
Abstract
The prevalence of urolithiasis and renal colic-like pain symptoms differs by region because of geographical, climatic, dietary, genetic, and lifestyle factors. In addition, reliable data for Central and Eastern Europe are lacking. Therefore, we analyzed the prevalence, correlates, and treatment behaviors for these conditions in a representative sample of 10,029 adult Poles. We used an Internet interview format and based our sample on the latest population census data. The lifetime prevalence of urolithiasis was 12.85% (n = 1289), and renal colic-like pain symptoms during lifetime were reported to be 43.05% (n = 4317). Sociodemographic factors such as age, place of residence, education, marital and employment status, and workplace-related circumstances (particularly exposure to high temperatures) were associated with urolithiasis and renal colic-like pain symptoms; no sex differences were observed. Over 20 conditions correlated with high prevalence of urolithiasis and renal colic-like pain symptoms. Lifestyle habits also influenced prevalence, with salting food increasing the risk of urolithiasis, and smoking and alcohol consumption being linked to renal colic-like pain symptoms. Encouragingly, most participants with urolithiasis and renal colic-like pain symptoms sought and received treatment. These findings, consistent with studies worldwide, provide valuable guidance for developing and implementing effective health improvement programs targeting urolithiasis in Poland.
Similar content being viewed by others

Introduction
Urolithiasis, commonly known as stone disease, is a significant global health concern. Urolithiasis is characterized by the formation of calculi in the urinary tract. Its prevalence is influenced by a complex interplay of geographical, climatic, dietary, genetic, and lifestyle factors; frequencies exist from 1 to 20% across different populations1. Recent evidence suggests an increasing trend in prevalence worldwide, driven by changes in diet, sedentary lifestyles, and rising rates of metabolic disorders such as obesity and diabetes2,3,4. Urolithiasis can lead to a variety of effects, from mild discomfort (e.g., pain—renal colic) to severe complications (e.g., hydronephrosis and decreased kidney function). Further effects of urolithiasis may even include psychological issues (e.g., depression and anxiety) and economic and lifestyle problems (e.g., reduced work productivity and the financial burden of medical costs)5,6.
Despite many epidemiological studies, reliable population-level data for urolithiasis and renal colic-like pain symptoms are still lacking for Central and Eastern Europe. Even in large-scale European studies conducted to ascertain the prevalence of urolithiasis, investigators have not included countries from Central and Eastern Europe7,8,9. Although some population-level analyses on urolithiasis from Eastern Europe exist (e.g., Russia), often the raw data are not publicly available or the methodologies are unclear10. Furthermore, many of published studies were conducted in single cities (e.g., the Russian study was limited to the St. Petersburg area)10. In sum, no large population-representative study in any Central or Eastern Europe country has been conducted to reliably evaluate the prevalence of urolithiasis and renal colic-like pain symptoms.
Because of high rates of new and recurrent stones, the management of urolithiasis is costly, and the disease carries a significant morbidity and social burden, leading to considerable absence from one’s place of employment. Importantly, understanding the prevalence and associated treatment behaviors related to urolithiasis is essential for increasing general awareness, improving disease management, reducing its long-term complications, and potentially aiding in prevention. The prevalence and treatment data may also support developing targeted public health strategies with multidisciplinary frameworks for national health improvement programs and service delivery, with appropriate allocation of resources by governments and healthcare systems.
Poland, the largest country in Central Europe11,12, is also the third largest in Eastern Europe by land area, following Russia and Ukraine. Poland is also the easternmost country within the European Union13. To date, no reliable, population-representative study on urolithiasis and renal colic-like pain symptoms has been conducted in Poland. Importantly, the country, like others in Central and Eastern Europe, has unique demographic characteristics, including a highly homogenous population; over 99% of residents are Caucasian and more than 90% identify as Polish (i.e., supra-ethnic uniformity)14. Indeed, Slavic populations are often regarded as culturally distinct from other parts of Europe, mainly distinct from Germanic and Romance people15. Cultural norms may also have a significant influence in healthcare-related behaviors, with local traditions often discouraging open discussions about health16. Additionally, a significant portion of Poland’s population resides in rural areas, setting it apart from countries from which most urolithiasis epidemiological data originate. Many existing studies are focused on industrialized regions17,18; these studies lack specific comparisons between urban and rural areas. Consequently, population estimates from other countries or regions may not be fully applicable to Poland’s unique sociocultural and demographic context; in population-based studies, it crucial to consider sociocultural and demographic factors of the study population.
In sum, our knowledge is insufficient regarding the prevalence and actual burden of urolithiasis and renal colic-like pain symptoms in Poland. However, there has been growing recognition of the value of population-based research in Poland and across Central-Eastern Europe19,20,21. In response, in this study, we aimed to provide a reliable assessment of the prevalence, correlates, and treatment behaviors for urolithiasis and renal colic-like pain symptoms in a population-representative sample of adults aged 18 years and older from all regions of Poland.
Methods
The study was population-based, representative, and cross-sectional, conducted in accordance with standardized guidelines and established recommendations for reporting observational research22. The goal was to provide reliable estimates of urolithiasis and renal colic-like pain symptoms in Poland (running title: POLSTONE).
The Research Ethics Committee of Jagiellonian University Medical College, Krakow, Poland approved the study (118.6120.94.2023), and the study is registered with ClinicalTrials.gov (NCT06176469). Informed consent was obtained from all participants prior to their inclusion in the study. All respondents were informed about the survey’s duration, the type of data collected, data storage details, identity of the investigator, and the study’s purpose.
