
Abstract
B-cell depletion therapy is employed in a variety of clinical contexts from auto-immune diseases to malignancy. Prior research on patients with prior B-cell depletion treatment has suggested a mortality risk in patients hospitalized with COVID-19 however previous case–control studies have differed in their methods of patient comparison. Patients previously treated with B-cell-depletion hospitalized with COVID-19 were compared to matched controls in the Johns Hopkins Health System between March 1, 2020 and November 30, 2021. The primary outcome was 30-day all-cause mortality. Secondary outcomes included time to severe illness or death and time to clinical improvement. To eliminate bias due to imbalanced covariates, each patient who had previously received B-cell depletion therapy was matched with patients who had not received therapy based on age, sex, race, WHO severity score, admission date, COVID-19 specific treatment, and vaccination status. Propensity scores were calculated from a multivariable logistic regression model and performed on the matched sets, using B-cell depletion as the outcome, where the propensity score was the probability of receiving B-cell depletion therapy. The propensity score included matched covariates as well as smoking status, medical comorbidities, and vaccination status. Cox proportional-hazards regression models were applied on the matched sets to perform time to death, time to severe illness or death, and time to clinical improvement analyses. 50 patients were identified who had received B-cell depletion therapy and were compared to 186 matched controls. Patients treated with B-cell depletion experienced 30-day mortality of 6.0% compared to 3.8% in controls, adjusted hazard ratio (aHR) 1.45 (95% CI 0.30 to 6.95). B-cell-depleted patients experienced a longer time to clinical improvement, aHR 0.65 (95% CI 0.45–0.94). In this cohort, patients treated with B-cell depletion experienced a higher mortality rate compared to matched controls however this was not statistically significant. This group also experienced a prolonged time to clinical improvement based on WHO severity score.
Similar content being viewed by others

Introduction
A variety of factors have been found to be associated with worse outcomes for patients diagnosed with COVID-19 including age, sex, body-mass index (BMI), and smoking status1,2,3,4. Outcomes for immunocompromised patients who develop COVID-19 remains an area of active study as this population may have special vulnerabilities to the disease. Biologic therapies that target B-cell function are effective for a range of indications from rheumatologic diseases to treatment for malignancy. However, immunosuppressive therapies may impair humoral responses to SARS-CoV-2 infection, leading to suboptimal immunity and continued risk for severe infection5,6,7.
Some authors have reported increased severity of COVID-19 in patients with history of B-cell depletion treatment8,9,10,11,12,13. The primary goal of this study was to compare outcomes of patients hospitalized with COVID-19 who had received B-cell depletion therapy with a matched contemporaneous cohort by severity of illness of admission, in a large registry within one hospital system, to further assess the effect of this treatment on outcomes.
Methods
This study was developed using the JH-CROWN: COVID Precision Medicine Analytics Platform Registry, which includes inpatient and outpatient records for patients who tested positive for SARS-CoV-2 in the Johns Hopkins Health System (JHHS). The JHHS comprises six hospitals and over forty outpatient facilities located in Maryland, Florida and Washington, DC. The research was approved by the Johns Hopkins Institutional Review Board. Patients hospitalized within the JHHS for COVID-19 infection during the period of March 1, 2020 until November 30, 2021 were eligible for inclusion. A query identified patients who were previously treated with B-cell depletion therapy on or after September 1, 2019 and who were subsequently hospitalized in the Johns Hopkins Health System with a laboratory-confirmed SARS-CoV-2 infection. No common platform for SARS-CoV-2 testing was employed during the period of study. B-cell depletion therapy was defined as rituximab, ocrelizumab, obinutuzumab, ibritumomab tiuxetan, and ofatumumab. A full list of medication search terms is included in the Appendix. Individual charts were reviewed to ensure that only patients who previously received B-cell depletion therapy on or after September 1, 2019 and prior to hospitalization with SARS-CoV-2 infection were included in the analysis. September 1, 2019 was chosen as it is six months prior to the start of COVID-19 hospitalizations among JHHS patients and would reflect the biologic effects of prior B-cell therapy. JHHS instituted mandatory screening of hospitalized patients for SARS-CoV-2 during the study period; patients with an incidentally positive SARS-CoV-2 test were eligible for analysis. The need to obtain informed consent was waived by the Johns Hopkins University School of Medicine Institutional Review Board (IRB00247569).
