
Abstract
The effect of hypertension on cardiovascular disease is increasingly evident, but the effect of hypertension with chronic medical conditions on adverse outcomes is less clear. To explore the minimum threshold range of target systolic blood pressure (SBP) in hypertensive population with comorbidities. A total of 11,388 hypertensive participants with comorbidities in the Kailuan cohort were selected. Propensity score matching (PSM) was also conducted among the 27,541 participants who suffered from hypertension without comorbidities and had received a physical examination in the same period. Finally, totaling 22,546 participants. After a follow-up of more than 7 years, the occurrence rate of CVD events in hypertensive participants with comorbidities was the minimum in the 110 ≤ SBP < 120 mm Hg group; the occurrence rate of CVD events in hypertensive participants without comorbidities was the minimum in the SBP < 110 mm Hg group; the all-cause mortality in participants with comorbidities and without comorbidities were the minimum in the 120 ≤ SBP < 130 mm Hg group. The results of the time-dependent Cox model and death competition risk model used in the two groups were consistent with those of the master model. The ideal post-treatment SBP in participants with comorbidities should be individualized. If the patient has a short life expectancy, his/her post-treatment SBP should be kept at 120 to 130 mm Hg. If the patient has a long life expectancy, his/her post-treatment SBP should be kept at 110 to 120 mm Hg.
Similar content being viewed by others

Introduction
Globally, the prevalence of hypertension ranges from 22% to 31%1. Among the Chinese population, the prevalence of hypertension is 28%2. Most individuals with hypertension also suffer from comorbidities, including diabetes mellitus (DM), chronic kidney disease (CKD), malignant tumors, and chronic obstructive pulmonary disease (COPD)3. Both the prevalence of hypertension and comorbidities increase with age, and, due to increasing life expectancy, the prevalence of hypertension with comorbidities is also expected to rise4. The interaction between advanced age, comorbidities, and medications used to treat these comorbidities may not only increase the risk of adverse events in hypertensive patients but also complicate the management of hypertension. Since there is a U-shaped relationship between post-treatment systolic blood pressure (SBP) and adverse outcomes in hypertensive patients with comorbid DM and CKD, it is necessary to explore the minimum threshold range of SBP in hypertensive patients with comorbidities.
Although various guidelines for the treatment of hypertension provide target blood pressure values for initiating treatment in hypertensive patients, the minimum threshold range of target SBP has not yet been clearly defined. Only the ESC (European Society of Cardiology) guidelines explicitly state that 120/70 mm Hg is the minimum safety threshold for target SBP, emphasizing that SBP should not be lower than 120 mm Hg5. For elderly participants with comorbidities, the American College of Cardiology (ACC)/American Heart Association (AHA) guidelines offer general recommendations but do not specify a minimum threshold for target SBP6. These guidelines are based on evidence from randomized controlled trials (RCTs), which often exclude patients with comorbidities. In the real world, however, studies have shown that two-thirds of individuals with hypertension suffer from more than one comorbidity7. Due to the lack of a unified minimum threshold range of target SBP for hypertensive patients with comorbidities, physicians and patients often face uncertainty when making treatment decisions. To address this clinical gap and complement the limitations of RCTs, we analyzed real-world data (RWD) to examine the impact of different post-treatment SBP levels on cardiovascular disease (CVD) events and all-cause mortality in hypertensive patients with comorbidities. Additionally, we present an in-depth discussion on the minimum threshold range of target SBP for hypertensive patients with comorbidities.
Data and methods
Participants
The participants in this study were drawn from the population of the Kailuan study (registration No.: ChiCTR-TNRC-11001489). The Kailuan study began in 2006, with follow-up conducted every two years. To date, six follow-up assessments have been completed. New cardiovascular disease (CVD) events and all-cause deaths were confirmed annually. All participants in the Kailuan study are covered by medical insurance. According to relevant regulations, individuals with 34 specified diseases—including hypertension, diabetes mellitus (DM), stroke, coronary heart disease (CHD), liver disease, kidney disease, chronic obstructive pulmonary disease (COPD), pulmonary heart disease, tumors, rheumatoid disease, mental disorders, myasthenia gravis (MG), Parkinson’s disease (PD), and aplastic anemia—receive healthcare through dedicated outpatient services for chronic diseases and benefit from higher medical insurance reimbursement rates.