Study design
Computer-assisted web interviews were conducted from November 1, 2023, to January 15, 2024. This time frame was selected specifically to exclude the high-temperature season because hot weather may predispose individuals to the symptoms of renal colic-like pain and thereby skew their prevalence17,23; high temperature accounts for 24%-84% of increase in stone presentation24. Considering that 93.33% of Polish households had internet access in 2022, with no significant difference between urban and rural areas (as reported by Eurostat and the Central Statistical Office of Poland)25, web-based interviews were deemed a justified method for conducting a reliable population-based study. We based our sample on the latest population census data (2021)26 and employed a proportionate quota sampling technique to create a representative sample of respondents, ensuring that the data accurately reflected the entire population. Quota controls were used for age, sex, and place of residence, encompassing all 16 voivodships/states in Poland and distinguishing between urban and rural areas. Urban areas were defined as areas within the administrative boundaries of cities and towns, whereas rural areas included regions outside these boundaries, such as rural gminas and rural sections of urban–rural gminas, in accordance with definitions provided by the Central Statistical Office of Poland27.
Survey distribution
The survey was conducted by 4P, a research agency accredited with appropriate quality certifications (PKJPA) and memberships in OFBOR and ESOMAR28,29. The agency also maintains extensive population-level respondent databases, including pre-existing internet panels with approximately 80,000 members at the time of this study. Panel members were selected using quota controls and invited via email to participate in the confidential and voluntary survey, with a total of 43,453 invitations sent. Each participant was provided with a unique Uniform Resource Locator (URL, i.e., duplicated completions were not permitted) to access the survey. Responses were securely collected on a web server equipped with a Secure Sockets Layer (SSL) certificate, ensuring website authentication and encrypted data transmission.
To ensure integrity, quality control measures and stratification checks were implemented during data collection. Post-stratification weights, after data collection, were used to address response rate discrepancies, aligning completed interviews with key variables such as age, sex, and residence. Suspicious responses, including those from participants completing the survey too quickly (under 20% of the average time) or too slowly (over 10 min per page), were excluded to maintain reliability.
Measure
The literature lacks a reliable, widely accessible, and validated tool for measuring the prevalence, correlates, and treatment behaviors associated with urolithiasis and renal colic-like pain symptoms. To address this gap, we developed a new questionnaire specifically for this study; the questionnaire was based on respected urology reference texts30,31 and the European Association of Urology (EAU) Guidelines for Urolithiasis32. Three authors (JS, PC, MP) developed the initial draft of the questionnaire, which was then revised with four rounds of discussions with the remaining authors (MC, PD, PR, WK, PB). After unanimous approval, a Polish language specialist reviewed the questionnaire for semantic and conceptual accuracy. To assess clarity and relevance of the questionnaire in one-on-one discussions (i.e., direct interviews), pilot testing was conducted with 50 patients scheduled for surgical intervention for urolithiasis and 50 patients with urolithiasis confirmed via computed tomography in an emergency unit. Feedback indicated that the questionnaire was clear and quick to complete, requiring only one minor language adjustment to improve flow without altering content. All questions and terms were presented in Polish. The finalized questionnaire, along with its English translation, is included in the Supplementary Information.
Objectives
The primary study objective was to assess the prevalence of urolithiasis and renal colic-like pain symptoms in Polish adults (≥ 18 years).
The secondary objectives were to determine the correlations between urolithiasis or symptoms of renal colic and demographic parameters, relevant comorbidities, or lifestyle factors, and treatment-related behaviors in Poland.
Statistics
Descriptive statistics included means, standard deviations, medians, quartiles, and ranges for quantitative variables, and absolute/relative frequencies (N, %) for qualitative variables. Group comparisons were conducted with chi-squared tests with Yates’ correction or Fisher’s exact test for qualitative data and Mann–Whitney or Kruskal–Wallis tests with post-hoc Dunn tests for quantitative data. Multiple logistic regression was used to analyze dichotomous variables, reporting odds ratios with 95% confidence intervals, including all predictors without selection. A 0.05 significance level was applied, and analyses were conducted using R (version 4.4.1).
For sample size calculation, we followed the methodology that was used in other population-level studies of prevalence of urological conditions19,20,33,34,35. The sample size was predetermined prior to the start of the study and remained unaltered throughout its duration. The determination of the sample size for our study was influenced by factors such as the expected event rate within the population, the standard deviation of the population, the chosen significance threshold, the expected magnitude of the effect, and the required statistical power36. Using the population age distribution and guidelines from the most recent census for conducting future population-representative studies in Poland26, we determined a sample size of 10,000 respondents. With a national sample of 10,000, there was a 95% certainty that the overall survey results would deviate by less than 1% from what would have been obtained if the entire adult population of Poland had been surveyed.
Results
Demographics
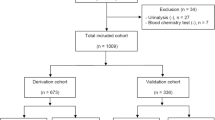
A total of 10,029 participants completed the survey, with 48.34% men (n = 4,848) and 51.66% women (n = 5,181). Given the large sample size, we categorized the respondents into five age groups: 18–29 (n = 1,655; 16.5%), 30–39 (n = 1,964; 19.58%), 40–49 (n = 1,923; 19.17%), 50–59 (n = 1,506; 15.02%), and ≥ 60 years (n = 2,981; 29.72%). Most participants had at least secondary education (n = 7,093; 70.72%), were employed (n = 5,409; 53.93%), and married (n = 5,281; 52.66%). More participants lived in urban areas than in rural regions (n = 6,678; 66.59% vs. n = 3,351; 33.41%). The response rate of our survey was 23.1%.
Prevalence of urolithiasis and renal colic-like pain symptoms.
The lifetime prevalence of urolithiasis was 12.85% (n = 1,289), and the lifetime prevalence of renal colic-like pain symptoms was 43.05% (n = 4,317). Among individuals with urolithiasis, kidney stones were the most often reported followed by ureteral and bladder stones (Fig. 1). Additionally, 41.04% (n = 529) reported experiencing recurrent urolithiasis. Similarly, 64.19% (n = 2,771) of persons with renal colic-like pain symptoms reported recurrent episodes, and 12.05% (n = 520) stated that their symptoms first appeared within the preceding 12 months.

