
Abstract
Metastatic colorectal cancer (mCRC) differs clinically based on RAS and BRAF mutations or DNA methylation. However, in mCRC, the prognostic value and biological characteristics of genome-wide DNA methylation status (GWMS) in each RAS/BRAF genotype is unknown. To clarify this, primary tumor samples from patients with informed consent in the phase III TRICOLORE study were collected, and RAS and BRAF mutations, immunohistochemical staining of mismatch repair-related proteins, comprehensive gene expression, and genome-wide DNA methylation were analyzed. The tumor samples were classified into high-methylated colorectal cancer (HMCC) and low-methylated colorectal cancer (LMCC). Gene set enrichment analysis (GSEA) was conducted using microarray data. A total of 226 patients were included and classified into the RAS/BRAF wild-type (wt) (n = 125), RAS mutant (mt) (n = 87), and BRAF mt (n = 14), of whom 22 (17.6%), 30 (34.5%), and 14 (100%) had HMCC. HMCC exhibited significantly worse overall survival (OS) than that of LMCC in the RAS/BRAF wt group but not in the RAS mt group. In GSEA, RAS/BRAF wt HMCC was associated with microsatellite instability and BRAF V600E mutation. The poor prognosis of RAS/BRAF wt HMCC may be attributed to gene expression patterns associated with microsatellite instability and BRAF V600E mutation.
Similar content being viewed by others


Introduction
Aberrant DNA methylation1, chromosomal instability2, and microsatellite instability (MSI)3 are the major carcinogenic mechanisms underlying colorectal cancer (CRC). There are several classification methods for CRC DNA methylation status, including the CpG island methylator phenotype (CIMP)1 and genome-wide DNA methylation status (GWMS)4. CIMP is associated with approximately 20% of CRCs5,6 and has been identified as a prognostic factor for stage II–III CRC7,8,9,10. On the other hand, we have previously shown that GWMS, based on unsupervised hierarchical clustering of genome-wide DNA methylation probes, classifies metastatic CRC (mCRC) into high-methylated colorectal cancer (HMCC) and low-methylated colorectal cancer (LMCC). Classification with GWMS seems to identify a broader range of clinically distinct groups of mCRC patients as HMCC compared to CIMP1,4. Among RAS/BRAF wild-type (wt) metastatic CRCs, HMCC has a worse prognosis than LMCC4,11,12,13 and exhibits resistance to anti-epidermal growth factor receptor (EGFR) antibodies in several reports4,11,13. However, it remains unclear whether HMCC is associated with shorter OS regardless of the coexistence of major drivers of CRC, such as RAS or BRAF mutations, as well as what biological pathway drives HMCC to show its poor prognosis.
To answer these questions, we utilized data obtained in the TRICOLORE study. It was an open-label, multicenter, randomized phase III study that examined the non-inferiority of bevacizumab + irinotecan (IRI) + S-1 combination therapy to bevacizumab + oxaliplatin (OX)-based combination therapy (mFOLFOX6 or CapeOX) in terms of progression-free survival (PFS) in patients with previously untreated mCRC. The non-inferiority of the former has been statistically confirmed in both initial and extended analyses14,15. Using data obtained from this study, we previously reported that the GWMS was not a treatment response predictor for either OX- and IRI-based combination therapy16 and that HMCC was associated with worse survival than LMCC in mCRC12.
The objective of this study is to determine whether the prognosis of mCRC across RAS/BRAF genotypes is influenced by GWMS and to elucidate the mechanism at the gene expression level.
Materials and methods
Patients and materials
The TRICOLORE study was conducted in accordance with the Declaration of Helsinki and the Japanese Guidelines for the Ethics of Clinical Research. The study was approved by the institutional review board of each participating facility16 and registered in UMIN-CTR (http://www.umin.ac.jp/ctr/) (UMIN000007834). Informed consent was obtained from all the study participants. Only patients who provided informed consent for the translational research (TR) before treatment initiation were included. The formalin-fixed, paraffin-embedded (FFPE) tissues were collected from surgical or biopsy specimens of primary CRC.