Outcomes
The primary outcome was time to death from hospital admission. The secondary outcome was time to a composite outcome of severe illness or death from hospital admission. An additional secondary outcome was time to clinical improvement from the date of hospital admission, defined as a 2-point decrease in World Health Organization (WHO) severity score or discharge alive from the hospital within 30 days. The WHO Severity score is a 10-point scale ranging from 0 (uninfected) to 10 (deceased)14.
Disease severity at admission was defined by the highest WHO severity score in the first 12 h of the patient’s admission. Severe illness was defined as score ≥ 6. Failure of clinical improvement was censored at the last day of follow-up or 30 days, whichever came first. Patients who were discharged alive were censored at 30 days.
Statistical analysis
A two-step, hybrid approach was used to account for the differences between the groups with and without B-cell therapy. In the first step, patients hospitalized with COVID-19 who received prior B-cell treatment were identified. Then a comparison group from the registry of patients who had not received B-cell therapy but matched on characteristics with the treated patient was selected. Matching criteria included age at time of hospitalization (± 5 years), timing of hospitalization (± 28 days), sex at birth, race, WHO COVID-19 disease severity, COVID-19 specific treatments (remdesivir, dexamethasone), and vaccination status before admission. All the patients who were matched to the b-cell cohort were included in the comparison group.
The second step employed overlap weighting, a propensity score (PS) approach, to further address differences between the B-cell treatment population and controls15. The PS score, indicating the likelihood of receiving B-cell depletion treatment, was derived from age, race, sex, body mass index (BMI), COVID-19 severity on the WHO scale, smoking status, existing comorbidities, specific COVID-19 treatments, and vaccination status at the time of admission. Medical comorbidities included hypertension, chronic obstructive lung disease, congestive heart failure, chronic kidney disease, end stage renal disease, human immunodeficiency virus, cirrhosis and cancer. Comorbidities were determined from relevant ICD codes present in the medical record. Use of overlap weighting based on the propensity score estimated from a logistic model leads to an exact balance for all covariates between different groups16,17.
Finally, inverse probability weighted Cox regression was used to estimate the association between B-cell depletion treatment and outcomes of interests. Age, BMI, COVID-19 specific medications and vaccination information were included as covariates in Cox regression models based on clinical interest and knowledge. The proportional hazards assumption was tested for violation using individual covariates and each outcome. A prespecified subgroup analysis was conducted to examine effects in patients with B-cell depletion treatment less than 90 days prior to COVID-19 hospitalization. For the sensitivity analysis we used the original control group and reperformed overlap weighting for the subgroup. All data analyses were executed using R software version 4.0.2 (R Foundation for Statistical Computing, Vienna, Austria)18.
Results
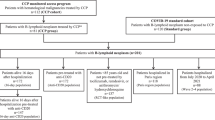
A total of 9,233 patients were admitted to the Johns Hopkins Health System between March 1, 2020 and November 30, 2021 with COVID-19. Seventy-two of the patients hospitalized with COVID-19 within JHHS had been treated with B-cell depletion therapy after September 1, 2019. Twenty-one patients were excluded from the analysis due to receiving B-cell depletion therapy after testing positive for SARS-CoV-2. One patient treated with B-cell depletion was excluded due to missing BMI records (Fig. 1). A control group of 186 distinct patients was selected from the original cohort of patients based on the method described above. Summary statistics of the cohort and the matched controls are presented in Table 1. After performing overlap weighting, absolute standardized differences were no longer present indicating balanced covariates. The indications and timing of prior B-cell depletion therapy is summarized in Table 2. The proportional hazards assumption was individually evaluated for individual covariates and outcomes. There were no violations of the assumption for mortality, severe illness or death, or clinical improvement.

Identification of study cohort of patients treated with prior B-cell depletion and hosptialization for COVID-19 between March 1, 2020 and November 30, 2021.