Since 2010, the electronic medical record (EMR) system has been implemented in the outpatient clinics for chronic diseases. Although the Kailuan study commenced in 2006, the diagnosis of comorbidities prior to 2010 was based solely on self-reported questionnaires, which may be subject to recall bias. Therefore, to ensure the accuracy of comorbidity information, we included only participants who had detailed comorbidity diagnoses and medication records from the chronic disease outpatient EMR system after its implementation in 2010. The baseline physical examination data for these participants could be derived from any examination round between 2006 and 2021, but the key inclusion criterion was the availability of post-2010 EMR data for comorbidities. For this study, we selected hypertensive patients with at least one chronic disease who were taking antihypertensive medications and receiving care at these dedicated outpatient clinics. We matched these patients with hypertensive individuals without comorbidities who were also on antihypertensive medications and receiving care at general outpatient clinics. This matching process allowed us to observe the impact of different post-treatment systolic blood pressure (SBP) levels (when integrated into chronic disease management) on adverse outcomes in hypertensive patients with comorbidities.
This study was approved by the Medical Ethics Committee of Kailuan General Hospital ([2006] YLZ No. 5), and all participants provided written informed consent.
Inclusion Criteria
The inclusion criteria for this study were as follows ① Participants from the population of the Kailuan study; ② Participants who had hypertension with comorbidities and sought diagnosis and treatment in the outpatient clinics for chronic diseases from 2010 to 2021; ③ Participants who had simple hypertension and received a physical examination during the same period as those with comorbid hypertension (to serve as the control group). This study adhered to the principles of the Declaration of Helsinki and was approved by the Ethics Committee of Kailuan Medical Group ([2006] No. 5).
Exclusion Criteria
Hypertensive participants who were diagnosed with ischemic heart disease (IHD) and/or stroke were excluded from the study, as the adverse outcomes being observed included IHD and stroke.
Data collection
Collection of Baseline Data
The survey contents, anthropometric indicators, and biochemical indicators of the Kailuan study are detailed in the published articles (8–10) by our research group. Physical examination data collected during the same period for the diagnosis of chronic diseases were used as reference data. If relevant data from that period were missing, previous physical examination data, recorded prior to the diagnosis of chronic diseases, were used as baseline data. Data on the diagnosis and medication of chronic diseases were obtained from outpatient electronic medical records. Information on the medication of hypertensive participants without comorbidities was collected through a questionnaire survey conducted during their physical examination. Medication information for each comorbidity was extracted from the chronic disease outpatient electronic medical records. To provide therapeutic context, we compiled lists of the top six most frequently prescribed medications for each of the five major comorbidities (diabetes mellitus, tumors, chronic kidney disease, liver disease, and COPD/cor pulmonale) based on chronic disease outpatient prescription data. These lists are presented in eTable 12.
Blood Pressure Measurement
Blood pressure measurements were taken between 7:00 and 9:00 a.m. on the day of the physical examination. Specifically, blood pressure was measured at the right brachial artery using a calibrated desktop mercury sphygmomanometer. Beginning with the fourth follow-up (2014 to 2015), the blood pressure measurement method was standardized to the use of the Omron HBP-1300 Medical Electronic Sphygmomanometer.
Relevant definitions
Hypertension is defined as a systolic blood pressure (SBP) ≥ 140 mm Hg and/or diastolic blood pressure (DBP) ≥ 90 mm Hg, or as self-reported hypertension diagnosis, or the use of antihypertensive drugs.
Hypertension with comorbidities refers to a hypertensive patient who is diagnosed with more than one of the 34 chronic diseases listed above (excluding coronary heart disease [CHD] and stroke).
Hypertension without comorbidities refers to a hypertensive patient who does not exhibit target organ damage (as indicated by negative urine protein and the absence of left ventricular hypertrophy [LVH] in electrocardiogram [ECG]) and is not complicated by any chronic disease.
Diabetes mellitus (DM) is defined as a fasting blood glucose (FBG) level ≥ 7.0 mmol/L, a self-reported history of DM, or the use of hypoglycemic drugs.
The diagnostic criteria for other chronic diseases are listed in the attached table.
Smoking is defined as smoking at least one cigarette per day on average for the past year.
Drinking is defined as consuming an average of 100 mL of liquor (with an alcohol content of > 50%) per day for at least one year.
Physical exercise is defined as engaging in exercise at least three times per week, with each session lasting ≥ 30 min.
Follow-up and outcomes
The start of the observation period for hypertensive participants with comorbidities was the time at which they were initially diagnosed with chronic diseases. For participants without comorbidities, the observation period began when the matched participants with comorbidities were diagnosed with chronic diseases.
De novo cardiovascular disease (CVD) events and all-cause mortality were considered adverse outcomes. CVD events included both fatal and nonfatal myocardial infarction (MI) (ICD-10 code: I21), cerebral infarction (ICD-10 code: I63), cerebral hemorrhage (ICD-10 code: I61), and subarachnoid hemorrhage (SAH) (ICD-10 code: I60).
For participants in whom no endpoint event occurred, December 31, 2021, was taken as the endpoint for follow-up.
