
Abstract
Patent foramen ovale (PFO) is the most common congenital heart abnormality of foetal origin and has been associated with cryptogenic ischemic stroke (CIS) through several mechanisms, with most theories supporting paradoxical embolism. Other possible but unknown contributing factors, such as the role of the microbiome in PFO-associated strokes, remain unclear. We analysed saliva metagenomes to study the differences in the oral microbiome between young-onset CIS patients with clinically relevant high-risk PFO (n = 52) and those without PFO (n = 52). Age- and sex-matched stroke-free controls (n = 16) with high-risk PFO were included for the comparison. Beta diversity was significantly different between patients and controls with high-risk PFO, but not between patients with and without high-risk PFO. The phylum Ascomycota and class Saccharomycetes were significantly more abundant in patients with high-risk PFO than in those without high-risk PFO. Additionally, the abundance of Lactococcus, including Lactococcus raffinolactis and L. cremoris, was higher in controls with high-risk PFO than in patients with high-risk PFO. These findings highlight that oral dysbiosis and high-risk PFO may form a critical but under-recognized combination in the aetiology of CIS. Future research should focus on elucidating the precise mechanisms of these interactions and developing targeted interventions.
Similar content being viewed by others


Introduction
Patent foramen ovale (PFO) is the most common congenital cardiac anomaly of foetal origin and is characterized by incomplete closure of the atrial septum between the right and left atria1. Approximately 25–30% of the adult population have PFO, whereas the prevalence of PFO is 40–50% in patients diagnosed with cryptogenic ischemic stroke (CIS)1,2. PFO is implicated in paradoxical embolism, where venous thrombi bypass pulmonary circulation and enter the systemic arterial system, significantly increasing the risk of cerebral ischemic events3. Current understanding supports the idea that PFOs, in particular with certain high-risk features, such as large-sized shunt and associated atrial septal aneurysm, carry the highest causality and are clinically relevant, i.e. often referred to transcatheter closure if detected after CIS4.
The incidence of ischemic stroke among young adults is rising globally5, particularly those with no apparent aetiology (cryptogenic), and poses significant clinical challenges because of its multifactorial nature and frequent indeterminate origins6. The risk factors for stroke in young adults closely mirror those observed in the general population, with predominant modifiable factors including hypertension, smoking, obesity, and diabetes mellitus7,8. However, behavioural risk factors are more common among younger individuals and several risk factors specific to young age have been identified, including pregnancy, puerperium, heavy alcohol consumption, and illicit drug use9.
Recent research has elucidated the potential impact of oral microbiome dysbiosis on various systemic conditions, such as cardiovascular and neurological outcomes and stroke10,11,12, through mechanisms involving systemic inflammation, immune modulation, and direct bacterial translocation. In our previous study, we observed that dysbiosis of the oral microbiota was associated with CIS in young adults and identified a series of oral markers, including bacterial, viral, and fungal species associated with CIS13.
Oral microbiota and their products can enter the bloodstream, potentially contributing to endothelial dysfunction, thrombosis, and atherogenesis14, which are significant factors in CIS patients. Similarly, in patients with PFO, right-to-left shunting can facilitate the direct passage of oral microbiota from venous circulation into arterial circulation15. Consequently, these microbial emboli (clusters of microbes or infected material) can travel to the brain, occluding the cerebral vessels and leading to ischemic stroke. Bacteraemia is frequent during invasive dental treatments and can also occur during routine oral hygiene practices, such as tooth brushing16, thus potentially increasing the risk of acute cardiovascular events17. Indeed, in our previous study, prior invasive dental treatment was associated with an increased risk of CIS18. Furthermore, this association was especially strong among patients with PFO.
Despite established connections between PFO and CIS19, the specific role of the oral microbiome in CIS patients with high-risk PFO remains poorly understood. To our knowledge, no study has directly investigated the relationship between oral microbiome dysbiosis and PFO-associated stroke risk. We hypothesized that (1) the oral microbiome in CIS patients with high-risk PFO differs from that in patients without PFO, and (2) the oral microbiome in CIS patients with high-risk PFO differs from that in controls with high-risk PFO. To investigate this hypothesis, we utilized high-throughput shotgun metagenomic sequencing of saliva to identify the diversity and composition of microbiota linked to high-risk PFO in young patients with CIS.
