
Abstract
Infective endocarditis (IE) is a serious condition with high morbidity and mortality. This retrospective cohort study evaluated the evolution of clinical characteristics, microbiological profiles, and treatment outcomes in 435 Thai IE patients, spanning three distinct periods, at a Chiang Mai tertiary-care hospital. Patients were categorized into three timeframes: 1998–2001 (n = 134), 2012–2015 (n = 117), and 2016–2020 (n = 184). The median patient age significantly increased from 42 years (IQR 34–51) to 58 years (IQR 44–65) (p = 0.003). The study also identified an increased prevalence of co-morbidities in recent years. Notably, there was a marked decrease in the prevalence of rheumatic heart disease, from 23.1 to 10.9% (p = 0.009). Streptococcus suis is a unique and increasingly prevalent cause of IE in northern Thailand. Additionally, the rate of culture-negative IE declined from 38.1 to 23.9% (p = 0.018). Surgical interventions increased from 52.2 to 64.1% (p = 0.072), while the median time to surgery remained constant at 12 days. Despite advancements in diagnosis and treatment, the length of hospitalization remained stable throughout the study periods, and the in-hospital mortality rate consistently stayed at 18.6%. This study highlights significant shifts in the epidemiology and management of IE, indicating persistent challenges in reducing mortality despite improved care.
Similar content being viewed by others

Introduction
In 2019, there were an estimated 13.8 cases of infective endocarditis (IE) per 100,000 individuals annually, resulting in approximately 66,300 deaths worldwide1. Initiating antibiotic therapy and performing timely surgery in indicated patients are crucial to preventing significant complications such as heart failure, stroke, systemic embolization, and sepsis/septic shock2. Diagnosing IE presents a challenge due to its various clinical manifestations3. The modified Duke criteria, including clinical, microbiological, and imaging evidence, offer about 80% sensitivity and specificity in diagnosing IE4. The diagnosis of IE relies on clinical suspicion, reinforced by microbiological evidence and the identification of IE-related cardiac lesions through imaging techniques, with transthoracic echocardiography being the most commonly utilized worldwide5.
Over the last two decades, the incidence of IE in Europe has doubled, with nationwide registries confirming this rise6,7. The epidemiology of IE varies across continents, geographic regions, and types of hospitals8. The majority of available data on IE comes from non-Asian populations, with limited information specific to Asian patients. Data on clinical trends, pathogens, echocardiogram findings, and mortality outcomes in the Asian population remain sparse9,10.
Previous studies on the clinical characteristics of IE in Thai patients have typically spanned three to ten years11,12,13. The objective of this study was to analyze the changes in clinical characteristics, echocardiography findings, microbial etiology, mortality rates, and outcomes of patients diagnosed with IE over a span of two decades in Thai patients.
Methods
Study design and population
This retrospective cohort study investigated patients diagnosed with IE from a tertiary-care hospital in Chiang Mai, Thailand, spanning three distinct periods: 1998–2001, 2012–2015, and 2016–2020. The 2001–2011 period was omitted due to incomplete medical records.
This study was approved by the Institutional Research Ethics Committee of the Faculty of Medicine at Chiang Mai University. It received approval under exemption number 0392/2024, which waives the requirement for informed consent due to the retrospective nature of the research and was conducted in accordance with the Declaration of Helsinki 2013. The study was registered in thaiclinicaltrials.org, identification number TCTR20240726001.
All patients diagnosed with IE according to ICD-10 and aged 18 years or older were initially identified using diagnosis codes. To ensure diagnostic accuracy, all cases were subsequently reviewed based on the modified Duke criteria. Only cases meeting the criteria for definite IE were included in the study. Between 2016 and 2020, a total of 211 patients had diagnostic codes for IE. Of these, 184 patients (87.2%) were diagnosed with definite IE based on the modified Duke criteria. The remaining 27 patients, diagnosed with possible or probable IE, were excluded from the study. However, we were unable to identify a complete set of records using diagnostic codes from earlier time periods (1998–2001 and 2012–2015), due to the use of paper records. We only have information indicating that 134 patients were diagnosed with definite IE during 1998–2001, and 117 patients during 2012–2015.
Baseline characteristics, such as age, sex, underlying diseases, predisposing conditions, clinical presentation, and physical examination findings were collected for analysis. Echocardiography findings, such as the site of valvular involvement and severity of valvular destruction, along with microbial etiology, surgical intervention rate, time to surgery, length of stay, and in-hospital mortality rates, were recorded for analysis.
