
Abstract
Digital mobility outcomes (DMOs) offer unique insights into recovery of real-world mobility after proximal femoral fracture (PFF), but their clinical validity remains to be established. This study assessed construct validity (convergent, divergent, and known-groups) of 24 DMOs measuring walking activity (amount, pattern) and gait (pace, rhythm, bout-to-bout variability) in patients within one year after PFF. Patients were recruited from inpatient and outpatient lists at five European sites, resulting in 505 included participants (66% female), with mean age of 77.6 ± 9.4 years and supervised gait speed of 0.7 ± 0.4 m/s. Mobility was monitored over seven days using a single wearable device on the lower back. Convergent and divergent validity analyses were stratified by two groups: acute (≤ 14 days since surgery) and non-acute (≥ 15 days since surgery). Correlations between DMOs and related (clinical- and patient-reported mobility outcomes) and unrelated constructs (hearing impairment and systolic blood pressure) were compared to a priori expected correlations. Known-groups validity was assessed across four recovery phases. The results were evaluated individually by experts and in a subsequent consensus meeting, with 17 of 24 DMOs showing evidence of construct validity in non-acute PFF patients. These findings represent an initial step in a larger process towards regulatory endorsement.
Similar content being viewed by others

Introduction
Proximal femoral fractures (PFF) in older adults represent a life-changing clinical event with high one-year mortality rates ranging between 20 and 30%1. Many patients experience long-term functional decline, with high rates of care home admission and only 40–60% regaining their pre-fracture mobility in extended activities of daily living2. Independent mobility plays a central role in social participation and quality of life after a PFF3, making recovery of walking ability a key rehabilitation target. Mobility recovery evolves over the first postoperative year, beginning with an acute phase focused on surgery, mobilisation and pain management4. This is followed by a post-acute rehabilitation phase, aimed at restoring physical function and preparing patients for discharge5. Recovery then continues in an extended phase during the first six months, and ultimately a long-term phase in the latter half of the year, when mobility tends to stabilise6,7,8,9. Tracking mobility recovery across these phases may help clinicians identify mobility limitations and potential risks, and guide patient treatment and rehabilitation.
Traditionally, mobility has been measured with clinical tests under standardised, supervised conditions, offering recovery snapshots that may not capture how people move in daily life with changing environments10. Further, clinical tests are susceptible to floor and ceiling effects as well as reactivity to observation11,12. Wearable devices equipped with inertial measurement units offer a more differentiated and ecologically valid insight into patients’ mobility in real-world environments13,14. These devices enable the quantification of various walking-related digital mobility outcomes (DMOs)14 in walking domains such as amount, pattern, pace, rhythm and variability of walking15. However, research on real-world DMOs in older adults after PFF has been limited largely to the amount domain, e.g. number of steps per day and daily active time16,17. Due to technical complexity, spatial and temporal parameters that provide information on other domains of mobility, such as activity patterns (e.g., number of walking bouts), pace (e.g., walking speed) or rhythm (e.g., cadence) have rarely been measured in the real world after a PFF18. Recent methodological advances now make it possible to address this gap.
Building on a core set of technically validated measures, the Mobilise-D project created a processing pipeline that enables the estimation of 24 DMOs that reflect walking activity (amount- and pattern domains) and gait (pace, rhythm and bout-to-bout variability domains) across health conditions such as Parkinson’s disease (PD), chronic obstructive pulmonary disease (COPD), multiple sclerosis (MS) and older adults after a PFF19,20,21. Although valid in terms of criterion validity, the accuracy and reliability of some DMOs were lower in patients with more pronounced mobility limitations, such as those with slow walking speeds and gait irregularities19,20,21. These challenges in assessing real-world gait in populations with impaired gait function, together with the current lack of studies validating DMOs specifically in patients after a PFF15, emphasise the need for clinical validation. This is currently being addressed by the Mobilise-D consortium through a comprehensive assessment of the DMOs’ construct validity, ability to detect change, and predictive capacity, with the first descriptive results from the PFF cohort recently released22. This broad assessment lays the groundwork towards endorsement of DMOs by regulatory authorities.
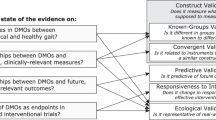
This study assesses the construct validity of 24 real-world walking activity and gait DMOs in a large, heterogeneous, international sample of patients recruited within the first year after PFF surgery. We apply a comprehensive framework of construct validity following the COSMIN guidelines23, encompassing convergent validity (moderate-to-strong associations with established mobility measures), divergent validity (weak or absent associations with unrelated constructs), and known-groups validity (ability to distinguish between different phases of mobility recovery)24,25.
Methods
Study design
This cross-sectional analysis is part of the Mobilise-D clinical validation study (CVS; ISRCTN: 12051706), a multicentre prospective cohort study funded by the Innovative Medicines Initiative, aiming to clinically validate multiple DMOs in four clinical cohorts: PD, MS, COPD, and PFF13. Data were collected between April 2021 and June 2024. For this study, data from the first study visit of patients after PFF was used, based on the study database version 7.1.
Ethics approval
This study was performed in line with the principles of the Declaration of Helsinki. Approval was granted at each study site by the Committee of the Protection of Persons, South-Mediterranean II, Montpellier (ref.: 221BO8), the EC of the Medical Faculty of Eberhard-Karls-University Tubingen, Stuttgart (ref.: 976/2020BO2), the EC of the Medical Faculty at Heidelberg University (ref.: S-719/2021), and the Regional Committee for Medical and Health Research Ethics, Central Norway (ref.: 216069).