Statistical analysis
Statistical analysis was performed using SAS 9.4 software. For normally distributed measurement data, values are expressed as mean ± standard deviation (± s), and comparisons among groups were conducted using analysis of variance (ANOVA). For measurement data with a skewed distribution, values are expressed as median (interquartile range). Enumeration data are presented as composition ratios, and group comparisons were performed using the chi-squared (χ²) test.
Hypertensive participants with and without comorbidities were matched using the propensity score matching (PSM) method. The dependent variable was the presence or absence of comorbidities, and the PSM model included age, gender, and history of hypertension as covariates. Propensity scores were calculated through logistic regression analysis. Participants with similar propensity scores in both groups were matched in a 1:1 ratio using the best neighborhood matching (BNM) method (caliper value: 0.2). To ensure accurate matching, any matched participants who developed comorbidities during the follow-up period were excluded, and re-matching was performed.
Based on baseline systolic blood pressure (SBP), participants were categorized into the following groups: SBP < 110 mm Hg, 110 ≤ SBP < 120 mm Hg, 120 ≤ SBP < 130 mm Hg, 130 ≤ SBP < 140 mm Hg, 140 ≤ SBP < 160 mm Hg, and SBP ≥ 160 mm Hg. The incidence density of de novo cardiovascular disease (CVD) events and all-cause mortality in these groups was calculated using the life table method. A log-rank test was performed to compare the incidence densities of adverse events among the groups. The proportional hazards (APH) assumption was tested for verification.
The 110 ≤ SBP < 120 mm Hg group and the 120 ≤ SBP < 130 mm Hg group, which had the lowest incidence rates of CVD and mortality events, were used as reference groups. A Cox proportional hazards (PH) model was used to analyze the effects of post-treatment SBP on adverse events in participants with and without comorbidities. The 5th, 35th, 65th, and 95th percentiles of SBP were selected for analysis using a restricted cubic spline plot.
To compare the effects of the same post-treatment SBP level on adverse outcomes in participants with and without comorbidities, a Cox PH model analysis was conducted on the total matched population. Considering the dynamic changes in blood pressure during the follow-up period, time-dependent Cox regression analysis was performed to observe the effects of blood pressure changes on adverse outcomes.
To address the potential heterogeneity arising from the inclusion of multiple comorbidity types, we performed sensitivity analyses focusing on participants with the five most prevalent comorbidities (diabetes mellitus, tumors, chronic kidney disease, liver disease, and COPD/cor pulmonale). We also conducted additional sensitivity analyses by sequentially excluding each of these five comorbidities from the comorbid population and re-evaluating the associations between SBP categories and adverse outcomes. To address concerns about potential reverse causality—where very low SBP might reflect poor health status rather than intentional intensive treatment—we performed sensitivity analyses by sequentially excluding participants with markers of poor health, including low BMI (< 17 kg/m²), anemia (hemoglobin < 120 g/L in men and < 110 g/L in women), elevated hs-CRP (≥ 15 mg/L), and malignancy. We then re-evaluated the associations between post-treatment SBP categories and adverse outcomes in each excluded population. To further explore the potential confounding effect of antihypertensive treatment intensity, we categorized participants into three intensity groups based on the number and combination of antihypertensive medications: low-intensity (monotherapy or dual combination of β-blockers and diuretics), moderate-intensity (other dual combinations excluding β-blockers plus diuretics, or triple combinations including both β-blockers and diuretics), and high-intensity (triple or more combinations not simultaneously including β-blockers and diuretics). We then re-evaluated the associations between post-treatment SBP categories and adverse outcomes within each treatment intensity stratum. To account for the potential effects of age and the number of comorbidities on adverse outcomes, a subgroup analysis was conducted based on age (≥ 65 years and ≥ 80 years) and the number of comorbidities (≥ 3). Given the relatively large number of deaths, a competing risks analysis was conducted for the death outcome. A two-sided test was performed, and differences were considered statistically significant if P < 0.05.
Results
General information of observation objects
From 2010 to 2021, a total of 20,600 participants from the Kailuan cohort sought diagnosis and treatment at the outpatient clinics for chronic diseases. After excluding 6,264 participants diagnosed with chronic diseases due to cardiovascular disease (CVD) events and 2,948 non-hypertensive participants, a total of 11,388 hypertensive participants with comorbidities remained. Of these, 11,273 participants were successfully matched using the propensity score matching (PSM) method with 27,541 participants without comorbidities who received follow-up during the same period. After matching, the total number of participants was 22,546. The flowchart is shown in Fig. 1, and the general information is provided in Table 1.

Flowchart.
