
Abstract
Infants born in Japan are reported to have a low incidence of necrotizing enterocolitis (NEC) among countries, and these differences remained significant after adjusting for common clinical factors. To investigate the impact of ethnic background, we compared the incidence of NEC between infants born in Japan and those born to mothers of Japanese ethnicity in California. Preterm infants born between 2008 and 2019 at 22–29 weeks of gestational age were analyzed retrospectively. Four groups were analyzed: infants born in Japan (JP), infants born in California to mothers born in Japan (JP-J), infants born in California to mothers with Japanese ethnicity but born in the United States or another country (JP-CA), and a comparison group of infants born in California to non-Hispanic White mothers (NHW-CA). Each cohort consisted of 52,049, 115, 226, and 12,275 infants, respectively. Unadjusted NEC incidences were significantly lower in JP compared to the other three cohorts (1.7% JP, 4.5% JP-J, 4.6% JP-CA, and 3.3% NHW-CA, respectively; p < 0.01). After adjusting for confounding factors, odds ratios for NEC in JP vs. JP-J, JP-CA, and NHW-CA were 3.04 (1.18–7.80), 2.89 (1.45–5.75), and 1.96 (1.56–2.47), respectively. This study suggests that differences in NEC incidence in Japan are not explained by ethnicity.
Clinical trial regstration number: Registration numbers is UMIN000006961 (https://center6.umin.ac.jp/cgi-open-bin/ctr_e/ctr_view.cgi?recptno=R000008217) for the Neonatal Research Network of Japan. However, the the California Perinatal Quality Care Collaborative (CPQCC) aims only to assess neonatal outcomes for the purpose of quality assessment and improvement. So, no clinical trial number is available. Please refer to the web site https://www.cpqcc.org/.
Similar content being viewed by others

Introduction
The mortality rate among extremely preterm infants has decreased dramatically, especially in developed countries1,2, including Japan and California in the United States of America (USA)3,4. However, there is still difficulty in preventing their morbidities, and their current long-term outcomes are not satisfactory5,6,7. Necrotizing enterocolitis (NEC) is still one of the most important life-threatening morbidities among extremely preterm infants and remains difficult to prevent or treat8,9. Poor long-term outcomes among NEC survivors have also been reported10. Many investigations have been carried out to identify risk factors and preventive measures for NEC. Although several risk factors have been reported, including not being fed by human breastmilk, rapidly increasing enteral feeding volume, excessive use of antibiotics, and blood transfusion, the direct causality of these factors has yet to be established11. Furthermore, there is a huge variation in the incidence of NEC among countries12. Japan has reported a relatively low incidence of NEC as compared with the US and European countries5,6,13,14. Its recent incidences in Japan and California were reported around 1.6% and 3.9% in very-low-birth-weight (VLBW) infants, respectively15,16. Several reports suggested a genetic difference could explain frequency variations17,18,19. Variation in incidence within a country has also been reported based on racial/ethnic differences20. Even in a single USA state, California, there exists racial/ethnic disparities in the incidences of NEC21. Even though there are possibilities that this difference could be explained by baseline characteristics, including social health status and low exposure to breast milk, genetic contribution still needs to be explored. However, these comparisons are often difficult because of differences in cohort selection, definitions, and risk considerations. Therefore, in this study, two datasets of VLBW infants were selected to compare NEC incidences between Japan and California employing a strategy similar to that used in our previous study of intraventricular hemorrhage (IVH)22, with careful matching of cohort criteria, risk adjustment, and definitions.
Comparing NEC incidences among Japanese mothers who gave birth in Japan and Japanese women born in Japan who gave birth in California could provide insight into the potential impact of ethnic factors on the onset of NEC. If preterm infants born to Japanese mothers in California showed a rate of NEC that was significantly higher than the rate seen in preterm infants born in Japan, changes in maternal lifestyle and/or differences in perinatal practices are most likely the source. Furthermore, this finding would open the possibility of identifying important drivers for developing NEC by comparing maternal health and perinatal care practices in future studies.
