.3389/fnins.2024.1390977 (2024).
Rezanejad Gatabi, Z. et al. The accuracy of electrical impedance tomography for breast cancer detection: A systematic review and meta-analysis. Breast J. 2022, 8565490. https://doi.org/10.1155/2022/8565490 (2022).
Tomasino, S. et al. Electrical impedance tomography and prone position during ventilation in COVID-19 pneumonia: Case reports and a brief literature review. Semin. Cardiothorac. Vasc. Anesth. 24, 287–292. https://doi.org/10.1177/1089253220958912 (2020).
Tan, A., Newey, C. & Falter, F. Pulsatile perfusion during cardiopulmonary bypass: A literature review. J. Extra Corpor. Technol. 54, 50–60. https://doi.org/10.1182/ject-50-60 (2022).
Zhang, H. et al. Effects of different VV ECMO blood flow rates on lung perfusion assessment by hypertonic saline bolus-based electrical impedance tomography. Crit. Care (London, England) 28, 274 (2024).
Nguyen, D. T. et al. Electrical impedance tomography for assessing ventilation/perfusion mismatch for pulmonary embolism detection without interruptions in respiration. Annual International Conference of the IEEE Engineering in Medicine and Biology Society. IEEE Engineering in Medicine and Biology Society. Annual International Conference 2014, 6068–6071 (2014). https://doi.org/10.1109/embc.2014.6945013
He, H. W. et al. Technology specification of bedside hypertonic saline-contrast electrical impedance tomography of lung perfusion and clinical application. Zhonghua yi xue za zhi 101, 1097–1101. https://doi.org/10.3760/cma.j.cn112137-20200926-02723 (2021).
Frerichs, I. et al. Chest electrical impedance tomography examination, data analysis, terminology, clinical use and recommendations: consensus statement of the TRanslational EIT developmeNt stuDy group. Thorax 72, 83–93. https://doi.org/10.1136/thoraxjnl-2016-208357 (2017).
Li, W. C. et al. Fast high-precision electrical impedance tomography system for real-time perfusion imaging. IEEE Access 7, 61570–61580. https://doi.org/10.1109/access.2019.2902975 (2019).
Adler, A. et al. GREIT: A unified approach to 2D linear EIT reconstruction of lung images. Physiol. Meas. 30, S35-55. https://doi.org/10.1088/0967-3334/30/6/s03 (2009).
Grychtol, B., Müller, B. & Adler, A. 3D EIT image reconstruction with GREIT. Physiol. Meas. 37, 785–800. https://doi.org/10.1088/0967-3334/37/6/785 (2016).
Gao, Y. et al. Feasibility of 3D-EIT in identifying lung perfusion defect and V/Q mismatch in a patient with VA-ECMO. Crit. Care 28, 90. https://doi.org/10.1186/s13054-024-04865-8 (2024).
Tuffet, S. et al. Impact of cardiac output and alveolar ventilation in estimating ventilation/perfusion mismatch in ARDS using electrical impedance tomography. Crit. Care (London, England) 27, 176 (2023).
Larrabee, S. et al. Three-dimensional electrical impedance tomography to study regional ventilation/perfusion ratios in anesthetized pigs. Am. J. Physiol. Lung Cell Mol. Physiol. 325, L638-l646. https://doi.org/10.1152/ajplung.00180.2023 (2023).
Zhu, Z., Li, G., Luo, M., Zhang, P. & Gao, Z. Electrical impedance tomography of industrial two-phase flow based on radial basis function neural network optimized by the artificial bee colony algorithm. Sensors (Basel, Switzerland). 23(17), 7645. https://doi.org/10.3390/s23177645 (2023).
Mata, D. A. & Milner, D. A. Jr. Statistical methods in experimental pathology: A review and primer. Am J Pathol 191, 784–794. https://doi.org/10.1016/j.ajpath.2021.02.009 (2021).
Gerke, O. Reporting standards for a Bland-Altman agreement analysis: A review of methodological reviews. Diagnostics (Basel) https://doi.org/10.3390/diagnostics10050334 (2020).
Tsikas, D. Mass spectrometry-based evaluation of the Bland-Altman approach: Review, discussion, and proposal. Molecules https://doi.org/10.3390/molecules28134905 (2023).
