
Abstract
There is insufficient evidence regarding the use of second-line vasopressors following norepinephrine administration in the post-resuscitation management of patients with out-of-hospital cardiac arrest (OHCA). Therefore, this study aimed to investigate the survival outcomes between norepinephrine plus epinephrine and norepinephrine plus vasopressin as vasopressor combinations after return of spontaneous circulation (ROSC) in patients with OHCA. This retrospective observational study included data from a prospective multicenter registry. Adult patients with OHCA who achieved sustained ROSC and received vasopressor combinations of norepinephrine plus epinephrine or norepinephrine plus vasopressin were included in the study. The variable of interest was the vasopressor combination either norepinephrine plus epinephrine or norepinephrine plus vasopressin within 24 h from sustained ROSC. The primary outcome was survival to discharge. Multivariable logistic regression analysis was conducted. Between October 2015 and June 2024, 901 patients were analyzed. Survival to discharge and good neurological outcome were significantly higher in the group with norepinephrine plus epinephrine than in the group with norepinephrine plus vasopressin (17.0% vs. 9.1%, p = 0.001, and 8.1% vs. 3.2%, p = 0.002, respectively). Norepinephrine plus vasopressin was independently associated with worse survival to discharge and neurological outcome compared to norepinephrine plus epinephrine, after adjusting for potential confounders (adjusted odds ratio [aOR] 0.454, 95% confidence interval [CI] 0.277–0.746, p = 0.002 and aOR 0.346, 95% CI 0.150–0.794, p = 0.012, respectively). These findings were maintained in multiple regression models and sensitivity analyses. Norepinephrine plus epinephrine administration within 24 h from sustained ROSC showed better survival to discharge than norepinephrine plus vasopressin in patients with OHCA.
Similar content being viewed by others
Introduction
Annually, approximately 356,000 patients in the United States and 275,000 patients in Europe experience out-of-hospital cardiac arrest (OHCA)1,2. Despite improvements over the past few decades, OHCA remains a global health burden with high mortality3,4,5,6. High-quality cardiopulmonary resuscitation (CPR) is crucial in patients with OHCA7. After achieving return of spontaneous circulation (ROSC), hemodynamic stabilization, identifying the cause of cardiac arrest, and correcting reversible causes are important7,8,9. Vasopressors are frequently required after ROSC to achieve hemodynamic optimization7,8,9.
Norepinephrine, epinephrine, and vasopressin are widely used vasopressors. Norepinephrine is a potent α1 adrenergic receptor agonist and a less potent β1 adrenergic receptor agonist, resulting in vasoconstriction with some inotropic effects10,11. Norepinephrine is recommended as the first-line vasopressor of choice in most situations, including sepsis, cardiogenic shock, and post-resuscitation management8,12,13. Epinephrine is a more potent β1-adrenergic receptor agonist than norepinephrine and a moderate α1 and β2 adrenergic receptor agonist, resulting in strong inotropic effects and vasoconstriction10,11,12,13,14. Epinephrine is commonly used as a second-line vasopressor11,12. In patients with sepsis, epinephrine was formerly recommended as a second-line vasopressor13; however, it was recently recommended as a third-line vasopressor after norepinephrine and vasopressin14. Vasopressin is a V1 and V2 agonist, resulting in vasoconstriction10,11,15. Vasopressin is also commonly used as a second-line vasopressor, including sepsis12,13,14. The combination of vasopressin with norepinephrine has been shown to decrease catecholamine dose requirements16,17 and reduce the risk of renal replacement therapy in patients with sepsis17. Because of these benefits, vasopressin has been solely recommended as a second-line vasopressor for sepsis in recent guidelines14.
In patients with OHCA, vasopressors in addition to norepinephrine administration are often required to stabilize hemodynamics after ROSC. However, there is insufficient evidence regarding the use of second-line vasopressors following norepinephrine administration in the post-resuscitation management of patients with OHCA8. Therefore, this study aimed to investigate the survival outcomes between norepinephrine plus epinephrine (NE + E) and versus norepinephrine plus vasopressin (NE + V) as vasopressor combinations after ROSC in patients with OHCA.