Results
Patient characteristics
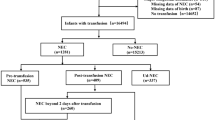
Of the registered total of 58,306 infants in the Neonatal Research Network of Japan (NRNJ) databases, after excluding 2,131 infants born after 29 gestational age or with a birthweight > 1500 g and 4,216 with major congenital anomalies, a final study sample of 52,049 infants was used for the analysis. In the California Perinatal Quality Care Collaborative (CPQCC) database, of the 181,456 total registered infants, 118,337 infants were excluded for not meeting gestational age or birthweight criteria, 7,163 infants were excluded due to major congenital anomalies, which was used for the epidemiological study; including chromosomal/genetic disorders and central nervous, cardiovascular, urogenital, gastrointestinal, respiratory, and skeletal organs23, 848 without ethnicity information, and 42,492 infants who were not Japanese or non-Hispanic White for a final cohort of 12,616 infants. Among them, 341 infants were born to Japanese mothers. One hundred fifteen of these infants were born to mothers who were born in Japan and 226 to mothers born in the USA or other countries (174 in California, 38 in other states, and 14 in other countries). The comparison group included 12,275 infants born in California to non-Hispanic White mothers (Fig. 1).

Patient flow. NRNJ: the Neonatal Research Network of Japan CPQCC: the California Perinatal Quality Care Collaborative GA: gestational age.
Maternal and infant risk profiles by birthplace and maternal ethnicity are shown in Table 1. There were no significant differences in gestational ages among the four cohorts. However, infants born in Japan had lower birthweights, were more likely to be small-for-gestational age (SGA), singleton, and had a low 5-min Apgar. Mothers giving birth in Japan had a higher percentage of chorioamnionitis but were less likely to be teenagers, have diabetes or hypertension, receive antenatal steroids, or have an outborn birth when compared to non-Hispanic White mothers in California. When compared to mothers in Japan, mothers born in Japan who delivered in California were older and had a higher percentage of diabetes, multiple births, antenatal steroids, and outborn infants. With the exception of mothers over 39 years of age, the profiles and gestational age of California born Japanese mothers were similar to those of Japanese born mothers who delivered in California. These factors were used for risk adjustment in our mixed logistic regression models.
Outcome comparisons
Unadjusted clinical outcomes are shown in Table 2. The mortality of infants born in Japan was lowest compared to infants born in California to mothers born in Japan, mothers of Japanese ethnicity born in the USA, and non-Hispanic White mothers (unadjusted logistic regression, p < 0.01). To explore the possibility that these low incidences could be explained by a high rate of delivery room deaths, delivery room deaths by ethnicity were compared. Delivery room deaths were also lowest in Japan when compared with rates for infants of Californian mothers born in Japan, California Japanese mothers born in the USA, and non-Hispanic White mothers (unadjusted logistic regression, p < 0.01). Although there were no differences in the incidences of spontaneous intestinal perforation (SIP), the incidences of NEC and either NEC or SIP were lowest in infants born in Japan compared with infants born in California to Japanese mothers born in Japan, Japanese mothers born in the USA, and Californian non-Hispanic White mothers (unadjusted logistic regression, p < 0.01). Although the observed overall mortality, delivery room deaths, NEC, and NEC or spontaneous SIP were lowest in infants born in Japan, there were no differences among Californian infants born to Japanese mothers born in Japan, Japanese mothers born in the USA, and non-Hispanic White mothers (Fig. 2).

Necrotising enterocolitis, spontaneous gastrointestinal perforation, and death/necrotizing enterocolitis rates among different cohorts. NEC and its composite outcome in preterm infants born in Japan were significantly lower than all other cohorts in California (unadjusted logistic regression, p < 0.01). Although spontaneous intestinal perforation was lowest in non-Hispanic White infants, there was no significant difference among cohorts. (Refer to Table 2). Vertical bars show 95% confidential limits. NEC: necrotizong enterocolitis, SIP: spontanous intestinal perforation JP: Japan, CA: California, NHW: non-Hispanic White.
The composite outcome, either death or NEC, was also lowest in infants born in Japan (6.1%, 3,149/52,049) compared with infants born to mothers born in Japan (16.5%, 19/115), infants born to mothers with Japanese ethnicity born in the USA (14.2%, 32/226), and infants born to non-Hispanic White mothers (13.8%, 1,691/12,275) (unadjusted logistic regression, p < 0.01) (Fig. 2). However, regardless of maternal place of birth, there were no differences in the odds ratios (ORs) between Japanese infants born in California and non-Hispanic White infants born in California (unadjusted logistic regression).