Methods
Study design
The present study, SECRETO Oral, is a substudy of the international, multicenter SECRETO study (Searching for Explanations for Cryptogenic Stroke in the Young: Revealing the Etiology, Triggers, and Outcome, NCT01934725)20. The SECRETO Oral cohort included data from 329 participants (169 cases and 160 controls) 13,18. For this study, we included CIS patients with high-risk PFO, CIS patients without PFO, and stroke-free controls with high-risk PFO, excluding participants who had used antibiotics within one-month preceding saliva sample collection, as well as those without information on antibiotic use history. Participants were recruited in this study between December 2013 and November 2019 at Helsinki University Hospital and Turku University Central Hospital.
We screened consecutive young adults aged 18–49 years with first-ever imaging-positive acute ischemic stroke, diagnosed by neurologists in the participating centres. All patients underwent brain magnetic resonance imaging (MRI), angiography of intracranial and extracranial vessels, echocardiography, and screening for coagulopathies, and laboratory testing per protocol. One sex-, age- (± 5 years), and ethnicity-matched stroke-free control for each patient from the same region was sought locally at each study centre.
CIS was then defined according to the Atherosclerosis, Small vessel disease, cardiac source, and other causes (A-S-C-O) classification21, with minor adjustments to better capture the clinical uncertainties typically observed in younger patient studies20. We included all patients with PFO to capture the full range of PFO-related stroke, as knowledge of factors that increase PFO causality has been accruing over time and the inaugural mechanism of thrombosis in PFO-associated strokes remain poorly studied. All strokes were acute, and chronic stroke was excluded. Stroke severity was evaluated using the National Institutes of Health Stroke Scale (NIHSS) score (range 0–42, with higher scores indicating greater disease severity), and was classified as: (1) 0 (no scorable symptoms on admission), (2) 1–4 (mild symptoms) (3), 5–9 (moderate), and (4) ≥ 10 (severe).
Cardiac and aortic examinations
The participants underwent transthoracic echocardiography (TTE) and transesophageal echocardiography (TEE) to assess the cardiac structure and function. The ejection fraction was calculated from the echocardiographic data. Additionally, transcranial Doppler ultrasound bubble tests (TCD-BS) were conducted to identify right-to-left shunts. The maximum volume of the interatrial and right-to-left shunts was classified as small, moderate, or severe based on the bubble count. Atherosclerosis assessments of the ascending aorta and the aortic arch were also performed.
PFO was diagnosed with colour Doppler imaging showing spontaneous right-to-left shunt or shift of shunt direction using Valsalva manoeuvre. Confirmation of PFO required a bubble study with microbubbles appearing in the left atrium during the first 3–5 cardiac cycles in TEE. In most participants, an additional TCD-BS with Valsalva manoeuvre was performed to quantify the right-to-left shunts. All available information from TTE, TEE, and TCD bubble studies were used to identify and define high-risk PFO. Clinically relevant high-risk PFO was then defined as PFO with an atrial septal aneurysm or a large-sized shunt (≥ 25 microbubbles crossing the atrial septum in TEE or detected in transcranial Doppler).
Cardiovascular risk factors and clinical oral examination
The participants underwent a thorough structured interview at the time of recruitment and a detailed clinical history was obtained from all participants using medical records. Body mass index (BMI) was determined by measuring the participants’ weight and height. Data on antibiotic use were collected from medical records. The registered cardiovascular risk factors included hypertension, abdominal obesity, current or former tobacco smoking, and heavy alcohol consumption20.
The same periodontal specialist (SP) conducted the clinical oral examinations in a standard dental office setting between April 2014 and February 2020. During the examinations, bleeding on probing (BOP) was recorded at six sites per tooth and the number of missing teeth was documented. Regular dentist check-ups were also documented. Caries lesions were diagnosed in clinical settings using the complete International Caries Detection and Assessment System (ICDAS) code. Periodontitis staging and grading were also performed18,22 and mucosal lesions and changes were recorded.
Saliva sample processing and metagenomic analysis
Details on saliva sample collection, processing, DNA extraction, and metagenomic sequencing have been previously described13,23. In brief, saliva samples were mixed with lysis buffer and subjected to repeated bead beating for DNA extraction. DNA extraction followed the protocols of the ChemagicTM 360 instrument (PerkinElmer). DNA libraries were prepared using the NEBNext® Ultra™ II FS DNA Library preparation kit. Paired-end shotgun metagenomic sequencing was conducted on an Illumina NovaSeq 6000 (San Diego, CA, USA). Subsequent preprocessing of sequence data was performed using FastQC (v. 0.11.9), MultiQC (v. 1.9), and Trimmomatic (v. 0.39). Host-associated reads were removed using Kneaddata with the human genome (GRCh38.p14). Taxonomy profiling was performed using Kraken2 (v. 2.1.2)24. Bracken (v. 2.7) was used to refine the estimates of species-level abundance25.