Participants
Participants were invited to an initial screening appointment. They were recruited through inpatient and outpatient lists across five sites in three European countries: Trondheim and Oslo (Norway), Stuttgart and Heidelberg (Germany), and Montpellier (France). Inclusion criteria required participants to be aged 45 years or older, be community-dwelling prior to the fracture, and have undergone surgical treatment (osteosynthesis or arthroplasty) for PFF. Participants were enrolled up to 52 weeks postoperatively. They had to be able to walk at least four metres at the first visit and be willing to wear a single wearable device. Further inclusion and exclusion criteria are listed in the study protocol13. Written informed consent was obtained from all participants included in the study13.
Digital mobility outcomes
Real-world mobility performance of patients after PFFs was assessed for up to 7 days using one of two single wearable devices: the MoveMonitor+ worn on a belt around the waist (McRoberts B.V., The Hague, The Netherlands) or an Axivity AX6 (Axivity Ltd, Newcastle Upon Tyne, UK) fixed to the skin of the participants’ lower back with adhesive tape. Both devices included a 6 Degrees of Freedom inertial measurement unit with the following configuration: triaxial accelerometer with a range of +/-8 g and a resolution of 1 mg, triaxial gyroscope with a range of +/- 2000 degrees per second (deg/s) and a resolution of 70 milli-degrees per second (mili-deg/s), sampling frequency of 100 Hz (Hz). The devices were evaluated in a comprehensive technical validation study26. Both devices showed comparable technical specifications and met the predefined minimum performance requirements, ensuring no meaningful impact on algorithm performance.
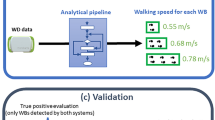
We removed participants who did not have a minimum of at least 12 h of daily wear time (07:00–22:00 h) across ≥ 3 days27. In the preceding technical validation work, a broad array of available algorithms to detect digital mobility outcomes (DMOs) from a single wearable device were implemented according to agreed definitions28, and tested for criterion validity against gold and silver standards19,20. We first identified walking bouts (WBs, walking events of at least two strides of both feet28, and obtained WB-level DMOs aggregated at the weekly level29, resulting in 24 technically valid DMOs that encompass both walking activity (amount and pattern) and gait domains (pace, rhythm, and bout-to-bout variability)19,20. All 24 DMOs are described in Supplementary Table S1.
Clinical outcome assessments (COAs)
We collected information on the following COAs: (i) Lower limb physical capacity measured using the Short Physical Performance Battery (SPPB), consisting of standing balance, gait speed, and five chair-rise tests, with total score as the outcome variable30; (ii) Mobility function and functional independence measured using the Timed Up and Go test (TUG), considering the total time taken to complete the task31; Walking ability as measured using (iii) the 4 m supervised gait speed test and (iv) the 6-minute walk test (6MinWT), including the endpoint of distance walked32. COAs were used for convergent validity.
Patient-reported outcome measures (PROMs)
PROMs were used for convergent validity and included (i) perceived function using the function component of the Late-Life Function and Disability Instrument Functional Component (LLFDI-FC)33, (ii) concerns about falling using the Short Falls Efficacy Scale International (Short FES-I)34, and (iii) symptoms of fatigue measured using the Functional Assessment of Chronic Illness Therapy Fatigue Scale (FACIT-F)35.
Other clinical outcomes
To test divergent validity, we collected information on: (i) systolic blood pressure; and (ii) hearing impairment during (a) a phone call and (b) a group conversation, assessed using the sum score of these two survey questions (range: 2–8), where lower scores indicate better hearing. These variables were a priori selected by a large expert panel in the Mobilise-D validation study.
Statistical analysis
Assuming an alpha level of 0.05 and a power of 80%, we estimated that detecting statistically significant correlations of ≥ 0.6, ≥ 0.4, ≥ 0.3 and ≥ 0.2 would require sample sizes of 20, 46, 85, and 193 participants, respectively, based on Fisher’s z-transformation36. Given our available sample size, we had sufficient power to conduct the planned analyses, except for one subgroup as detailed below.
Statistical analyses were pre-specified and conducted using R Statistical Software (v4.3.2: R Core Team 2023). Given the absence of missing values in the constructs analysed in relation to the DMOs, and considering that missing DMO values were structurally determined by the absence of the corresponding walking behaviour, analyses were conducted using a complete-case approach. Data were tested for normality using histograms, QQ plots and skewness analysis. Patients’ characteristics and DMOs were described using mean (SD) or median (p25-p75), depending on distribution. This study followed the COSMIN guidelines for assessing construct validity, defining a priori hypotheses for both convergent and divergent validity, and including a rigorous assessment of known-groups validity23.
The convergent and divergent validity analyses were stratified a priori into an acute group (≤ 14 days since surgery) and a non-acute group (≥ 15 days after surgery). The acute group was kept separate for several reasons: (i) The Mobilise-D technical validation study identified challenges related to the accuracy and reliability of stride length and walking speed DMOs in patients after PFF with low physical capacity21; (ii) acute patients have very low physical capacity compared to patients in later recovery phases8; (iii) patients were not allowed to perform the 6MinWT and TUG tests during the acute state; and (iv) the LLFDI could not be collected meaningfully in the acute phase. The 14-day cut-off was selected as it reflects the transition from inpatient care to non-supervised independent mobility37,38.
To assess convergent validity, Pearson Product-Moment or Spearman Rank Correlation coefficients (with 95% CIs) were calculated between the 24 DMOs and the corresponding constructs (COAs and PROMs). A DMO was considered to demonstrate convergent validity when its correlation coefficients matched the hypothesised values39. The expected correlation coefficients are detailed in Supplementary Tables S2 and S3, and were based on a pilot study20, previous literature, and expert consultation. We expected no correlation to exceed 0.9, as that would indicate that the DMO provides the same information as existing constructs39. Correlation coefficients were classified as either very weak (< 0.3), weak (0.3–0.4), moderate (0.4–0.6), or strong (> 0.6), similar to previously proposed guidelines40. As some DMOs (e.g., bout-to-bout variability and rhythm domain) have not been measured under real-life conditions in patients after a PFF before, this part of the study was exploratory in nature. We hypothesised that the following would show weak to strong positive correlations with better physical capacity (COAs: high SPPB scores, fast gait speed, shorter TUG time) and mobility perception (PROMs: high LLFDI scores, low Short FES-I scores, high FACIT-F scores): (a) a higher number of steps and longer walking durations (amount), (b) a higher number of different WBs and WB durations (pattern), (c) faster walking speed (pace), (d) higher cadence and shorter stride duration (rhythm), and (e) greater bout-to-bout variability.