Risk-adjusted primary outcome
Table 3 shows the risk-adjusted ORs in NEC incidence among four cohorts from a mixed logistic regression using the following risk factors indicated by univariate analyses: maternal age, chorioamnionitis, hypertension, diabetes, gestational age, multiple births, cesarean delivery, antenatal steroids, outborn, 5-min Apgar score, birth year, SGA, gender, and random effect of hospital clustering. The observed and adjusted ORs were very similar (Tables 2 and 3). For example, compared to births in Japan, the observed OR to non-Hispanic Whites in California was 2.0 (1.7–2.2) vs. a risk-adjusted OR of 2.0 (1.6 -2.5). When compared to the mothers born in Japan who delivered in California, the observed OR was similar to the adjusted OR of 3.0 (1.2–7.8). The risk-adjusted ORs for the other clinical outcomes listed in Table 2 were also similar to their observed ORs (data on request to authors). Even with risk adjustment, compared to infants born in Japan, the OR for developing NEC remained significantly higher for infants born in California to mothers born in Japan (3.0, 1.2–7.8), born in California to Japanese mothers born in the USA (2.9, 1.5–5.8), and to non-Hispanic White mothers (2.0, 1.6–2.5).
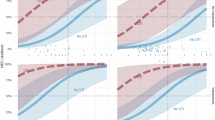
Trends in NEC rates in Japan and California
While the NEC incidence in infants born in Japan was stable, averaging 1.7% beginning in 2008, those in non-Hispanic White infants decreased from 4.9% in 2008 till approximately 2015 and then stabilized at an average of 2.7% (Cochran-Armitage trend test, p < 0.01 from 2008 to 2019). Actual decreases in the incidences of NEC in non-Hispanic White infants from 2008 to 2019 was about 55% (Fig. 3). Due to the relatively small sample size, there was marked variability in the year-to-year NEC incidence of Californian Japanese infants born to mothers born either in Japan or outside of Japan. Even when combined (n = 341 with NEC incidence of 4.6%), they did not show a significant decrease over time.

Trends in necrotizing enterocolitis in Japan and California. Comparison of annual trends in incidences in three groups revealed no significant differences for Japan (Cochran-Armitage trend test), while significant decreases for the CPQCC (p < 0.01) and non-Hispanic White infants born in California (p < 0.01). The NEC incidences in each year group are described at the bottom of the figure. CPQCC: the California Perinatal Quality Care Collaborative, NHW-CA: non-Hispanic White infants in Calfornia, JP: infants born in Japan.
Discussion
The purpose of this study was to explore the possibility that the low incidence of NEC in Japan could be attributed to a genetic advantage. If that were the case, one would expect that the low rate of NEC observed in infants born to Japanese mothers in Japan would persist if the mother gave birth in California. Using the same cohort selection criteria and definitions, we found that the incidence of NEC or NEC and death in infants born in Japan was significantly lower than in infants born in California to women born in Japan. This difference persisted even after adjusting for several confounding background risks. Furthermore, there was no statistical difference in NEC incidences among the infants born in California, whether born to Japanese mothers born in Japan, Japanese mothers born in the USA, or to non-Hispanic White mothers, and their NEC rates were all significantly higher than those of infants born in Japan. This is the first and unique study to show the difference in NEC incidences among preterm infants born in different birthplaces with the same maternal ethnic background. Our findings suggest that the low rate of NEC in Japan could not be explained simply by ethnicity. Ethnicity may depend on social constructs in part rather than genetic basis. Furthermore, the use of breast milk is more significantly influenced by the NICU management policies of the region of birth rather than by ethnic differences. While considering such backgrounds, our current study clearly indicates that NEC cannot be strongly involved in genetic basis in the onset.
Unfortunately, we were unable to assess the potential impact of socioeconomic and lifestyle factors (such as dietary and exercise habits and smoking) on developing NEC, as this information was not available11,24. Recognizing the limitations of our available risk factors (maternal age, hypertension, chorioamnionitis, diabetes, gestational age, sex, plurality, birthweight, SGA, antenatal steroids, cesarean delivery, neonatal transport, 5-min Apgar score, and teenage pregnancy), we interpreted the lack of significant difference between unadjusted and adjusted estimates to suggest that the low NEC incidences seen in Japan were not due to a more advantageous available risk profile.