We also examined the predictors of in-hospital in our studied population. We chose to analyze mortality risk in the most recent period because it best reflects contemporary clinical practice. Given that management strategies have evolved significantly over time, analyzing mortality risk across all periods could introduce confounding factors that may not accurately represent current outcomes.
Statistical analysis
The continuous data were expressed as medians with interquartile ranges (IQR), while categorical data were presented as frequencies and percentages. To compare continuous variables among the three groups, analysis of variance was employed. For categorical variables, a chi-square test was used to compare between the three groups. Post hoc pairwise comparisons were conducted to identify specific differences between groups, with Bonferroni correction applied to adjust for multiple testing and control the risk of Type I error. The multivariable model was constructed using logistic regression, with covariates selected based on clinical relevance and statistical significance from univariate analyses. To check for collinearity, we used variance inflation factors, and variables with high collinearity were either excluded or combined. Statistical significance was determined with a threshold of p-values less than 0.05. All statistical analyses were conducted using STATA program version 16 (Stata Corp. 2019, Stata Statistical Software: Release 16, Stata Corp. LLC, College Station, TX, USA).
Results
Our study comprised a total of 435 patients, with 134 included during the period 1998–2001, 117 during 2012–2015, and 184 during 2016–2020, respectively. Table 1 presents the baseline characteristics of patients with IE in Thai population. The median age of individuals in the overall population was 51 years (IQR 39, 62). Notably, there was a significant increase in the median age from 42 years (IQR 34, 51) to 58 years (IQR 44, 65) over two decades (p = 0.003). The majority of patients with IE were male (66.2%). There was a non-significant trend in the increasing proportion of females over time.
Over 20 years, there has been a significant decrease in the prevalence of rheumatic heart disease in patients with IE, dropping from 23.1 to 10.9% (p = 0.009). Conversely, congenital heart disease, encompassing both cyanotic conditions like tetralogy of Fallot and non-cyanotic conditions such as atrial septal defect, small ventricular septal defect, and patent ductus arteriosus showed an increasing trend from 7.5 to 14.7% (p = 0.105), though this was not statistically significant. The temporal trend among IE patients showed a decrease in other valvular heart diseases, including myxomatous mitral valve, degenerative aortic stenosis, mitral valve prolapses, and mitral annular calcification from 36.6 to 11.4% (p = 0.003). Furthermore, the diagnosis of prosthetic valve IE tended to increase from 6.0 to 13.0% (p = 0.192). The previous history of IE was reported in 7.8% in the overall population, with no significant change observed across the two decades.
Along with the increasing age of patients with IE, there has been a significant rise in the prevalence of co-morbidities, including hypertension, diabetes, chronic kidney disease, and cerebrovascular disease. In contrast, the prevalence of people living with HIV (PLWH) has significantly declined from 6.0 to 1.1% (p = 0.021). Similarly, the proportion of patients with intravenous drug use has reduced from 9.7 to 2.2% (p = 0.006).
The onset of symptoms has been decreasing from 30 days to 14 days (p = 0.024). The most frequent presentation among our patients was a history of fever, reported in 83.9%, followed by dyspnea described in 60.2%, and it remained unchanged across the three periods. Arthralgia/arthritis has manifested more frequently in IE patients, increasing from 7.5 to 20.1% (p = 0.006) across two decades.
The most common clinical finding in IE patients was an abnormal cardiac murmur, reported in 92.5%, followed by fever, present in 76.3%, and both remained consistent across the three studied periods. Classic features of IE, including Osler’s nodes, Janeway lesions, and splinter hemorrhages, were present in 6.9%, unchanged overtime. Clubbing of the fingers was reported only in 3.9%. Abnormal urine sediments were observed in 31.3% of the overall population, and this prevalence remained comparable across the different studied periods.
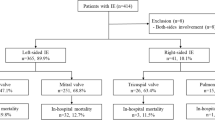
The echocardiographic findings are presented in Table 2. The prevalence of IE at the aortic valve has witnessed a significant decrease from 50.7 to 33.2% (p = 0.006), while there has been a concurrent rise in the prevalence of IE at the mitral valve, increasing from 23.1 to 38.1% (p = 0.018) over the study period. There is a trend showing a decrease in the prevalence of tricuspid valve involvement in IE, although it is not statistically significant (11.2 to 6.5%, p = 0.429). The severity of valvular destruction leading to valvular regurgitation was categorized into mild, moderate, severe, and very severe, which encompasses the perforation of valve leaflets.