Statistical analysis
Statistical analyses were performed using IBM SPSS Statistics (version 29.0.2.0, IBM Corp.). The analyses included Mann–Whitney U test, Kruskal–Wallis test, and independent samples t-test, depending on the data type. All microbiome analyses were performed in R (v. 4.3.1). The sequence data, along with the metadata, were stored in specialized data containers designed for microbiome research in R, namely Phyloseq (v. 1.44.0) and TreeSummarized Experiment (v. 2.10.0) for further analysis. Before analysis, we removed sequences with fewer than 100 reads. We also excluded taxa present in < 10% of the samples. For analysis, taxonomic read counts were normalized to relative abundances and transformed using a centered log-ratio (CLR) method for downstream statistical analyses.
Alpha diversity was estimated using the Shannon and Inverse Simpson indices. Differences in community composition (beta diversity) were determined by permutational multivariate ANOVA (PERMANOVA) using the vegan package (v. 2.6.4)26 with the adonis2 function. Principal Coordinate Analysis (PCoA) was performed based on both Bray–Curtis dissimilarity and Jaccard distance to visualize the microbiome structure. We used the DESeq2 (v1.38.2) to identify differentially abundant microbiome features between the groups27. P-values were corrected for multiple testing using the Benjamini–Hochberg procedure, with a significance threshold set at q ≤ 0.05.
Results
Clinical characteristics
A total of 120 participants (52 patients with high-risk PFO, 52 patients without PFO, and 16 controls with high-risk PFO) were included in this study. Mean age (SD) of participants was 40.6 (8.1) years.
The clinical characteristics of the patients with and without high-risk PFO are summarized in Table 1. The difference in sex distribution between the two groups was not statistically significant (p = 0.158). Patients with high-risk PFO had a significantly higher mean age (41.01 ± 6.5 years) than patients without PFO (36.98 ± 9.2 years) (p = 0.040). Heavy alcohol use was reported by 13.5% of patients with high-risk PFO and 42.3% patients without high-risk PFO (p = 0.001). Additionally, 13.5% of the patients used antibiotics in the preceding 3 months (17.3% of patients with high-risk PFO and 9.6% of patients without high-risk PFO, p = 0.253). Dentine caries lesions were present in 48.1% of the patients (p = 0.118), periodontitis in 26.9% (p = 0.206), and mucosal lesions in 19.2% (p = 0.150). None of these conditions showed a significant difference between patients with and without high-risk PFO. However, a significantly higher proportion of patients without PFO had hypertension (32.7%) than those with high-risk PFO (3.8%) (p < 0.001). The distribution of stroke severity showed no significant difference between patients with high-risk PFO and those without PFO (p = 0.413, Table 1).
There was no significant difference in ejection fraction between patients with high-risk PFO and those without PFO (p = 0.315). Atrial septal aneurysm was found in 11.5% of patients with high-risk PFO; none was found in patients without PFO (p = 0.011) (Table 2).
Oral microbiome composition
Individual oral microbiome diversity and composition were characterized by metagenomic sequencing of saliva samples. We focused on microbial taxa whose relative abundance exceeded 0.001% (detection) in at least 10% (prevalence) of the samples, which yielded 26 phyla, 53 classes, 115 orders, 243 families, 721 genera, and 2374 species. A taxonomic tree was constructed for the 10 most abundant phyla to illustrate the composition and abundance of the taxonomy (Fig. 1a). Oral microbiota was dominated by the phyla Bacillota, Actinomycetota, Bacteroidota, Pseudomonadota, and Fusobacteriota (Fig. 1b). At the genus level, the most abundant genera in the samples were Prevotella, Streptococcus, Neisseria, Veillonella, Schaalia and Haemophilus (Fig. 1c).

Composition and taxonomic distribution of the oral microbiome. (a) Taxonomic tree of the oral microbiome showing the prevalence of top 10 phyla as determined by mean abundance. (b) Stacked bars of relative abundances of the five most abundant phyla for all samples, shown in descending order of total abundance. (c) Stacked bars of relative abundances of the 10 most abundant genera for all samples, displayed in descending order of total abundance. Genera not included in the top 10 are grouped into the category ‘Others’.
Microbiome diversity and composition in CIS patients with and without high-risk PFO
Alpha and beta diversities in each sample were compared between patients with high-risk PFO and without PFO to evaluate the characteristics of the oral microbiota associated with CIS. There was no significant difference in alpha diversity between the two groups (Shannon index, p = 0.642; Inverse Simpson index, p = 0.460) (Fig. 2a,b, and Table S1). No significant differences were found in the microbial composition (beta diversity) between patients with high-risk PFO and without PFO groups (R2 = 0.007, F = 0.727, p = 0.693, Table S2). To further illustrate the microbial composition, PCoA was used to examine the extent of similarity of the oral microbial communities based on Bray–Curtis dissimilarity (Fig. 2c) and Jaccard distance (Fig. 2d).