After matching, the mean age of participants with comorbidities was 60.49 ± 9.36 years, with 9,027 (80.08%) males. The most common comorbidity was diabetes mellitus (DM) [7,822 (69.39%)], followed by tumors [1,364 (12.10%)]. A total of 8,254 participants (73.22%) had fewer than three comorbidities, while 3,019 participants (26.78%) had more than three comorbidities. The mean systolic blood pressure (SBP) was 147.03 ± 20.87 mm Hg. Other baseline data are shown in eTables 1 and 2. After matching, the mean age of participants without comorbidities was 60.62 ± 10.31 years, with 8,982 (79.68%) males. The mean SBP was 147.09 ± 19.88 mm Hg. Other baseline data are shown in eTable 3.
Main results
The mean follow-up times for hypertensive participants with and without comorbidities were 7.10 ± 4.13 and 7.38 ± 3.94 years, respectively. The occurrence rate of cardiovascular disease (CVD) events in participants with comorbidities was lowest in the 110 ≤ SBP < 120 mm Hg group, while the occurrence rate in participants without comorbidities was lowest in the SBP < 110 mm Hg group. All-cause mortality was lowest in the 120 ≤ SBP < 130 mm Hg group.
A multivariate Cox regression analysis was conducted with de-novo CVD events as the dependent variable, different SBP groups as the independent variables, and the 110 ≤ SBP < 120 mm Hg group as the reference category. The results indicated that the risk of onset increased in all groups except for a non-statistically significant increase in the SBP < 110 mm Hg group among participants with comorbidities. Among participants without comorbidities, the risk of onset only increased in the SBP ≥ 160 mm Hg group.
The results of the time-dependent Cox model and the competing risks model for death were consistent with those of the main Cox model. When myocardial infarction (MI) was used as the dependent variable, the risk of onset only increased in the SBP ≥ 160 mm Hg group among participants with comorbidities, while no statistically significant results were observed in participants without comorbidities across all SBP groups. For stroke, the onset risk in both participants with and without comorbidities followed the same pattern as that for CVD events.
When all-cause mortality was used as the dependent variable, and the 120 ≤ SBP < 130 mm Hg group was used as the reference, no significant increase in mortality risk was observed when the blood pressure of participants with comorbidities was lower than this value. Among the participants with comorbidities, the mortality risk significantly increased only in the SBP ≥ 160 mm Hg group, as shown in Tables 2 and 3 and eTable 4.
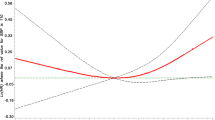
A restricted cubic spline plot was used for participants with and without comorbidities, with the 5th, 35th, 65th, and 95th percentiles of SBP selected for analysis. The nonlinear hypothesis test for participants with and without comorbidities revealed that P > 0.05, as shown in Fig. 2.

SBP was used as the independent variable, with CVD events, myocardial infarction, stroke, and all-cause death as dependent variables in the comorbidity(A、B、C and D) and non-comorbidity(E、F、G and H) groups, respectively, and with a median SBP of 145.33 as the reference. We adjusted for age, sex, BMI, fasting blood glucose, triglyceride, low-density lipoprotein, high-density lipoprotein, high-sensitivity C-reactive protein, hemoglobin, duration of hypertension, smoking, alcohol consumption, and physical activity.There were 11,273 participants.
To compare the effects of the same post-treatment systolic blood pressure (SBP) levels on adverse outcomes in participants with and without comorbidities, a multivariate Cox regression analysis was conducted on the total matched cohort of 22,546 participants. Using the 110 ≤ SBP < 120 mm Hg group (representing participants without comorbid hypertension) as the control, the risk of cardiovascular disease (CVD) and myocardial infarction (MI) in participants with comorbidities increased significantly in all groups. When the 120 ≤ SBP < 130 mm Hg group (representing participants without comorbidities) was used as the control, the risk of all-cause death in participants with comorbidities increased significantly in all SBP groups. See eTable 5 and Fig. 3.

Multivariate cox models with CVD events, myocardial infarction, stroke, and death from any cause as dependent variables and with adjustment for age, sex, BMI, fasting plasma glucose, triglycerides, low-density lipoprotein, high-density lipoprotein, high-sensitivity C-reactive protein, hemoglobin, duration of hypertension, smoking, alcohol consumption, and physical activity, respectively.There were 22,546 participants.
Sensitivity analyses
To further evaluate the robustness of our findings, we performed several sensitivity analyses. First, we restricted the analysis to participants with the five most prevalent comorbidities (diabetes mellitus, tumors, chronic kidney disease, liver disease, and COPD/cor pulmonale), which comprised 10,290 individuals (91.3% of the comorbid cohort). The results were consistent with the main analysis: the lowest risk for CVD events remained in the 110 ≤ SBP < 120 mm Hg group, and the lowest risk for all-cause mortality remained in the 120 ≤ SBP < 130 mm Hg group (eTable 9).