Distribution of stone location: (a) individual locations and (b) combinations.
Most respondents diagnosed with urolithiasis reported experiencing renal colic-like pain symptoms (81.23%; 1,047 out of 1,289), whereas less than one in five participants with a diagnosis of urolithiasis did not report such symptoms (18.77%; 242 out of 1,289). Conversely, only one-fourth of all respondents with renal colic-like pain symptoms reported a diagnosis of urolithiasis (24.25%; 1,047 out of 4,317), with most reporting renal colic-like symptoms denying having received a urolithiasis diagnosis (75.75%; 3,270 out of 4,317).
Correlates
Sociodemographic parameters.
Urolithiasis prevalence (Table 1) was highest among individuals aged 60 + (16.87%) and lowest in the 18–29 age group (7.79%; p < 0.001). Urolithiasis was more common in residents of cities having over 500,000 inhabitants (15.35%) compared with rural areas (10.74%; p < 0.001). Urolithiasis was more common among persons with higher education (13.82%) compared with persons having only primary education (9.83%; p = 0.027). Widowed individuals had the highest prevalence (16.18%), whereas unmarried individuals had the lowest (8.76%; p < 0.001). In terms of professional activity and work-related factors, the highest percent of urolithiasis was observed among retirees and pensioners (16.45%), whereas the lowest was recorded for the unemployed (9.33%; p < 0.001). Workplace exposure to high ambient temperatures nearly doubled prevalence (19.29% vs. 11.09%; p < 0.001). Intellectual/white-collar workers had the highest prevalence (14.41%), whereas individuals who were never employed had the lowest (10.79%; p < 0.001). Urolithiasis prevalence was unaffected by free workplace access to drinking water or toilets. Finally, we did not observe differences in prevalence of urolithiasis between men and women.
Renal colic-like pain symptoms (Table 2) were most prevalent in the 30–39 age group (49.80%) and least in persons aged 60 + (35.09%; p < 0.001). Prevalence was highest in cities with 20,000–100,000 inhabitants (45.72%) and lowest in rural areas (41.33%; p = 0.012). Respondents with vocational education had the highest prevalence (48.78%) compared with persons who had higher education (38.85%; p < 0.001). Married individuals reported the highest prevalence (44.42%), whereas widowed respondents had the lowest (38.73%; p = 0.011). In terms of professional activity and work-related factors, housewives/husbands showed the highest prevalence (46.76%) and pensioners the lowest (36.20%; p < 0.001). Workplace exposure to high ambient temperatures nearly doubled prevalence of symptoms (61.55% vs. 37.98%; p < 0.001). Manual/blue-collar workers had the highest prevalence (47.89%), whereas persons who were never employed had the lowest (35.97%; p < 0.001). Prevalence of renal colic-like pain symptoms was unaffected by workplace access to drinking water or toilets. There were no differences observed between men and women, mirroring the estimates for urolithiasis.
Comorbidities
Compared with persons who did not have other conditions (p < 0.001, Table 3), the percent of respondents diagnosed with urolithiasis was higher for persons with the following comorbidities: hypertension, heart failure, diabetes, overweight/obesity, gout, liver diseases, bowel diseases, after bowel surgeries, chronic kidney disease, polycystic kidney disease, hyperparathyroidism, any oncological diseases (including hematopoietic system and urological cancers), sarcoidosis, multiple sclerosis, spinal cord injury, neurogenic lower urinary tract dysfunction (previously known as neurogenic bladder), benign prostatic enlargement, recurrent urinary tract infections, and other urological conditions.
The percent of respondents with renal colic-like pain symptoms was higher among persons who had one of the same conditions as for urolithiasis listed above, compared with persons without these conditions (p < 0.01, Table 4).
Lifestyle habits
For urolithiasis (Table 5), the percent of patients diagnosed with urolithiasis was higher only among persons who added salt to their food compared with people who did not add salt (p < 0.001). Smoking, excessive alcohol consumption, and high fluid intake were not associated with urolithiasis.
Conversely, the percent of respondents who had renal colic-like pain symptoms was higher among smokers and persons who consumed two or more servings of alcohol per day compared to non-smokers and persons who consumed lower amounts of alcohol (p < 0.001, Table 5). Salting food and high fluid intake were not associated with renal colic-like pain symptoms.
Multiple logistic regression
With regression models, we examined the relations of urolithiasis and renal colic-like pain symptoms with all potential predictors (classified as independent variables). For urolithiasis (Table 6), the regression model confirmed the effects of age (the higher the age, the higher likelihood of urolithiasis), marital status (a marital relationship increases the likelihood of urolithiasis), workplace-related factors (high ambient temperature in the workplace increases the likelihood of urolithiasis), comorbidities (hypertension, gout, chronic kidney disease, and recurrent urinary tract infections increase the likelihood of urolithiasis), and lifestyle habits (whereas adding salt to food increases the likelihood of urolithiasis, excessive alcohol consumption reduces urolithiasis likelihood).
For renal colic-like pain symptoms (Table 7), the regression model confirmed the effects of age (the higher the age, the lower likelihood of symptoms), marital status (a marital relationship increases the likelihood of symptoms), employment status (whereas working in a blue-collar profession increases the likelihood of symptoms, being a pensioner decreases it), workplace-related factors (high ambient temperature in the workplace increases the likelihood of symptoms), comorbidities (hypertension, heart failure, diabetes, overweight/obesity, gout, any liver disease, any bowel disease, chronic kidney disease, polycystic kidney disease, spinal cord injury, recurrent urinary tract infections, and any other urological conditions increase the likelihood of symptoms), and lifestyle habits (smoking and excessive alcohol intake increase the likelihood of symptoms).