Oral microbiome diversity in CIS patients with and without high-risk PFO. Alpha diversity measurements using the (a) Shannon and (b) Inverse Simpson index between CIS patients with high-risk PFO and without PFO. PCoA plot of beta diversity of the oral microbiome based on (c) Bray–Curtis dissimilarity and (d) Jaccard distance between CIS patients with high-risk PFO and without PFO.
To visualize differences in oral microbiome composition between patients with and without high-risk PFO, bar plots displaying the relative abundance of taxa at the phylum and genus levels are shown (Fig. 3). At the phylum level, Bacillota, Actinomycetota, and Fusobacteriota were more abundant (Fig. 4a), whereas Bacteroidota and Pseudomonadota were less abundant in CIS patients with high-risk PFO than in those without PFO (Fig. 4b); however, these differences were not statistically significant. At the phylum level, only Ascomycota was positively associated with CIS patients with high-risk PFO (adjusted for age, hypertension, and heavy alcohol use; q = 0.039). At the class level, Saccharomycetes was significantly more abundant in high-risk PFO patients (q = 0.047) (Fig. 4c, Table S3). None of the genera or species were statistically significant in the adjusted model.

Relative abundance of oral microbiome in CIS patients with high-risk PFO and without PFO. Stacked bar chart illustrating the mean relative abundance of microbial taxa at the (a) phylum and (b) genus levels in CIS patients with high-risk PFO and without PFO.

Taxonomic composition of the oral microbiome in CIS patients with and without high-risk PFO. Boxplots showing the abundance of the top phyla that were (a) higher and (b) lower in CIS patients with high-risk PFO than in those without PFO. (c) Taxa significantly different between CIS patients with high-risk PFO and those without PFO.
Microbiome diversity and composition in CIS patients and controls with high-risk PFO
We next compared the differences in the oral microbiome between CIS patients with high-risk PFO (n = 52) and stroke-free controls with high-risk PFO (n = 16). Clinical characteristics of both groups are shown in Table S4. There were no significant differences in gender distribution, age, BMI, smoking history, heavy alcohol use, abdominal obesity, dentine caries lesions, periodontitis, mucosal lesions, or regular dentist check-ups between patients and controls. A total of 17.3% of patients and no controls used antibiotics in the past 3 months; this was not statistically significant (p = 0.076). However, there was a significant difference in hypertension; 25% of controls and 3.8% of patients had hypertension (p = 0.010, Table S4). No major differences were observed in cardiac and aortic examinations between patients and controls (Table S5). The average ejection fraction was similar between patients and controls (patients: 64.6 ± 7.6%, controls: 65.5 ± 7.5%, p = 0.214). Atherosclerosis in the ascending aorta and aortic arch was predominantly absent in both groups, with no significant differences (Table S5).
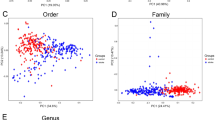
There was no significant difference in alpha diversity between patients and controls with high-risk PFO (Shannon index, p = 0.197; Inverse Simpson index, p = 0.196) (Fig. 5a,b, and Table S6). Beta diversity analysis revealed a significant difference in microbiome composition between patients and controls with high-risk PFO (R2 = 0.031, F = 2.108, p = 0.032, Fig. 5c,d, Table S7). Bar plots showing the relative abundance of major taxa at the phylum and genus levels revealed differences in oral microbiome composition between patients and controls with high-risk PFO (Fig. 6). We found six taxa (two phyla, one order, one genus, and two species) that were significantly different between the patients and controls with high-risk PFO in the adjusted model (adjusted for hypertension). At the phylum level, Bacteroidota and Synergistota were higher in patients. Similarly, the order Desulfobacterales (members of the Pseudomonadota phylum) was significantly more abundant in patients. Conversely, the genus Lactococcus and species Lactococcus raffinolactis and Lactococcus cremoris were less abundant in patients than in controls (q < 0.05) (Fig. 7, Table S8).

Oral microbiome diversity in CIS patients and controls with high-risk PFO. Alpha diversity measurements using the (a) Shannon and (b) Inverse Simpson index between CIS patients and controls with high-risk PFO. PCoA plot of beta diversity of the oral microbiome based on (c) Bray–Curtis dissimilarity and (d) Jaccard distance between CIS patients and controls with high-risk PFO.

