
Abstract
The aim of this randomized clinical trial was to evaluate the retention performance of filled and unfilled fluoride-containing resin-based fissure sealants applied to permanent first molars of children, and to assess the effect of rubber dam and cotton roll isolation techniques over an 18-month period. A total of 100 children/200 teeth participated in the study. The study was designed as a randomized, single-blinded, split-mouth trial. Mandibular permanent first molars of each patient divided into two groups: a-highly-filled pit-and-fissure sealant (Fissurit FX, Voco, Cuxhaven, Germany) and a-non-filled pit-and-fissure sealant (Teethmate F-1, Kuraray, Okayama, Japan), both containing fluoride. Considering the method of isolation of the dry working field, each group was further divided into two subgroups: rubber dam isolation and cotton roll isolation. The retention of the sealing material was analyzed at 6, 12, and 18 months. The primary outcome of the study was sealant retention, while the presence of caries lesions was recorded as a secondary outcome. The data were statistically analyzed at a significance level of 0.05. At the 18-month follow-up, the complete retention rates were 76.4% for Teethmate F1 (80.0% with cotton-roll isolation, 73.0% with rubberdam isolation), and 58.3% for Fissurit FX (59.5% with cotton-roll isolation, 57.7% with rubberdam isolation), respectively. There was no statistically significant difference between the groups in terms of the effect of isolation methods on the retention of materials. No caries lesion was detected among all the teeth being followed up after 18 months. Within the limitations of this study, sealant retention was more strongly influenced by filler content than by the isolation method used, with unfilled fluoride-containing sealants showing superior long-term retention. Both sealant types provided effective caries prevention over the 18-month follow-up period. Both fluoride-containing filled, and non-filled pit-and-fissure sealants demonstrated comparable retention and caries-preventive effects over 18 months, regardless of the isolation method, supporting their flexible use in clinical practice.
The study was registered at CliniccalTrials.gov (Registration number: NCT07110701; Date of registration: 07 August 2025).
Similar content being viewed by others


Introduction
Dental caries is among the most prevalent oral health problems worldwide and represents a major global public health concern across the life course1,2. Recent global epidemiological evidence indicates that untreated dental caries continues to affect billions of individuals and remains a leading cause of oral health–related disability1,2. Importantly, analyses of 2021 global burden data have demonstrated an increasing trend in caries prevalence over the past decade, particularly among children, underscoring that dental caries remains a persistent public health challenge despite advances in preventive strategies1,2,3. This growing burden has been observed across different regions and income levels, highlighting the need for effective and accessible preventive interventions1,2,3. The occlusal surfaces of young permanent teeth are particularly vulnerable to caries due to the deep, narrow pits and fissures in their morphology4,5. These anatomical features make them difficult to clean effectively, provide a favorable environment for the accumulation of bacteria and food, thereby facilitating the development of carious lesions4,5.
Systemic and topical fluoride applications, along with the use of fissure sealants, are well-established preventive measures aimed at halting the progression of dental caries6,7,8. Among these, fissure sealants are extensively documented as an effective intervention for preventing occlusal caries7,8,9,10,11,12,13,14,15,16. When applied correctly, sealants create a physical barrier that prevents biofilm accumulation on occlusal surfaces, arrests the progression of incipient lesions and limits bacterial colonization7,17. Evidence syntheses, including recent systematic and Cochrane reviews, support the effectiveness of resin-based fissure sealants in reducing the incidence of occlusal caries in permanent molars when compared with no treatment4,5,17. When applied correctly, sealants create a physical barrier that prevents biofilm accumulation on occlusal surfaces, arrests the progression of non-cavitated incipient lesions, and limits bacterial colonization within pits and fissures4,5,7,17,18. Accordingly, fissure sealants are consistently recommended in contemporary clinical guidelines as a core preventive measure in pediatric dentistry4,5,17,19. Despite strong evidence supporting their caries-preventive effectiveness, considerable variability in the long-term retention of fissure sealants has been reported, suggesting that material-related and clinical factors may influence clinical outcomes7,8,9,10,11,12,13,14,15,16.
The long-term efficacy of fissure sealants is highly dependent on their retention rate8,9,10,11,12,13,14,15,16,17,18. Retention is influenced by several factors, including the quality of isolation during application, the physicochemical characteristics of the sealant material, operator technique and the adequacy of the polymerization process8,9,10,11,12,13,14,15,16,17,18. Collectively, these variables play a critical role in determining the clinical performance and long-term durability of fissure sealants, thereby influencing their preventive effectiveness over time.
The management of fluids, including saliva, gingival exudate, and blood, is a critical aspect of moisture control, as it plays a pivotal role in the retention of pit and fissure sealants19,20,21,22. Inadequate isolation can reduce the sealant’s bonding efficiency, resulting in loss of retention and secondary caries developing under the material19,20,21,22. The most used isolation methods for applying pit and fissure sealants are rubber dam isolation (RDI) and cotton roll isolation (CRI). Each method has its own advantages and limitations. RDI involves isolating the treatment area in a completely dry, contamination-free environment to prevent saliva and other oral fluids from coming into contact with the sealant material19,20,21,22. This method is widely recognized as highly effective because it provides a clean, dry and sterile working area. Furthermore, it prevents the swallowing or aspiration of dental materials or instruments during treatment, thereby increasing the safety of both patient and practitioners20,21. However, rubber dam application is not always well tolerated by patients, particularly in pediatric dentistry, here it may compromise patient comfort and cooperation. In many cases, its use also necessitates local anesthesia, further limiting its practicality19,22. Unlike rubber dam, cotton roll isolation is a simpler, less invasive technique that uses cotton rolls placed around the teeth to absorb moisture and control saliva flow. Although it is easy to apply and generally more advantageous in terms of patient comfort, cotton roll isolation does not provide the same level of dryness in the working area as rubber dam isolation22. In the posterior regions in particular, cotton rolls may be insufficient to completely control moisture, which can lead to contamination. Furthermore, the success of cotton roll isolation depends heavily on the practitioner’s experience and the patient’s ability to tolerate the procedure, particularly with pediatric patients21,22.