Treatment-Related Behavior.
A significant proportion of respondents with renal colic-like symptoms sought (68.4%, n = 2,853) and received (65.32%, n = 2,820) treatment; women were significantly more likely to seek help than men (70.17% vs. 66.49%; n = 1,576 vs. 1,377; p = 0.01). Even higher rates of treatment-seeking and treatment-receiving were observed among respondents who reported renal colic-like pain symptoms along with the diagnosis of urolithiasis, with 91.6% (959 out of 1,047) seeking and 89.4% (936 out of 1,047) receiving treatment.
Older respondents, those with higher education, married or widowed, and pensioners or employed individuals were more likely to seek treatment (p < 0.001; Table 8). Work-related factors, such as intellectual occupations, exposure to high ambient temperatures, and easy access to drinking water or toilets at work, also correlated with treatment-seeking (p < 0.01). Place of residence had no effect (p = 0.527). Logistic regression confirmed significant effects of sex, age, marital status, employment, and work-related factors (Table 9).
Treatment-receiving rates were similarly higher among older individuals, with higher education, widowed or married, and pensioners or employed but also persons living in urban areas (p < 0.05; Table 10). Work-related factors mirrored the treatment-seeking trends (p < 0.05). Sex had no significant effect (p = 0.092). Logistic regression confirmed associations with age, place of residence, marital status, employment, and work-related factors (Table 11).
Among respondents reporting renal colic symptoms, 46.63% (n = 2,013) described moderate (n = 1,243), severe (n = 613), or very severe (n = 157) bother. Excessive bother was reported by women, those aged 50–59, with at least secondary education, married or widowed, and pensioners (p < 0.001; Table 12). Interestingly, limited access to drinking water or toilets at work was also linked to high bother (p < 0.05).
Discussion
This study is the first population-representative and reliable epidemiological analysis of urolithiasis and renal colic-like pain symptoms conducted in a Central and Eastern European country, namely, Poland. The analysis included men and women aged 18 years and older from all geographical regions, ensuring appropriate representation from both urban and rural areas. Multiple detailed questions were posed, and regular quality-control measures were implemented to ensure reliability. As a result, our investigation offers consistent and dependable population-level estimates of the prevalence, associated factors, and treatment behaviors related to urolithiasis and renal colic-like pain symptoms. The findings revealed that these conditions are prevalent and significantly associated with various sociodemographic factors, comorbidities, and lifestyle habits. Encouragingly, because the symptoms were reported to carry a substantial burden, most respondents experiencing renal colic-like symptoms sought and received treatment.
Sorokin et al. conducted a comprehensive analysis of the global epidemiology of stone disease, highlighting its widespread prevalence across various regions1. Their findings revealed that urolithiasis affects 7–13% of individuals in North America, 5–9% in Europe, and 1–5% in Asia1,37,38,39. Differences in prevalence were associated with factors such as genetics, environmental temperature, latitude, water quality, affluence, dietary habits, age distribution, and, importantly, methodology (e.g., population surveys, physician-administered surveys, analyses of databases for inpatient and outpatient care). Additionally, challenges in data availability hindered a full understanding of global patterns. Although some countries, such as the United States, maintain robust data by initiatives like the Urologic Diseases of America Project40, reliable epidemiological data are lacking for one-third to one-half of the global population. Particularly, large-scale studies from South Central Asia and Sub-Saharan Africa are absent, and data accessibility in regions like China is limited due to language barriers1. Even within Europe, prevalence varies widely. For instance, Hesse et al. reported a prevalence of urolithiasis of 4.7% (n = 7,500) in Germany8, and in Spain Arias Vega et al. estimated the prevalence of urolithiasis at 14.6% (n = 2,444)41. In comparison, the prevalence in the United States falls between these estimates at 11% (n = 10,521)42. Therefore, our study’s finding of the urolithiasis prevalence of 12.85% (n = 10,029) is broadly consistent with data from similar population-based studies in other regions. Nevertheless, despite the variations discussed, it is essential to acknowledge that urolithiasis is a global issue, and it represents a significant public health challenge. Although genetic, environmental, lifestyle, and cultural factors all influence its development, none fully account for the occurrence of urolithiasis. With aging populations and the increasing prevalence of obesity, diabetes, and hypertension, urolithiasis is becoming increasingly common, particularly in developed countries.
Surprisingly, the prevalence of renal colic-like pain symptoms has not been analyzed as extensively as that of urolithiasis. Most studies are focused on presentations to emergency departments due to renal colic symptoms, with limited data on the true population-level prevalence of these symptoms. In fact, we identified only one population estimate. Patti et al., in their review paper, noted that “according to the National Institutes of Health, approximately 6% of women and 11% of men in the US will experience a kidney stone attack at some point in their lives”43; however, this statement lacks a supporting reference. More comprehensive data come from emergency department studies. In the United States, data from 15 New Jersey emergency departments revealed that, of 3.5 million patient visits over a six-year period, 30,358 (0.9%) were due to renal colic44. Similarly, in France, renal colic accounts for 1–2% of emergency consultations, corresponding to approximately 170,000 visits annually45. In Pisa, Italy, renal colic symptoms constituted 1% of yearly emergency department appointments (696 cases out of 70,621 visits)46. In South Korea, 23,653 cases of renal colic recorded annually across 46 participating emergency departments accounted for 1.8% of all emergency department visits47. Finally, in Qatar, renal colic presentations were estimated at 27.9 per 1,000 visits48. These findings suggest that renal colic-like symptoms are common conditions. However, it is important to note that not all individuals experiencing renal colic symptoms immediately seek emergency care; some may not seek medical help at all or some may consult primary care physicians instead. This lack of seeking emergency care raises the hypothesis that the true prevalence of kidney stone attacks may be greater than reported in emergency department studies. Our observed lifetime prevalence of renal colic-like pain symptoms, 43.05%, represents the first population-level estimate derived from a representative study with well-balanced demographic characteristics. Importantly, our study warrants further investigation on the true population-level prevalence of renal colic-like symptoms.