Patients who had received prior B-cell depletion therapy had a 30-day mortality rate of 6.0% (n = 3) compared to 3.8% (n = 7) in the control group. This difference was not statistically significant in overlap weighting-adjusted regression analysis, adjusted hazard ratio (aHR) 1.45 (95% confidence interval (CI) 0.30 to 6.95). The time to severe illness or death from time of hospitalization was 2.4 days (IQR 0.5 to 4.0 days) in the B-cell depletion group and 2.2 days (IQR 1.0 to 4.4 days) among controls. In adjusted analysis there was no difference between the B cell depletion group and the controls, aHR 0.91 (95% CI 0.41 to 2.03). (Fig. 2).

Time to death (a) and severe disease or death within 30 days of impatient admission (b).
Patients treated with B-cell depletion experienced longer time to clinical improvement, (aHR 0.65 ([0.45–0.94]). In this analysis, a reduced adjusted hazard (aHR < 1) indicated that time to event (in this case clinical improvement) was prolonged. The median time to improvement or hospital discharge was 6.3 days in the B-cell depleted group (IQR 3.3 to 11.2 days) and 4.2 days in the control group (IQR 2.2 to 7.7 days) (Table 3).
Subgroup analysis was performed for patients who had received B-cell depletion treatment within 90 days of COVID-19 hospitalization. There were no significant differences in 30-day mortality or time to severe illness compared to the control group. Among patients treated with B-cell depletion within the past 90 days, the B-cell depletion treatment group similarly experienced a longer median time to clinical improvement 6.3 days (IQR 2.9 to 10.9 days) vs. 4.2 days (IQR 2.2 to 7.7 days), aHR 0.54 (95% CI 0.33 to 0.89). These findings are illustrated in Fig. 3.

Cumulative improvement rate for (a) all patients treated with B-cell depletion therapy and (b) patients who received B-cell therapy within 90 days.
Discussion
This study has several important findings. First, patients who received B-cell depletion therapies matched to patients with similar demographic characteristics, comorbidities and severity of COVID-19 at hospital admission did not experience higher mortality rates within 30 days. Second, patients with prior B-cell depletion therapy experienced increased time to clinical improvement compared to matched controls. Finally, remote or more proximal treatment with B-cell depletion therapy did not result in different mortality rates.
The literature is mixed regarding the impact of B-cell depletion on outcomes with COVID-19. Prior work has found no increased risk in patients with lymphoid malignancies treated with B-cell depletion19,20,21,22 while other authors have demonstrated an increased risk of severe disease in patients treated with B-cell depletion9,11,23 and death8,10,13,24 in various populations treated with B-cell depletion. This discrepancy is likely explained due to heterogeneity within comparable studies including different eras, matching technique, particularly use of severity of illness on admission, and immunization in the population. A matched national cohort study in France of 63 patients with rheumatological and musculoskeletal diseases treated with rituximab, demonstrated a higher rate of severe disease but did not find increased risk of death9. A retrospective observational study in Spain including 57 patients treated with B-cell depletion for any indication found a higher rate of severe illness, longer length of stay and higher risk of death in patients with SARS-CoV-2 infection compared to patients without this treatment13. A comparative cohort study of 114 patients with rheumatological illness, using multivariate regression, found a higher mortality rate in recipients of B-cell depletion therapy compared to matched controls8. A large study including information from 42 health systems in the USA found an increased risk of in-hospital death in patients who had received rituximab prior to COVID-19 hospitalization; however, when stratified by sex, rituximab was associated with higher in-hospital death in women with cancer but not for women with rheumatological conditions or at all in men24. To account for these differences, risk may vary based on indications for B-cell treatment, comorbidities, center-specific management, different phases of the pandemic and different viral variants. This study also incorporates COVID-19 vaccination in matching which may affect disease outcomes. More recent work looking at vaccinated patients, has suggested that patients with prior B-cell depletion treatment have a higher rate of hospitalization due to breakthrough infection, although incidence is very low25,26.