Bernard, G. R. et al. The American-European Consensus Conference on ARDS Definitions, mechanisms, relevant outcomes, and clinical trial coordination. Am. J. Respir. Crit. Care Med. 149, 818–824 (1994). https://doi.org/10.1164/ajrccm.149.3.7509706
Brown, B. H. Electrical impedance tomography (EIT): A review. J. Med. Eng. Technol. 27, 97–108. https://doi.org/10.1080/0309190021000059687 (2003).
Alves Bersot, C. D., Linhares, R. M., Guimarães Pereira, J. E. & Galhardo, C. Jr. Is the prone position indicated in critically ill patients with SARS-CoV-2 during the peri-operative period?. Trends Anaesth. Crit. Care 34, 38–41. https://doi.org/10.1016/j.tacc.2020.06.006 (2020).
Laveneziana, P. et al. ERS statement on respiratory muscle testing at rest and during exercise. Eur. Respir. J. https://doi.org/10.1183/13993003.01214-2018 (2019).
Kim, S. H. & Fechner, J. Remimazolam—current knowledge on a new intravenous benzodiazepine anesthetic agent. Korean J. Anesthesiol. 75, 307–315. https://doi.org/10.4097/kja.22297 (2022).
Gazzolo, D. et al. Elevated S100 blood level as an early indicator of intraventricular hemorrhage in preterm infants. Correlation with cerebral Doppler velocimetry. J. Neurol. Sci. 170, 32–35. https://doi.org/10.1016/s0022-510x(99)00194-x (1999).
Dai, F. et al. Comparison of the different animal modeling and therapy methods of premature ovarian failure in animal model. Stem Cell Res. Ther. 14, 135. https://doi.org/10.1186/s13287-023-03333-4 (2023).
Jang, G. Y. et al. Integrated EIT system for functional lung ventilation imaging. Biomed. Eng. Online 18, 83. https://doi.org/10.1186/s12938-019-0701-y (2019).
Shi, X. T. et al. High-precision electrical impedance tomography data acquisition system for brain imaging. IEEE Sensors J. 18, 5974–5984. https://doi.org/10.1109/jsen.2018.2836336 (2018).
Martin, K. T. et al. Electrical impedance tomography identifies evolution of regional perfusion in a porcine model of acute respiratory distress syndrome. Anesthesiology 139, 815–826. https://doi.org/10.1097/aln.0000000000004731 (2023).
Spadaro, S. et al. Variation of poorly ventilated lung units (silent spaces) measured by electrical impedance tomography to dynamically assess recruitment. Crit. Care 22, 26. https://doi.org/10.1186/s13054-017-1931-7 (2018).
Hamahata, N. & Pinsky, M. R. Heart-lung interactions. Semin. Respir. Crit. Care Med. 44, 650–660. https://doi.org/10.1055/s-0043-1770062 (2023).
Leali, M. et al. Absolute values of regional ventilation-perfusion mismatch in patients with ARDS monitored by electrical impedance tomography and the role of dead space and shunt compensation. Crit. Care 28, 241. https://doi.org/10.1186/s13054-024-05033-8 (2024).
Acknowledgements
The authors thank all the subjects for their participation in this study.
Funding
This work was supported by the Key Research and Development Projects of the Science and Technology Committee (2022YFC2404803); the Key Basic Research Projects of the Basic Strengthening Plan of the Science and Technology Committee (2019-JCJQ-ZD-115–00-02); the National Natural Science Foundation of China under Grant (No.52207008).
Author information
Authors and Affiliations
Contributions
JL, YG, MZ, YW, WW, RS, BL, ZJ and XS contributed substantially to this research and manuscript from conception to final preparation of the article, including the experiment design, data analysis, and the writing of the manuscript. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Competing interest
The authors declare no competing interests.
Ethical approval and consent to participate
The study protocol was approved by the Ethics Review Board of the Air Force Medical University and found to comply with the ARRIVE guidelines.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Li, J., Guo, Y., Zhu, M. et al. Feasibility of the dynamic EIT technique for non-invasive monitoring of V/Q: a preliminary study. Sci Rep 15, 33452 (2025). https://doi.org/10.1038/s41598-025-91660-2
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-91660-2