Interestingly, only one-third of respondents who experienced renal colic symptoms reported receiving a diagnosis of urolithiasis, even though most sought professional medical help and underwent treatment. This discrepancy may arise from the similarity of renal colic symptoms to symptoms of non-urological conditions, such as musculoskeletal pain, gastrointestinal disorders, or gynecological issues of women. Notably, Moore et al. demonstrated that, over a five-year period at two emergency departments, ureteral stones were identified as the cause of symptoms in only 47.7% of flank pain protocol computed tomography scans, and no identifiable cause of symptoms was found in 43.3% of scans49. These overlapping symptoms can pose significant diagnostic challenges, particularly when initial evaluations are limited to basic assessments or are limited by a lack advanced imaging techniques. Additionally, the transient nature of some renal colic episodes, possibly due to the spontaneous passage of small stones, may further contribute to the underdiagnosis of urolithiasis. On the contrary, the economic burden of widespread imaging for all cases of renal colic could pose a significant challenge for public healthcare systems. This emphasizes the importance of clinical judgment and risk stratification in determining the need for further evaluation, balancing the potential benefits of advanced imaging against economic and healthcare resource considerations. Additionally, the role of conservative management, including pain control and hydration, should be considered in cases where immediate imaging is not required. Therefore, if symptoms subside without recurrence, further advanced imaging may not be necessary. This may also help explain the discrepancy we observed in our study between experiencing renal colic symptoms and receiving a diagnosis of urolithiasis. In summary, all these findings highlight the importance of improving diagnostic accuracy through standardized clinical protocols, while carefully selecting patients for further evaluation based on clinical presentation, risk factors, and symptom severity. The use of advanced imaging modalities and enhanced awareness among healthcare providers are also crucial to ensure timely and accurate identification and management of urolithiasis.
Sociodemographic parameters have significant effects on urolithiasis. In the United States, a study by Scales et al. demonstrated that stone disease affected Caucasian persons more frequently than Hispanic and African American individuals50. The study also demonstrated that the overall prevalence of stone disease was higher in men than in women (10.6% vs. 7.1%). This finding contrasts with our observation that no difference existed in urolithiasis prevalence between men and women. The US study also differs from findings in claims-based analyses of health care utilization, particularly in inpatient settings40,51. These studies have suggested a narrowing of the historical risk difference for stone disease between men and women. Experts postulate that men are historically more likely to form stones, as represented by the large difference in prevalence between older men and women. However, risks are now more balanced, particularly among younger men and women aged 20–49 years, as reflected by the similar prevalence of stone disease between sexes in this age group50.
Geographic variability also has a crucial influence, with studies indicating a 20–50% higher prevalence of nephrolithiasis in the US Southeast compared with the Northwest. The greater prevalence in the South is attributed to climatic factors such as higher temperature, humidity, and greater sunlight exposure52. Our findings reinforce the influence of residence; we observed significant differences in urolithiasis prevalence between urban and rural areas. These differences could be explained by differences between these populations in dietary habits, occupation types, and lifestyle factors.
Interesting differences were also observed in education level and type of work. Individuals with higher education or white-collar occupations exhibited a greater prevalence of urolithiasis but a lower prevalence of renal colic symptoms. Conversely, those with primary or vocational education had a lower prevalence of urolithiasis but a higher prevalence of renal colic symptoms. These patterns may be attributed to the fact that blue-collar workers and individuals with lower education levels are often engaged in physically demanding work, which can lead to symptoms frequently misinterpreted as renal colic, such as musculoskeletal pain. Persons with higher education and white-collar jobs likely have better access to professional healthcare and more accurate diagnoses of urolithiasis. Further, our study confirms the link between occupational heat exposure and urolithiasis, with affected individuals having nearly double the prevalence of kidney stones. This finding aligns with findings of Lu et al. who identified heat exposure as an independent risk factor among 1,681 steel workers in Southern Taiwan53, highlighting the need for preventive measures in high-temperature workplaces. Interestingly, our study revealed that free access to drinking water and workplace toilets did not significantly influence the prevalence of urolithiasis. Nevertheless, respondents with limited access to drinking water or workplace toilets were more likely to report being bothered by their symptoms. Thus, although hydration and urination frequency may influence stone formation in occupational settings, other factors beyond hydration and urination frequency are also involved. Potential contributors could include diet, genetic predisposition, or inadequate use of available hydration resources, warranting further investigation.
Multiple links have been reported between urolithiasis and comorbidities. The EAU Guidelines list dozens conditions associated with an increased risk of urolithiasis32. We identified more than 20 conditions correlating with a higher prevalence of urolithiasis. Notably, multivariate regression confirmed that hypertension, gout, chronic kidney disease, and recurrent urinary tract infections were significantly associated with an increased prevalence of urolithiasis. In hypertension, altered renal handling of calcium and kidney damage due to chronic high blood pressure are postulated to increase the risk of urolithiasis54. In gout, elevated serum urate levels along with predispositions to dehydration can lead to the formation and deposition of monosodium urate crystals, contributing to urolithiasis55. In chronic kidney disease, impaired excretion, metabolic acidosis, and dietary restrictions can alter urine composition, promoting stone formation54. Recurrent urinary tract infections, especially those caused by urease-producing bacteria, can lead to the formation of struvite stones32. In contrast, our regression models identified even more conditions independently correlated with renal colic-like pain symptoms, highlighting the overlap between renal colic due to urolithiasis and various non-urological conditions. Understanding these correlations and potential pathophysiological mechanisms may aid in targeted diagnostics and management of underlying conditions, thereby improving urolithiasis diagnosis and even its prevention.