Gene mutational analysis
In this study, BRAF mutation exclusively refers to BRAF V600E mutation here. Mutational analyses of KRAS (codons 12, 13, 59, and 61), NRAS (codons 12, 13, 59, and 61), BRAF (codon 600), PIK3CA (exons 9 and 20), and AKT1 (codon 17) were conducted via direct DNA sequencing as described previously17,18. Genomic DNA was extracted from FFPE tissue slides or sections using QIAamp DNA FFPE tissue kit (Qiagen, Hilden, Germany) according to the manufacturer’s instructions. DNA sequences were analyzed using the automated CEQ2000XL DNA analysis system (Beckman Coulter, Fullerton, CA, USA).
Immunohistochemistry
Immunohistochemistry (IHC) for mismatch repair proteins (MLH1, MSH2, MSH6, and PMS2) and phosphatase and tensin homolog (PTEN) was performed at the Department of Pathology, Tohoku University Hospital. Details of the IHC were described in a previous report16. The following antibodies were used for IHC: an anti-human mouse MLH-1 clone G168-15 (1/100; BD Biosciences, San Jose, CA, USA), an anti-MSH2 mouse mAb clone FE11 (1/200; Sigma-Aldrich, St. Louis, MO, USA), an anti-MSH6 mouse clone 44 (1/1000; BD Biosciences), an anti-PMS2 mouse clone 16-4 (1/100; BD Biosciences), and a PTEN clone 6H2.1 (1/100; DAKO, Carpinteria, CA, USA). MMR-related proteins and PTEN positivity was classified according to the stainability of nuclei and cytoplasm, respectively.
Comprehensive gene expression analysis
Comprehensive gene expression analysis was conducted using the Whole Human Genome 4 × 44K Microarray Kit (Agilent, Santa Clara, CA, USA) as previously described16,19. We collected tumor cells by macrodissection and performed comprehensive gene-expression analysis with GeneSpringGX ver. 14.5 (Agilent). In the advanced CRC subtype, tumors were classified into A1, A2, B1, and B2 using unsupervised hierarchical clustering based on the Pearson uncentered and complete linkage clustering algorithm19. The CMS classification was performed by the gene expression profile using the single-sample predictor installed in the R package “CMS classifier”20. The similarity of the expression profile to the four subtypes (CMS1 to CMS4) was calculated in each case as “nearest CMS”21.
Genome-wide DNA methylation analysis
Genome-wide DNA methylation analysis was conducted using the Infinium MethylationEPIC BeadChip (Illumina, San Diego, CA, USA) as previously described4. The BeadChip was scanned using the iScan, and the DNA methylation β-value was calculated as intensity of methylated probe / (intensity of methylated probe + intensity of unmethylated probe). After excluding probes for the X and Y chromosomes, those with ≥ 0.25 SD of the β-value in all CRC samples were selected for further analyses. Based on hierarchical clustering of the genome-wide DNA methylation profile, the tumors were classified into HMCC and LMCC. The resulting heatmap and dendrogram has been previously described12. Tumors with three or more positive methylation regions among the five promoter regions, namely, CACNA1G, IGF2, NEUROG1, RUNX3, and SOCS1, were considered to be CIMP-positive1.
Gene set enrichment analysis
Gene set enrichment analysis (GSEA)22 was conducted using the GSEA software (a joint project of UC San Diego, San Diego, CA, and Broad Institute, Cambridge, MA; https://www.gsea-msigdb.org/gsea/index.jsp, RRID: SCR_003199). Permutation was performed 1,000 times for each phenotype. The C2.cgp gene set (c2.cgp.v2023.1.Hs.symbols.gmt) was obtained from MSigDB23, and the other gene sets were obtained from each report24,25,26. The chip platform was set to “Human_AGILENT_Array_MSigDB.v2023.1.Hs.chip,” which is contained in the GSEA software. A nominal P-value < 0.05 and a false discovery rate (FDR) Q-value < 0.25 were considered significant.
Outcome
Overall survival (OS) was defined as the time from the date of enrollment to the date of death from any cause.
Statistical analysis
The two-sided Fisher exact and Wilcoxon rank-sum (or the Kruskal–Wallis) tests were conducted to evaluate statistical significance in patient background. OS was estimated using the Kaplan–Meier method, and statistical significance was tested using the log-rank test. Hazard ratios and their 95% confidence intervals were calculated using the Cox proportional hazards model. P < 0.05 was considered to indicate statistical significance. All statistical analyses were conducted using JMP Pro, version 16.2.0 (SAS, Cary, NC, USA).