The effect of isolation on the retention of fissure sealant materials is well understood; however, isolation alone does not determine success. The success of fissure sealants is significantly influenced by the type of material used and its physical properties, such as viscosity, flowability and abrasion resistance23,24,25. A variety of fissure sealants have been developed for clinical use, including resin-based and glass ionomer-based options, as well as flowable composite materials4,10,11,12,13,14,15,16,17,19,20,22,23,24. These materials differ in their chemical composition, adhesive properties, and resistance to oral conditions. The success of fissure sealant application depends not only on the mechanical closure of deep pits and fissures, but also on its ability to prevent caries formation4,5,8,10,11,12,13,14,15,16,17. Therefore, when evaluating fissure sealants, both their retention performance and their long-term caries preventive contribution should be considered.
Although many resin-based fissure sealants with different compositions have been developed, clinical studies directly comparing different commercial products are limited. Most of the existing studies focus only on the retention rates of the fissure sealants used, other factors and clinical conditions affecting the clinical performance of the materials are often ignored19,25,26,27. However, the success of a fissure sealant depends not only on the composition of the material but also on the treatment conditions such as moisture control during application21,22,28,29. Therefore, the aim of this randomized, controlled clinical trial was to evaluate (i) the retention rates of two different resin-based fissure sealant materials (a pit and fissure sealant containing high-filler fluoride and a pit and fissure sealant containing non-filler fluoride) and (ii) the effect of the isolation method (rubber dam isolation and cotton roll isolation) on sealant retention. In children with newly erupted permanent first molars, this study compared the 18-month retention of filled versus unfilled fluoride-containing resin-based fissure sealants placed under rubber dam or cotton roll isolation, with sealant retention as the primary outcome and caries occurrence as a secondary outcome. The null hypotheses were that (i) sealant retention does not differ between filled and unfilled fluoride-containing resin-based sealants, and (ii) isolation method (rubber dam vs. cotton roll) does not affect sealant retention.
Materials and methods
Study design
The randomized, controlled, single-blind study was approved by the Medical Ethics Committee of Izmir Katip Celebi University (approval number: 2025/059). Prior to the initiation of treatment, written informed consent was obtained from the parents of the children participating in the study. The study was registered at ClinicalTrials.gov (Registration number: NCT07110701; Date of registration: 07 August 2025). The study was conducted in accordance with the CONSORT (Consolidated Standards of Reporting Trials) guidelines to ensure transparent and comprehensive reporting of the clinical trial methodology and findings. Participants were consecutively recruited from children who presented for routine dental care at the pediatric dentistry clinic. All participants were regular patients attending the clinic for standard dental examinations or preventive treatments. Participant recruitment was conducted over a 6-month period.
Sample size
The sample size calculation was based on a superiority trial framework and was performed using G*Power software (version 3.1.9.7; Heinrich Heine University, Dusseldorf, Germany). Based on statistical parameters derived from a previously published clinical study29, the effect size was set at 0.56, with an alpha error probability of 0.05 and a statistical power of 0.81. According to these parameters, the minimum required sample size was calculated a priori as 43 teeth per group. To account for potential losses to follow-up, an overestimation of approximately 20% was applied, which is considered methodologically acceptable in pediatric clinical studies. Accordingly, the target sample size was increased to 50 teeth per group, corresponding to an approximate 20% increase. Consequently, a total of 200 teeth (100 teeth per material and 50 teeth for four subgroups) was established to ensure sufficient statistical power and maintain the validity of the study despite potential participant loss.
Sample inclusion and exclusion criteria
The study comprised 100 healthy children aged between 6 and 12 years (mean age: 7.9 years) who were classified as ASA I (American Society of Anesthesiologists) and demonstrated cooperative behavior, defined as a score of 3 or 4 on the Frankl Behavior Rating Scale. This age range was selected to include children in the early post-eruption period, during which permanent first molars are fully erupted yet remain at increased risk for occlusal caries development. All participants presented with fully erupted mandibular first permanent molars on both sides (200 teeth in total) requiring pit and fissure sealant application. Inclusion criteria were defined according to the International Caries Detection and Assessment System II (ICDAS II) and included teeth with deep and retentive pits and fissures classified as ICDAS scores 0, 1, or 2, with no restorations present. Children with special healthcare needs or systemic disease (ASA class II or higher), those requiring emergency dental treatment, exhibiting a severe gag reflex, having a known latex allergy, demonstrating uncooperative behavior (Frankl score 1 or 2), presenting with developmental enamel or dentin anomalies in the target teeth, or unable to attend follow-up visits were excluded from the study.