Divergent validity was assessed by analysing the Pearson Product-Moment or Spearman Rank Correlation coefficients between each of the DMOs and hearing loss and systolic blood pressure. The latter were expected to correlate very weakly with the DMOs (r/ρ’s < 0.2). Divergent validity was tested for the non-acute group only, as the sample size was insufficient for the acute group.
Known-groups validity was assessed by testing the distribution of DMOs across four PFF groups defined by time since surgery: acute (≤ 14 days), post-acute (15–42 days), extended recovery (43–182 days), and long-term recovery (≥ 183 days), consistent with established postoperative recovery trajectories22. These phases reflect clinically distinct stages of recovery, during which mobility is expected to improve progressively and then stabilise. Known-groups validity was supported when the p-for-trend from linear regression was ≤ 0.05. We expected statistically significant differences in mobility between the phases.
Final construct validity was determined through a structured expert consensus process. Nine experts from different professional backgrounds (geriatrics, orthopaedic surgery, physiotherapy, movement and exercise science, epidemiology, and data science) independently evaluated each DMO. Experts were provided with standardised summaries of the convergent, divergent and known-groups validity results for each DMO. They were instructed to base their judgment on the predefined assumptions described above and their clinical or methodological expertise. For each DMO, experts recorded a binary judgment (agree/disagree) on whether construct validity was achieved. These initial judgements were performed independently. Subsequently, disagreements were discussed in a joint meeting, during which experts could identify the reasoning behind differing opinions and clarify interpretations. Sources of discrepancy were documented. Final decisions on whether a DMO demonstrated construct validity were based on consensus.
Results
From a total of 567 recruited participants after a PFF, the current analyses included 505 participants (89%), of which 100 (20%) were assessed in the acute phase, 117 (23%) in the post-acute phase, 201 (40%) in the extended recovery phase, and 87 (17%) in the long-term recovery phase (Table 1). No differences were observed between included and excluded participants, apart from higher indoor walking aid usage, less hearing impairment and a larger proportion of participants in the post-acute and extended recovery phases in the included sample (Supplementary Table S4). The reasons for exclusion were not using the wearable device (n = 24), not having available DMO measures due to technical problems (n = 11), or not having valid DMOs (n = 5 due to not having wear time available for technical reasons, and n = 22 not meeting the minimal wear time criteria).
The included sample had more females (66%) than males, a mean (SD) age of 77.6 (9.4) years, and was measured at a median (p25-p75) of 60 (23–140) days after PFF surgery (Table 1). The full study sample had a mean (SD) SPPB score of 6.2 (3.1), a four-meter gait speed of 0.70 (0.40) m/s, a TUG time of 19.8 (12.3) s, and a 6MinWT distance of 283.6 (125.9) m (Table 2). Groups assessed early after surgery (acute and post-acute) showed worse physical function compared to those assessed in later recovery phases (extended and long-term) (Table 2). Acute patients walked a median of 519 (241–1069) steps in a total walking time of 7 (3–14) minutes per day (Supplementary Table S5), and non-acute participants walked a median of 2702 (1346–5280) steps with a total walking time of 32 (16–58) minutes per day (Table 3).
Convergent validity
The walking amount domain DMOs showed very weak to strong correlations with the related constructs (|ρ| = 0.08–0.76) (non-acute group, n = 405: Table 3; acute group, n = 100: Supplementary Table S5), consistent with the anticipated coefficients (non-acute group: Supplementary Table S2; acute group: Supplementary Table S3). Similarly, walking pattern and pace DMOs showed very weak to strong correlations with related constructs (|ρ| = 0.01–0.80), with the vast majority matching the expected coefficients in the non-acute group. Rhythm DMOs provided very weak to strong correlations (|ρ| = 0.01–0.60), with three of five coefficients in the non-acute group matching the expected correlations. The bout-to-bout variability DMOs demonstrated very weak to moderate associations with the related constructs (|ρ| = 0.02–0.58), with less than half of the coefficients meeting the expected correlations. Overall, DMOs in the non-acute group demonstrated stronger and more consistent correlations with related constructs compared to the acute group, with a larger number of coefficients aligning with expected values. Also, correlations between DMOs and COAs were consistently stronger than between DMOs and PROMs, matching the expectations.
Divergent validity
Very weak correlations were observed between all DMOs and the constructs of divergent validity (|ρ| = 0.01–0.22) for the non-acute group (Table 3), as expected (Supplementary Table S2). Only two DMOs exceeded the expected correlation threshold of 0.2, namely walking speed in shorter WBs (ρ = -0.21) and P90 walking speed in WBs > 10s (ρ = -0.22).
Known-groups validity
In total, 21 of 24 DMOs statistically differentiated across the four recovery groups (Supplementary Fig. S6), supporting known-groups validity. The three DMOs that did not differentiate between the recovery groups were WB duration, P90 WB duration, and stride length bout-to-bout variability in longer (> 30s) WBs.