Table 3 illustrates the epidemiology of the causative pathogens among patients diagnosed with IE. The predominant pathogen identified was streptococci, observed in 44.8%, followed by staphylococci reported in 17.5%, and enterococci documented in 5.3% in the overall population. The prevalence of staphylococcal and enterococcal IE increased non-significantly over two decades, while streptococcal IE prevalence remained unchanged. Remarkably, the frequency of culture-negative IE progressively decreased from 38.1 to 30.8% and 23.9% across three distinct periods (p = 0.018). Among streptococcal IE, the viridans group streptococci were identified as the causative pathogen less frequently, decreasing from 24.6 to 15.8%. Interestingly, Streptococcus suis IE was documented more frequently, increasing from 4.5 to 13.0% (p = 0.042). Streptococcus agalactiae IE and Streptococcus bovis IE were not detected during the first studied period but emerged as pathogens, being observed more frequently during the subsequent two periods.
During the period from 2016 to 2020, tissue samples were collected for 16 S rRNA detection in cases of culture-negative IE. Out of 20 cases tested, 18 cases tested positive for 16 S rRNA detection, representing a positivity rate of 90%. Six cases were identified as Streptococcus suis, five as Bartonella henselae, three as Streptococcus agalactiae, two as the viridans group streptococci, and one each as Streptococcus pneumoniae and Streptobacillus spp.
Table 4 presents the outcomes of patients with IE. There was an observed increasing trend in surgical treatment, rising from 52.2% during the period of 1998–2001 to 64.1% during 2016–2020 (p = 0.072). However, the median time from diagnosis to surgery remained at 12 (IQR 6, 27) days throughout the study period. The median study length stayed consistent at 24 (IQR 14, 40 days) days, and the overall mortality rate was 18.6%, with no significant differences observed across the different time periods.
We examined the predictors of in-hospital morality in IE patients during the most recent periods (2016–2020), as it reflects contemporary clinical practice. Our analysis demonstrated that the presentation with hypotension and the presence of severe valvular dysfunction or perforation were independently associated with the increased risk of in-hospital morality. Conversely, undergoing surgery remained a protective factor against mortality (Table 5).
Discussion
In our study, we identified a temporal trend showing a gradual increase in the average age of the population from 1998 to 2020. Specifically, the median age of patients diagnosed with IE exhibited a noteworthy shift from 42 years to 58 years over a 20-year period. This observed aging trend coincided with a concurrent rise in the detection of comorbid diseases, including diabetes, hypertension, cerebrovascular disease, and chronic kidney disease. We have illustrated a notable reduction in the prevalence of rheumatic heart disease among IE patients in our studied population, aligning with the observed decline in global incidence14. This decline may offer an explanation for the observed trend of increasing age in our population, as rheumatic heart disease was more commonly observed in younger patients. The decline in degenerative valve disorders despite increasing patient age may reflect evolving diagnostic practices, shifting risk profiles with more healthcare-associated IE, and improved cardiovascular care leading to earlier detection and management. Furthermore, in our study, a decreasing trend was noted in PLWH and a history of intravenous drug use. These factors, typically more prevalent in younger patients, further contribute to the overall shift towards an aging demographic observed in our population.
Compared to the European Infective Endocarditis Registry (EURO-ENDO)10, we observed a higher incidence of congestive heart failure (41% vs. 27%) in our study cohort. This may indicate a more severe manifestation of the disease or reflect differences in heart failure definitions, as our study defined heart failure retrospectively based on diagnoses recorded in medical records, with cardiologists making the diagnosis according to established clinical criteria.
IE affecting the left side, involving either the aortic valve or the mitral valve, is the most prevalent form of valve involvement15,16. However, our study unveils a declining trend in aortic valve IE and a concurrent rise in mitral valve IE compared to the preceding two decades.
Our data showed a non-significant increase in the detection of very severe valvular regurgitation or perforation over time, possibly due to the increasing severity of the disease or improved image detection from higher-quality echocardiograms compared to the previous decade17. Recently, significant advancements have been made in other imaging modalities such as computed tomography, magnetic resonance imaging, and nuclear imaging. Utilizing these modalities for detecting cardiac and extracardiac lesions related to IE appears to offer a strategic approach in the management of patients with suspected IE18.