This study attempts to match across a variety of factors. Notable strengths including access to granular hospitalization data and severity of illness, manual chart review of individual records, and use of propensity score matching to isolate effect of B-cell depletion. It also has several limitations. This study reflects the treatment of patients at a tertiary care center who were infected with SARS-CoV-2 prior to the rise of the Omicron variant which may have implications for disease severity. Use of overlap propensity score weighting is a statistical attempt to control differences between heterogenous populations whose treatment with B-cell depletion therapy may be further confounded by other unaccounted differences between groups. While we performed extensive matching, we did not account for baseline use of medications such as steroids which may account for some of the differences noted. This study is limited by its size and may be insufficiently powered to detect a mortality difference given the low incidence. Although the Johns Hopkins Health System treats many immunocompromised patients, these are part of a large and heterogeneous patient population with many different underlying diseases, whereas centers specializing in the treatment of cancer, for example, may have larger numbers of patients who had received B-cell depletion, and a more comparable control group. In particular, patients in this study were matched according to presence of any cancer diagnosis, not on the type of cancer and stage, both of which are important prognostic features, which further limits the matching technique. Similarly, additional chemotherapy beyond B-cell depletion was not accounted for in the matching process. The current study also did not consider immunoglobulin levels or treatment with monoclonal antibodies which may also contribute to the likelihood of progressing to severe illness and death. Additionally, a minority of patients with B-cell depletion were vaccinated, which further limits generalizability. The registry does not account for patients who may have been treated with B-cell depletion outside of the Johns Hopkins Health System; however, this likely accounts for a very small number of patients.
Conclusions
This study illustrates that patients treated with B-cell depletion experienced prolonged hospitalization due to SARS-CoV-2 infection but did not show an increased mortality compared to similar patients who had not received B-cell depletion therapy. These findings suggest that, in some settings, prior B-cell depletion therapy may not necessarily portend an adverse outcome in terms of mortality from COVID-19 however the study may be underpowered to determine a difference. Larger studies utilizing data from multiple centers would be helpful to confirm these findings. More research on the effect of vaccination status on outcomes, the impact of prompt treatment or pre-exposure prophylaxis with SARS-CoV-2 monoclonal antibodies, the incidence of PASC and persistent SARS-CoV-2 PCR positivity in this population, as well as the impact of future variants, will be needed to best protect and care for this vulnerable population.
Data availability
De-identified data and analytic code are available from the corresponding author upon reasonable request.
References
Ho, F. K. et al. Is older age associated with COVID-19 mortality in the absence of other risk factors? General population cohort study of 470,034 participants. PLoS ONE 15(11), e0241824. https://doi.org/10.1371/journal.pone.0241824 (2020).
Nguyen, N. T. et al. Male gender is a predictor of higher mortality in hospitalized adults with COVID-19. PLoS ONE 16(7), e0254066. https://doi.org/10.1371/journal.pone.0254066 (2021).
Kompaniyets, L. et al. Body mass index and risk for COVID-19–related hospitalization, intensive care unit admission, invasive mechanical ventilation, and death—United States, March–December 2020. MMWR Morb. Mortal. Wkly. Rep. 70(10), 355–361. https://doi.org/10.15585/mmwr.mm7010e4 (2021).
Poudel, R. et al. Smoking is associated with increased risk of cardiovascular events, disease severity, and mortality among patients hospitalized for SARS-CoV-2 infections. PLOS ONE 17(7), e0270763. https://doi.org/10.1371/journal.pone.0270763 (2022).
Furer, V. et al. 2019 update of EULAR recommendations for vaccination in adult patients with autoimmune inflammatory rheumatic diseases. Ann. Rheum. Dis. 79(1), 39–52. https://doi.org/10.1136/annrheumdis-2019-215882 (2020).
Mitchell, J. et al. Effect of mycophenolate mofetil dosing on antibody response to SARS-CoV-2 vaccination in heart and lung transplant recipients. Transplantation 106(5), e269–e270. https://doi.org/10.1097/TP.0000000000004090 (2022).