Expert consensus on construct validity
There was expert consensus that 17 of the 24 DMOs showed evidence for construct validity, covering almost all DMOs in the domains of amount (2 of 2), pattern (5 of 7), and pace (6 of 6), and fewer DMOs in the domains of rhythm (3 of 5) and bout-to-bout variability (1 of 4). Experts considered the three cadence DMOs and the walking speed bout-to-bout variability in longer (> 30s) WBs as valid but exploratory. The independent voting showed that among the 17 DMOs considered valid, three had unanimous expert agreement (100% in favour) and 14 had minor disagreements (78–89% in favour) (Table 4). All disagreements were discussed in the subsequent joint expert meeting, after which a consensus decision was made on all the DMOs (Table 4). Experts placed larger emphasis on the results for the non-acute group and gave greater weight to correlation coefficients with COAs than PROMs. There was expert consensus that 7 DMOs did not show evidence for construct validity: two pattern DMOs (mean and P90 WB duration), two rhythm DMOs (stride duration in all WBs and in longer (> 30s) WBs), and three bout-to-bout variability DMOs (stride length bout to bout variability in longer (> 30s) WBs, cadence bout-to-bout variability, and stride duration bout-to-bout variability).
Discussion
This is the first multi-site study to evaluate the construct validity of real-world DMOs in a large representative sample of both acute and non-acute patients within the first year of recovery following PFF - a population at high risk of poor mobility recovery, loss of functional independence, care home admission, and accelerated mortality. Based on consensus and focus on non-acute patients, evidence for construct validity was observed for 17 of 24 DMOs, specifically in (almost) all DMOs of amount (2 of 2), pattern (5 of 7), and pace (6 of 6) domains. Evidence for construct validity was more variable for the rhythm (3 of 5) and bout-to-bout variability (1 of 4) domains. Accordingly, the majority of DMOs can capture the intended mobility and health aspects in patients after a PFF, providing valid insights into their health status, complementing clinical tests in non-acute and home-based settings.
Amount of walking activity
Our results demonstrate construct validity for the DMOs WB step count and walking duration, supported by our convergent, divergent and known-groups validity analyses. The consistent strong correlations between DMOs and related mobility constructs even exceeded correlation coefficients found in previous observational studies17,41,42. The WB step count and walking duration have the discriminative power to distinguish between patients in different recovery phases. However, the differences are particularly accentuated between the earlier phases. This aligns with previous findings of longitudinal observational studies, which observed a steep increase in mobility capacity in the first six months and subsequent stabilisation in months 6–126,7,8, with the number of steps per WB peaking nine months postoperatively9.
Pattern of walking activity
Seven walking activity pattern DMOs were assessed, of which five demonstrated construct validity, namely the number of WBs per day in the different WB duration categories (overall, and longer than 10s, 30s, 60s) and the variability in WB duration. These DMOs showed moderate to strong correlations with the COAs, of which four met the predefined thresholds for convergent validity. Although the coefficients for the number of WBs > 30s remained slightly below the a priori threshold of ρ = 0.6, the expert panel regarded this DMO as valid due to its consistent moderate associations with related mobility constructs and its support from both divergent and known-groups validity.
Unexpectedly, the two DMOs representing WB duration did not meet the criteria for construct validity. A likely explanation is that most WBs were under 10s across all recovery phases, with a median WB duration in our study of 7.5 s. Such short durations may be feasible for most patients, regardless of their physical capacity. Previous studies have similarly reported a large number of short WBs during the entire recovery process after a PFF18. The latter study also highlighted the potential environmental impact on WB duration, as a decline was observed in patients’ WB duration from the hospital to the home environment18. People’s home environment may offer limited space for longer WBs, in contrast to hospitals with long corridors. While very short WBs are frequent and clinically relevant in patients after a PFF18,21, their ability to represent typical walking patterns is questionable, since they often occur indoors in cluttered spaces and may include other daily activities43.
Pace of gait
Real-world walking speed and stride length are two prominent gait metrics whose construct validity has not yet been established in people after a PFF. In this study, all pace-related DMOs met the expected moderate to strong correlations with the related constructs in the non-acute group, with most of them showing divergent validity as well. In the acute group, weak to moderate expected correlations were observed only for walking speed and stride length in longer WBs. The absence of associations in shorter WBs may be attributed to overestimation of these DMO estimates in individuals with lower physical capacity and slower walking speed after a PFF, leading to reduced variability and a more homogeneous sample19,21. This finding highlights a broader methodological challenge: short WB durations in combination with severe mobility limitations pose difficulties for the accurate estimation of real-world walking speed by sensor-based algorithms19,21. Therefore, only WBs longer than 10 s were included in the clinical validation of pace-related DMOs. Although convergent validity was not consistently demonstrated in the acute group, known-groups validity was observed across all four recovery phases, and the expert group reached consensus that all pace DMOs fulfilled construct validity for the non-acute group. These findings are of high clinical relevance, as supervised walking speed has high predictive capacity for long-term functional changes and mortality risk in older adults44,45.
Rhythm of gait
Cadence and stride duration represent the temporal and rhythmic components of gait. Despite all five rhythm DMOs differentiating between the four phases of PFF recovery (Supplementary Fig. S6), only the three cadence DMOs showed evidence of construct validity. This may be attributed to the higher accuracy and reliability of cadence estimation compared to stride duration estimation in PFF21. The present results indicated that higher cadence was moderately associated with better mobility capacity, whereas step duration showed weaker associations. This finding is somewhat surprising, as a previous study conducted in laboratory-based conditions demonstrated high intercorrelations between cadence and step duration, with both closely linked to metrics of pace46. Given the inconsistent associations between rhythm DMOs and measures of mobility capacity, in combination with the lack of evidence in real-world settings, our clinical experts considered the domain of rhythm to remain exploratory and recommend further investigation to gain insight into the clinical meaning of cadence after a PFF. Additional rhythm-related DMOs – such as measures of gait asymmetry (e.g., right-left imbalance) – may offer further insight into recovery trajectories and should be explored in future follow-up assessments of patients after PFF46.