Screening participants
The clinical phase of the study was conducted by two researchers. One was responsible for examination and clinical treatment procedures (TO), while the other (who was blinded) was responsible for follow-up procedures (MNC). The training process was repeated at 20 randomly selected sites until examiners demonstrated substantial correlation, as measured by Cohen’s Kappa (k ≥ 0.7). After the training of the examiners, the study was initiated. The first operator, who had undergone training and performed the evaluation of the presence of caries using visual examination methods following ICDAS criteria, screened 178 children to determine their eligibility. The health history and demographics of each participant were obtained, and a clinical examination was carried out. The latter was performed with the aid of a blunt instrument and a mouth mirror with the objective of ruling out the presence of any signs of dental caries. Bitewing radiographs were obtained only when clinically indicated, such as in cases of suspected proximal caries, to support the clinical diagnosis and to ensure accurate exclusion of carious lesions. Radiographic examinations were performed in accordance with standard pediatric dental guidelines, minimizing radiation exposure.
In addition, a caries risk assessment was performed on the patients to be included in the study using the Cariogram programme (CarEng, version 3.0, Malmö University, Sweden). The following factors were taken into consideration during the evaluation process: caries experience (DMFT/DMFS values, new caries in the last year, number of fillings and missing teeth); systemic diseases; dietary content (especially sugar consumption); number of daily meals and snacks; Silness-Löe Plaque Index scores; Streptococcus mutans level in saliva (by strip test); fluoride exposure information; salivary flow rate (by stimulated saliva test); and salivary buffer capacity (by Saliva-Check Buffer or strip tests). All data were entered into the Cariogram programme, which created a caries risk profile for each patient. Patients with moderate caries risk were included in the study. Participants who met the inclusion criteria were enrolled in the study after obtaining consent from their parents or legal guardians and assent from the participants themselves.
Blinding and randomization
A split-mouth study design was employed, whereby two different fissure sealant materials were applied using two different isolation techniques. Each patient received both sealants, with one applied under rubber dam isolation and the other under cotton roll isolation. The allocation of materials and isolation methods to specific teeth was randomized to minimize bias. A computer-generated randomized list was employed to determine the sequence of application of fissure sealant materials, as well as the side (right or left mandibular molar) on which each material would be applied. In accordance with the sealant material and isolation protocol, this randomized process resulted in the formation of four different study groups.
-
a.
Fissurit FX, a highly filled fluoride-containing fissure sealant with rubber dam isolation,
-
b.
Fissurit FX, a highly filled fluoride-containing fissure sealant with cotton roll isolation,
-
c.
Teethmate F-1, an unfilled fluoride-containing fissure sealant with rubber dam isolation,
-
d.
Teethmate F-1, an unfilled fluoride-containing fissure sealant with cotton roll isolation.
The chemical composition, manufacturer, and application procedures of the tested fissure sealant materials are shown in Table 1.
Clinical procedure
The plaque and debris were removed from the occlusal surfaces using a rotating brush and non-fluoride prophylactic paste. All fissure sealant applications were performed during a single clinical visit by a single experienced operator, with the assistance of a dental assistant using four-handed dentistry. In accordance with the results of the randomization process and following the determination of the materials and isolation methods to be employed on each side of the patient, each tooth was isolated using a rubber dam, an arch and metal clasps, or cotton rolls with a high-volume suction, to avoid contamination from saliva. The application was carried out under proper illumination in accordance with the manufacturers’ recommendations, as outlined in Table 1. Following the successful application of the designated sealant to the first tooth, the contralateral homologous tooth was sealed using an alternative material. The polymerisation of all materials was conducted using an LED light-curing unit (Valo, Ultradent Products Inc., South Jordan, Utah, USA), in accordance with the manufacturer’s instructions. After each application, the sealant was subjected to testing for the absence of air bubbles, marginal adaptation, retention, and complete polymerisation. If a deficiency was identified, the tooth was re-treated. The occlusion was then subjected to evaluation, with any potential premature contacts being eliminated. All children were provided with oral hygiene instructions and any other necessary dental treatment.
Follow-up
The evaluation of pit-and-fissure sealants was conducted to record the presence of caries lesions and sealant retention at 6-, 12-, and 18-month follow-up visits. The evaluation was performed by one calibrated pediatric dentist (MNC), who had five years of clinical experience in pediatric dentistry, and was unaware of which sealant had been used, and the teeth were air-dried and observed under appropriate illumination following toothbrush prophylaxis. Sealant retention, defined as the primary outcome, was evaluated according to the Simonsen criteria (1 = complete retention; 2 = partial loss; or 3 = complete loss)30. Caries occurrence, recorded as the secondary outcome, was assessed using the International Caries Detection and Assessment System (ICDAS II) criteria. Teeth that exhibited complete sealant loss during follow-up were re-treated with fissure sealant application, as no caries lesions were detected in any of these teeth at the time of evaluation. These cases were documented as complete loss for outcome assessment and excluded from further retention analysis to avoid confusion.
Statistical analysis
The analysis of the retention rates of the fissure sealant materials was conducted utilizing the IBM SPSS Statistics 23.0 statistical software package (SPSS, Chicago, Illinois, USA). Chi-square tests were used to determine whether there were statistically significant differences in retention rates between sealant materials and isolation techniques at different time points at the 5% significance level. The Kaplan-Meier survival analysis was applied to assess the cumulative retention rates of the sealants over time. Teeth that could not be evaluated due to missed follow-up visits were treated as censored observations, whereas complete sealant loss was recorded as the event. The Log-Rank test was utilized to compare the survival distributions between different groups. The median and mean survival times for each fissure sealant and isolation technique were calculated, along with their 95% confidence intervals (CI).