We were also unable to assess the possibility of paternal impact. In our cohort, among the first-generation Japanese mothers, 40% (47/115) had fathers of Japanese ethnicity, while for the later generation, only 9.3% (21/226) had fathers of Japanese ethnicity. Although it would be informative to see if the incidence of NEC differed by paternal ethnicity, our data set was too small to perform this analysis.
Although all cases reported as having NEC on each database were not validated about the accuracy of diagnosis, this study makes a strong case that ethnic differences alone could not account for the variation in NEC incidences among countries. We believe that differences in perinatal practices should play an important role in the incidence of NEC. While identifying what practice differences might account for Japan’s low incidence of NEC is beyond the scope of this first investigation, the trend patterns in practices in Japan and California have now been collected and may provide some clues in the next manuscript under preparation. For example, the low incidence of NEC in Japan has been stable from 2008 to 2019, suggesting that whatever perinatal factors and approaches to care contributed to the low incidence were present as early as 2008. In contrast, the NEC incidence in California decreased from 2008 to approximately 2015 and was then stable. An analysis of changes in the perinatal care associated with this decrease could provide important clues to how daily NICU practice might be essential in preventing NEC or enhancing NEC onset. For example, differences in nutritional management, particularly feeding practices and breast milk feeding, among NICUs or changes over time are of significant interest in relation to the onset of NEC, as nutritional management has been discussed as the most critical factor in its development25,26,27,28. Additionally, administering Bifidobacterium to preterm infants during their stay in NICUs is also an area of interest29. An investigation to examine the potential relationships between NEC onset and differences in NICU practices is underway using these same cohorts.
Another factors need to be clarified is the effect of active treatment of infants born below 24 gestation because lower gestation is the most substantial known risk for NEC. If there was a policy change, active resuscitation towards infants born under 24 gestation might affect NEC incidences between countries. However, rates of infants born before 24 gestation analyzed for this study in Japan and California were 6.5% for infants born in Japan, 7.0% for infants born in California to Japanese mothers born in Japa, 6.6% for those born in California to Japanese mothers born in the USA, and 6.7% for infants born to Californian non-Hispanic White mothers, respectively. Therefore, there was no selection bias in the gestational age distribution among infants studied.
The strengths of this study are that it compares two well-organized network databases in Japan and California that used the same risk factor and outcomes definitions, which increased the analytical power of the study. The limitations of this study are as follows. Firstly, although the diagnostic criteria for NEC were standardized across all registered hospitals, the possibility that a similar case, especially if it is a mild expression of NEC, might be diagnosed differently across institutions can not be excluded. Secondly, even including all births from 2008 until 2019, the sample size of Japanese mothers who gave birth to preterm infants in California was small. We were able to report the statistical significance level for all our comparisons. However, when utilizing vital records to ascertain ethnicity and country of birth in California, we could not disclose the number and percentage of infants in a table cell if it was less than 12. Although the differences in NEC incidences were significant among cohorts, a larger sample size would have allowed us to share the details of our findings more completely.
Conclusion
The NEC incidence in preterm infants born in Japan was significantly lower than those born to Japanese mothers in California. This suggests that ethnic differences alone could not account for the low rate of NEC in Japan. A detailed analysis of the differences in lifestyle and perinatal practice between Japan and California is warranted to identify potential care strategies to reduce NEC in preterm infants.
Methods
Data sources
In this retrospective cohort study, two large neonatal network databases, the NRNJ30 and the CPQCC31 data registries, were analyzed.
Approximately 230 hospitals have participated in the NRNJ since 2003, collecting information on short-term outcomes at NICU discharge from infants born with birth weight at or less than 1500 g. More than 83,000 infants have been registered in the NRNJ database, covering > 65% of infants with VLBW born in Japan. There is no variable regarding ethnicity in the NRNJ dataset, but according to the Vital Statistics in Japan, more than 97% of infants were born to mothers of Japanese ethnicity.