Results
Patient characteristics
A total of 487 patients were enrolled in the TRICOLORE study. Those without consent to participate in the TR (n = 119), FFPE specimens (n = 33), or data of the RAS/BRAF mutation status or GWMS (n = 109) were excluded (Fig. 1). The patients were classified into HMCC and LMCC according to the unsupervised clustering analysis of the data from their tumor samples. Ultimately, 226 patients were included in the molecular analysis.

CONSORT diagram. From the initial cohort (n = 487), 368 (75.6%) provided consensus to the translational research. After excluding patients without FFPE specimens (n = 33) and patients without RAS/BRAF mutation status or GWMS (n = 109), 226 patients were included in this study. FFPE, formalin-fixed, paraffin-embedded.
The patients’ tumor genotypes were classified as RAS/BRAF wt (n = 125), RAS mt (n = 87), and BRAF mt (n = 14) (Table 1). The number of patients with HMCC in each genotype was 22 (17.6%), 30 (34.5%), and 14 (100%), respectively. As regards the RAS/BRAF wt genotype, the HMCC group had significantly higher proportions of tumors with deficient MMR and PTEN-negative than the LMCC group. Furthermore, PIK3CA mt tended to be more common in the HMCC than in the LMCC group, although the difference was not significant. In the RAS mt genotype, no significant difference in patient background was observed between the HMCC and LMCC groups. All tumors with BRAF mt were classified as HMCC. Regardless of the genotypes of RAS and BRAF, CIMP-positive significantly overlapped with HMCC and most of the former was included in the latter.
OS of the HMCC was shorter than that of the LMCC in the RAS/BRAF wt group
First, OS was compared in each RAS/BRAF genotype and GWMS (Fig. 2). The OS of the RAS/BRAF wt group was significantly longer than that of the RAS mt group (42.1 months vs. 28.1 months; P = 0.0004) and BRAF mt group (42.1 months vs. 16.7 months; P = 0.0001) (Fig. 2a). The OS of the RAS mt group was numerically longer than that of the BRAF mt group, but it was not statistically significant (P = 0.08). As for GWMS, the OS of the HMCC group was significantly shorter than that of the LMCC group (median, 25.1 months vs. 40.1 months; P = 0.0001) (Fig. 2b).

Kaplan–Meier survival curves for OS in each RAS/BRAF genotype and GWMS. (A) OS according to the RAS/BRAF genotype; (B) OS according to the GWMS. Abbreviations: OS, overall survival; wt, wild type; GWMS, genome-wide DNA methylation status; LMCC, low-methylated colorectal cancer; HMCC, high-methylated colorectal cancer; CI, confidence interval.
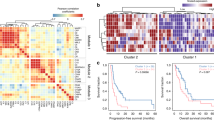
Subsequently, OS was compared between the GWMS groups in each RAS/BRAF genotype (Fig. 3). The OS of the HMCC was significantly shorter than that of the LMCC in the RAS/BRAF wt group (median, 25.3 months vs. 45.0 months; P = 0.006) but not in the RAS mt group (median, 25.4 months vs. 29.0 months; P = 0.51) (Fig. 3a, b). It is noted that the OS of the RAS/BRAF wt HMCC was comparable to that of the RAS mt group (median, 25.3 months vs. 28.1 months; P = 0.90) (Fig. 3c).

Kaplan–Meier survival curves for OS between GWMS groups in each RAS/BRAF genotype. OS according to the GWMS (LMCC or HMCC) in the RAS/BRAF wt group (A), the RAS mt group (B) and the mCRC subtypes (RAS/BRAF wt LMCC, RAS/BRAF wt HMCC, RAS mt mCRC, and BRAF mt mCRC) (C). Abbreviations: OS, overall survival; mt, mutant; wt, wild type; GWM, genome-wide methylation; LMCC, low-methylated colorectal cancer; HMCC, high-methylated colorectal cancer; CI, confidence interval; mCRC, metastatic colorectal cancer.