Methods
Study design and setting
This retrospective observational study analyzed data from a prospective multicenter registry, the Korean Cardiac Arrest Resuscitation Consortium (KoCARC) registry18,19. The KoCARC registry is a university-affiliated, hospital-based research network that enrolled patients with OHCA having a medical cause of cardiac arrest who were resuscitated by emergency medical services (EMS). Patients with obvious non-cardiac etiology, such as trauma, drowning, poisoning, burns, asphyxia, or hanging; patients with terminal illnesses receiving hospice care; pregnant patients; and those with a do-not-resuscitate order were excluded from the KoCARC registry. The KoCARC registry collects data on patient demographics, epidemiology, prehospital variables, in-hospital variables, and outcomes. It was registered with ClinicalTrials.gov (NCT03222999) and approved by the Institutional Review Boards of each participating hospitals.
This study was conducted in accordance with the principles of the Declaration of Helsinki. The Institutional Review Board of the Korea University Ansan Hospital approved this study and waived the requirement for informed consent owing to the observational nature of the study (2024AS0203).
In South Korea, a typical EMS ambulance includes two to three personnel: one level-1 emergency medical technician (EMT; equivalent to EMT-intermediate in North American EMS), one level-2 EMT (equivalent to EMT-basic), and nurses. Advanced airway insertion and on-scene administration of resuscitation medications are allowed only for level-1 EMTs under direct medical supervision. Because death declaration at the scene is prohibited unless the patient shows obvious signs of death, most patients with cardiac arrest are transported to a hospital19.
In South Korea, norepinephrine is recommended as a first-line vasopressor for most forms of shock, including septic shock, in accordance with international guidelines20,21. Epinephrine and vasopressin are typically administered as additional vasopressors in patients requiring further hemodynamic support. As there are no specific recommendations for vasopressor combinations in patients with OHCA requiring more than one vasopressor after sustained ROSC, the vasopressor combination was selected at the physicians’ discretion.
Study population and data extraction
Adult patients with OHCA having sustained ROSC who received vasopressors between October 2015 and June 2024 were included in this study. Sustained ROSC was defined as ROSC lasting more than 20 min. For patients who received extracorporeal CPR, sustained ROSC was considered achieved when extracorporeal membrane oxygenation (ECMO) was initiated. Patients receiving a single type of vasopressor or a vasopressor combination other than NE + E or NE + V were excluded from the study. Patients with missing or unknown prehospital and in-hospital variables were also excluded. The following data were extracted from the KoCARC registry: age, sex, calendar year, comorbidities, witness status, place of arrest, bystander CPR, initial cardiac arrest rhythm, prehospital defibrillation, prehospital advanced airway insertion, total epinephrine dose during CPR, CPR time, initial lactate level, in-hospital management such as coronary angiography (CAG), percutaneous coronary intervention (PCI), targeted temperature management (TTM), and ECMO, survival to discharge, and neurological outcome at discharge. A good neurological outcome was defined as a cerebral performance category score of one or two22,23.
Variable of interest
The variable of interest was the vasopressor combination of NE + E or NE + V administered within 24 h from sustained ROSC.
Outcomes
The primary outcome was survival to discharge. The secondary outcomes were a good neurological outcome at discharge, survival at 6 months, and a good neurological outcome at 6 months.
Statistical analysis
Normally distributed continuous variables were expressed as means and standard deviations and compared using the Student’s t-test. Non-normally distributed continuous variables were expressed as medians and interquartile ranges and compared using the Mann–Whitney U test. Categorical variables were expressed as numbers and percentages and were compared using the chi-square or the Fisher’s exact tests.
Univariable logistic regression analysis was performed (Supplementary Table 1). Multivariable logistic regression analyses were used to evaluate independent associations between vasopressor combinations and outcomes. Multiple models were performed: Model 1 adjusted for age, sex, and calendar year; Model 2 adjusted for comorbidities and prehospital variables in addition to those in Model 1; Model 3 adjusted for total epinephrine dose, CPR time, and initial lactate level in addition to those in Model 2; and Model 4 adjusted for CAG, PCI, TTM, and ECMO in addition to those in Model 3. The Hosmer–Lemeshow test was performed to evaluate the goodness of fit of the models. Further analysis after categorizing into three groups (NE + E, NE + V without dobutamine, and NE + V with dobutamine) were performed.