We demonstrated that the most common pathogens are streptococci. Importantly, this pattern remained consistent throughout the two decades of our study. Our findings align with a study conducted in low-income countries, which similarly identified the streptococci as the most prevalent causative pathogen19. This contrasts with findings from high-income countries, where staphylococci is reported as the predominant causative pathogen10,20. Nevertheless, we observed a trend similar to that reported in European registry10. The prevalence of staphylococcal and enterococcal IE increased non-significantly over time, along with a rising incidence of prosthetic valve IE. These findings suggest a shift toward healthcare-associated IE, although the changes were not statistically significant. However, despite noting an increasing trend in prosthetic valve IE from 6 to 13% in our study, this proportion remained significantly lower than the 30% reported in the EURO-ENDO registry10,21.
Interestingly, our study revealed a trend of decreasing cases associated with the oral viridans group streptococci and an increase in cases linked to Streptococcus suis, Streptococcus bovis and Streptococcus agalactiae. Of note, the rate of culture-negative IE in our population has progressively declined from 38 to 24%, aligning closely with recent report22. Beginning in 2016, we initiated the collection of tissue samples for 16 S rRNA detection in cases of culture-negative IE undergoing surgery. It has been shown that the most common cause of culture-negative IE is prior exposure to antibiotics23. Thus, 16 S rRNA detection is particularly valuable in patients who received antibiotics before sample collection. This approach exhibited a high yield, with a 90% success rate in identifying pathogens. Consequently, this strategy significantly contributed to reducing the rate of culture-negative IE. As a result, the enhancement in pathogen identification enables more precise diagnoses and facilitates the administration of suitable antibiotic treatments24,25.
Our study provides unique data highlighting Streptococcus suis as a significant cause of IE in northern Thailand, where its endemic presence is linked to high exposure to pigs and pork products. This finding emphasizes regional differences in IE epidemiology and the need for improved diagnostic strategies and preventive measures in high-risk populations.
Despite the reduction in cases of culture-negative IE through the use of 16 S rRNA detection, the increasing rate of surgical treatments, and the reduction in median time to surgery observed in our study, there was no significant alteration in the mortality rate, which remained constant at 18.6% over two decades. Nevertheless, this mortality rate aligns with findings from previous reports26,27. The lack of a decline in mortality rates may be attributed to the increased identification of older patients with coexisting comorbidities compared to previous periods. While surgery is associated with improved outcomes, potential selection bias should be considered, as surgical patients are often younger, fitter, and have fewer comorbidities, which may independently influence outcomes. In addition, the length of hospitalization remained relatively consistent. This may be due to the disease’s complexity, prolonged antibiotic therapy, and challenges in managing complications.
Establishing multidisciplinary teams for IE, following recent guidelines, have improved diagnosis through timely transesophageal echocardiography (TEE), advanced imaging for early complication detection, and improved microbiological workup with pathogen-specific testing. This approach has also optimized antibiotic use and surgical timing3,28,29. Furthermore, early identification of complications, optimized perioperative care, and the use of outpatient parenteral antimicrobial therapy (OPAT) could help reduce hospital stays. Encouraging a multidisciplinary team approach is essential to further improving patient outcomes.
Limitations of our study
The present study has several limitations. Firstly, its retrospective nature poses a limitation to the completion of the analysis. Secondly, the lack of information regarding antibiotic use and dosing, despite treatment largely aligned with guidelines, may impact the detailed understanding of treatment outcomes. Thirdly, insufficient data on dental hygiene, cardiac device implantation, and dialysis catheter usage further restricts the comprehensive assessment of factors associated with an increased risk of IE. Fourthly, there is the lack of exact data on the frequency of TEE performed in our patient cohort. While TEE was utilized in some cases, our retrospective data collection was based on existing medical records, which did not consistently document its use. As TEE plays a crucial role in confirming the diagnosis of IE and assessing its severity, the absence of detailed information on its application may have influenced our findings. Fifthly, the automated blood culture systems and changes in collection and processing methods over time may have influenced pathogen detection rates, but detailed data on these transitions were not available in our retrospective study. Lastly, the transition from paper-based records to electronic medical records over time may have influenced the completeness of symptom documentation, potentially affecting our findings. As a result, we were unable to obtain a complete set of records with diagnostic codes from earlier time periods. This may have led to a higher number of cases that did not meet the criteria for definite IE and could have introduced systematic bias.