Relative abundance of phyla and genera in the oral microbiome in CIS patients and controls with high-risk PFO. Stacked bar chart illustrating the mean relative abundance of major microbial taxa at the (a) phylum and (b) genus levels in CIS patients with high-risk PFO and controls with high-risk PFO.

Taxonomic composition of the oral microbiome in CIS patients and controls with high-risk PFO. Boxplots showing the microbial taxa that exhibit significant differences between patients and controls with high-risk PFO.
Discussion
In this study, we compared the oral microbiome in young-onset CIS patients with high-risk PFO to that of (1) young-onset CIS patients without PFO and (2) controls with high-risk PFO to investigate the relationship between oral microbiome dysbiosis and high-risk PFO. Our findings revealed that although no significant differences were observed in alpha or beta diversity between CIS patients with and without high-risk PFO, notable differences were found at various taxonomic levels. Our findings showed that Ascomycota was the major phylum associated with CIS patients with high-risk PFO. We identified six taxa that exhibited differential abundance between patients and controls with high-risk PFO, highlighting the significant interplay between oral microbiome composition and CIS. To the best of our knowledge, this is the first study to examine the oral microbiota and PFO in patients with CIS.
The relationship between PFO and CIS has been previously debated28, and knowledge of causality has increased only relatively recently after the completion of randomized clinical trials4. Larger PFOs are linked to an increased risk of stroke, especially when a large shunt or an atrial septal aneurysm is present4. The traditional mechanism connecting PFO to CIS involves paradoxical embolism, where venous blood clot bypasses pulmonary filtration and enters cerebral circulation29. Poor oral health, particularly periodontal disease, can lead to bacteremia, in which bacteria enter the bloodstream, increasing inflammation and the risk of clot formation. Recent surgery or use of oral contraceptives (or both), which are known to increase blood hypercoagulability, contribute to the risk of ischemic stroke30. Our previous findings suggest that this risk is particularly pronounced in individuals with a PFO, as evidenced by a strong association between CIS and invasive dental treatments in this population18.
The present study found that the abundances of the phyla Ascomycota and class Saccharomycetes were significantly higher in patients with high-risk PFO than without PFO. Similarly, the abundances of the phyla Bacteroidota and Synergistota were significantly higher in CIS patients than in the control group. Dysbiosis of the oral microbiota, especially increased proportions of Gram-negative species31, may contribute to an increased risk of thrombus formation, particularly in the venous system, potentially influencing the development of high-risk PFOs and subsequent thromboembolic events. Furthermore, they support the paradoxical embolism mechanism, indicating that oral microbial dysbiosis may directly contribute to PFO-related CIS through bacteraemia. This effect is further influenced by chronic inflammatory conditions, such as periodontitis, which can independently increase stroke risk by promoting systemic inflammation and bacteraemia32,33. However, it is important to note that our study lacked direct biomarker evidence for thrombus formation, coagulation, or inflammation to conclusively support this hypothesis. Future studies incorporating these biomarkers should provide stronger insights into the relationship between oral dysbiosis, thrombus formation, and CIS risk.
Recent studies have highlighted the putative importance of the oral fungal microbiome (mycobiome) in oral and systemic health. Oral mycobiome comprises an estimated 100 species34 but their association with stroke is seldom studied. In this study, we observed that Ascomycota (phylum) and Saccharomycetes (class) were the two taxa associating positively with high-risk PFO in patients. Ascomycota is the largest and most species-rich phylum in the fungal kingdom and is the predominant phylum in the oral cavity35. Some genera in the phylum such as Aspergillus and Candida, which include several pathogenic species, are associated with stroke36. To our knowledge, these fungal taxa have not been previously reported in high-risk PFO-related CIS, and their mechanisms affecting PFO-related CIS and patient prognosis remain unclear, warranting further investigations.
In this study, we observed that at the phylum level, Bacteroidota and Synergistota were higher in patients than controls. Bacteroidota, one of the most prominent and abundant phylum of Gram-negative bacteria and predominant in the oral cavity, has been linked to immune dysregulation and systemic diseases through mechanisms such as glycoprotein secretion, short-chain fatty acid imbalance, and toxin production37. A previous animal study found that stroke induces gut microbiota dysbiosis, characterized by reduced species diversity and Bacteroidota overgrowth38. Phylum Synergistota comprises anaerobic bacteria with Gram-negative staining39. Synergistota is also higher in the oral cavity of patients with periodontitis40,41, suggesting that this phylum is disease-associated.