To identify the strong prognostic factor in the RAS/BRAF wt group and the RAS mt group, univariate and multivariate analyses were performed. In the RAS/BRAF mt group, sex, CIMP, and GWMS were significantly associated with OS (Fig. 4). Among these, only GWMS remained significant in the multivariate analysis of the RAS/BRAF wt group (Fig. 4, Supplementary Table S1). There were no significant factors in the RAS mt group (Fig. 4, Supplementary Table S2). These results indicate that GWMS affects the prognosis of mCRC in the RAS/BRAF wt group.

Univariate and multivariate analysis on OS in RAS/BRAF wt or mt patients. Forest plot of the HR on OS from univariate or multivariate analysis in the indicated subgroup. *P < 0.05. Abbreviations: PS, Eastern Cooperative Oncology Group performance status; MMR, mismatch repair; CIMP, CpG island methylator phenotype; GWMS, genome-wide DNA methylation status; OX, mFOLFOX6/CapeOX plus bevacizumab; IRI, S-1 and irinotecan plus bevacizumab; LMCC, low-methylated colorectal cancer; HMCC, high-methylated colorectal cancer; OS, overall survival; HR, hazard ratio; wt, wild type; mt, mutant.
HMCC in the RAS/BRAF wt group exhibits a gene expression pattern related to MSI-high, BRAF V600E , and anti-EGFR antibody resistance
To elucidate the molecular difference between HMCC and LMCC in the RAS/BRAF wt genotype, GSEA was conducted (n = 125) (Table 2). Analysis of the C2.cgp database, which represents the expression signatures of genetic and chemical perturbations, revealed that the gene set upregulated in microsatellite instability-high (MSI-H) CRC compared with microsatellite-stable (MSS) CRC27 was significantly enriched in RAS/BRAF wt HMCC at the top score among 3,405 gene sets in the database (Supplementary Table S3). Conversely, the gene set downregulated in MSI-H CRC compared with MSS CRC was significantly enriched in RAS/BRAF wt LMCC (Supplementary Table S4). Furthermore, GSEA using other gene sets altered in MSI-H CRC26 showed that RAS/BRAF wt HMCC and RAS/BRAF wt LMCC were enriched for genes up- and down-regulated in MSI-H tumors, respectively. The analyzed population includes patients with mismatch repair-deficient (dMMR) CRC (n = 4). Even after excluding patients with dMMR, similar findings were observed (Supplementary Table S5).
Both hypermethylated CRC and MSI-H CRC are correlated with BRAFV600E mutation1,12. Thus, we checked the correlation between HMCC in the RAS/BRAF wt group and CRC with BRAFV600E mutation via GSEA (Table 3). The gene set upregulated in BRAFV600E CRC compared with BRAF wt CRC25 was significantly enriched in RAS/BRAF wt HMCC.
GWMS is correlated with anti-EGFR antibody sensitivity4; therefore, GSEA was conducted in the RAS/BRAF wt group (n = 125) using gene sets related to cetuximab response24. The gene set upregulated in cetuximab-responding patient-derived xenograft (PDX) in the report was significantly enriched in RAS/BRAF wt LMCC, whereas the gene set upregulated in nonresponding PDX exhibited potential enrichment in RAS/BRAF wt HMCC (Table 3). A similar trend was observed in the total cohort, excluding patients with RAS mt and BRAF mt (n = 226; Supplementary Table S6).
Discussion
We analyzed the prognostic value of GWMS across RAS/BRAF genotypes in a prospective cohort of mCRC and found that GWMS was a prognostic factor only in RAS/BRAF wt mCRC. Notably, multivariate analyses of OS among patients with RAS/BRAF wt mCRC showed that HMCC was a significant prognostic factor, whereas CIMP-positivity was not, suggesting that GWMS captures a clinically aggressive epigenetic phenotype beyond conventional CIMP classification in this population. Moreover, GSEA revealed that the gene expression pattern of RAS/BRAF wt HMCC was associated with MSI-high status, BRAFV600E mutation, and resistance to anti-EGFR antibodies. These findings could partially explain the molecular mechanism of the poor prognosis of RAS/BRAF wt HMCC.
mCRC with high DNA methylation status is associated with poor prognosis7,8,9. The present study further showed that the poor prognosis of HMCC compared with LMCC was observed only in RAS/BRAF wt mCRC patients. Therefore, we focused on this group.