Results
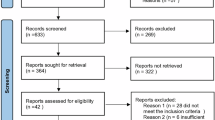
In the present study, a total of 200 fissure sealants were applied to the permanent first molars of 100 patients; however, not all patients attended the scheduled follow-up appointments throughout the 18-month trial period. During the 18-month follow-up period, 72 patients attended all the scheduled appointments, and a total of 144 teeth were evaluated for the fissure sealants’ retention rates at the end of the study. Of the 28 patients (56 teeth) lost to follow-up, the distribution across the original randomized groups was as follows: Fissurit FX/Cotton Roll: 13 teeth; Fissurit FX/Rubber Dam: 15 teeth; Teethmate F1/Cotton Roll: 15 teeth; and Teethmate F1/Rubber Dam: 13 teeth. Attrition was balanced across the four groups (χ² = 0.286, p = 0.963), indicating no evidence of differential loss to follow-up that is likely to bias the primary outcome. The primary reason for withdrawal from the study included refusal to continue participation in the trial, parents’ inability to take their children to scheduled appointments (Fig. 1).

Flow diagram of the study.
Table 2 presents the distribution of sealant retention rates after 6, 12 and 18 months for the two materials. The mean retention scores were higher for Teethmate F1 than for Fissurit FX across all time points. The complete retention rates were 58.3% for Fissurit FX and 76.4% for Teethmate F1 at the conclusion of the 18-month period. Pearson’s Chi-square tests revealed no statistically significant differences between the two materials at 6 months (χ² = 2.24, p = 0.135, df = 1), 12 months (χ² = 21.99, p = 0.157, df = 1), or 18 months (χ² = 5.48, p = 0.1064, df = 2) (p > 0.05). To further investigate the longitudinal effect of retention performance, Kaplan-Meier survival analysis was performed. The survival curves exhibited a significant difference between the two groups (Log-Rank test, χ² = 74467, df = 1, p = 0.035) (Fig. 2). The mean survival time was found to be higher for Teethmate F1 (2.942, 95% CI: 2.902–2.982) in comparison to Fissurit FX (2.850, 95% CI: 2.786–2.913).

Kaplan-Meier survival curves comparing sealant retention rates between Teethmate F1 and Fissurit FX over an 18-month period.
Table 3 provides a representation of the distribution of sealant retention rates following 6-, 12-, and 18-months for the two materials and two isolation methods. At the 18-month follow-up, the complete retention rates were 57.1% for Fissurit FX with rubber dam isolation, 59.5% for Fissurit FX with cotton roll isolation, 73.0% for Teethmate F1 with rubber dam isolation, and 80.0% for Teethmate F1 with cotton roll isolation. Chi-square analysis revealed no significant differences in full retention rates between the four groups at 6 months (χ² = 6.76, p = 0.080 df = 3), 12 months (χ² = 2.82, p = 0.419, df = 3), or 18 months (χ² = 6.03, p = 0.420, df = 6) (p > 0.05). Kaplan-Meier survival analysis revealed no significant difference in cumulative retention rates among the four groups (Log-Rank test, χ² = 4.550, df = 3, p = 0.208) (Fig. 3). The longest mean survival time was observed in Teethmate F1 with cotton roll isolation (2.986, 95% CI: 2.957–3.015), followed by Teethmate F1 with rubber dam isolation (2.899, 95% CI: 2.825–2.973). Conversely, the shortest retention times were exhibited by the Fissurit FX with rubber dam and cotton roll isolation groups (2.850, 95% CI: 2.759–2.941).

Kaplan-Meier survival curves showing cumulative sealant retention rates over 18 months for Teethmate F1 and Fissurit FX under two isolation techniques: rubber dam and cotton roll.
During the 18-month evaluation period, no caries lesions were observed in the sealed fissures of any of the materials.
Discussion
The primary objective of occlusal pit-and-fissure sealing is to create a physical barrier between the oral environment and the occlusal surfaces of the teeth, thereby preventing the ingress of food particles and bacteria that contribute to the development of dental caries. Despite the extensive range of resin-based fissure sealants available on the commercial market, comparative clinical studies evaluating their performance according to filler content remain limited, with most of the extant literature focusing primarily on retention outcomes19,27,28,31. Furthermore, the number of scientific studies investigating the effect of isolation techniques on the effectiveness of sealants in clinical settings is limited to 521,22,23,29,30. To address these gaps in the literature, the present randomized, controlled clinical was designed with two complementary objectives: first, to compare the retention of filled and unfilled resin-based fissure sealants; and second, to evaluate the effect of isolation technique (rubber dam versus cotton roll) on sealant retention.
In this study, a split-mouth design was employed to compare the clinical efficacy of two different fissure sealants and two different isolation methods. The experimental design, incorporating a split-mouth configuration, enables the assessment of each participant as their own control, thereby significantly reducing the potential influence of inter-individual biological variability28,29,32. This method offers significant advantages, especially in the field of clinical dentistry research, where factors that vary widely between individuals, such as salivary composition, occlusal loading patterns, oral hygiene habits and dietary style, can be a significant source of bias for parallel group studies27,31,32. The experimental design, which involved the utilization of a split-mouth configuration, effectively mitigated the impact of inherent biological and behavioral variability. This enabled the investigation to be concentrated exclusively on the properties of fissure sealant materials and the efficacy of isolation methods. Although quadrant-level split-mouth designs have been suggested as an alternative approach, a tooth-level split-mouth design was deliberately selected in the present study to reflect routine clinical practice and to simplify randomization and application procedures in pediatric patients. The use of homologous mandibular molars allowed for effective control of inter-individual variability while minimizing treatment complexity and patient burden. This design was considered appropriate for addressing the study objectives without compromising internal validity.