In California, approximately 130 hospitals are members of CPQCC, caring for more than 95% of all VLBW infants (1.1% of California births). We used the California birth certificate to obtain self-identified nativity, maternal race, and ethnicity for the California-born infants. These vital statistics data were then linked to the CPQCC demographic and clinical outcomes data using a probabilistic linkage algorithm with a success rate of greater than 98%.
Study population
All infants born at 22–29 weeks of gestational age or with a birthweight between 401–1,500 g between January 1, 2008, and December 31, 2019, admitted for neonatal care within 28 days of birth to hospitals participating in the network databases were included in the study cohort. Gestational age was determined using the following hierarchy: a best estimate based on early prenatal ultrasound, last menstrual period, or physical examination at birth. Infants with major congenital anomalies and incomplete data were excluded. After the exclusion of ineligible infants, 4 groups were defined for data analyses: 1) infants born in Japan, 2) infants born in California to mothers born in Japan, 3) infants born in California to mothers with Japanese ethnicity but who were born in the USA or another country, and 4) infants born in California to non-Hispanic White mothers. To assess the potential impact of acculturation, we compared the risk profiles and neonatal outcomes for infants born to first-generation mothers who were born in Japan to those of Japanese ancestry who were born in the USA (later generations). Infants born in California to non-Hispanic White mothers were set as a comparison group.
Outcome measures and risk factors
The primary outcome was NEC or mortality during the stay in the NICU. NEC was defined as grade II or III by Bell’s criteria diagnosed with clinical findings, including increased gastric residue, a distended abdominal wall, increased inflammatory indicators, and abdominal X-ray findings with or without intestinal perforation. All information on the diagnosis of NEC was exclusively based on the clinical or pathological findings from hospitals belonging to both networks. SIP, which was defined as the sudden onset of perforation without any preceding signs or symptoms of NEC, was also evaluated because a precise differential diagnosis between these two morbidities is not always possible. Although the diagnosis of NEC or SIP is defined in the operational manual for both cohorts, the final diagnosis exclusively depends on the physician’s reports. Mortality included delivery room deaths, however, clinical outcomes during the stay in the NICU were analyzed only for infants admitted into the NICU. The same outcome definitions are used in Japan and California30,31.
To assess the potential impact of differential risk profiles, we compared the percentage of maternal risk factors (age, hypertension, chorioamnionitis, and diabetes), infant factors (gestational age, sex, plurality, birthweight, SGA), healthcare differences (antenatal steroid use, cesarean delivery, neonatal transport, and Apgar score at 5 min), and a social risk factor (teenage pregnancies) in the study groups. These factors and birth year were used for risk adjustment in our regression analyses. Our main exposure variable is the maternal cohort defined by delivery location and ethnicity.
Statistical analyses
To assess the maternal cohort effect (the exposure variable) the association of outcomes and the selected variables were examined using descriptive analysis and chi-square tests for categorical variables and ANOVA for continuous variables. Observed outcome rates were assessed for statistical significance between the four cohorts using unadjusted logistic regression. Multivariable hierarchical logistic regression models with hospitals as a random effect were used to estimate adjusted ORs. Candidate variables to account for differences in patient case mix include the maternal, infant, and care factors listed in the previous section. The birth year was also included to adjust for temporal trends in the outcomes over time. The models were estimated based on maximum likelihood with Laplace approximation. All infants in our final cohort were included in all of our analyses, and the level of significance stated. However, because self-identified maternal Race and Country of birth were obtained from California Vital records, to protect the privacy of individuals, we are required by the State to not report the number and percentage of infants in a table cell of less than 12. The analysis was conducted in SAS 9.4 (SAS Institute, USA).
Ethical consideration
All information about the infants was collected anonymously, and the stored data were unlinked from individual identifiers. The protocol of this study was approved by the central internal review board at Tokyo Women’s Medical University (Registration number: 692), and informed consent from the parents for registering and analyzing the data was obtained, where all Japanese data were collected, and at Stanford University, where the analyses comparing Japanese and Californian cohorts were conducted in collaboration in accordance with the requirements for the Committee for the Protection of Human Subjects/the Health Care Access and Information (CPHS/HCAI).
All methods were performed in accordance with the relevant guidelines and regulations.