Metastatic and recurrent dMMR CRC has a poorer prognosis than pMMR CRC28. In our cohort, the gene sets up- and down-regulated in MSI-H CRC were enriched in RAS/BRAF wt HMCC and RAS/BRAF wt LMCC, respectively. These symmetrical characteristics suggest that gene expression patterns between GWMS4 and MSI27 are similar. Thus, the poor prognosis of RAS/BRAF wt HMCC could be attributed to this similarity. Since HMCC exhibited gene expression patterns similar to those of MSI-H CRC, even when patients with dMMR were excluded from the analysis, GWMS may identify a broader range of MSI-H CRC and MSI-H-like CRC than IHC of MMR-related proteins.
The similarity between RAS/BRAF wt HMCC and MSI-H CRC may also indicate the importance of GWMS in predicting the treatment response to immune checkpoint inhibitors (ICIs). In the KEYNOTE-177 trial, pembrolizumab or chemotherapy was administered to patients with metastatic MSI-H CRC29. In a multivariate analysis of PFS, pembrolizumab was preferred in the right-sided CRC subgroup but not in the left-sided CRC subgroup. As HMCC frequently occurs in the right-sided colon4, the improvement of PFS in the right-sided CRC subgroup may be attributable to HMCC. Thus, HMCC could be a positive predictor for the treatment effect of ICI in the future.
Moreover, the RAS/BRAF wt HMCC was similar to BRAFV600E CRC in the gene expression profiles. Because BRAFV600E is a well-known poor prognostic factor in CRC, this similarity in gene expression profile may partially explain the poor prognosis in this group.
The anti-EGFR antibody resistance of RAS/BRAF wt HMCC could be attributed to a gene expression pattern similar to that of BRAFV600E CRC. In this study, the gene set related to cetuximab response in CRC, the cetuximab signature24, was correlated with GWMS. In LMCC and HMCC, genes for the cetuximab responder and non-responder were enriched, respectively. The gene set of the cetuximab was created using PDX including RAS and BRAF mutants, according to their response to cetuximab. These driver mutations were frequently seen in PDXs not responding to cetuximab compared to those responding to cetuximab. Thus, non-responder gene set in cetuximab signature could potentially include genes upregulated by RAS or BRAF mutation. Moreover, mCRC is known to be anti-EGFR antibody-resistant partially due to the aberrant activation of the mitogen-activated protein kinase (MAPK) pathway30. Therefore, RAS/BRAF wt HMCC was expected to have a gene expression pattern related to MAPK pathway activation. However, GSEA failed to detect such enrichments in HMCC using the gene sets related to the MAPK pathway and RAS-mutated CRC (data not shown). Thus, the type of alterations in gene expression that causes these similarities should be determined in the future.
As for the RAS/BRAF wt LMCC, the good OS in our cohort could be due to the therapeutic effect of anti-EGFR antibodies in the later line after the first-line regimens containing either oxaliplatin or irinotecan. Although RAS/BRAF wt HMCC is reportedly anti-EGFR antibody-resistant in the later line compared with RAS/BRAF wt LMCC and has a poor prognosis4,31, similar to RAS and BRAF mt mCRC32,33,34, some patients in our cohort received anti-EGFR antibody treatment regardless of their GWMS. Thus, the different anti-EGFR antibody responses across GWMS may have affected prognosis in the RAS/BRAF wt group. However, the number of patients who were administered anti-EGFR antibodies was too small to conduct a statistical analysis. Therefore, the speculation that differences in anti-EGFR antibody responses may have affected OS in our cohort remains a hypothesis (data not shown).
This study has some limitations. First, the population was limited to Japanese patients, and the number of patients is small. Additionally, the analyzed population comprised 226 of 487 patients enrolled in the TRICOLORE trial. This could lead to selection bias influencing treatment outcomes and prognosis; patients with resected samples tended to have good performance status and thus were more likely to undergo surgery, which could result in better OS, for example. Second, the molecular mechanism was deduced via GSEA based on statistical inference; therefore, more evidence such as transcriptomic data from other cohorts, multiomics analysis, and in vitro experiments, is necessary to confirm the logic. Third, patients with RAS mutations were treated as a single group due to the small sample size, although they should be analyzed in each specific mutation group, given the recent development of RAS inhibitors for mCRC treatment.