Considering life-style factors, our study confirmed that salting food was an independent risk factor for urolithiasis whereas excessive alcohol consumption reduced the risk. High sodium intake increases urinary calcium excretion (hypercalciuria) and reduces urinary citrate, both promoting stone formation56,57. Conversely, in a systematic review and meta-analysis, Wang et al. found a 10% reduction in kidney stone risk for every 10 g/day increase in alcohol intake58. Similarly, a recent study by Wei et al. from the US found that heavy alcohol consumption was linked to a significantly reduced likelihood of kidney stone occurrence in various subgroups59. Nevertheless, alcohol consumption, although associated with a reduced risk of kidney stones in some studies, should be approached with caution due to its potential to cause dehydration if consumed excessively. Interestingly, our study also showed that excessive alcohol drinking was an independent risk factor for occurrence of renal colic-like pain symptoms.
Our study demonstrated that renal colic-like pain symptoms impose a substantial burden, with a significant proportion of respondents seeking and receiving treatment for these symptoms. Notably, women were more likely than men to seek medical assistance. Among the various sociodemographic factors influencing treatment-related behaviors, one factor deserves particular attention: Although the place of residence did not affect the likelihood of seeking help, individuals from rural areas reported lower rates of actually receiving treatment. This disparity may reflect limited access to healthcare services, fewer medical facilities, or longer travel distances in rural regions, underscoring the need for targeted strategies to improve healthcare accessibility and equity. Therefore, our healthcare system should consider including increasing the availability of rural healthcare facilities, implementing telemedicine services, and enhancing public health education.
Our study’s notable strength lies in its robust population representation, with balanced demographics and proportional inclusion of urban and rural participants, based on recent census data. The large sample size (n = 10,029) ensured a statistical error below 1%, making this analysis one of the most accurate on urolithiasis and renal colic-like symptoms prevalence within a single country. A tailored survey instrument, developed after an extensive literature review, was validated with a pilot trial. However, the study’s reliance on self-reported data without clinical verification poses a main limitation, as noted in similar urology research by Coyne et al.60. Some respondents may also have misunderstood certain questions despite efforts to ensure clarity, and the survey length limited the inclusion of all possible influencing factors. For instance, the term “renal colic” may remain vague for many individuals. Therefore, more accurate data could be obtained through further research that integrates clinical data or verification methods to cross-check self-reported information with actual medical records, providing more reliable prevalence estimates of urolithiasis and renal colic-like symptoms. Additionally, findings may not be fully generalizable to other cultures or ethnicities because the data reflect only a single country from Central and Eastern Europe.
Conclusions
This investigation is the first nationwide, population-representative epidemiological study of urolithiasis and renal colic-like pain symptoms conducted in Poland. Urolithiasis and renal colic-like pain symptoms were found to be prevalent conditions, closely associated with various comorbidities, lifestyle habits, and workplace-related factors. The majority of respondents experiencing these symptoms reported seeking and receiving treatment. Our findings align with epidemiological reports on urolithiasis from other regions worldwide and provide valuable insights that can inform health improvement programs for patients with urolithiasis.
Data availability statement
All data generated or analysed during this study are included in this published article.
References
Sorokin, I. et al. Epidemiology of stone disease across the world. World J. Urol. 35, 1301–1320 (2017).
Indridason, O. S. et al. Epidemiology of kidney stones in Iceland: A population-based study. Scand. J. Urol. Nephrol. 40, 215–220 (2006).
Edvardsson, V. O., Indridason, O. S., Haraldsson, G., Kjartansson, O. & Palsson, R. Temporal trends in the incidence of kidney stone disease. Kidney Int. 83, 146–152 (2013).
Yasui, T., Iguchi, M., Suzuki, S. & Kohri, K. Prevalence and epidemiological characteristics of urolithiasis in Japan: National trends between 1965 and 2005. Urology 71, 209–213 (2008).
Ni Neill, E., Richards, H. L., Hennessey, D., Ryan, E. M. & Fortune, D. G. Psychological distress in patients with urolithiasis: A systematic review and meta-analysis. J. Urol. 209, 58–70 (2023).
The global, regional, and national burden of urolithiasis in 204 countries and territories, 2000–2021: A systematic analysis for the Global Burden of Disease Study 2021. EClinicalMedicine 2024. 78, 102924.
Sánchez-Martín, F.M., Millán Rodríguez, F., Esquena Fernández, S., et al. [Incidence and prevalence of published studies about urolithiasis in Spain. A review]. Actas Urol Esp 2007. 31, 511–520.
Hesse, A., Brandle, E., Wilbert, D., Kohrmann, K.U., Alken, P. Study on the prevalence and incidence of urolithiasis in Germany comparing the years 1979 vs. 2000. European urology 2003. 44, 709–713.
Trinchieri, A. et al. Increase in the prevalence of symptomatic upper urinary tract stones during the last ten years. Eur. Urol. 37, 23–25 (2000).
Novikov, A., Nazarov, T. & Startsev, V. Y. Epidemiology of stone disease in the Russian Federation and Post Soviet Era. In Urolithiasis, Basic Science and Clinical Practice (eds Talati, J. et al.) 97–105 (Springer, 2012).
World Bank Group, World Bank; Poland At-A-Glance, Publicated: 2019 [Accessed: 2024 December]. Available from: https://www.worldbank.org/en/country/poland.
Organisation for Economic Co-operation and Development, OECD. “Constitutions of Central and Eastern European Countries and the Baltic States”, SIGMA Papers, No. 2, OECD Publishing 1995, Paris, https://doi.org/10.1787/5kml6gf26mvk-en.