Compared with patients, controls in our study were enriched in the genus Lactococcus, including L. raffinolactis and L. cremoris. The genus Lactococcus was first proposed by Schleifer et al42 in 1985 and comprises Gram-positive, facultative anaerobic lactic acid bacteria (LAB) that ferment lactose to produce lactic acid. Lactococcus spp. play a significant role in oral health43. A recent study on oral microbiota showed that the abundance of LAB, including Lactococcus, was lower in the saliva of oral lichen planus cases and negatively correlated with disease severity44. L. raffinolactis, formerly known as Streptococcus raffinolactis, is a LAB capable of metabolizing vitamin B3 and fermenting α-galactosides, such as melibiose and raffinose45. L. cremoris is another important species within the Lactococcus genus, widely recognized for its significant role in the dairy industry46. However, its potential health benefits in the oral cavity and role in major oral and systemic diseases remain unclear. Studies have highlighted that certain species within the Lactococcus genus, including L. lactis, exhibit a range of beneficial properties, such as antimicrobial, anti-halitosis, anti-inflammatory, and inhibitory activities against periodontopathogens47. Additionally, L. lactis can adhere to dental surfaces and inhibit the growth of cariogenic bacteria such as Streptococcus mutans48. We are unaware of the exact mechanism and significance of dysbiosis in each microbial taxa, but our study findings can be used in basic research on the oral-gut-brain interaction.
Although this study provides valuable insights, there are certain limitations to consider. The present findings support that these identified microbes are associated with CIS patients who have high-risk PFO. However, it remains unclear whether these changes are a key cause of CIS related to high-risk PFO, as the cross-sectional design limits the ability to infer causation between oral microbiome dysbiosis and stroke risk. Additionally, the relatively small sample size may limit the generalizability of our findings. Saliva samples in this study were collected only once. Given that variations in the oral microbiome may occur in the period following a stroke, future research should examine microbiome changes at multiple intervals after stroke to gain a more detailed understanding of their relationship with cerebrovascular health. To better understand the dynamic changes in oral microbiota abundance, multiple saliva samples should be collected during treatment, which may help assess the potential of oral microbiota as a therapeutic target for high-risk PFO-related CIS.
Conclusion
Our study revealed a novel association between oral microbiome dysbiosis and high-risk PFO in patients with CIS. We found changes in the oral microbial composition among CIS patients with and without high-risk PFO and when compared with controls, suggesting that these alterations may contribute to CIS risk through mechanisms such as paradoxical embolism associated with initial venous thrombosis, systemic inflammation, and bacteraemia. While these findings are promising, further research is needed to explore how oral microbiome changes affect stroke risk over time and to evaluate targeted preventive interventions.
Data availability
Sequence data that support the findings of this study have been deposited in the European Genome-Phenome Archive (accession no: EGAS00001007505).
References
Homma, S. et al. Patent foramen ovale. Nat. Rev. Dis. Primers 2, 15086 (2016).
Mojadidi, M. K. et al. Cryptogenic stroke and patent foramen ovale. J. Am. Coll. Cardiol. 71, 1035–1043 (2018).
Lee, P. H. et al. Cryptogenic stroke and high-risk patent foramen ovale: The DEFENSE-PFO trial. J. Am. Coll. Cardiol. 71, 2335–2342 (2018).
Kent, D. M. et al. Heterogeneity of treatment effects in an analysis of pooled individual patient data from randomized trials of device closure of patent foramen ovale after stroke. JAMA 326, 2277–2286 (2021).
Boot, E. et al. Ischaemic stroke in young adults: a global perspective. J. Neurol. Neurosurg. Psychiatry 91, 411–417 (2020).
Bukhari, S., Yaghi, S. & Bashir, Z. Stroke in young adults. J. Clin. Med. 12, 4999 (2023).
Boehme, A. K., Esenwa, C. & Elkind, M. S. Stroke risk factors, genetics, and prevention. Circ. Res. 120, 472–495 (2017).
George, M. G. Risk factors for ischemic stroke in younger adults: A focused update. Stroke 51, 729–735 (2020).
Putaala, J. Ischemic stroke in young adults. Continuum (Minneap Minn) 26, 386–414 (2020).
Shoemark, D. K. & Allen, S. J. The microbiome and disease: reviewing the links between the oral microbiome, aging, and Alzheimer’s disease. J. Alzheimer’s Dis. 43, 725–738 (2015).
Tonelli, A., Lumngwena, E. N. & Ntusi, N. A. The oral microbiome in the pathophysiology of cardiovascular disease. Nat. Rev. Cardiol. 20, 386–403 (2023).