In conclusion, we demonstrated that RAS/BRAF wt HMCC is a poor prognostic factor in mCRC. Its gene expression pattern is associated with that of MSI-H and BRAFV600E mutation, which could play a role in its cetuximab resistance.
Data availability
The microarray data are publicly available in Gene Expression Omnibus (GEO; [https://www.ncbi.nlm.nih.gov/geo/], RRID: SCR\_005012) at GSE147571. Other data generated in this study are available from the corresponding author upon reasonable request.
References
Weisenberger, D. J. et al. CpG island methylator phenotype underlies sporadic microsatellite instability and is tightly associated with BRAF mutation in colorectal cancer. Nat. Genet. 38(7), 787–93 (2006).
Pino, M. S. & Chung, D. C. The chromosomal instability pathway in colon cancer. Gastroenterology 138(6), 2059–72 (2010).
Boland, C. R. & Goel, A. Microsatellite instability in colorectal cancer. Gastroenterology 138(6), 2073-2087.e3 (2010).
Ouchi, K. et al. DNA methylation status as a biomarker of anti-epidermal growth factor receptor treatment for metastatic colorectal cancer. Cancer Sci. 106(12), 1722–9 (2015).
Toyota, M. et al. CpG island methylator phenotype in colorectal cancer. Proc. Natl. Acad. Sci. U. S. A. 96(15), 8681–6 (1999).
Ogino, S. et al. CpG island methylator phenotype (CIMP) of colorectal cancer is best characterised by quantitative DNA methylation analysis and prospective cohort studies. Gut 55(7), 1000–6 (2006).
Shen, L. et al. Association between DNA methylation and shortened survival in patients with advanced colorectal cancer treated with 5-fluorouracil based chemotherapy. Clin. Cancer Res. 13(20), 6093–8 (2007).
Chen, K. H. et al. CpG Island methylator phenotype may predict poor overall survival of patients with stage iv colorectal cancer. Oncology 96(3), 156–163 (2019).
Cha, Y. et al. Adverse prognostic impact of the CpG island methylator phenotype in metastatic colorectal cancer. Br. J. Cancer 115(2), 164–71 (2016).
Juo, Y. Y. et al. Prognostic value of CpG island methylator phenotype among colorectal cancer patients: A systematic review and meta-analysis. Ann. Oncol. 25(12), 2314–2327 (2014).
Osumi, H. et al. Effect of DNA methylation status on first-line anti-epidermal growth factor receptor treatment in patients with metastatic colorectal cancer. Int. J. Colorectal Dis. 37(6), 1439–1447 (2022).
Wakayama, S. et al. TP53 gain-of-function mutation is a poor prognostic factor in high-methylated metastatic colorectal cancer. Clin. Colorectal Cancer 22(3), 327–338 (2023).
Ishioka, C. Harnessing epigenetics: Genome-wide DNA methylation assay for colorectal cancer therapy. Cancer Treat. Rev. 143, 103062 (2025).
Yamada, Y. et al. S-1 and irinotecan plus bevacizumab versus mFOLFOX6 or CapeOX plus bevacizumab as first-line treatment in patients with metastatic colorectal cancer (TRICOLORE): A randomized, open-label, phase III, noninferiority trial. Ann. Oncol. 29(3), 624–631 (2018).
Denda, T. et al. Combination therapy of bevacizumab with either S-1 and irinotecan or mFOLFOX6/CapeOX as first-line treatment of metastatic colorectal cancer (TRICOLORE): Exploratory analysis of RAS status and primary tumour location in a randomised, open-label, phase III, non-inferiority trial. Eur. J. Cancer 154, 296–306 (2021).
Takahashi, S. et al. Advanced colorectal cancer subtypes (aCRCS) help select oxaliplatin-based or irinotecan-based therapy for colorectal cancer. Cancer Sci. 112(4), 1567–1578 (2021).