Bout-to-bout variability of gait
The bout-to-bout variability domain captures fluctuations in walking behaviour – such as in stride duration, stride length, speed, or cadence – across separate walking episodes throughout the day. This aspect of mobility has not been investigated before in individuals recovering from PFF. Of the four variability-related DMOs, only bout-to-bout variability of walking speed in longer WBs correlated moderately with mobility capacity in the non-acute group and distinguished between recovery phases. This finding suggests that individuals with greater mobility capacity may display higher variability in real-world walking speed. In this context, higher variability between WBs may indicate adaptivity to varying environmental demands, as previously described in individuals with Parkinson’s disease43. From a clinical perspective, bout-to-bout variability could complement traditional average-based mobility metrics by capturing flexibility and context-dependent modulation of real-world walking.
The remaining three bout-to-bout variability DMOs (in stride duration, stride length, and cadence) failed to meet the criteria for construct validity. Stride length bout-to-bout variability showed a moderate association with mobility capacity, but did not show known-groups validity, possibly due to the technical challenges in estimating stride length in PFF21. In sum, walking speed bout-to-bout variability in longer bouts may be a relevant DMO in non-acute patients. However, further research is needed to better understand its potential clinical relevance and utility in monitoring patients after a PFF.
Construct validity of DMOs in the acute phase after PFF
As anticipated, correlations between DMOs and established clinical outcome measures were substantially lower in acute patients compared to non-acute patients. Notably, only six DMOs – spanning the domains of amount, pattern, and pace - met the expected correlations with COAs. The weak to moderate correlation coefficients observed between the amount-related DMOs and COAs align with previous research that reported moderate correlations between upright time and TUG in a small sample of acute patients16. However, direct comparison is limited due to differences in DMO definitions and methodologies across studies.
The low associations observed in the acute group may reflect the severely reduced mobility typically seen in the early stages of recovery after PFF surgery16,47,48. During this phase, patients often show restricted physical function and reduced ability to walk for longer durations22, resulting in fewer WBs of sufficient duration for reliable DMO estimations. Moreover, the acute sample tends to be relatively homogenous regarding mobility behaviour and capacity, which limits variation and hence statistical power. Additionally, walking behaviour in this setting is likely influenced more by structured clinical routines than by real-world autonomy.
Implications
Our findings support the use of DMOs for monitoring and guiding the care of older adults in the year following PFF surgery, although DMOs may have limited utility during the first two weeks post-surgery and should be supplemented with more traditional clinical tests of physical capacity in this acute phase. Clinically validated real-world DMOs derived from a single wearable device offer promising opportunities for remote monitoring of home-dwelling older adults after PFF. First, mobility monitoring might serve in the prediction of fall risk49 and poor mobility recovery, which are currently being examined within the Mobilise-D consortium. Second, validated DMOs could facilitate the design and implementation of personalised rehabilitation programs50, with tailored exercise interventions informed by patients’ functional capacity and environmental constraints. Objective mobility data may also serve as motivational feedback, potentially enhancing engagement and the effectiveness of transitional care following PFF51. Third, remote monitoring offers logistical and economic advantages. Its non-intrusive nature can increase adherence to long-term monitoring by eliminating the need for frequent clinical visits – an especially important factor for individuals in rural or underserved areas52. The feasibility of this approach is underscored by the high completion rate of > 90%, defined as wear time of at least three days and 12 h per day. Reducing the burden of travel and the time demands on clinical staff may also contribute to cost savings, while enabling continuous and objective assessment of recovery in real-world settings.
Strengths and limitations
This study included a large and diverse sample of patients recovering from PFF, recruited across three countries at various time points up to one year post-surgery. This broad recruitment strategy enhances the generalizability of findings by including patients at various stages of functional recovery and from different healthcare settings. A further strength lies in the application of a comprehensive construct validity framework following the COSMIN guidelines, assessing convergent, divergent, and known-groups validity23. Notably, the known-groups approach based on recovery phase has not previously been applied in studies validating DMOs in patients after hip fracture. The DMOs’ ability to differentiate between these recovery phases supports the validity of this approach. Furthermore, this study followed a rigorous protocol for data quality with predefined thresholds for valid wear time, ensuring high data reliability. The validity of the findings was strengthened by the use of a priori hypotheses and multi-professional expert consensus, aligning with best practices for digital biomarker validation. However, some limitations must be acknowledged. Key clinical assessments relevant to convergent validity, such as the SPPB, TUG and LLFDI, could not be performed in the acute recovery phase. Additionally, differences in healthcare systems across countries may have influenced recovery trajectories and mobility outcomes. For example, acute participants in Germany typically receive more intensive and prolonged inpatient rehabilitation, whereas participants in Norway are often discharged to home at an earlier stage. The number of patients in the acute group was too small to allow for site-specific analyses or to examine divergent validity.
In addition to validating the DMOs against established clinical tests of mobility capacity, PROMs were also included as criteria for convergent validity. This reflects Mobilise-D’s holistic view of mobility, which encompasses capacity, daily performance, and patients’ perceptions14. Another strength is the inclusion of DMOs across multiple mobility domains. However, this introduces some methodological challenges. Among the PROMs included, the Short FES-I and the FACIT-F primarily assess fear of falling and fatigue, respectively, which are related to mobility but do not directly capture mobility performance. This may partly explain their weaker associations with the DMOs compared to measures that more explicitly reflect functional mobility. For domains such as rhythm and bout-to-bout variability, where limited prior evidence exists, clinical expertise was required to develop a priori hypotheses. Consequently, these aspects of the study are exploratory in nature. Further research is needed to improve the understanding of the interpretability and clinical relevance of DMOs related to rhythm and bout-to-bout variability, including a possible expansion of these domains.