An exploratory analysis was performed after additional adjustments for dobutamine use. An additional exploratory analysis was conducted after adjusting for the sequential organ failure assessment (SOFA) score24,25. Subgroup analysis was performed according to initial cardiac arrest rhythm, witness status, and total epinephrine dose (< 4 mg or ≥ 4 mg). Sensitivity analysis was performed after multiple imputations using Multivariate Imputation by Chained Equations (‘mice’ package) for missing in-hospital variables26.
Statistical significance was set at p < 0.05. Statistical analyses were performed using R version 4.0.2 (R Foundation for Statistical Computing, Vienna, Austria).
Results
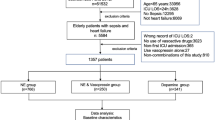
Between October 2015 and June 2024, 10,105 adult patients with OHCA having ROSC were screened from the KoCARC registry. Vasopressors were administered to 7,539 patients after ROSC. Of these, 4,253 patients were excluded because of the administration of a single type of vasopressor, 412 patients were excluded because of the administration of vasopressor combinations other than NE + E or NE + V, 44 patients were excluded because of missing or unknown prehospital variables, and 181 patients were excluded because of missing or unknown in-hospital variables. Finally, 901 patients were included in the analysis (Fig. 1).

Flowchart of study population.
Baseline characteristics between norepinephrine plus epinephrine and norepinephrine plus vasopressin
Calendar years 2016–2019, cardiac arrest in a public place, initial shockable rhythm, prehospital defibrillation, and performance of CAG were more frequent in the NE + E group than in the NE + V group. The total epinephrine dose during CPR was higher, and the initial lactate level was lower in the NE + E group than in the NE + V group. TTM was performed less frequently, and malignancy was less frequent in the NE + E group than in the NE + V group. Among survival outcomes, survival to discharge, a good neurological outcome at discharge, survival at 6 months, and a good neurological outcome at 6 months were significantly higher in the group with NE + E than in the group with NE + V (survival to discharge: 17.0% vs. 9.1%, p = 0.001; good neurological outcome at discharge: 8.1% vs. 3.2%, p = 0.002; survival at 6 months: 7.2% vs. 1.5%, p = 0.001; good neurological outcome at 6 months: 4.8% vs. 0.8%, p < 0.001; Table 1).
Multivariable logistic regression analysis
NE + V was independently associated with worse survival to discharge than NE + E in all models (Model 1: adjusted odds ratio [aOR] 0.467, 95% confidence interval [CI] 0.306–0.713, p < 0.001; Model 2: aOR 0.564, 95% CI 0.363–0.876, p = 0.011; Model 3: aOR 0.574, 95% CI 0.364–0.905, p = 0.017; Model 4: aOR 0.454, 95% CI 0.277–0.746, p = 0.002; Table 2). NE + V was independently associated with worse neurological outcome than NE + E in all models (Model 1: aOR 0.319, 95% CI 0.166–0.612, p = 0.001; Model 2: aOR 0.421, 95% CI 0.207–0.857, p = 0.017; Model 3: aOR 0.449, 95% CI 0.214–0.941, p = 0.034; Model 4: aOR 0.346, 95% CI 0.150–0.794, p = 0.012; Table 2). NE + V was independently associated with worse survival at 6 months and a worse neurological outcome at 6 months compared to NE + E in all models (Table 2). The Hosmer–Lemeshow test indicated a good fit in all models (p > 0.05).
Analysis after categorizing into three groups
When vasopressors were categorized into three groups (NE + E, NE + V without dobutamine, and NE + V with dobutamine), survival to discharge and good neurological outcome were significantly different between the groups. In post hoc analysis, survival to discharge and good neurological outcome were significantly lower in the NE + V without dobutamine group than in the NE + E group (survival to discharge: NE + E 17.0% vs. NE + V without dobutamine 9.0% vs. NE + V with dobutamine 12.5%, p = 0.002, and good neurological outcome: NE + E 8.1% vs. NE + V without dobutamine 2.9% vs. NE + V with dobutamine 12.5%, p = 0.001, respectively; Supplementary Table 2).