In the present study, all clinical procedures were carried out by a single experienced clinician, while controls were performed by a single independent observer. The implementation of the treatment procedures by a single experienced clinician ensured standardization of the application protocols and minimized operator-dependent variations. The methodological approach adopted in this study was designed to eliminate the potential impact of variations in operator skill levels and application habits on the study outcomes. Moreover, the control examinations were carried out by an independent assessor to reduce the risk of observer bias by increasing the blinding level of the study. The examiner’s lack of familiarity with the treatment process, as well as the materials and isolation methods employed, ensured the evaluations were conducted in a more impartial and objective manner.
The Cariogram is a comprehensive and objective assessment tool that calculates the caries risk profile of individuals using a scientifically proven algorithm32. The algorithm in question integrates a multitude of factors, including, but not limited to, dietary habits, salivary flow rate, salivary buffer capacity, plaque index and bacterial load32. The utilization of a cariogram in the selection of patients ensures that the individuals included in the study possess comparable biological characteristics at the point of baseline measurement. Consequently, the impact of individual variations in caries development on study outcomes is mitigated. The inclusion of individuals at moderate caries risk provided a balanced basis for the evaluation of both the caries preventive efficacy of fissure sealants and the success of isolation methods. Since minimal caries incidence in the low-risk group or rapid caries development in the high-risk group may make it difficult for the study to reflect only the effect of materials and application protocols, it was preferred to select the medium-risk group. However, this targeted selection should be considered when interpreting the findings, as the results may not be directly generalizable to low- or high-caries-risk populations.
Considering the findings of this study, the primary null hypothesis proposing that there would be no significant difference in retention rates between the two resin-based fissure sealant materials could not be rejected, as no statistically significant differences were observed between the sealants at any of the evaluated time points. However, survival analysis demonstrated a significantly longer mean survival time for the unfilled fluoride-containing sealant (Teethmate F1) compared to the highly filled fluoride-containing sealant (Fissurit FX). Similarly, the second null hypothesis stating that the type of isolation method (rubber dam or cotton roll) would not significantly affect sealant retention could not be rejected, as no statistically significant differences in retention rates were observed between the isolation methods for either material. The findings of the study demonstrated that Teethmate F1 fissure sealant exhibited superior retention rates in comparison to Fissurit FX across all follow-up periods, although there was no statistically significant difference in retention data obtained at control times. This finding was supported by the results of Kaplan-Meier survival analysis, which showed a significant difference in the survival distributions between the two materials. These results suggest that Teethmate F1 not only has a higher initial retention rate but also retains its integrity over time and remains retentive for longer periods. The findings of the present study are generally consistent with previously published clinical trials evaluating the retention performance of fissure sealant materials. Several clinical studies with follow-up periods of 12 months or longer have reported comparable retention rates for Teethmate F1 when compared with conventional resin-based fissure sealants, including Fissurit FX. Clinical evaluations conducted over 12-month follow-up periods have demonstrated complete retention rates for Teethmate F1 of approximately 76–77%, with no statistically significant differences when compared with other commonly used fissure sealants11,15,16. Longer-term clinical studies extending to 24 months have reported complete retention rates for Teethmate F1 of approximately 60%, again without statistically significant differences compared with alternative sealing materials17. Similarly, studies evaluating Fissurit FX in comparison with other resin-based or flowable materials have reported moderate to high retention rates over follow-up periods ranging from 12 to 24 months, frequently without statistically significant inter-material differences12,13,14. In some studies, Fissurit FX demonstrated retention outcomes comparable to or numerically higher than other resin-based sealants, although these differences were generally not statistically significant11,13. Collectively, the available clinical evidence indicates that Teethmate F1 and Fissurit FX exhibit comparable retention performance under clinical conditions, with observed variations largely attributable to differences in study design, evaluation criteria, and follow-up duration. In this context, the present study contributes additional evidence by demonstrating numerically higher retention rates and longer survival for Teethmate F1 compared with Fissurit FX under the evaluated conditions, as supported by Kaplan–Meier survival analysis.
The adhesion of the sealant to the enamel surface is achieved by the penetration of the resin material into the acid-roughened enamel surface, where it forms resin tags. The monomers within the sealant material undergo a polymerisation process, resulting in the formation of a structure that is micromechanically locked to the enamel surface25,26. In principle, high filler materials are hypothesized to exhibit enhanced resistance to wear and facilitate long-term retention24. However, an elevated filler content may result in an increase in the material’s viscosity, thereby limiting its penetration capacity into the deep and narrow fissures25,26,33. This, in turn, may have a detrimental effect on micromechanical retention. Conversely, the reduced viscosity of a filler-free material, such as Teethmate F1, may have facilitated a more effective adaptation to the deep and complex fissure anatomy and facilitated better diffusion into the micropores on the acid-roughened enamel surface, thereby creating a stronger micromechanical bond25,26,33. This finding may offer a potential explanation for the observed improvement in long-term retention outcomes. This finding is consistent with the studies in the literature indicating that low viscosity materials provide enhanced fissure penetration and may thus contribute to increased adhesion over time. For instance, Prabhakar et al.24conducted an in vitro study in which they compared high viscosity resin-based fissure sealants with low viscosity resin-based fissure sealants. This study revealed that the average length of resin tags varied between 10 μm and 5 μm. The researchers observed that microleakage was less prevalent in fissure sealants with longer resin tags and emphasised that viscosity plays an important role in the formation of resin tags, thus indicating that pit and fissure sealants with low viscosity are more advantageous. Similarly, Percinoto et al.33reported that low viscosity sealants have the capacity to penetrate more effectively into microporosities and fissures on the acid-etched enamel surface with phosphoric acid. In a similar direction, Irinoda et al.26emphasised that the structural change in the acid-etched enamel surface and the composition and viscosity of the sealants are critical in the formation of micromechanical retention, and that low viscosity sealants are more effective in completely penetrating the roughened enamel compared to high viscosity sealants. Nevertheless, materials without fillers are also associated with lower mechanical wear resistance, which should be considered when interpreting their long-term clinical performance. In addition, methacrylates are suggested to exhibit a high affinity for tissues due to their hydrophilic and hydrophobic functional groups, a property that may facilitate the diffusion of monomers35,36. In this context, the MDP (10-Methacryloyloxydecyl Dihydrogen Phosphate) contained in Teethmate F1 may have played a key role in enhancing bonding by promoting resin infiltration and the formation of resin tags on the enamel surface. Additionally, the self-etching capability of MDP may have further improved its penetration into the enamel, thereby contributing to the microretentive capacity of Teethmate F126,36.