Conclusion
A total of 17 DMOs related to walking activity and gait demonstrated evidence supporting construct validity in non-acute patients recovering from PFF. Construct validity was supported through rigorous statistical testing and expert consensus, incorporating convergent, divergent, and known-groups validity in accordance with the COSMIN guidelines. Specifically, all DMOs within the amount and pace domains, as well as most within the pattern domain, demonstrated construct validity, whereas a minority of rhythm and bout-to-bout variability DMOs fulfilled these criteria. In sum, real-world DMOs offer a cost-effective and clinically relevant solution with strong clinimetric properties, capable of reflecting a diverse range of clinical outcomes – from objective functional mobility capacity to patients’ subjective perceptions about their mobility. These DMOs may deepen our understanding of functional recovery outside controlled clinical settings, offering clinicians valuable information about how functional gains translate into daily life. In addition, evidence for construct validity is a necessary but not sufficient step towards regulatory endorsement of DMOs in for example PFF rehabilitation or routine follow-up. Additional evidence on responsiveness, predictive validity, longitudinal outcomes, and clinically meaningful change is needed before regulatory endorsement can be supported.
Data availability
The data presented in this paper was generated during the IMI2 Mobilise-D project. The dataset from this project will be released under a C.C.4.0 NC license in June 2026 at https://zenodo.org/communities/mobilise-d/ according to the data release schedule agreed by the Mobilise-D consortium. Please direct any data-related queries to: Brian CaulfieldEmail: b.caulfield@ucd.ie.
References
Papanicolas, I. et al. Differences in health outcomes for high-need high-cost patients across high-income countries. Health Serv. Res. 56, 1347–1357. https://doi.org/10.1111/1475-6773.13735 (2021).
Dyer, S. M. et al. A critical review of the long-term disability outcomes following hip fracture. BMC Geriatr. 16, 158. https://doi.org/10.1186/s12877-016-0332-0 (2016).
Segev-Jacubovski, O., Magen, H. & Maeir, A. Functional Ability, Participation, and Health-Related Quality of Life After Hip Fracture. OTJR: Occup. Therapy J. Res. 39, 41–47. https://doi.org/10.1177/1539449218796845 (2019).
Nijdam, T. M. P. et al. The goals of care in acute setting for geriatric patients in case of a hip fracture. Eur. J. Trauma Emerg. Surg. 49, 1835–1844. https://doi.org/10.1007/s00068-023-02258-0 (2023).
Reyes, B. J. et al. Postacute Management of Older Adults Suffering an Osteoporotic Hip Fracture: A Consensus Statement From the International Geriatric Fracture Society. Geriatric Orthop. Surg. Rehabilitation. 11 https://doi.org/10.1177/2151459320935100 (2020).
Munter, L. et al. Trajectories and prognostic factors for recovery after hip fracture: a longitudinal cohort study. Int. Orthop. 46, 2913–2926. https://doi.org/10.1007/s00264-022-05561-4 (2022).
Dakhil, S. et al. Longitudinal trajectories of functional recovery after hip fracture. PLOS ONE. 18, e0283551. https://doi.org/10.1371/journal.pone.0283551 (2023).
Magaziner, J. et al. Recovery from hip fracture in eight areas of function. J. Gerontol. Biol. Sci. Med. Sci. 55, M498–507. https://doi.org/10.1093/gerona/55.9.m498 (2000).
Engdal, M. et al. Real-world mobility recovery after hip fracture: secondary analyses of digital mobility outcomes from four randomized controlled trials. Age Ageing. 53 https://doi.org/10.1093/ageing/afae234 (2024).
Foucher, K. C., Thorp, L. E., Orozco, D., Hildebrand, M. & Wimmer, M. A. Differences in preferred walking speeds in a gait laboratory compared with the real world after total hip replacement. Arch. Phys. Med. Rehabil. 91, 1390–1395. https://doi.org/10.1016/j.apmr.2010.06.015 (2010).
Rix, A. et al. Measurement of Mobility and Physical Function in Patients Hospitalized With Hip Fracture: A Systematic Review of Instruments and Their Measurement Properties. Phys. Ther. 103 https://doi.org/10.1093/ptj/pzac142 (2022).
Warmerdam, E. et al. Long-term unsupervised mobility assessment in movement disorders. Lancet Neurol. 19, 462–470. https://doi.org/10.1016/s1474-4422(19)30397-7 (2020).
Mikolaizak, A. S. et al. Connecting real-world digital mobility assessment to clinical outcomes for regulatory and clinical endorsement-the Mobilise-D study protocol. PLOS ONE. 17, e0269615. https://doi.org/10.1371/journal.pone.0269615 (2022).
Rochester, L. et al. A Roadmap to Inform Development, Validation and Approval of Digital Mobility Outcomes: The Mobilise-D Approach. Digit. biomarkers. 4, 13–27. https://doi.org/10.1159/000512513 (2020).
Polhemus, A. et al. Walking on common ground: a cross-disciplinary scoping review on the clinical utility of digital mobility outcomes. NPJ Digit. Med. 4, 149. https://doi.org/10.1038/s41746-021-00513-5 (2021).
Kronborg, L., Bandholm, T., Palm, H., Kehlet, H. & Kristensen, M. T. Physical Activity in the Acute Ward Following Hip Fracture Surgery is Associated with Less Fear of Falling. J. Aging Phys. Act. 24, 525–532. https://doi.org/10.1123/japa.2015-0071 (2016).
Benzinger, P. et al. Geriatric rehabilitation after hip fracture. Role of body-fixed sensor measurements of physical activity. Z. Gerontol. Geriatr. 47, 236–242. https://doi.org/10.1007/s00391-013-0477-9 (2014).
Kampe, K. et al. Change of physical activity parameters of hip and pelvic fracture patients during inpatient rehabilitation and after discharge: analysis of global and in-depth parameters. Eur. Rev. Aging Phys. Activity. 18, 9. https://doi.org/10.1186/s11556-021-00261-1 (2021).