Connolly, C. M. et al. Absence of humoral response after two-dose SARS-CoV-2 messenger RNA vaccination in patients with rheumatic and musculoskeletal diseases: A case series. Ann. Intern. Med. 174(9), 1332–1334. https://doi.org/10.7326/M21-1451 (2021).
Patel, N. J. et al. Coronavirus disease 2019 outcomes among recipients of ANTI-CD20 monoclonal antibodies for immune-mediated diseases: A comparative cohort study. ACR Open Rheumatol. 4(3), 238–246. https://doi.org/10.1002/acr2.11386 (2022).
Avouac, J. et al. COVID-19 outcomes in patients with inflammatory rheumatic and musculoskeletal diseases treated with rituximab: A cohort study. Lancet Rheumatol. 3(6), e419–e426. https://doi.org/10.1016/S2665-9913(21)00059-X (2021).
Strangfeld, A. et al. Factors associated with COVID-19-related death in people with rheumatic diseases: Results from the COVID-19 global rheumatology alliance physician-reported registry. Ann. Rheum. Dis. 80(7), 930–942. https://doi.org/10.1136/annrheumdis-2020-219498 (2021).
Sparks, J. A. et al. Associations of baseline use of biologic or targeted synthetic DMARDs with COVID-19 severity in rheumatoid arthritis: Results from the COVID-19 global rheumatology alliance physician registry. Ann. Rheum. Dis. 80(9), 1137–1146. https://doi.org/10.1136/annrheumdis-2021-220418 (2021).
Levavi, H., Lancman, G. & Gabrilove, J. Impact of rituximab on COVID-19 outcomes. Ann. Hematol. 100(11), 2805–2812. https://doi.org/10.1007/s00277-021-04662-1 (2021).
Calderón-Parra, J. et al. Incidence, clinical presentation, relapses and outcome of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection in patients treated with anti-CD20 monoclonal antibodies. Clin. Infect. Dis. 74(10), 1786–1794. https://doi.org/10.1093/cid/ciab700 (2022).
Marshall, J. C. et al. A minimal common outcome measure set for COVID-19 clinical research. Lancet Infect. Dis. 20(8), e192–e197. https://doi.org/10.1016/S1473-3099(20)30483-7 (2020).
Thomas, L. E., Li, F. & Pencina, M. J. Overlap weighting: A propensity score method that mimics attributes of a randomized clinical trial. JAMA 323(23), 2417. https://doi.org/10.1001/jama.2020.7819 (2020).
Li, F. & Thomas, L. E. Addressing extreme propensity scores via the overlap weights. Am. J. Epidemiol. https://doi.org/10.1093/aje/kwy201 (2018).
Li, F., Morgan, K. L. & Zaslavsky, A. M. Balancing covariates via propensity score weighting. J. Am. Stat. Assoc. 113(521), 390–400. https://doi.org/10.1080/01621459.2016.1260466 (2018).
R Core Team. R: A language and environment for statistical computing. Published online 2020. https://www.R-project.org/
Riches, J. C. Impact of COVID-19 in patients with lymphoid malignancies. World J. Virol. 10(3), 97–110. https://doi.org/10.5501/wjv.v10.i3.97 (2021).
Vijenthira, A. et al. Outcomes of patients with hematologic malignancies and COVID-19: A systematic review and meta-analysis of 3377 patients. Blood 136(25), 2881–2892. https://doi.org/10.1182/blood.2020008824 (2020).
Lamure, S. et al. Determinants of outcome in Covid-19 hospitalized patients with lymphoma: A retrospective multicentric cohort study. EClinicalMedicine 27, 100549. https://doi.org/10.1016/j.eclinm.2020.100549 (2020).
Regalado-Artamendi, I. et al. Risk factors and mortality of COVID-19 in patients with lymphoma: A multicenter study. HemaSphere 5(3), e538. https://doi.org/10.1097/HS9.0000000000000538 (2021).
Sormani, M. P. et al. Disease-modifying therapies and coronavirus disease 2019 severity in multiple sclerosis. Ann. Neurol. 89(4), 780–789. https://doi.org/10.1002/ana.26028 (2021).