Conclusion
We have demonstrated that clinical characteristics and microbiology of IE have changed significantly over two decades. The increasing age of IE patients with higher prevalence of co-morbidities has been observed across the three studied periods. Despite prompt medical attention and early surgical intervention, the in-hospital mortality rates remain high.
Data availability
The data that support the findings of this study are available from the corresponding author upon reasonable request.
References
Momtazmanesh, S. et al. Global, regional, and National burden and quality of care index of endocarditis: the global burden of disease study 1990–2019. Eur. J. Prev. Cardiol. 29, 1287–1297. https://doi.org/10.1093/eurjpc/zwab211 (2022).
Murdoch, D. R. et al. Clinical presentation, etiology, and outcome of infective endocarditis in the 21st century: the international collaboration on Endocarditis-Prospective cohort study. Arch. Intern. Med. 169, 463–473. https://doi.org/10.1001/archinternmed.2008.603 (2009).
Delgado, V. et al. 2023 ESC guidelines for the management of endocarditis. Eur. Heart J. 44, 3948–4042. https://doi.org/10.1093/eurheartj/ehad193 (2023).
Li, J. S. et al. Proposed modifications to the Duke criteria for the diagnosis of infective endocarditis. Clin. Infect. Diseases: Official Publication Infect. Dis. Soc. Am. 30, 633–638. https://doi.org/10.1086/313753 (2000).
Ivanovic, B., Popovic, J., Dukic, D., Petkovic, A. & Petrovic, O. The role of imaging in infective endocarditis. J. Clin. Ultrasound: JCU. 50, 1060–1065. https://doi.org/10.1002/jcu.23346 (2022).
Cresti, A. et al. Epidemiological and mortality trends in infective endocarditis, a 17-year population-based prospective study. Cardiovasc. Diagnosis Therapy. 7, 27–35. https://doi.org/10.21037/cdt.2016.08.09 (2017).
Talha, K. M. et al. Escalating incidence of infective endocarditis in Europe in the 21st century. Open. Heart 8. https://doi.org/10.1136/openhrt-2021-001846 (2021).
Tleyjeh, I. M. et al. In the ESC Textbook of Cardiovascular Medicine.0 (Oxford University Press, 2018).
Noubiap, J. J., Nkeck, J. R., Kwondom, B. S. & Nyaga, U. F. Epidemiology of infective endocarditis in Africa: a systematic review and meta-analysis. Lancet Global Health. 10, e77–e86. https://doi.org/10.1016/s2214-109x(21)00400-9 (2022).
Habib, G. et al. Clinical presentation, aetiology and outcome of infective endocarditis. Results of the ESC-EORP EURO-ENDO (European infective endocarditis) registry: a prospective cohort study. Eur. Heart J. 40, 3222–3232. https://doi.org/10.1093/eurheartj/ehz620 (2019).
Angsutararux, T. & Angkasekwinai, N. Cumulative incidence and mortality of infective endocarditis in Siriraj hospital-Thailand: a 10-year retrospective study. BMC Infect. Dis. 19, 1062. https://doi.org/10.1186/s12879-019-4689-5 (2019).
Pachirat, O. et al. Clinical outcome of native valve infective endocarditis in Khon Kaen: 1990–1999. J. Med. Association Thail. = Chotmaihet Thangphaet. 85, 139–146 (2002).
Watt, G. et al. Infective endocarditis in Northeastern Thailand. Emerg. Infect. Dis. 20, 473–476. https://doi.org/10.3201/eid2003.131059 (2014).
Watkins, D. A. et al. Rheumatic heart disease worldwide: JACC scientific expert panel. J. Am. Coll. Cardiol. 72, 1397–1416. https://doi.org/10.1016/j.jacc.2018.06.063 (2018).
Gálvez-Acebal, J. et al. Influence of early surgical treatment on the prognosis of left-sided infective endocarditis: a multicenter cohort study. Mayo Clin. Proc. 89, 1397–1405. https://doi.org/10.1016/j.mayocp.2014.06.021 (2014).
Van Vlasselaer, A., Rasmussen, M., Nilsson, J., Olaison, L. & Ragnarsson, S. Native aortic versus mitral valve infective endocarditis: a nationwide registry study. Open. Heart. 6, e000926. https://doi.org/10.1136/openhrt-2018-000926 (2019).