One of the primary objectives of this study was to conduct a comparative analysis of the effects of rubber dam and cotton roll isolation on sealant retention. In the extant literature, rubber dam isolation is recognized as the gold standard for adhesive restorative procedures by it provides a completely dry and contamination-free working area19,21,22. Nevertheless, its clinical applicability may be constrained by factors such as the time required for application, patient comfort and cooperation, particularly in pediatric patients. Conversely, cotton roll isolation is a less complex and expeditious method, but its efficacy in preventing saliva contamination, particularly in posterior areas, may be contentious23. The findings of the present study demonstrated that there was no statistically significant difference between the retention rates of the materials tested for both isolation methods. The data obtained suggest that, despite the theoretical advantages of rubber dam isolation, cotton roll isolation, when properly applied, can provide similar clinical results in terms of long-term retention success of fissure sealants. These findings are in line with the existing evidence evaluating isolation techniques in restorative and preventive dental procedures. A recent Cochrane systematic review reported that, although rubber dam isolation may offer advantages in moisture control, the available evidence regarding its superiority over cotton roll isolation in terms of long-term clinical outcomes remains limited and of low certainty, particularly beyond short-term follow-up periods36. Similarly, systematic reviews focusing on tooth-colored restorative materials have demonstrated that, in most clinical studies with follow-up periods of 12 months or longer, the use of rubber dam isolation did not significantly influence restoration longevity when compared with cotton roll isolation37. With specific regard to pit and fissure sealants, recent meta-analytical data indicate that while rubber dam isolation may be associated with improved retention at certain follow-up intervals, particularly at 12 months, differences between rubber dam and cotton roll isolation are not consistently observed across all time points38. Furthermore, practical and patient-related factors must be considered when selecting an isolation method in pediatric dentistry. Alternative isolation approaches have been shown to provide comparable clinical effectiveness while offering advantages in terms of reduced chairside time and improved patient comfort, which may indirectly contribute to treatment success39. In the present study, slightly higher retention rates that observed when cotton roll isolation was used may be explained by the fact that cotton roll isolation represents a more familiar and routinely applied technique in pediatric dentistry, allowing for easier manipulation of materials and reduced chairside time. In addition, rubber dam placement in young patients may introduce unintended stresses, such as clamp-related movement or soft tissue tension, which could potentially affect isolation stability during sealant placement. Nevertheless, when adequate moisture control is achieved, both isolation methods appear capable of producing clinically acceptable outcomes.
The present study evaluated the clinical efficacy of two distinct fissure sealants, each comprising a unique formulation, which were applied using divergent isolation methods. The findings revealed that both sealants exhibited effective caries-prevention properties, with no occurrence of caries observed during the 18-month follow-up period. This outcome aligns with the findings of studies and systematic reviews and meta-analysis in the literature, which indicate that even in cases where fissure sealants are partially lost, the remaining material, particularly in the deeper sections of the fissures, can offer a residual protective effect that can impede caries development4,5,9,11,12,13,14,15,16,17,18. The absence of caries formation detected in this study, even in cases where loss of retention was observed, demonstrates that fissure sealants function not only as a mechanical barrier but also maintain their long-term caries preventive effect in the area of application. This finding can be explained by the ability of both materials to release fluoride, given its recognized remineralization capacity and inhibitory effects on bacterial activity. These effects may contribute to the prevention of localized or marginal caries at the sealed fissure sites, even in cases where complete retention is not achieved.
The present study has several notable strengths. The randomized split-mouth design using homologous mandibular molars allowed for effective control of inter-individual variability under real clinical conditions. The simultaneous evaluation of filled versus unfilled fissure sealants and rubber dam versus cotton roll isolation addresses two clinically relevant decision points within a single study framework. In addition, the use of time-to-event analysis with Kaplan–Meier survival curves enabled a dynamic assessment of sealant retention over an 18-month follow-up period. The use of Cariogram to characterize caries risk contributed to the selection of a relatively homogeneous study population. The balanced distribution of follow-up losses across groups and transparent reporting of attrition further support the internal validity and clinical relevance of the findings. However, despite the valuable insights this study provides into the clinical performance of two resin-based fissure sealants and the effects of different isolation methods, it is important to acknowledge certain limitations. The 18-month follow-up period, while informative, may not fully capture long-term retention patterns, as sealant loss can occur beyond this timeframe, longer observation periods of two to five years would be necessary to fully assess long-term sealant longevity. The attrition rate over the 18-month follow-up period may have reduced statistical power and should be considered when interpreting the results. Although the use of a single experienced operator ensured procedural standardization and minimized operator-related variability, this approach may limit the generalizability of the findings to broader clinical settings involving multiple clinicians with varying levels of experience. Future studies incorporating multiple calibrated operators may further enhance external validity. Cariogram was used to characterize caries risk and ensure a relatively homogeneous study population, but the absence of detailed baseline demographic and risk-profile data limits the extent to which these findings can be contextualized. Future studies may benefit from presenting Cariogram results alongside comprehensive baseline characteristics. The study design also focused on a single tooth type (mandibular first permanent molars) and included only children with moderate caries risk profiles, which may limit the generalizability of the findings to broader populations or different clinical scenarios. It is imperative that future research addresses the limitations identified in this study, incorporating longer observation periods, diverse tooth types, and more comprehensive patient-level variables. Only then can the complex interactions between material properties, isolation techniques, and clinical outcomes be fully elucidated.