In multivariable logistic regression analysis, NE + V without dobutamine was independently associated with worse survival to discharge and neurological outcome than NE + E after adjusting for age, sex, calendar year, comorbidities, prehospital, and in-hospital variables (aOR 0.458, 95% CI 0.277–0.758, p = 0.002, and aOR 0.302, 95% CI 0.126–0.722, p = 0.007, respectively; Table 3). However, NE + V with dobutamine was not independently associated with outcomes (aOR 0.394, 95% CI 0.070–2.208, p = 0.289, and aOR 1.065, 95% CI 0.157–7.215, p = 0.949, respectively; Table 3).
Exploratory analysis
Dobutamine use was comparable between the groups (Supplementary Table 3). When dobutamine was additionally adjusted for in multivariable analysis, NE + V was still independently associated with worse survival to discharge and neurological outcome compared to NE + E (aOR 0.454, 95% CI 0.277–0.746, p = 0.002, and aOR 0.354, 95% CI 0.154–0.812, p = 0.014, respectively; Supplementary Table 4).
The SOFA score was significantly higher in the NE + V group than in the NE + E group (Supplementary Table 3). When the SOFA score was additionally adjusted for in multivariable analysis, NE + V was still independently associated with worse survival to discharge and neurological outcome compared to NE + E (aOR 0.525, 95% CI 0.316–0.871, p = 0.013, and aOR 0.408, 95% CI 0.174–0.957, p = 0.039, respectively; Supplementary Table 4).
Subgroup analysis
Survival to discharge was significantly lower in the NE + V group than in the NE + E group, regardless of initial cardiac arrest rhythm, and in the subgroup with witnessed cardiac arrest and a total epinephrine dose < 4 mg (Table 4).
Sensitivity analysis
A total of 1082 patients were analyzed after multiple imputations for missing in-hospital variables. NE + V was still independently associated with worse survival to discharge and neurological outcome compared to NE + E after adjustment for age, sex, calendar year, prehospital, and in-hospital variables (aOR 0.538, 95% CI 0.347–0.832, p = 0.005, and aOR 0.411, 95% CI 0.212–0.798, p = 0.009, respectively; Supplementary Table 4).
Discussion
In patients with OHCA, NE + E after ROSC was associated with better survival to discharge, a better neurological outcome at discharge, better survival at 6 months, and a better neurological outcome at 6 months compared to NE + V. Survival to discharge was higher in the NE + E group than in the NE + V group in subgroups with initial shockable rhythm, non-shockable rhythm, witnessed cardiac arrest, and a total epinephrine dose of < 4 mg. While NE + V without dobutamine was associated with decreased survival to discharge and neurological outcome compared to no NE + E, NE + V with dobutamine showed comparable survival outcomes compared to NE + E. Since there are no specific recommendations for vasopressor use after norepinephrine administration in the post-resuscitation management of patients with OHCA8, and recent recommendations are based on studies of critically ill patients, including those with hypotensive, distributive, or cardiogenic shock8, our findings suggest that epinephrine may be a suitable second-line vasopressor following norepinephrine for the post-resuscitation management of these patients. Further large-cohort studies or randomized controlled trials are warranted to confirm these findings.
The strengths of our study include the use of a multicenter prospective registry. In addition, to the best of our knowledge, this is the first study to directly compare NE + E and NE + V as vasopressor combinations after ROSC in patients with OHCA. We further adjusted for multiple in-hospital variables, including important procedures that impact survival outcomes. To address the potential differences in severity between groups, we adjusted for initial lactate levels and further adjusted for SOFA scores, which showed similar results. Additionally, further analysis was conducted considering the use of dobutamine, a widely used inotrope, which showed results consistent with the main findings. Moreover, we conducted multiple logistic regression models and applied a multiple imputation method, both of which produced similar results, leading to the robustness of our findings. Our study provides novel insights into vasopressor management after ROSC in patients with OHCA.