Publications Office of the European Union; Country profile, Publicated: 2004. https://european-union.europa.eu/principles-countries-history/country-profiles/poland_en. [Accessed: 2024 December].
Glowny Urzad Statystyczny (GUS), Narodowy Spis Powszechny, Struktura narodowo-etniczna, językowa i wyznaniowa ludności Polski [National-ethnic, linguistic and religious structure of Poland. National Census of Population and Housing 2011] (in Polish); Publicated: 2015 [Cited: 2024 December] ISBN 978-83-7027-597-6.
Jarczak, J. et al. Mitochondrial DNA variability of the Polish population. Eur. J. Hum. Genet. 27, 1304–1314 (2019).
Branowitzer, Z. Number of patients seeking medical advice and morbidity in Poland (July 1967-June 1968). VII. Morbidity in urban and rural population in Poland based on a representative study. Przegl Epidemiol. 28, 195–204 (1974).
Chen, Y. K., Lin, H. C., Chen, C. S. & Yeh, S. D. Seasonal variations in urinary calculi attacks and their association with climate: A population based study. J. Urol. 179, 564–569 (2008).
Khan, A. S. et al. Epidemiological risk factors and composition of urinary stones in Riyadh Saudi Arabia. J. Ayub. Med. Coll. Abbottabad. 16, 56–58 (2004).
Przydacz, M., Chlosta, M., Rajwa, P. & Chlosta, P. Population-level prevalence, effect on quality of life, and treatment behavior for erectile dysfunction and premature ejaculation in Poland. Sci. Rep. 13, 13168 (2023).
Przydacz, M., Golabek, T., Dudek, P., Lipinski, M. & Chlosta, P. Prevalence and bother of lower urinary tract symptoms and overactive bladder in Poland, an Eastern European Study. Sci. Rep. 10, 19819 (2020).
Przydacz, M. et al. Sexual activity in a large representative cohort of Polish men: Frequency, number of partners, correlates, and quality of life. PLoS ONE 19, e0296449 (2024).
von Elm, E. et al. The strengthening the reporting of observational studies in epidemiology (STROBE) Statement: guidelines for reporting observational studies. Int. J. Surg. 12, 1495–1499 (2014).
Fukuhara, H., Ichiyanagi, O., Kakizaki, H., Naito, S. & Tsuchiya, N. Clinical relevance of seasonal changes in the prevalence of ureterolithiasis in the diagnosis of renal colic. Urolithiasis 44, 529–537 (2016).
Geraghty, R. M., Proietti, S., Traxer, O., Archer, M. & Somani, B. K. Worldwide impact of warmer seasons on the incidence of renal colic and kidney stone disease: Evidence from a systematic review of literature. J. Endourol. 31, 729–735 (2017).
Glowny Urzad Statystyczny (GUS), Spoleczenstwo informacyjne w Polsce w 2022 r. Publicated: 2022 [Cited: 2024 December]. https://stat.gov.pl/download/gfx/portalinformacyjny/pl/defaultaktualnosci/5497/2/12/1/spoleczenstwo_informacyjne_w_polsce_w_2022_r.pdf.
Glowny Urzad Statystyczny (GUS), Narodowe Spisy Powszechne; Publicated: 2021 [Cited: 2024 December]. https://stat.gov.pl/spisy-powszechne/.
Glowny Urzad Statystyczny (GUS) Regional Statistics. Classification of Territorial Units. Administrative Division of Poland Types of Gminas and Urban and Rural Areas Publicated: 2022 [Cited: 2024 December]. https://stat.gov.pl/en/regional-statistics/classification-of-territorial-units/administrative-division-of-poland/types-of-gminas-and-urban-and-rural-areas/.
4P Group, Pulawska Street 12A, 02–566, Warsaw, Poland. https://grupa4p.pl.
Program Kontroli Jakosci Pracy Ankieterow (PKJPA), Organizacja Firm Badania Opinii i Rynku (OBFOR); Publicated: 2000. https://www.pkjpa.pl [Cited: 2024 December].
Partin, A.W., Dmochowski, R.R., Kavoussi, L.R., Peters, C.A., Wein, A.J. (Editors). Campbell Walsh Wein Urology, 12th Edition (Book). Section IX Urinary Lithiasis and Endourology. Elsevier, 2020, ISBN 9780323546423.
Talati, J.J., Tiselius, H.G., Albala, D.M., Ye, Z. (Eds.). Urolithiasis, Basic Science and Clinical Practice (Book). Springer, London (2012) https://doi.org/10.1007/978-1-4471-4387-1.
European Association of Urology (EAU), Non-Oncology Guidelines [Internet]; Urolithiasis, Publicated: 2024. Available from: https://uroweb.org/guideline/urolithiasis/ [Cited: 2024 December].
Coyne, K. S. et al. Rationale for the study methods and design of the epidemiology of lower urinary tract symptoms (EpiLUTS) study. BJU Int. 104, 348–351 (2009).
Mak, R., De Backer, G., Kornitzer, M. & De Meyer, J. M. Prevalence and correlates of erectile dysfunction in a population-based study in Belgium. Eur. Urol. 41, 132–138 (2002).
Chen, K. K. et al. Prevalence of erectile dysfunction and impacts on sexual activity and self-reported intercourse satisfaction in men older than 40 years in Taiwan. Int. J. Impot. Res. 16, 249–255 (2004).
Kadam, P. & Bhalerao, S. Sample size calculation. Int. J. Ayurveda Res. 1, 55–57 (2010).
Ramello, A., Vitale, C. & Marangella, M. Epidemiology of nephrolithiasis. J. Nephrol. 13(Suppl 3), S45-50 (2000).
Pinduli, I. et al. Prevalence of urolithiasis in the autonomous city of Buenos Aires, Argentina. Urol. Res. 34, 8–11 (2006).