Conclusion
Within the limitations of this study, no statistically significant differences were observed in sealant retention between filled and unfilled resin-based fissure sealants over the 18-month follow-up period. Similarly, the choice of isolation method, rubber dam or cotton roll did not significantly influence sealant retention for either material. During the 18-month follow-up period, no caries formation was detected, including cases where partial loss of retention was observed. These results emphasize the protective effect of fissure sealants and the contribution of fluoride release and demonstrate once again that material selection and application technique are critical for long-term efficacy.
Data availability
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
References
Costa, C. M. et al. Increasing global trends in early childhood caries prevalence over the last decade: global burden of disease study 2021. Caries Res. 27, 1–7 (2025).
Kimmie-Dhansay, F., Nkambule, N. R., Schoonraad, N., Albougy, H. & Bhayat, A. Prevalence of early childhood caries in africa: a systematic review. Int. J. Paediatr. Dent. 36 (1), 157–186 (2026).
Flink, H., Hedenbjörk-Lager, A., Liljeström, S., Nohlert, E. & Tegelberg, Å. Caries experience among children and adolescents from a longitudinal Swedish National registry study over a 10-year period. Acta Odontol. Scand. 85, 4–13 (2026).
Ramamurthy, P. et al. Sealants for preventing dental caries in primary teeth. Cochrane Database Syst. Rev. 2 (2), CD012981 (2022).
Ahovuo-Saloranta, A. et al. Pit and fissure sealants for preventing dental decay in permanent teeth. Cochrane Database Syst. Rev. 7 (7), CD001830 (2017).
Bahrololoomi, Z., Soleymani, A. & Heydari, Z. In vitro comparison of microleakage of two materials used as pit and fissure sealants. J. Dent. Res. Dent. Clin. Dent. Prospects. 5 (3), 83–89 (2011).
Deery, C. Caries detection and diagnosis, sealants and management of the possibly carious fissure. Br. Dent. J. 214 (11), 551–557 (2013).
Unal, M., Oznurhan, F., Kapdan, A. & Dürer, S. A comparative clinical study of three fissure sealants on primary teeth: 24-month results. J. Clin. Pediatr. Dent. 39 (2), 113–119 (2015).
Unal, M. & Oztas, N. Remineralization capacity of three fissure sealants with and without gaseous Ozone on non-cavitated incipient pit and fissure caries. J. Clin. Pediatr. Dent. 39 (4), 364–370 (2015).
Feigal, R. J. The use of pit and fissure sealants. Pediatr. Dent. 24 (5), 415–422 (2002).
Dukić, W., Dukić, O. L., Milardović, S. & Vindakijević, Z. Clinical comparison of flowable composite to other fissure sealing materials—a 12 months study. Coll. Antropol. 31 (4), 1019–1024 (2007).
Smitha, M., Paul, S. T., Nagaraj, T., Khan, A. R. & Rinu, K. Comparison and clinical evaluation of two pit and fissure sealants on permanent mandibular first molars: an in vivo study. J. Contemp. Dent. Pract. 20 (10), 1151–1158 (2019).
Kucukyilmaz, E. & Savas, S. Evaluation of different fissure sealant materials and flowable composites used as pit-and-fissure sealants: a 24-month clinical trial. Pediatr. Dent. 37 (5), 468–473 (2015).
Yilmaz, Y., Beldüz, N. & Eyüboglu, O. A two-year evaluation of four different fissure sealants. Eur. Arch. Paediatr. Dent. 11 (2), 88–92 (2010).
Dukić, W. & Glavina, D. Klinicka Evaluacija Triju Razlicitih Materijala Za pecaćenje Fisura Nakon 12 Mjeseci Uporabe [Clinical evaluation of three different materials for fissure sealing after 12 months]. Acta Med. Croatica. 60 (3), 209–214 (2006).
Dukic, W. & Glavina, D. Clinical evaluation of three fissure sealants: 24 month follow-up. Eur. Arch. Paediatr. Dent. 8 (3), 163–166 (2007).
Beauchamp, J. et al. Evidence-based clinical recommendations for the use of pit-and-fissure sealants: a report of the American dental association Council on scientific affairs. J. Am. Dent. Assoc. 139 (3), 257–268 (2008).
Ganss, C., Klimek, J. & Gleim, A. One year clinical evaluation of the retention and quality of two fluoride releasing sealants. Clin. Oral Investig. 3 (4), 188–193 (1999).
Alhareky, M. S., Mermelstein, D., Finkelman, M., Alhumaid, J. & Loo, C. Efficiency and patient satisfaction with the isolite system versus rubber dam for sealant placement in pediatric patients. Pediatr. Dent. 36 (5), 400–404 (2014).
Shukla, N. et al. Comparative evaluation of pit & fissure sealant retention using cotton roll & rubber dam isolation techniques: a systematic review & meta-analysis. Evid. Based Dent. 26 (2), 112 (2025).