Sun, W. et al. The oral microbiome of patients with ischemic stroke predicts their severity and prognosis. Front Immunol. 14, 1171898 (2023).
Manzoor, M. et al. Multikingdom oral microbiome interactions in early-onset cryptogenic ischemic stroke. ISME Commun. 4, ycae088 (2024).
Peng, X. et al. Oral microbiota in human systematic diseases. Int. J. Oral Sci. 14, 14 (2022).
Li, Y. et al. The oral microbiota and cardiometabolic health: A comprehensive review and emerging insights. Front. Immunol. 13, 1010368 (2022).
Lockhart, P. B. et al. Bacteremia associated with toothbrushing and dental extraction. Circulation 117, 3118–3125 (2008).
Elkind, M. S. V., Boehme, A. K., Smith, C. J., Meisel, A. & Buckwalter, M. S. Infection as a stroke risk factor and determinant of outcome after stroke. Stroke 51, 3156–3168 (2020).
Leskelä, J. et al. Periodontitis, dental procedures, and young-onset cryptogenic stroke. J. Dent. Res. 103, 494–501 (2024).
Lucà, F. et al. Patent foramen ovale and cryptogenic stroke: Integrated management. J. Clin. Med. 12, 1952 (2023).
Putaala, J. et al. Searching for explanations for cryptogenic stroke in the young: Revealing the triggers, causes, and outcome (SECRETO): Rationale and design. Eur. Stroke J. 2, 116–125 (2017).
Amarenco, P., Bogousslavsky, J., Caplan, L. R., Donnan, G. A. & Hennerici, M. G. New approach to stroke subtyping: The A-S-C-O (phenotypic) classification of stroke. Cerebrovasc. Dis. 27, 502–508 (2009).
Tonetti, M. S., Greenwell, H. & Kornman, K. S. Staging and grading of periodontitis: Framework and proposal of a new classification and case definition. J. Periodontol. 89, 159–172 (2018).
Manzoor, M. et al. Shotgun metagenomic analysis of the oral microbiome in gingivitis: A nested case-control study. J. Oral. Microbiol. 16, 2330867 (2024).
Wood, D. E., Lu, J. & Langmead, B. Improved metagenomic analysis with Kraken 2. Genome Biol. 20, 257 (2019).
Lu, J., Breitwieser, F. P., Thielen, P. & Salzberg, S. L. Bracken: Estimating species abundance in metagenomics data. PeerJ Comput. Sci. 3, e104 (2017).
Oksanen, J. et al. Package “vegan”. A community ecology package. Commun. Ecol. Packag. 2, 1–295 (2013).
Love, M. I., Huber, W. & Anders, S. Moderated estimation of fold change and dispersion for RNA-seq data with DESeq2. Genome Biol. 15, 550 (2014).
Di Tullio, M. R., Sacco, R. L., Sciacca, R. R., Jin, Z. & Homma, S. Patent foramen ovale and the risk of ischemic stroke in a multiethnic population. J. Am. Coll. Cardiol. 49, 797–802 (2007).
Pristipino, C. et al. European position paper on the management of patients with patent foramen ovale. General approach and left circulation thromboembolism. Eur. Heart. J. 40, 3182–3195 (2019).
Roach, R. E. et al. Combined oral contraceptives: the risk of myocardial infarction and ischemic stroke. Cochrane Database Syst. Rev. 8, CD011054 (2015).
Leskelä, J. et al. Genetic profile of endotoxemia reveals an association with thromboembolism and stroke. J. Am. Heart Assoc. 10, e022482 (2021).
Pussinen, P. J. et al. Antibodies to periodontal pathogens and stroke risk. Stroke 35, 2020–2023 (2004).
Lee, Y. T. et al. Periodontitis is a potential risk factor for transient ischemic attack and minor ischemic stroke in young adults: A nationwide population-based cohort study. J. Periodontol. 93, 1848 (2022).
Ghannoum, M. A. et al. Characterization of the oral fungal microbiome (mycobiome) in healthy individuals. PLoS Pathog. 6, e1000713 (2010).
Peters, B. A., Wu, J. & Hayes, R. B. The oral fungal mycobiome: Characteristics and relation to periodontitis in a pilot study. BMC Microbiol. 17, 157 (2017).
Hier, D. B. & Caplan, L. R. Stroke due to fungal infections. In Uncommon Causes of Stroke (eds Caplan, L. R. & Bogousslavsky, J.) 47–52 (Cambridge University Press, 2008).
Gibiino, G. et al. Exploring bacteroidetes: Metabolic key points and immunological tricks of our gut commensals. Dig. Liver Dis. 50, 635–639 (2018).