One of the major differences between epinephrine and vasopressin is the presence of a potent inotropic effect via β1 adrenergic receptor agonism. As cardiac arrest is an extreme form of cardiac failure, inotropes may help restore myocardial dysfunction, which frequently occurs after cardiac arrest8. Additionally, inotropic support might increase the likelihood of achieving hemodynamic stabilization, allowing time and the opportunity to identify and address the cause of cardiac arrest in unstable patients. However, vasopressin does not exert any inotropic effects. This limitation may be overcome by using dobutamine, which has a potent inotropic effect; however, it may also have vasodilatory effects10,11,27. The addition of dobutamine to vasopressin may provide sufficient inotropic support without vasodilatory effect, due to vasoconstriction via V1 receptor agonism. This can be supported by our results, showing comparable survival outcomes in the group with NE + V with dobutamine compared to the group with NE + E. Therefore, in patients who require more than one type of vasopressor, administering agents with inotropic effects, such as epinephrine or vasopressin plus dobutamine, may help restore perfusion to vital organs, leading to better survival outcomes.
Another difference between epinephrine and vasopressin is the presence of the effect on coronary blood flow via adrenergic receptor agonism. Coronary blood flow is highly influenced by the balance between vasoconstriction through α1 adrenergic receptors and vasodilation through β2 adrenergic receptors28,29. These receptors are heterogeneously distributed in coronary arteries: α1 adrenergic receptors are predominant in larger coronary vessels, whereas β2 adrenergic receptors are predominant in smaller coronary vessels28. The vasodilatory effect via β2 adrenergic receptor stimulation is helpful for increasing coronary blood flow, especially during exercise or stressful conditions28. This vasodilatory effect is impaired in patients with coronary atherosclerosis28,29. Furthermore, the regulation of coronary collateral circulation is mediated by β2 adrenergic receptors, and the redistribution of transmural blood flows is balanced by α and β adrenergic receptors28. Additionally, coronary blood flow can be affected by heart rate. Epinephrine has the greatest chronotropic effect, which increases heart rate by approximately 15% compared to norepinephrine11,30. Conversely, vasopressin reduces heart rate by approximately 10%11,30. Coronary blood flow can be enhanced by increased relative duration of diastole at higher heart rates via adrenergic receptor stimulation10,30. These mechanisms may contribute to the better survival outcomes in the NE + E group than in the NE + V group. The balance between stimulation of α and β adrenergic receptors is important for maintaining optimal coronary blood flow. The dose and timing of adrenergic vasopressors should be optimized for individual patients, which warrants further study.
The combination of vasopressors varied significantly according to calendar year. The frequency of administration of NE + V was increased in 2020–2024. This might be due to the recently published Surviving Sepsis Campaign guidelines, which recommended vasopressin as a second-line vasopressor because of survival benefits and renoprotective effects14,16,17. In the past, both epinephrine and vasopressin were recommended as second-line vasopressors13. As sepsis is one of the most frequent forms of shock in the emergency department, many physicians may have been influenced by the recent sepsis guidelines, resulting in similar management approaches for hemodynamically unstable OHCA patients with ROSC.
In the subgroup with a total epinephrine dose < 4 mg, NE + E showed better survival to discharge than NE + V. These patients might be more sensitive to epinephrine. Patients with a total epinephrine dose ≥ 4 mg might be refractory to epinephrine, or their adrenergic receptors might be fully saturated, resulting in comparable survival outcomes between groups. Therefore, epinephrine might be a good second vasopressor of choice after norepinephrine administration, especially in patients who achieved ROSC with lower epinephrine use during CPR.