Second, we sequentially excluded each of these five comorbidities from the comorbid population. Regardless of whether participants with diabetes mellitus (n = 3,451 remaining), cancer (n = 9,384 remaining), kidney disease (n = 10,863 remaining), liver disease (n = 10,917 remaining), or COPD/pulmonary heart disease (n = 10,935 remaining) were excluded, the results remained consistent with the main analysis: the lowest risk for CVD events was consistently observed in the 110 ≤ SBP < 120 mm Hg group, and the lowest risk for all-cause mortality was consistently observed in the 120 ≤ SBP < 130 mm Hg group in all these sensitivity analyses (eTable 6).
Finally, to address potential reverse causality, we excluded participants with markers of poor health. After excluding participants with low BMI, anemia, elevated hs-CRP, and malignancy, the results remained consistent with the main analysis (eTable 11).
Subgroup analyses
The results of the multivariate Cox regression analysis for participants with fewer than three comorbidities were generally consistent with those for the overall population. Among participants with three or more comorbidities, the risk of cardiovascular disease (CVD) and stroke in the SBP ≥ 140 mm Hg group increased significantly, while no significant differences were observed in the incidence of myocardial infarction (MI) across the groups. Using the SBP < 110 mm Hg group as the control, the risk of all-cause death in the SBP ≥ 140 mm Hg group increased, as shown in eTable 7.
Among participants aged < 65 years, the risk of adverse outcomes in each group was similar to the results observed in the overall cohort. Among participants aged ≥ 65 years, the incidence of CVD events was lowest in the 110 ≤ SBP < 120 mm Hg group, with no significant differences in the onset risk across other groups. The risk of all-cause death remained lowest in the 120 ≤ SBP < 130 mm Hg group, while the risk increased in the three groups with SBP ≥ 130 mm Hg. No significant differences were observed between the two groups with SBP < 120 mm Hg. The results of the death competition risk model analysis were consistent with those of the main model, as shown in eTable 8. In the subgroup of participants aged ≥ 80 years (n = 227), statistical power was limited due to small sample size. Nevertheless, the lowest point estimate for all-cause mortality remained in the 120 ≤ SBP < 130 mm Hg group, consistent with the main analysis. For CVD events, after combining SBP < 130 mmHg as the reference, hazard ratios for higher SBP groups were directionally consistent but not statistically significant (eTable 8). To assess whether antihypertensive treatment intensity influenced the relationship between post-treatment SBP and adverse outcomes, we stratified participants with comorbidities by treatment intensity. In the low-intensity group (n = 1,371), the lowest risk for all-cause mortality was observed in the 120 ≤ SBP < 130 mm Hg group, with significantly increased risk only in the SBP ≥ 160 mmHg group. No significant differences in CVD risk were observed across SBP categories.In the moderate-intensity group (n = 974), the lowest risk for all-cause mortality also remained in the 120 ≤ SBP < 130 mm Hg group. For CVD events, the HR for the 110 ≤ SBP < 120 mm Hg group could not be estimated due to zero events. Increased risk was observed starting from SBP ≥ 140 mmHg, with an HR of 3.14 (95% CI 1.11–8.86) in the SBP ≥ 160 mmHg group.In the high-intensity group (n = 8,656), the lowest risk for CVD events was observed in the 110–119 mmHg group, consistent with the main analysis. For all-cause mortality, risk gradually increased from SBP ≥ 130 mmHg onward. Detailed results are presented in eTable 10.
Discussion
Using real-world data from 11,273 hypertensive participants with comorbidities and 11,273 hypertensive participants without comorbidities, we identified heterogeneity in the association between post-treatment SBP levels and outcomes such as cardiovascular disease (CVD), myocardial infarction (MI), and stroke. In participants with comorbidities, the minimum risk range for blood pressure was found to be 110 ≤ SBP < 120 mm Hg. However, in participants without comorbidities, the minimum risk range was found to be SBP < 110 mm Hg.The minimum risk range for all-cause death in both participants with and without comorbidities was found to be 120 ≤ SBP < 130 mm Hg. Although this range was associated with the lowest risk for relevant events, no statistically significant increase in the risk of these events was observed when blood pressure was lower than this minimum risk range.
Anti-hypertensive therapy has been shown to effectively reduce the risk of cardiovascular disease (CVD) and death in participants with comorbidities. However, different studies have drawn varying conclusions about the minimum safety threshold for blood pressure. The ACCORD study revealed that intensive anti-hypertensive therapy does not provide benefits for hypertensive participants with diabetes mellitus (DM) and may even increase relevant side effects8. In support of this, a study by Michal Bohm also recommended that blood pressure in hypertensive participants with DM should not fall below 120/70 mm Hg. Conversely, a meta-analysis conducted by Milad reached a different conclusion, suggesting a lower threshold for treatment.