Data availability
The datasets generated by the current study are available in the Database repository, http://plaza.umin.ac.jp/nrndata/indexe.htm and https://www.cpqcc.org/nicu/nicu-reports.
References
Bell, E. F. et al. Mortality, in-hospital morbidity, care practices, and 2-year outcomes for extremely preterm infants in the US, 2013–2018. JAMA. 327, 248–263. https://doi.org/10.1001/jama.2021.23580 (2022).
Helenius, K. et al. Survival in very preterm infants: An international comparison of 10 national neonatal networks. Pediatrics. 140, e20171264. https://doi.org/10.1542/peds.2017-1264 (2017).
Nakanishi, H., Suenaga, H., Uchiyama, A., Kono, Y. & Kusuda, S. Trends in the neurodevelopmental outcomes among preterm infants from 2003–2012: a retrospective cohort study in Japan. J Perinatol. 38, 917–928. https://doi.org/10.1038/s41372-018-0061-7 (2018).
Lee, H. C., Liu, J., Profit, J., Hintz, S. R. & Gould, J. B. Survival without major morbidity among very low birth weight infants in California. Pediatrics. 146, e20193865. https://doi.org/10.1542/peds.2019-3865 (2020).
Stoll, B. J. et al. Trends in care practices, morbidity, and mortality of extremely preterm neonates, 1993–2012. JAMA. 314, 1039–1051. https://doi.org/10.1001/jama.2015.10244 (2015).
Kusuda, S., Fujimura, M., Uchiyama, A., Totsu, S. & Matsunami, K. Trends in morbidity and mortality among very-low-birth-weight infants from 2003 to 2008 in Japan. Pediatr Res. 72, 531–538. https://doi.org/10.1038/pr.2012.114 (2012).
Torchin, H., Morgan, A. S. & Ancel, P. Y. International comparisons of neurodevelopmental outcomes in infants born very preterm. Semin Fetal Neonatal Med. 25, 101109. https://doi.org/10.1016/j.siny.2020.101109 (2020).
Patole, S. Prevention and treatment of necrotising enterocolitis in preterm neonates. Early Hum Dev. 83, 635–642. https://doi.org/10.1016/j.earlhumdev.2007.07.007 (2007).
Neu, J. & Walker, W. A. Necrotizing enterocolitis. N. Engl. J. Med. 364, 255–264. https://doi.org/10.1056/NEJMra1005408 (2011).
Schulzke, S. M., Deshpande, G. C. & Patole, S. K. Neurodevelopmental outcomes of very low-birth-weight infants with necrotizing enterocolitis: a systematic review of observational studies. Arch Pediatr Adolesc Med. 161, 583–590. https://doi.org/10.1001/archpedi.161.6.583 (2007).
Samuels, N., van de Graaf, R. A., de Jonge, R. C. J., Reiss, I. K. M. & Vermeulen, M. J. Risk factors for necrotizing enterocolitis in neonates: a systematic review of prognostic studies. BMC Pediatr 17, 105. https://doi.org/10.1186/s12887-017-0847-3 (2017).
Alsaied, A., Islam, N. & Thalib, L. Global incidence of necrotizing enterocolitis: a systematic review and meta-analysis. BMC Pediatr. 20, 344. https://doi.org/10.1186/s12887-020-02231-5 (2020).
Edstedt Bonamy, A. K. et al. Wide variation in severe neonatal morbidity among very preterm infants in European regions. Arch Dis Child Fetal Neonatal Ed. 104, F36–F45 (2019).
Ahle, M., Drott, P. & Andersson, R. E. Epidemiology and trends of necrotizing enterocolitis in Sweden: 1987–2009. Pediatrics. 132, e443-451. https://doi.org/10.1542/peds.2012-3847 (2013).
NRNJ database: http://plaza.umin.ac.jp/nrndata/reports/nrn1_2003_2019.pdf (Accessed on February 12, 2024).
CPQCC NICU reports. https://www.cpqcc.org/nicu/nicu-reports (Accessed on February 12, 2024).
Cuna, A., George, L. & Sampath, V. Genetic predisposition to necrotizing enterocolitis in premature infants: Current knowledge, challenges, and future directions. Semin Fetal Neonatal Med. 23, 387–393. https://doi.org/10.1016/j.siny.2018.08.006 (2018).