This study had some limitations. First, owing to the observational study design, there may have been missed covariables, and we could only identify associations. Second, this study was conducted in a single country, so the results cannot be generalized to other countries. Third, despite the use of a large multicenter prospective registry, a relatively small number of patients were analyzed. Therefore, caution is needed when interpreting the results for good neurological outcome, which had showed low incidence. Fourth, vasopressor dose, initiation timing, and duration were not collected. During data collection for the registry, the research coordinators at each participating hospital reviewed medical records for the vasopressor administration time and duration but only recorded whether the vasopressors were infused within 24 h from sustained ROSC. Although our study does not allow us to fully determine the sequence and simultaneous administration of vasopressors in all cases, norepinephrine is typically administered as a first-line vasopressor in most forms of shock, and epinephrine and vasopressin are typically administered as additional vasopressors in patients requiring further hemodynamic support in routine clinical practice, which is in line with international guidelines. The alternative administration of vasopressors cannot be fully ruled out; however, such cases would be minimal. Further studies are warranted to evaluate the effects of dose, initiation timing, and duration of second vasopressor use on survival outcomes in patients with OHCA who have achieved ROSC. Fifth, numerous patients were excluded because of missing data on in-hospital variables. However, we performed a sensitivity analysis after multiple imputations for the missing data, which showed findings consistent with the main results. Sixth, patients requiring two types of vasopressors might have different characteristics compared to the general cardiac arrest population, as the proportion of patients with a shockable rhythm was relatively low. Regarding the epidemiology of OHCA in Korea, 25,604 cases (76.7%) were of medical origin in 202331. Among medical causes, 23,991 cases (93.7%) were of cardiac origin, 347 cases (1.4%) were of respiratory origin, and 1,266 cases (4.9%) were due to other causes31. Most of the study population was likely to have experienced cardiac-origin OHCA. As the classification of the cause of OHCA follows the internationally accepted Utstein template32, the exact proportion of cardiac arrest caused by sepsis is unknown and is likely classified as other causes. In addition, these patients may represent an extreme form of shock. Further studies in this population are therefore required. Seventh, we did not collect data on do-not-resuscitate orders or the withdrawal of life-sustaining treatment after hospital admission, which may affect post-cardiac arrest management and outcomes. However, to address this limitation and enhance the robustness of our findings, we performed subgroup analyses according to initial cardiac arrest rhythm and witnessed status, as patients with initial shockable rhythm and witnessed cardiac arrest are associated with better survival outcomes and a lower likelihood of receiving do-not-resuscitate orders or withdrawal of life-sustaining treatment. The consistency of the results in subgroups with initial shockable rhythm and witnessed cardiac arrest further supports the robustness of our findings. Although do-not-resuscitate orders or the withdrawal of life-sustaining treatment after hospital admission were not recorded, the consistency of our findings in these subgroups suggests that vasopressor selection may influence outcomes independently of this limitation.
Conclusion
In the current OHCA registry analyses, norepinephrine plus epinephrine within 24 h from sustained ROSC was associated with better survival to discharge than norepinephrine plus vasopressin in patients with OHCA.
Data availability
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Abbreviations
- OHCA:
-
Out-of-hospital cardiac arrest
- CPR:
-
Cardiopulmonary resuscitation
- ROSC:
-
Return of spontaneous circulation
- NE + E:
-
Norepinephrine plus epinephrine
- NE + V:
-
Norepinephrine plus vasopressin
- KoCARC:
-
Korean Cardiac Arrest Resuscitation Consortium
- EMS:
-
Emergency medical services
- EMT:
-
Emergency medical technician
- CAG:
-
Coronary angiography
- PCI:
-
Percutaneous coronary intervention
- TTM:
-
Targeted temperature management
- ECMO:
-
Extracorporeal membrane oxygenation
- SOFA:
-
Sequential organ failure assessment
- aOR:
-
Adjusted odds ratio
- CI:
-
Confidence interval
References
Odom, E. et al. Trends in EMS-attended out-of-hospital cardiac arrest survival, United States 2015–2019. Resuscitation 179, 88–93. https://doi.org/10.1016/j.resuscitation.2022.08.003 (2022).
Atwood, C., Eisenberg, M. S., Herlitz, J. & Rea, T. D. Incidence of EMS-treated out-of-hospital cardiac arrest in Europe. Resuscitation 67(1), 75–80. https://doi.org/10.1016/j.resuscitation.2005.03.021 (2005).
Yan, S. et al. The global survival rate among adult out-of-hospital cardiac arrest patients who received cardiopulmonary resuscitation: A systematic review and meta-analysis. Crit. Care. 24(1), 61. https://doi.org/10.1186/s13054-020-2773-2 (2020).
Myat, A., Song, K. J. & Rea, T. Out-of-hospital cardiac arrest: current concepts. Lancet 391, 970–979. https://doi.org/10.1016/S0140-6736(18)30472-0 (2018).
Kiguchi, T. et al. Out-of-hospital cardiac arrest across the World: First report from the International Liaison Committee on Resuscitation (ILCOR). Resuscitation 152, 39–49. https://doi.org/10.1016/j.resuscitation.2020.02.044 (2020).