Compared to participants with post-treatment SBP between 110 and 120 mm Hg, we found no statistically significant difference, although a post-treatment SBP of < 110 mm Hg increased the risk of CVD, MI, and stroke in participants with comorbidities by 54%, 79%, and 46%, respectively. Among participants without comorbidities, the risk of CVD, MI, or stroke was lowest in those with an SBP of < 110 mm Hg. The results of the time-dependent Cox regression analysis were consistent with those of the primary analysis. These findings are also in line with the results of the ALLHAT study, which found that the risk of stroke was linearly associated with both SBP and DBP (diastolic blood pressure). Our results suggest that the optimal target SBP range for participants with comorbidities (not complicated by CVD) should be between 110 and 120 mm Hg. Given the potential limitations of the spline analysis due to sparse data at the lower SBP range, we interpret the categorical findings as identifying a range of optimal SBP rather than a strict threshold.
In contrast to the effects of post-treatment SBP on CVD, MI, and stroke, the effects of post-treatment SBP on all-cause mortality showed no significant heterogeneity in either hypertensive group, with or without comorbidities. The mortality risk in participants with and without comorbidities was lowest in the 120 ≤ SBP < 130 mm Hg group. Our findings are consistent with those of a study conducted by Michael Bohm, which found that mortality in hypertensive participants with DM and those with simple hypertension was lowest when post-treatment SBP was within the range of 120 to 140 mm Hg9. One meta-analysis has revealed that the mortality risk is lowest when the post-treatment SBP is within the range of 120 to 124 mm Hg. However, several previous RCTs have shown an increase in mortality risk when SBP is below 120 mm Hg. This disparity may be attributed to differences in the populations selected for each trial. Based on both previous results and our findings, the optimal safety threshold for target SBP in hypertensive participants with comorbidities appears to be within the range of 120 to 130 mm Hg, particularly in terms of minimizing mortality risk.
Age is an important factor influencing the relationship between post-treatment SBP and adverse outcomes, with older individuals exhibiting reduced tolerance to lower SBP thresholds. The Berlin Initiative Study10 has shown that the risk of all-cause death in elderly participants (≥ 70 years old) with a history of CVD may increase when post-treatment SBP is < 140 mm Hg. Similarly, the SPRINT study indicated that the risk of syncope, hypotension, and falls increases with age. According to our stratification analysis, the total risk of CVD, MI, and stroke in individuals ≥ 65 years old was similar to that in hypertensive participants with comorbidities. Specifically, the risk was lowest when SBP was between 110 and 120 mm Hg, while the risk of all-cause death was lowest when SBP ranged from 120 to 130 mm Hg. We did not observe a decline in tolerance to the minimum threshold range of post-treatment SBP in participants with comorbidities who were ≥ 65 years old. Additionally, the SPRINT study found that hypotension and syncope—two common side effects of treatment in the elderly—are primarily induced by intensive antihypertensive therapy and have little correlation with age11. For participants aged ≥ 80 years (n = 227), statistical power was limited. Nevertheless, the observed trends for all-cause mortality and CVD events aligned with the primary findings, suggesting a similar optimal SBP range. Larger studies are warranted to confirm these trends and establish definitive targets for the very elderly.
We further explored the potential confounding effect of antihypertensive treatment intensity by stratifying participants into low-, moderate-, and high-intensity groups. Although some between-stratum variations were observed—for instance, the optimal SBP range for CVD events was 110 ≤ SBP < 120 mm Hg in the high-intensity group but did not reach statistical significance in the low-intensity group—the overall trends remained consistent with the primary analysis. The lowest risk for all-cause mortality was consistently observed in the 120 ≤ SBP < 130 mm Hg range across all intensity strata, and higher SBP levels were generally associated with increased risk for both outcomes. These findings suggest that while treatment intensity may modestly influence the association, post-treatment SBP itself remains a primary determinant of adverse outcomes, independent of treatment intensity.