Cai, X., Golubkova, A. & Hunter, C. J. Advances in our understanding of the molecular pathogenesis of necrotizing enterocolitis. BMC Pediatr. 22, 225. https://doi.org/10.1186/s12887-022-03277-3 (2022).
Talavera, M. M. et al. Single nucleotide polymorphisms in the dual specificity phosphatase genes and risk of necrotizing enterocolitis in premature infant. J Neonatal Perinatal Med. 13, 373–380. https://doi.org/10.3233/NPM-190302 (2020).
Jammeh, M. L. et al. Racial/ethnic differences in necrotizing enterocolitis incidence and outcomes in premature very low birth weight infants. J. Perinatol. 38, 1386–1390. https://doi.org/10.1038/s41372-018-0184-x (2018).
Goldstein, G. P. et al. Racial/ethnic disparities and human milk use in necrotizing enterocolitis. Pediatric Res. 88(Suppl 1), 3–9. https://doi.org/10.1038/s41390-020-1073-5 (2020).
Kusuda, S., Bennett, M. & Gould, J. Outcomes of infants with very low birth weight associated with birthplace difference: A retrospective cohort study of births in Japan and California. J Pediatr. 229, 182-190.e6. https://doi.org/10.1016/j.jpeds.2020.10.010 (2021).
Eurocat. Q chapter, ICD10/BPA. https://eu-rd-platform.jrc.ec.europa.eu/sites/default/files/EUROCAT-Q-Chapter-2008.pdf. (Accessed Dec 21, 2024) (2008).
Quigley, M., Embleton, N. D. & McGuire, W. Formula versus donor breast milk for feeding preterm or low birth weight infants. Cochrane Database Syst. Rev. https://doi.org/10.1002/14651858.CD002971.pub5 (2019).
Downard, C. D. et al. Maternal cigarette smoking and the development of necrotizing enterocolitis. Pediatrics. 130, 78–82. https://doi.org/10.1542/peds.2011-3808 (2012).
Oddie, S. J., Young, L. & McGuire, W. Slow advancement of enteral feed volumes to prevent necrotising enterocolitis in very low birth weight infants. Cochrane Database Syst. Rev. https://doi.org/10.1002/14651858.CD001241.pub8 (2021).
Ibrahim, N. R., Van Rostenberghe, H., Ho, J. J. & Nasir, A. Short versus long feeding interval for bolus feedings in very preterm infants. Cochrane Database Syst. Rev. https://doi.org/10.1002/14651858.CD012322.pub2 (2021).
Young, L. & OddieSJ, M. W. Delayed introduction of progressive enteral feeds to prevent necrotising enterocolitis in very low birth weight infants. Cochrane Database Syst. Rev. https://doi.org/10.1002/14651858.CD001970.pub3 (2022).
Sharif, S., Oddie, S. J., Heath, P. T. & McGuire, W. Prebiotics to prevent necrotising enterocolitis in very preterm or very low birth weight infants. Cochrane Database Syst. Rev. https://doi.org/10.1002/14651858.CD015133.pub2 (2023).
The Neonatal Research Network of Japan (NRNJ http://plaza.umin.ac.jp/nrndata/indexe.htm) (Accessed on February 12, 2024).
The California Perinatal Quality Care Collaborative (CPQCC, https://www.cpqcc.org/nicu/nicu-reports) (Accessed on February 12, 2024).
Acknowledgements
We would like to express our sincere gratitude to all the staff of the facilities who provided valuable data for this study, as well as to the infants and their families who registered valuable data during their NICU stay. The complete list of the Neonatal Research Network of Japan and the California Quality Care Collaborative is shown in Appendix 1.
Funding
This study was partly supported by the Neonatal Research Network of Japan and the California Perinatal Quality Care Collaborative.
Author information
Authors and Affiliations
Consortia
Contributions
S.K. and J.B.G. wrote the main manuscript text, and M.V.B. conducted the initial statistical analyses. All authors reviewed the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Kusuda, S., Bennett, M.V., Gould, J.B. et al. Comparative analysis of necrotizing enterocolitis in preterm infants born in Japan and born to mothers of Japanese ethnicity in California. Sci Rep 15, 9943 (2025). https://doi.org/10.1038/s41598-025-92393-y
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-92393-y