Andersen, K. M. et al. Long-term use of immunosuppressive medicines and in-hospital COVID-19 outcomes: A retrospective cohort study using data from the National COVID Cohort Collaborative. Lancet Rheumatol. 4(1), e33–e41. https://doi.org/10.1016/S2665-9913(21)00325-8 (2022).
Boekel, L. et al. Breakthrough SARS-CoV-2 infections with the delta (B.1.617.2) variant in vaccinated patients with immune-mediated inflammatory diseases using immunosuppressants: A substudy of two prospective cohort studies. Lancet Rheumatol. 4(6), e417–e429. https://doi.org/10.1016/S2665-9913(22)00102-3 (2022).
Cook, C. et al. Clinical characteristics and outcomes of COVID-19 breakthrough infections among vaccinated patients with systemic autoimmune rheumatic diseases. Ann. Rheum. Dis. 81(2), 289–291. https://doi.org/10.1136/annrheumdis-2021-221326 (2022).
Acknowledgements
The data utilized for this publication were provided by the Johns Hopkins COVID-19 Precision Medicine Center of Excellence, officially designated by the Precision Medicine Analytics Platform (PMAP) leadership and based on the contribution of many patients and clinicians. We would like to thank Bonnie Woods, MS/ITS, MLA, IT Director, Institute for Clinical and Translational Research (ICTR) Informatics Core, Johns Hopkins University School of Medicine and Laura Prichett, PhD, faculty lead, Johns Hopkins BEAD Core (Biostatistics, Epidemiology, and Data Management Core). This work would not be possible without the work of Amanda Bertram, MS, Research Associate, Johns Hopkins University School of Medicine.
Funding
This publication was made possible by the Johns Hopkins Institute for Clinical and Translational Research (ICTR) which is funded in part by Grant Number UL1TR003098 from the National Center for Advancing Translational Sciences (NCATS) a component of the National Institutes of Health (NIH), and NIH Roadmap for Medical Research. Its contents are solely the responsibility of the authors and do not necessarily represent the official view of the Johns Hopkins ICTR, NCATS or NIH. Other funding reported by the authors is as follows: KW and YX report funding from Johns Hopkins in Health, BG reports funding from the Johns Hopkins University COVID-19 Research Response Program, SS reports funding from The National Heart, Lung, and Blood Institute at the National Institutes of Health (K23HL155507) and the Parker B. Francis Foundation. DG reports no funding sources. MR reports funding from the Sherrilyn and Ken Fisher Center for Environmental Infectious Diseases, Rapid Acceleration of Diagnostics (RADx) via the National Institute of Biomedical Imaging and Bioengineering at the National Institutes of Health U54EB007958 and the Critical Path Institute at the Food and Drug Administration 2U18FD005320. FD reports funding from The National Heart, Lung, and Blood Institute at the National Institutes of Health R01HL131812.
Author information
Authors and Affiliations
Contributions
Substantial contributions to the conception or design of the work; WMG, TL, KW, YX, BTG, MVDP. Substantial contributions to the acquisition or analysis of data for the work: WMG, TL, KW, YX, KAG, MR, BTG. Substantial contributions to the interpretation of data for the work: All authors. Drafting the work or revising it critically for important intellectual content: All authors. Final approval of the version to be published: All authors. Agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved: All authors.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval and consent to participate
The study was performed in accordance with the Declaration of Helsinki and was approved under protocol IRB00283579 by the Johns Hopkins University School of Medicine Institutional Review Board. The need to obtain informed consent was waived by the Johns Hopkins University School of Medicine Institutional Review Board.
Consent for publication
Due to the retrospective nature of the study, Johns Hopkins University School of Medicine Institutional Review Board waived the need of obtaining informed consent. Data for the study publication was obtained from protocol IRB00247569 which maintains current IRB approval and was included under a waiver of consent.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Garneau, W.M., Wang, K., Liang, T. et al. Effect of antecedent B-cell depletion therapy for patients hospitalized with COVID-19 within a single health system: a propensity score analysis. Sci Rep 15, 9647 (2025). https://doi.org/10.1038/s41598-025-94024-y
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-94024-y