The type and number of comorbidities in hypertensive patients may potentially influence the relationship between post-treatment SBP and adverse outcomes. However, after excluding patients with DM and tumors, we did not observe a statistically significant increase in the risk of CVD, MI, or stroke when SBP was < 110 mm Hg. The mortality risk remained consistent with the results observed in hypertensive participants with comorbidities. Furthermore, when participants were grouped based on the number of comorbidities, the effects of post-treatment SBP on CVD, MI, and stroke were similar in both the < 3 comorbidities group and the ≥ 3 comorbidities group. All-cause mortality in participants with ≥ 3 comorbidities was lowest in the SBP < 110 mm Hg group, while the mortality risk in participants with an SBP of 120 to 140 mm Hg did not show a statistically significant increase. These findings suggest that the association between post-treatment SBP and adverse outcomes is not influenced by the type or number of comorbidities. Sensitivity analyses focusing on the five most prevalent comorbidities (diabetes, tumors, kidney disease, liver disease, and COPD/cor pulmonale), which comprised over 90% of the comorbid cohort, yielded results consistent with the primary analysis. The optimal SBP range remained 110 ≤ SBP < 120 mm Hg for CVD events and 120 ≤ SBP < 130 mm Hg for all-cause mortality. Sequential exclusion of each of these common comorbidities did not alter these findings, confirming the robustness and generalizability of our conclusions. Furthermore, excluding participants with markers of poor health (low BMI, anemia, elevated hs-CRP, or malignancy) did not alter the optimal SBP ranges, further ruling out reverse causality as a major explanation for our findings.
Another important finding is that the absolute risk of CVD and all-cause death is higher in participants with comorbidities than in those without comorbidities when post-treatment SBP levels are the same. The incidence density of CVD events in the comorbidity group (SBP < 110 mm Hg to SBP ≥ 160 mm Hg) increased from 11.72/1,000 person-years to 29.88/1,000 person-years, while the incidence density of all-cause death increased from 18.88/1,000 person-years to 33.69/1,000 person-years. In participants without comorbidities, the incidence density of CVD events increased from 3.63/1,000 person-years to 14.22/1,000 person-years, while the incidence density of all-cause death increased from 4.41/1,000 person-years to 10.60/1,000 person-years. The relative risks of CVD, MI, and stroke in participants with comorbidities at any SBP level were higher than those in participants without comorbidities (110 ≤ SBP < 120 mm Hg). Similarly, the risk of all-cause death in the comorbidity group was higher than that in the non-comorbidity group (120 ≤ SBP < 130 mm Hg). Our study’s findings were similar to those concluded by Michael Bohm et al., who found that the relative and absolute risks in hypertensive participants complicated by DM were higher than those in participants with simple hypertension. This suggests that controlling blood pressure alone is insufficient for hypertensive participants with comorbidities. Treating comorbidities and controlling blood pressure may be equally important. The treatment of hypertensive participants with comorbidities should involve management by a multidisciplinary expert team.
We addressed a concern shared by both clinicians and participants using real-world data (RWD), showing that a post-treatment SBP below 120 mm Hg does not increase the risk of CVD and all-cause death in hypertensive participants with comorbidities. The ideal post-treatment SBP level for hypertensive participants with comorbidities should be personalized. For patients with a shorter life expectancy, a range of 120–130 mm Hg is recommended, while patients with a longer life expectancy should aim for a post-treatment SBP range of 110–120 mm Hg.
Our study has several advantages. Firstly, the data were derived from the high-quality Kailuan cohort study. Specifically, the diagnosis of comorbidities was well-defined, medication information was obtained from electronic outpatient records, and adverse event information was collected from inpatient medical records and the social insurance system. Secondly, considering the effects of dynamic changes in blood pressure on adverse outcomes during the follow-up period, we conducted a Cox regression analysis with the SBP value measured every two years as a time-varying variable. Additionally, given the high mortality among hypertensive participants with comorbidities, we also performed a competing risk analysis for death. Asthenia and nutritional status may also influence outcomes in elderly hypertensive participants with comorbidities. Although such data were missing, hemoglobin levels were used as a substitute indicator, and adjustments were made in the model to ensure the reliability of the results. Finally, the observation period was as long as seven years, surpassing that of most randomized controlled trials (RCTs).
Despite these advantages, our study has some inevitable limitations. Compared with RCTs, the risk factors of the non-comorbid hypertension group (used as the control) were still statistically different from those of the comorbid hypertension group. However, our main objective was to study the effects of post-treatment SBP on participants with comorbidities, and the control group did not affect the intra-group analysis of the comorbid hypertension group. Since medication information for the non-comorbid hypertension group was based on self-reports, there may be instances of underreporting or misreporting, and data on medication frequency were unavailable. Nevertheless, the comprehensive questionnaire data helped minimize such errors. Additionally, the replacement of mercury sphygmomanometers with Omron HBP-1300 electronic devices during follow-up may have introduced measurement variability, although previous studies have demonstrated acceptable agreement between the two methods12. Although 34 types of comorbidities were identified, the main comorbidities were diabetes mellitus (DM) and tumors, and participants who had already developed atherosclerotic cardiovascular disease (ASCVD) were excluded. Therefore, the results should be generalized with caution. Although we collected detailed medication information from electronic medical records and provided lists of commonly used drugs for major comorbidities, unmeasured confounding related to specific treatment regimens cannot be entirely ruled out. Variations in treatment intensity, adherence, and individual responses may have influenced the outcomes and were not fully captured in this real-world study. Finally, our study population was predominantly male and derived from a single occupational cohort in China, which limits the generalizability of our findings to females, other ethnic groups, and different healthcare settings. Future studies with more diverse populations are needed to validate these results.