Kirk, C. et al. Mobilise-D insights to estimate real-world walking speed in multiple conditions with a wearable device. Sci. Rep. 14, 1754. https://doi.org/10.1038/s41598-024-51766-5 (2024).
Micó-Amigo, M. E. et al. Assessing real-world gait with digital technology? Validation, insights and recommendations from the Mobilise-D consortium. J. Neuroeng. Rehabil. 20 https://doi.org/10.1186/s12984-023-01198-5 (2023).
Berge, M. et al. Evaluating the Accuracy and Reliability of Real-World Digital Mobility Outcomes in Older Adults After Hip Fracture: A Cross-Sectional Study. JMIR Formative Res. https://doi.org/10.2196/67792 (2025).
Becker, C. et al. Digital mobility outcomes to describe real-world walking during recovery from a hip fracture: the Mobilise-D perspective. Eur. Geriatr. Med. https://doi.org/10.1007/s41999-025-01391-w (2026).
Terwee, C. B. et al. COSMIN methodology for evaluating the content validity of patient-reported outcome measures: a Delphi study. Qual. Life Res. 27, 1159–1170. https://doi.org/10.1007/s11136-018-1829-0 (2018).
Smith, G. T. On construct validity: issues of method and measurement. Psychol. Assess. 17, 396–408. https://doi.org/10.1037/1040-3590.17.4.396 (2005).
Hattie, J. & Cooksey, R. W. Procedures for Assessing the Validities of Tests Using the Known-Groups Method. Appl. Psychol. Meas. 8, 295–305. https://doi.org/10.1177/014662168400800306 (1984).
Del Din, S. et al. Mobilise-D Technical Implementation Manual: How to validate and measure digital mobility outcomes from a wearable device (V1.0). Zenodo. https://zenodo.org/records/14901135 (2025).
Buekers, J. et al. Digital assessment of real-world walking in people with impaired mobility: How many hours and days are needed? Int. J. Behav. Nutr. Phys. Activity. 22, 148. https://doi.org/10.1186/s12966-025-01851-3 (2025).
Kluge, F. et al. Consensus based framework for digital mobility monitoring. PLOS ONE. 16, e0256541. https://doi.org/10.1371/journal.pone.0256541 (2021).
Koch, S. et al. From high-resolution time series to a single, clinically-interpretable value - considerations for the aggregation of real world walking speed assessed by wearable sensors in patients with chronic obstructive pulmonary disease (COPD). Eur. Respir. J. 62, PA1595. https://doi.org/10.1183/13993003.congress-2023.PA1595 (2023).
Guralnik, J. M. et al. A Short Physical Performance Battery Assessing Lower Extremity Function: Association With Self-Reported Disability and Prediction of Mortality and Nursing Home Admission. J. Gerontol. 49, M85–M94. https://doi.org/10.1093/geronj/49.2.M85 (1994).
Podsiadlo, D. & Richardson, S. The Timed Up & Go: A Test of Basic Functional Mobility for Frail Elderly Persons. J. Am. Geriatr. Soc. 39, 142–148. https://doi.org/10.1111/j.1532-5415.1991.tb01616.x (1991).
Guyatt, G. H. et al. The 6-minute walk: a new measure of exercise capacity in patients with chronic heart failure. Can. Med. Assoc. J. 132, 919–923 (1985).
Haley, S. M. et al. Late Life Function and Disability Instrument: II. Development and evaluation of the function component. J. Gerontol. Biol. Sci. Med. Sci. 57, M217–222. https://doi.org/10.1093/gerona/57.4.m217 (2002).
Kempen, G. I. J. M. et al. The Short FES-I: a shortened version of the falls efficacy scale-international to assess fear of falling. Age Ageing. 37, 45–50. https://doi.org/10.1093/ageing/afm157 (2007).
Webster, K., Cella, D. & Yost, K. The Functional Assessment of Chronic Illness Therapy (FACIT) Measurement System: properties, applications, and interpretation. Health Qual. Life Outcomes. 1, 79. https://doi.org/10.1186/1477-7525-1-79 (2003).
May, J. O. & Looney, S. W. Sample Size Charts for Spearman and Kendall Coefficients. J. Biomet. Biostat. 11. https://doi.org/10.37421/jbmbs.2020.11.440 (2020).
Werner, M., Macke, C., Gogol, M., Krettek, C. & Liodakis, E. Differences in hip fracture care in Europe: a systematic review of recent annual reports of hip fracture registries. Eur. J. Trauma Emerg. Surg. 48, 1625–1638. https://doi.org/10.1007/s00068-021-01797-8 (2022).
Medin, E. et al. European Regional Differences in All-Cause Mortality and Length of Stay for Patients with Hip Fracture. Health Econ. 24, 53–64. https://doi.org/10.1002/hec.3278 (2015).
Pesudovs, K., Burr, J. M., Harley, C. & Elliott, D. B. The development, assessment, and selection of questionnaires. Optom. Vis. Sci. 84, 663–674. https://doi.org/10.1097/OPX.0b013e318141fe75 (2007).
Evans, J. D. Straightforward Statistics for the Behavioral Sciences (Brooks/Cole Publishing Company, 1996).
Fleig, L. et al. Sedentary Behavior and Physical Activity Patterns in Older Adults After Hip Fracture: A Call to Action. J. Aging Phys. Act. 24, 79–84. https://doi.org/10.1123/japa.2015-0013 (2016).
Jeon, Y. T. et al. Post-operative Physical Performance Factors Associated With Gait Speed in Patients Surgically Treated for Hip Fracture: A Cross-Sectional Study. Annals Rehabilitation Med. 43, 570–580. https://doi.org/10.5535/arm.2019.43.5.570 (2019).