Park, J. S., Lee, B. K., Ko, S. K. & Ro, Y. S. Recent status of sudden cardiac arrests in emergency medical facilities: A report from the National Emergency Department Information System (NEDIS) of Korea, 2018–2022. Clin. Exp. Emerg. Med. 10, S36–S41. https://doi.org/10.15441/ceem.23.154 (2023).
Perman, S. M. et al. 2023 American Heart Association focused update on adult advanced cardiovascular life support: an update to the American Heart Association guidelines for cardiopulmonary resuscitation and emergency cardiovascular care. Circulation 149, e254–e273. https://doi.org/10.1161/CIR.0000000000001194 (2024).
Nolan, J. P. et al. European Resuscitation Council and European Society of Intensive Care Medicine guidelines 2021: post-resuscitation care. Intensive Care Med. 47(4), 369–421. https://doi.org/10.1007/s00134-021-06368-4 (2021).
Kim, Y. M. et al. 2020 Korean guidelines for cardiopulmonary resuscitation: Part 5: Post-cardiac arrest care. Clin. Exp. Emerg. Med. 8, S41–S64. https://doi.org/10.15441/ceem.21.025 (2021).
Overgaard, C. B. & Dzavík, V. Inotropes and vasopressors: review of physiology and clinical use in cardiovascular disease. Circulation 118, 1047–1056. https://doi.org/10.1161/CIRCULATIONAHA.107.728840 (2008).
Russell, J. A. Vasopressor therapy in critically ill patients with shock. Intensive Care Med. 45, 1503–1517. https://doi.org/10.1007/s00134-019-05801-z (2019).
Vahdatpour, C., Collins, D. & Goldberg, S. Cardiogenic shock. J. Am. Heart Assoc. 8, e011991. https://doi.org/10.1161/JAHA.119.011991 (2019).
Rhodes, A. et al. Surviving sepsis campaign: International guidelines for management of sepsis and septic shock: 2016. Intensive Care Med. 43, 304–377. https://doi.org/10.1007/s00134-017-4683-6 (2017).
Evans, L. et al. Surviving sepsis campaign: international guidelines for management of sepsis and septic shock 2021. Intensive Care Med. 47, 1181–1247. https://doi.org/10.1007/s00134-021-06506-y (2021).
Demiselle, J., Fage, N., Radermacher, P. & Asfar, P. Vasopressin and its analogues in shock states: A review. Ann. Intensive Care. 10, 9. https://doi.org/10.1186/s13613-020-0628-2 (2020).
Russell, J. A. et al. Vasopressin versus norepinephrine infusion in patients with septic shock. N. Engl. J. Med. 358, 877–887. https://doi.org/10.1056/NEJMoa067373 (2008).
Gordon, A. C. et al. Effect of early vasopressin vs norepinephrine on kidney failure in patients with septic shock: The VANISH randomized clinical trial. JAMA 316, 509–518. https://doi.org/10.1001/jama.2016.10485 (2016).
Kim, J. Y. et al. Korean Cardiac Arrest Research Consortium (KoCARC): Rationale, development, and implementation. Clin. Exp. Emerg. Med. 5(3), 165–176. https://doi.org/10.15441/ceem.17.259 (2018).
Lee, S. et al. Age and sex-related differences in outcomes of OHCA patients after adjustment for sex-based in-hospital management disparities. Am. J. Emerg. Med. 80, 178–184. https://doi.org/10.1016/j.ajem.2024.04.012 (2024).
Park, C. et al. Early management of adult sepsis and septic shock: Korean clinical practice guidelines. Acute Crit. Care. 39(4), 445–472. https://doi.org/10.4266/acc.2024.00920 (2024).
Hyun, J. et al. Korean society of heart failure guidelines for the management of heart failure: Advanced and acute heart failure. Korean Circ. J. 53(7), 452–471. https://doi.org/10.4070/kcj.2023.0115 (2023).
Jennett, B. & Bond, M. Assessment of outcome after severe brain damage. Lancet 1(7905), 480–484. https://doi.org/10.1016/s0140-6736(75)92830-5 (1975).
Edgren, E., Hedstrand, U., Kelsey, S., Sutton-Tyrrell, K. & Safar, P. Assessment of neurological prognosis in comatose survivors of cardiac arrest BRCT I Study Group. Lancet 343(8905), 1055–1059. https://doi.org/10.1016/s0140-6736(94)90179-1 (1994).