Data availability
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- SBP:
-
systolic blood pressure
- DM:
-
diabetes mellitus
- CKD:
-
chronic kidney disease
- COPD:
-
chronic obstructive pulmonary disease
- CVD:
-
cardiovascular disease
- MI:
-
myocardial infarction
- SAH:
-
subarachnoid hemorrhage
References
Mills, K. T., Stefanescu, A. & He, J. The global epidemiology of hypertension. Nat. Rev. Nephrol. 16 (4), 223–237 (2020).
Lu, J. et al. Prevalence, awareness, treatment, and control of hypertension in China: data from 1.7 million adults in a population-based screening study (China PEACE Million Persons Project). Lancet 390 (10112), 2549–2558 (2017).
He, L. et al. The prevalence of multimorbidity and its association with physical activity and sleep duration in middle aged and elderly adults: a longitudinal analysis from China. Int. J. Behav. Nutr. Phys. Act. 18 (1), 77 (2021).
Zhang, X. et al. Community prevalence and dyad disease pattern of multimorbidity in China and India: a systematic review. BMJ Glob Health 7(9), e008880 (2022).
Williams, B. et al. 2018 ESC/ESH Guidelines for the management of arterial hypertension: The Task Force for the management of arterial hypertension of the European Society of Cardiology and the European Society of Hypertension: The Task Force for the management of arterial hypertension of the European Society of Cardiology and the European Society of Hypertension. J. Hypertens. 36 (10), 1953–2041 (2018).
Whelton, P. K. et al. ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: Executive Summary: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J. Am. Coll. Cardiol., 71(19), 2199–2269 (2018).
Brilleman, S. L. et al. Implications of comorbidity for primary care costs in the UK: a retrospective observational study. Br. J. Gen. Pract. 63 (609), e274–282 (2013).
Group, A. S. et al. Effects of intensive blood-pressure control in type 2 diabetes mellitus. N Engl. J. Med. 362 (17), 1575–1585 (2010).
Bohm, M. et al. Cardiovascular outcomes and achieved blood pressure in patients with and without diabetes at high cardiovascular risk. Eur. Heart J. 40 (25), 2032–2043 (2019).
Douros, A. et al. Control of blood pressure in older patients with heart failure and the risk of mortality: a population-based prospective cohort study. Age Ageing. 50 (4), 1173–1181 (2021).
Sink, K. M. et al. Syncope, Hypotension, and Falls in the Treatment of Hypertension: Results from the Randomized Clinical Systolic Blood Pressure Intervention Trial. J. Am. Geriatr. Soc. 66 (4), 679–686 (2018).
Chen, Z. et al. Assessing the validity of oscillometric device for blood pressure measurement in a large population-based epidemiologic study. J. Am. Soc. Hypertens. 11 (11), 730–736e734 (2017).
Acknowledgements
Thanks to the Kailuan crowd.
Author information
Authors and Affiliations
Contributions
There are authors’ contributions: conception and design (Zhe Huang, Guodong Wang, Jingyuan Jiang, Yanfeng Zhou and Xiaokun Liu); analysis and interpretation of data (Zhe Huang, Guodong Wang, Liuxin Li, Chenrui Zhu, Shouling Wu and Huiying Li,); drafting of the manuscript (Zhe Huang, Guodong Wang, Xiaoming Wei, Chunpeng Ji, and Jinmei Wang); revising it critically for important intellectual content (Zhe Huang, Guodong Wang, Bing Han, Shuo Wang, and Shouling Wu); final approval of the manuscript submitted (Zhe Huang, Guodong Wang, Liuxin Li, Xiaokun Liu, and Shouling Wu).
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics declarations
This study was performed in line with the principles of the Declaration of Helsinki. Approval was granted by Kailuan Medical Group Ethics Committee (Approval No. 2006 Medical Ethics 5).
Consent for publication
Informed consent was obtained from all individual participants included in the study.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Huang, Z., Jiang, J., Wang, G. et al. Effects of post-treatment systolic blood pressure on adverse outcomes in hypertensive population with comorbidity. Sci Rep 16, 14594 (2026). https://doi.org/10.1038/s41598-026-42443-w
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-026-42443-w