Soeda, H. et al. KRAS mutation in patients with metastatic colorectal cancer does not preclude benefit from oxaliplatin-or irinotecan-based treatment. Mol. Clin. Oncol. 2(3), 356–362 (2014).
Soeda, H. et al. Phase II trial of cetuximab plus irinotecan for oxaliplatin- and irinotecan-based chemotherapy-refractory patients with advanced and/or metastatic colorectal cancer: Evaluation of efficacy and safety based on KRAS mutation status (T-CORE0801). Oncology 87(1), 7–20 (2014).
Inoue, M. et al. Gene-expression profiles correlate with the efficacy of anti-EGFR therapy and chemotherapy for colorectal cancer. Int. J. Clin. Oncol. 20(6), 1147–55 (2015).
Guinney, J. et al. The consensus molecular subtypes of colorectal cancer. Nat. Med. 21(11), 1350–6 (2015).
Okita, A. et al. Consensus molecular subtypes classification of colorectal cancer as a predictive factor for chemotherapeutic efficacy against metastatic colorectal cancer. Oncotarget 9(27), 18698–18711 (2018).
Subramanian, A. et al. Gene set enrichment analysis: A knowledge-based approach for interpreting genome-wide expression profiles. Proc. Natl. Acad. Sci. 102(43), 15545–15550 (2005).
Liberzon, A. et al. Molecular signatures database (MSigDB) 3.0. Bioinformatics 27(12), 1739–1740 (2011).
Schütte, M. et al. Molecular dissection of colorectal cancer in pre-clinical models identifies biomarkers predicting sensitivity to EGFR inhibitors. Nat. Commun. 8(1), 14262 (2017).
Popovici, V. et al. Identification of a poor-prognosis BRAF-mutant-like population of patients with colon cancer. J. Clin. Oncol. 30(12), 1288–95 (2012).
Tian, S. et al. A robust genomic signature for the detection of colorectal cancer patients with microsatellite instability phenotype and high mutation frequency. J. Pathol. 228(4), 586–95 (2012).
Watanabe, T. et al. Distal colorectal cancers with microsatellite instability (MSI) display distinct gene expression profiles that are different from proximal MSI cancers. Cancer Res. 66(20), 9804–9808 (2006).
Koopman, M. et al. Deficient mismatch repair system in patients with sporadic advanced colorectal cancer. Br. J. Cancer 100(2), 266–273 (2009).
André, T. et al. Pembrolizumab in Microsatellite-instability–high advanced colorectal cancer. New Engl. J. Med. 383(23), 2207–2218 (2020).
Beekhof, R. et al. Phosphoproteomics of patient-derived xenografts identifies targets and markers associated with sensitivity and resistance to EGFR blockade in colorectal cancer. Sci. Transl. Med. 15(709), eabm3687 (2023).
Ouchi, K. et al. A modified MethyLight assay predicts the clinical outcomes of anti-epidermal growth factor receptor treatment in metastatic colorectal cancer. Cancer Sci. 113(3), 1057–1068 (2022).
Soeda, H. et al. Clinical usefulness of KRAS, BRAF, and PIK3CA mutations as predictive markers of cetuximab efficacy in irinotecan- and oxaliplatin-refractory Japanese patients with metastatic colorectal cancer. Int. J. Clin. Oncol. 18(4), 670–677 (2013).
LièVre, A. et al. KRAS mutation status is predictive of response to cetuximab therapy in colorectal cancer. Cancer Res. 66(8), 3992–3995 (2006).
Di Nicolantonio, F. et al. Wild-type BRAF is required for response to panitumumab or cetuximab in metastatic colorectal cancer. J. Clin. Oncol. 26(35), 5705–5712 (2008).
Acknowledgments
The authors thank all the patients, their families, the medical staff who participated in this study, especially Ms. Hiromi Nakano, and the Tokyo Cooperative Oncology Group (TCOG) for their cooperation with the TRICOLORE study data.