Mattar, R. E., Sulimany, A. M., Binsaleh, S. S., Hamdan, H. M. & Al-Majed, I. M. Evaluation of fissure sealant retention rates using isolite in comparison with rubber dam and cotton roll isolation techniques: a randomized clinical trial. Int. J. Paediatr. Dent. 33 (1), 12–19 (2023).
Wang, Y. et al. Rubber dam isolation for restorative treatment in dental patients. Cochrane Database Syst. Rev. 17;(5):CD009858. (2021).
Hamza, B., Sekularac, M., Attin, T. & Wegehaupt, F. J. In vitro evaluation of fissure sealants’ wear under erosive, abrasive and erosive/abrasive conditions. Eur. Arch. Paediatr. Dent. 24 (1), 55–61 (2023).
Prabhakar, A. R., Murthy, S. A. & Sugandhan, S. Comparative evaluation of the length of resin tags, viscosity and microleakage of pit and fissure sealants—an in vitro scanning electron microscope study. Contemp. Clin. Dent. 2 (4), 324–330 (2011).
Irinoda, Y. et al. Effect of sealant viscosity on the penetration of resin into etched human enamel. Oper. Dent. 25 (4), 274–282 (2000).
Gisour, E. F., Jahanimoghadam, F. & Aftabi, R. Comparison of the clinical performance of self-adhering flowable composite and resin-based pit and fissure sealant: a randomized clinical trial in pediatric patients. BMC Oral Health. 24 (1), 943 (2024).
Svetha, S. et al. Comparison of retention rates of silver nanoparticles-based fissure sealant and conventional resin-based sealant: a one-year randomized clinical trial. Eur. Arch. Paediatr. Dent. 26 (4), 709–718 (2025).
Cortez, T. V. et al. Clinical performance of sealants under different humidity control conditions: a split-mouth 1-year randomized trial. Eur. Arch. Paediatr. Dent. 24 (6), 769–777 (2023).
Ammann, P., Kolb, A., Lussi, A. & Seemann, R. Influence of rubber dam on objective and subjective parameters of stress during dental treatment of children and adolescents—a randomized controlled clinical pilot study. Int. J. Paediatr. Dent. 23 (2), 110–115 (2013).
Simonsen, R. J. Retention and effectiveness of dental sealant after 15 years. J. Am. Dent. Assoc. 122 (10), 34–42 (1991).
Alharthy, H. et al. Clinical evaluation of hydrophilic and hydrophobic resin-based sealants in uncooperative children: a randomized controlled clinical trial. J. Clin. Pediatr. Dent. 48 (4), 149–159 (2024).
Bratthall, D. & Hänsel Petersson, G. Cariogram—a multifactorial risk assessment model for a multifactorial disease. Community Dent. Oral Epidemiol. 33 (4), 256–264 (2005).
Percinoto, C., Cunha, R. F., Delbem, A. C. & Aragones, A. Penetration of a light-cured glass ionomer and a resin sealant into occlusal fissures and etched enamel. Am. J. Dent. 8 (1), 20–22 (1995).
Nakabayashi, N., Ashizawa, M. & Nakamura, M. Identification of a resin-dentin hybrid layer in vital human dentin created in vivo: durable bonding to vital dentin. Quintessence Int. 23 (2), 135–141 (1992).
Wang, T., Nikaido, T. & Nakabayashi, N. Photocure bonding agent containing phosphoric methacrylate. Dent. Mater. 7 (1), 59–62 (1991).
Miao, C. et al. Rubber dam isolation for restorative treatment in dental patients. Cochrane Database Syst. Rev. 5 (5), CD009858 (2021).
Cajazeira, M. R., De Sabóia, T. M. & Maia, L. C. Influence of the operatory field isolation technique on tooth-colored direct dental restorations. Am. J. Dent. 27 (3), 155–159 (2014).
Muller-Bolla, M., Lupi-Pégurier, L., Tardieu, C., Velly, A. M. & Antomarchi, C. Retention of resin-based pit and fissure sealants: a systematic review. Community Dent. Oral Epidemiol. 34 (5), 321–336 (2006).
Siddalingappa, D., Reddy, V., Nayak, A. S., Urala, A. S. & Pentapati, K. C. Efficiency and patient-reported outcomes for isolite system: a systematic review of randomized controlled trials. Int. J. Clin. Pediatr. Dent. 18 (3), 331–338 (2025).
Acknowledgements
The authors declare that they have no acknowledgments.
Author information
Authors and Affiliations
Contributions
The responsibility of Ebru Kucukyilmaz was to conceive and design the study, contribute to writing the main manuscript, and draft the main manuscript. The responsibility of Tugba Ozdemir was to perform the experiments and collect the data. The responsibility of Merve Nur Celik was to perform the experiments and collect the data. The responsibility of Selcuk Savas was to analyze the data, interpret the results, and contribute to writing the main manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval and consent to participate
The randomized, controlled, single-blind study was approved by the Medical Ethics Committee of Izmir Katip Celebi University (approval number: 2025/059). The study was conducted in accordance with the CONSORT (Consolidated Standards of Reporting Trials) guidelines to ensure transparent and comprehensive reporting of the clinical trial methodology and findings. Both the children and their parents were informed about the study protocol, and written informed consent was obtained from the parents prior to treatment application.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Kucukyilmaz, E., Savas, S., Ozdemir, T. et al. Comparison of retention of resin-based filled and unfilled pit and fissure sealants using different isolation techniques. Sci Rep 16, 9055 (2026). https://doi.org/10.1038/s41598-026-40093-6
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-026-40093-6