Vincent, J. L. et al. The SOFA (sepsis-related organ failure assessment) score to describe organ dysfunction/failure: On behalf of the Working Group on Sepsis-Related Problems of the European Society of Intensive Care Medicine. Intensive Care Med. 22, 707–710. https://doi.org/10.1007/BF01709751 (1996).
Cour, M., Bresson, D., Hernu, R. & Argaud, L. SOFA score to assess the severity of the post-cardiac arrest syndrome. Resuscitation 102, 110–115. https://doi.org/10.1016/j.resuscitation.2016.03.001 (2016).
van Buuren, S. & Groothuis-Oudshoorn, K. mice: Multivariate imputation by chained equations in R. J. Stat. Softw. 45, 1–67. https://doi.org/10.18637/jss.v045.i03 (2011).
Suh, G. J. et al. Hemodynamic management of septic shock: Beyond the Surviving Sepsis Campaign guidelines. Clin. Exp. Emerg. Med. 10, 255–264. https://doi.org/10.15441/ceem.23.065 (2023).
Barbato, E. Role of adrenergic receptors in human coronary vasomotion. Heart 95, 603–608. https://doi.org/10.1136/hrt.2008.150888 (2009).
Barbato, E. et al. Role of beta2 adrenergic receptors in human atherosclerotic coronary arteries. Circulation 111, 288–294. https://doi.org/10.1161/01.CIR.0000153270.25541.72 (2005).
Bloom, J. E., Chan, W., Kaye, D. M. & Stub, D. State of shock: Contemporary vasopressor and inotrope use in cardiogenic shock. J. Am. Heart Assoc. 12, e029787. https://doi.org/10.1161/JAHA.123.029787 (2023).
Out-of-Hospital Cardiac Arrest Surveillance, 2023, Korea Disease Control and Prevention Agency.
Perkins, G. D., Jacobs, I. G., Nadkarni, V. M., et al. Cardiac arrest and cardiopulmonary resuscitation outcome reports: update of the Utstein Resuscitation Registry Templates for Out-of-Hospital Cardiac Arrest: a statement for healthcare professionals from a task force of the International Liaison Committee on Resuscitation (American Heart Association, European Resuscitation Council, Australian and New Zealand Council on Resuscitation, Heart and Stroke Foundation of Canada, InterAmerican Heart Foundation, Resuscitation Council of Southern Africa, Resuscitation Council of Asia); and the American Heart Association Emergency Cardiovascular Care Committee and the Council on Cardiopulmonary, Critical Care, Perioperative and Resuscitation [published correction appears in Circulation. 2015 Sep 29;132(13):e168–9. https://doi.org/10.1161/CIR.0000000000000301.]. Circulation. 132(13), 1286–1300. https://doi.org/10.1161/CIR.0000000000000144 (2015).
Acknowledgements
We would like to acknowledge and thank to investigators from all participating hospitals of KoCARC. A full list of the Korean Cardiac Arrest Research Consortium (KoCARC) Investigators is available in this Supplementary Information.
Author information
Authors and Affiliations
Consortia
Contributions
SA, BYJ and SM contributed to the study conception and design. SA, BYJ, SL, and SM contributed to investigation, methodology. The Korean Cardiac Arrest Research Consortium (KoCARC) Investigators contributed to data collection. SA, BYJ, SL, and SM contributed to data curation, formal analysis and interpretation. SA and BYJ contributed to manuscript drafting. JHP and HC provided professional suggestions. All authors have made substantial contributions to drafting the article. All authors read and approved the final article.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval and consent to participate
The Institutional Review Board of the Korea University Ansan Hospital approved this study and waived the requirement for informed consent owing to the observational nature of the study (2024AS0203).
Consent for publication
The need to obtain informed consent was waived by the Institutional Review Board of the Korea University Ansan Hospital (2024AS0203).
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Ahn, S., Jin, BY., Lee, S. et al. Comparison between norepinephrine plus epinephrine and norepinephrine plus vasopressin after return of spontaneous circulation in patients with out-of-hospital cardiac arrest. Sci Rep 15, 13375 (2025). https://doi.org/10.1038/s41598-025-96857-z
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-025-96857-z