Rehman, R. Z. U. et al. Investigating the Impact of Environment and Data Aggregation by Walking Bout Duration on Parkinson’s Disease Classification Using Machine Learning. Front. Aging Neurosci. 14, 808518. https://doi.org/10.3389/fnagi.2022.808518 (2022).
Studenski, S. et al. Gait Speed and Survival in Older Adults. JAMA 305, 50–58. https://doi.org/10.1001/jama.2010.1923 (2011).
Gherardini, S. et al. Prognostic implications of predischarge assessment of gait speed after hip fracture surgery. J. Geriatr. Phys. Ther. 42. https://doi.org/10.1519/JPT.0000000000000144 (2019).
Thingstad, P. et al. Identification of gait domains and key gait variables following hip fracture. BMC Geriatr. 15, 150. https://doi.org/10.1186/s12877-015-0147-4 (2015).
Prestmo, A. et al. Comprehensive geriatric care for patients with hip fractures: a prospective, randomised, controlled trial. Lancet 385, 1623–1633. https://doi.org/10.1016/S0140-6736(14)62409-0 (2015).
Hansen, M. S. et al. Very low levels of physical activity among patients hospitalized following hip fracture surgery: a prospective cohort study. Disabil. Rehabil. 21, 1–10. https://doi.org/10.1080/09638288.2025.2451769 (2025).
Howcroft, J., Kofman, J. & Lemaire, E. D. Review of fall risk assessment in geriatric populations using inertial sensors. J. Neuroeng. Rehabil. 10, 91. https://doi.org/10.1186/1743-0003-10-91 (2013).
Szabo, D. A. et al. The Role and Importance of Using Sensor-Based Devices in Medical Rehabilitation: A Literature Review on the New Therapeutic Approaches. Sensors 23 https://doi.org/10.3390/s23218950 (2023).
Pol, M. C., Riet, T., van Hartingsveldt, G., Krose, M., Buurman, B. M. & B. & Effectiveness of sensor monitoring in a rehabilitation programme for older patients after hip fracture: a three-arm stepped wedge randomised trial. Age Ageing. 48, 650–657. https://doi.org/10.1093/ageing/afz074 (2019).
Backman, C. et al. Patient-clinician digital health interventions for the hip fracture population: a scoping review. BMC Health Serv. Res. 23 https://doi.org/10.1186/s12913-023-09784-y (2023).
Acknowledgements
We extend our sincere thanks to the assessors, clinical site leads, and supporting orthopaedic surgeons in Trondheim, Oslo, Stuttgart, Heidelberg, and Montpellier for their dedication, collaboration, and good humour. In Trondheim and Oslo, we thank and acknowledge Erika Skaslien, Mari Odden, Ingalill Grøtta Midtsand, Karoline Blix Grønvik, Kjersti Opdal, Ola Grimstad, Hege Thrygg, Elise Berg Vesterhus. In Germany, we thank and acknowledge Martha Gierka, Clarissa Huber, Vanessa Zoller, Elena Litz, Jana Krespach, Carmen Lamparter, Dr. Ulrich Liener, Dr. Bernd Kinner, Dr. Markus Aarand. We greatly appreciate Lou Sutcliffe, David Singleton, Isabel Neatrour and Stefanie Mikolaizak for their support in data management, monitoring, training and supervision.
Funding
This study is part of the Mobilise-D project, which was funded by the Innovative Medicines Initiative 2 Joint Undertaking (JU) under grant agreement No. 820820. This JU received support from the European Union’s Horizon 2020 research and innovation program and the European Federation of Pharmaceutical Industries and Associations (EFPIA). This work was also supported by the National Institute for Health and Care Research (NIHR) Sheffield Biomedical Research Centre (NIHR203321). ISGlobal acknowledges support from the grant CEX2023-0001290-S funded by MCIN/AEI/ https://doi.org/10.13039/501100011033, and support from the Generalitat de Catalunya through the CERCA Program. MdlH was funded by European Union-NextGenerationEU, under the Program Investigo (INVESTIGO 2022, AGAUR- ref. BDNS 608313, file 2022 INV-1 00046 - Code 100046TC19). LR is supported by the IMI2 JU project IDEA-FAST (grant agreement 853981). LR is supported by the NIHR Newcastle Biomedical Research Centre based at The Newcastle upon Tyne Hospital National Health Service (NHS) Foundation Trust, Newcastle University, and the Cumbria, Northumberland, and Tyne and Wear NHS Foundation Trust and the NIHR/Wellcome Trust Clinical Research Facility infrastructure at Newcastle upon Tyne Hospitals NHS Foundation Trust. LR received funding from the NIHR Senior Investigator Awards (2020–2024 and 2024–2028). Content in this publication reflects the authors’ views and neither IMI nor the European Union, EFPIA, NHS, NIHR or the Department of Health and Social Care are responsible for any use that may be made of the information contained herein.
Author information
Authors and Affiliations
Contributions
Conceptualization and funding acquisition: B.C., L.R., C.B., B.V., and J.G.-A. Statistical analysis plan: M.L., A.F., A.I., V.L., J.G.-A. Data and statistical analysis: M.d.l.H, M.L, P.A., J.B., and J.G.-A. Drafting of the manuscript: T.E., M.A.B., M.L., and J.G.-A. Figure preparation: M.d.l.H. Supervision: V.L., C.B., B.V., and J.G.-A. All authors provided critical intellectual input during the preparation of the manuscript. All authors reviewed and edited the manuscript and approved the submitted version.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Eckert, T., Berge, M.A., Long, M. et al. Construct validity of real-world digital mobility outcomes in patients after proximal femoral fracture: a cross-sectional observational study. Sci Rep 16, 9535 (2026). https://doi.org/10.1038/s41598-026-43297-y
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-026-43297-y