Funding
The roles of funding source are as follows: Tokyo Cooperative Oncology Group was involved in the design and conduct of the study. However, the sponsors had no role in the collection, management, analysis, and interpretation of the data, the preparation of the manuscript, or the decision to submit the manuscript for publication. This work was supported by the Tokyo Cooperative Oncology Group with funding from Taiho Pharmaceutical Co. Ltd., Japan [no grant number] under the study contract, and partly supported by a grant from the Project for Development of Innovative Research on Cancer Therapeutics (P-DIRECT) [grant number 11110018], the Project for Cancer Research and Therapeutic Evolution (P-CREATE) by the Japan Agency for Medical Research and Development [grant number 16770660], and the Japan Society for the Promotion of Science, Grants-in-Aid for Scientific Research (Grant Number JP25K10554).
Author information
Authors and Affiliations
Contributions
ST, CI: conception and design, provision of study patients and study materials and data interpretation and paper writing; SW: data interpretation, paper writing and statistical analysis; KO experimental working and data interpretation and paper writing; YK, TY, KS, AS, SY: conception and design, provision of study patients and study materials and paper review; YS, TD, AT, MN, HO, YK, HB, MK, KA, HK: provision of study patients and study materials, data interpretation and paper review; AO, KK, MW: experimental working and data interpretation; SM: conception and design and statistical analysis.
Corresponding author
Ethics declarations
Competing interests
Dr. Shin Takahashi reports honoraria from Taiho, Chugai, Asahi Kasei, Bristol-Myers Squibb, Bayer, Japan blood products organization, Medicon, Takeda, Yakult, and Daiichi Sankyo, Eli Lilly, Eisai, and grants and personal fees from Merck Biopharma and Ono, outside the submitted work; Prof. Yoshito Komatsu reports grants and personal fees from Taiho, grants and personal fees from Chugai, personal fees from Takeda, grants and personal fees from Bayer, grants and personal fees from Sanofi, grants and personal fees from Ono, grants from MSD, grants and personal fees from Yakult, grants from NanoCarrier, grants from QuintilesIMS, grants from Sysmex, grants and personal fees from Mediscience planning, grants from Dainippon Sumitomo Pharma, personal fees from Kyowa Kirin, personal fees from Asahi Kasei, grants from Nippon Zoki Pharmaceutical, grants from A2 Healthcare, grants and personal fees from Daiichi Sankyo, grants from Eisai, grants from Parexel International, grants from Astellas, grants from Incyte, grants from Syneos health clinical, personal fees from Eli Lilly, personal fees from Nipro, personal fees from Bristol-Myers Squibb, personal fees from Moroo, personal fees from Pfizer, personal fees from Merck Biopharma, personal fees from Medical Review, personal fees from Mitsubishi Tanabe Pharma, personal fees from Nippon Kayaku, personal fees from Shire Japan, personal fees from Novartis, personal fees from Otsuka Pharmaceutical Factory, personal fees from 3H Medi Solution, grants from Shionogi, grants from ShiftZero, outside the submitted work; Dr. Atsushi Sato reports research grants from Chugai, Taiho, and Daiichi-Sankyo, and honoraria from Chugai and Taiho, outside the submitted work; Dr. Satoshi Yuki reports honoraria from Chugai Pharmaceutical, Eli Lilly, Takeda Pharmaceutical, Bayer Yakuhin, Bristol-Myers Squibb, Taiho Pharmaceutical, MSD, Ono Pharmaceutical, Merck Biopharma and Miyarisan Pharmaceutical, outside the submitted work; Dr. Ken Shimada reports honoraria from Taiho, Chugai, Yakult, Bristol-Myers Squibb, Takeda, Merck Biopharma and Eli Lilly, and grants and personal fees from Taiho, Chugai, and Ono, outside the submitted work; Prof. Yasuhide Yamada reports research grants from Chugai and honoraria from Janssen, Behringer-Ingelheim, Taiho, Ono outside the submitted work; Prof. Chikashi Ishioka reports research funds from Hitachi and Riken Genesis and research grants from Chugai, Taiho, Asahi Kasei, Daiichi-Sankyo, Takeda, and Ono and honoraria from Chugai and Daiichi-Sankyo, outside the submitted work.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Wakayama, S., Takahashi, S., Ouchi, K. et al. RAS/BRAF wild-type metastatic high-methylated colorectal cancer has gene expression patterns related to MSI-H and BRAF V600E mutant: a translational research. Sci Rep 16, 12566 (2026). https://doi.org/10.1038/s41598-026-42033-w
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-026-42033-w