Sordelli, C. et al. Infective endocarditis: echocardiographic imaging and new imaging modalities. J. Cardiovasc. Echography. 29, 149–155. https://doi.org/10.4103/jcecho.jcecho_53_19 (2019).
Erba, P. A. et al. Multimodality Imaging in Infective Endocarditis. 140, 1753–1765. https://doi.org/10.1161/CIRCULATIONAHA.119.040228 (2019).
Yew, H. S. & Murdoch, D. R. Global trends in infective endocarditis epidemiology. Curr. Infect. Dis. Rep. 14, 367–372. https://doi.org/10.1007/s11908-012-0265-5 (2012).
Nappi, F., Martuscelli, G., Bellomo, F., Avtaar Singh, S. S. & Moon, M. R. Infective endocarditis in High-Income countries. Metabolites 12. https://doi.org/10.3390/metabo12080682 (2022).
Glaser, N., Jackson, V., Holzmann, M. J., Franco-Cereceda, A. & Sartipy, U. Prosthetic valve endocarditis after surgical aortic valve replacement. 136, 329–331. https://doi.org/10.1161/CIRCULATIONAHA.117.028783 (2017).
Lin, K. P. et al. Blood culture negative endocarditis: A review of laboratory diagnostic approaches. Int. J. Gen. Med. 16, 317–327. https://doi.org/10.2147/ijgm.S393329 (2023).
McHugh, J. & Saleh, O. A. Updates in Culture-Negative Endocarditis. Pathogens 12. https://doi.org/10.3390/pathogens12081027 (2023).
Hong, H. L. et al. 16S rRNA gene PCR/Sequencing of heart valves for diagnosis of infective endocarditis in routine clinical practice. J. Clin. Microbiol. 61, e0034123. https://doi.org/10.1128/jcm.00341-23 (2023).
Anton-Vazquez, V. et al. 16S rDNA PCR for the aetiological diagnosis of culture-negative infective endocarditis. Infection 50, 243–249. https://doi.org/10.1007/s15010-021-01690-x (2022).
Chu, V. H. et al. Early predictors of In-Hospital death in infective endocarditis. 109, 1745–1749. https://doi.org/10.1161/01.CIR.0000124719.61827.7F (2004).
Chen, H. et al. The global, regional, and National burden and trends of infective endocarditis from 1990 to 2019: results from the global burden of disease study 2019. Front. Med. 9, 774224. https://doi.org/10.3389/fmed.2022.774224 (2022).
Camou, F. et al. Management of infective endocarditis and multidisciplinary approach. Med. Et Maladies Infectieuses. 49, 17–22. https://doi.org/10.1016/j.medmal.2018.06.007 (2019).
Baddour, L. M. et al. Infective endocarditis in adults: diagnosis, antimicrobial therapy, and management of complications: A scientific statement for healthcare professionals from the American heart association. Circulation 132, 1435–1486. https://doi.org/10.1161/cir.0000000000000296 (2015).
Funding
This work was supported by Faculty of Medicine Endowment Fund for Medical Research, Chiang Mai University, Thailand. The funding sources had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication.
Author information
Authors and Affiliations
Contributions
N.P. conducted the statistical analysis, drafted the manuscript, and created the tables. R.C. and A.P. provided critical revisions for important intellectual content. W.W. made substantial contributions to the conception and design of the study, as well as the acquisition, analysis, and interpretation of the data. All authors have agreed to take responsibility for all aspects of the work, ensuring that any questions related to the accuracy or integrity of any part of the study are properly investigated and addressed.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval
This study was approved by the Institutional Research Ethics Committee of the Faculty of Medicine, Chiang Mai University, and conducted in accordance with the Declaration of Helsinki. Approval was granted under exemption number 0392/2024. Written informed consent was waived by the Institutional Research Ethics Committee of the Faculty of Medicine, Chiang Mai University due to the retrospective nature of the study. The study was registered at thaiclinicaltrials.org, identification number TCTR20240726001.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Pongbangli, N., Chaiwarith, R., Phrommintikul, A. et al. Trends in infective endocarditis over two decades in a Thai tertiary care setting. Sci Rep 15, 13746 (2025). https://doi.org/10.1038/s41598-025-96609-z
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-96609-z