Medina-Escobedo, M., Zaidi, M., Real-de Leon, E. & Orozco-Rivadeneyra, S. Urolithiasis prevalence and risk factors in Yucatan, Mexico. Salud Publica Mex 44, 541–545 (2002).
Pearle, M. S., Calhoun, E. A. & Curhan, G. C. Urologic diseases of America P. urologic diseases in America project: urolithiasis. J. Urol. 173, 848–857 (2005).
Arias Vega, M. R. et al. Prevalence of urolithiasis in the 40 to 65 year old Spanish population: The PreLiRenE study. Med. Clin. (Barc). 146, 525–531 (2016).
Hill, A. J. et al. Incidence of kidney stones in the United States: The continuous national health and nutrition examination survey. J. Urol. 207, 851–856 (2022).
Patti, L., Leslie, S.W. Acute Renal Colic. StatPearls. Treasure Island (FL) ineligible companies. Disclosure: Stephen Leslie declares no relevant financial relationships with ineligible companies (2025).
Chauhan, V., Eskin, B., Allegra, J. R. & Cochrane, D. G. Effect of season, age, and gender on renal colic incidence. Am. J. Emerg. Med. 22, 560–563 (2004).
Daudon, M., Haymann, J. P., Estrade, V., Meria, P. & Almeras, C. 2022 Recommendations of the AFU Lithiasis committee: Epidemiology, stone analysis and composition. Prog. Urol. 33, 737–765 (2023).
Cupisti, A. et al. Renal colic in Pisa emergency department: epidemiology, diagnostics and treatment patterns. Intern. Emerg. Med. 3, 241–244 (2008).
Hong, D. Y., Kim, J. W., Lee, K. R., Park, S. O. & Baek, K. J. Epidemiologic and clinical characteristics of patients presenting with renal colic in Korea. Urol. J. 12, 2148–2153 (2015).
Pathan, S. A. et al. A comparative, epidemiological study of acute renal colic presentations to emergency departments in Doha, Qatar, and Melbourne Australia. Int. J. Emerg Med. 11, 1 (2018).
Moore, C. L., Daniels, B., Singh, D., Luty, S. & Molinaro, A. Prevalence and clinical importance of alternative causes of symptoms using a renal colic computed tomography protocol in patients with flank or back pain and absence of pyuria. Acad. Emerg. Med. 20, 470–478 (2013).
Scales, C. D., Smith, A. C., Hanley, J. M. & Saigal, C. S. Urologic diseases in America p. prevalence of kidney stones in the United States. Eur. Urol. 62, 160–165 (2012).
Scales, C. D. Jr. et al. Changing gender prevalence of stone disease. J. Urol. 177, 979–982 (2007).
Dallas, K. B. et al. Redefining the stone belt: Precipitation is associated with increased risk of urinary stone disease. J. Endourol. 31, 1203–1210 (2017).
Lu, I.C., Yang, C.C., Huang, C.H., et al. The risk factors for radiolucent nephrolithiasis among workers in high-temperature workplaces in the steel industry. Int. J. Environ. Res. Public Health 19 (2022).
Rule, A. D., Krambeck, A. E. & Lieske, J. C. Chronic kidney disease in kidney stone formers. Clin. J. Am. Soc. Nephrol. 6, 2069–2075 (2011).
Gustafsson, D. & Unwin, R. The pathophysiology of hyperuricaemia and its possible relationship to cardiovascular disease, morbidity and mortality. BMC Nephrol 14, 164 (2013).
Ticinesi, A., Nouvenne, A., Maalouf, N. M., Borghi, L. & Meschi, T. Salt and nephrolithiasis. Nephrol. Dial. Transplant. 31, 39–45 (2014).
Sakhaee, K., Harvey, J. A., Padalino, P. K., Whitson, P. & Pak, C. Y. The potential role of salt abuse on the risk for kidney stone formation. J. Urol. 150, 310–312 (1993).
Wang, X. et al. Systematic review and meta-analysis of the effect of alcohol intake on the risk of urolithiasis including dose-response relationship. Urol Int. 94, 194–204 (2015).
Wei, B. et al. Association between drinking status and risk of kidney stones among United States adults: NHANES 2007–2018. BMC Public Health 24, 820 (2024).
Coyne, K. S. et al. Risk factors and comorbid conditions associated with lower urinary tract symptoms: EpiLUTS. BJU Int. 103(Suppl 3), 24–32 (2009).
Acknowledgements
The authors are indebted to the study participants.
Funding
This study was supported by unrestricted grants from the Jagiellonian University Medical College. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript. The authors’ work was independent of the funders.
Author information
Authors and Affiliations
Contributions
Conceptualization: JS MP. Formal analysis: JS MP. Funding acquisition: PC MP. Investigation: JS, MC, PD, PR, WK, PB, KK, PC, MP. Methodology: JS, MC, PD, PR, WK, PB, KK, PC, MP. Project administration: MP. Resources: MP. Supervision: MP. Validation: JS MP. Visualization: JS MP. Writing—original draft: JS MP. Writing—review and editing: JS, MC, PD, PR, WK, PB, KK, PC, MP.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval
The study was performed in compliance with Good Clinical Practice and in accordance with the Declaration of Helsinki. The Research Ethics Committee of Jagiellonian University Medical College, Krakow, Poland approved the study; in addition, the study was registered with ClinicalTrials.gov. Informed consent was provided by all participants.
Consent to participate
All participants provided informed consent.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Szymanski, J., Chlosta, M., Dudek, P. et al. Prevalence, correlates, and treatment behaviors for urolithiasis and renal colic-like pain symptoms at the population level in Poland. Sci Rep 15, 10827 (2025). https://doi.org/10.1038/s41598-025-95504-x
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-95504-x