Singh, V. et al. Microbiota dysbiosis controls the neuroinflammatory response after stroke. J. Neurosci. 36, 7428–7440 (2016).
Hugenholtz, P., Hooper, S. D. & Kyrpides, N. C. Focus: Synergistetes. Environ. Microbiol. 11, 1327–1329 (2009).
Griffen, A. L. et al. Distinct and complex bacterial profiles in human periodontitis and health revealed by 16S pyrosequencing. ISME J. 6, 1176–1185 (2012).
Shi, M. et al. Alterations and correlations in microbial community and metabolome characteristics in generalized aggressive periodontitis. Front. Microbiol. 11, 573196 (2020).
Schleifer, K. H. et al. Transfer of Streptococcus lactis and related streptococci to the genus Lactococcus gen. nov. Syst. Appl. Microbiol. 6, 183–195 (1985).
Seminario-Amez, M., López-López, J., Estrugo-Devesa, A., Ayuso-Montero, R. & Jané-Salas, E. Probiotics and oral health: A systematic review. Med. Oral Patol. Oral Cir. Bucal. 22, e282–e288 (2017).
Ren, X., Li, D., Zhou, M., Hua, H. & Li, C. Potential role of salivary lactic acid bacteria in pathogenesis of oral lichen planus. BMC Microbiol. 24, 197 (2024).
Boucher, I., Vadeboncoeur, C. & Moineau, S. Characterization of genes involved in the metabolism of alpha-galactosides by Lactococcus raffinolactis. Appl. Environ. Microbiol. 69, 4049–4056 (2003).
Li, T. T., Tian, W. L. & Gu, C. T. Elevation of Lactococcus lactis subsp cremoris to the species level as Lactococcus cremoris sp. nov. and transfer of Lactococcus lactis subsp. tructae to Lactococcus cremoris as Lactococcus cremoris subsp. tructae comb. nov. Int J Syst Evol Microbiol. 71, 004727 (2019).
Shin, H. S., Baek, D. H. & Lee, S. H. Inhibitory effect of Lactococcus lactis on the bioactivity of periodontopathogens. J. Gen. Appl. Microbiol. 64, 55–61 (2018).
Tong, Z. et al. An in vitro investigation of Lactococcus lactis antagonizing cariogenic bacterium Streptococcus mutans. Arch. Oral. Biol. 57, 376–382 (2012).
Acknowledgements
We would like to thank the Biomedicum Functional Genomics Unit (FuGU) for their assistance with metagenomic sequencing. This work was supported by the Academy of Finland grants (316777 and 355532 for SP; 340750 for PJP; 286246, 318075, 322656 for JP), the Finnish Dental Society Apollonia (for PJP), and the Sigrid Jusélius Foundation (for PJP), the Finnish Medical Foundation (for JP), the Helsinki and Uusimaa Hospital District (TYH2014407, TYH2018318 for JP), and the Minerva Foundation Selma and Maja-Lisa Selander’s Fund (for MM). Open access funded by Helsinki University Library. The funders had no role in the design or execution of the study; the collection, management, analysis, or interpretation of data; the preparation, review, or approval of the manuscript; or the decision to submit the manuscript for publication.
Author information
Authors and Affiliations
Contributions
Conceptualization: MM, JL, EK, JS, JP, PJP, SP; Supervision: PJP, SP, JP; Funding acquisition: MM, JP, PJP, SP; Project administration: EK, JS, JP, PJP, SP; Performed the clinical work: JL, NMM, EK, JS, JP, SP; Performed the laboratory work: MM, JL, MP; Data analysis and interpretation: MM, JL, JP, PJP, SP; Writing – original draft preparation: MM, PJP, SP; Writing – review and editing: MM, JL, MP, NMM, EK, JS, JP, PJP, SP. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics, consent, and permissions
This study was approved by the Ethics Committee of the Hospital District of Helsinki and Uusimaa. All participating centres obtained approvals from the responsible local Ethics Committees. The study was performed in accordance with Good Clinical Practice and the Declaration of Helsinki. Written informed consent was obtained from all participants.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Manzoor, M., Leskelä, J., Pietiäinen, M. et al. Oral microbiome dysbiosis in cryptogenic ischemic stroke patients with high-risk patent foramen ovale. Sci Rep 15, 11535 (2025). https://doi.org/10.1038/s41598-025-95728-x
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-95728-x
Keywords
This article is cited by
-
Gut Microbiota Improve the Prediction of Stroke-Associated Pneumonia Risk and Outcomes in Acute Ischemic Stroke
Translational Stroke Research (2025)
