
Abstract
Population ageing and digital health have become important trend and challenge in today’s world development. And previous literature has concentrated on their causes and consequences. However, less is known about the bidirectional relationship between digital inclusion and healthy ageing among older adults, which is not conducive to governance of an ageing population and realization of digital health equity. Based on CHARLS database, this study empirically examines the bidirectional relationship between digital inclusion and healthy ageing using a four-wave cross-lagged model. The results show that digital inclusion significantly positively predicts healthy ageing (β = 0.049, p < 0.001; β = 0.037, p < 0.01; β = 0.086, p < 0.001). In addition, the role of healthy ageing in predicting digital inclusion is also emphasized (β = 0.057, p < 0.01; β = 0.048, p < 0.01; β = 0.043, p < 0.01). After controlling for covariates including sociodemographic characteristics, health-related behaviors and health outcomes, the bidirectional relationships are also significant (p < 0.05). Multi-group analyses indicate that these cross-lagged effects were invariant across gender, marital status, residence and income groups (p < 0.05), but varied significantly by education level (p < 0.05). And sensitivity analyses further confirm the robustness of the findings. The present study provides substantial evidence and reference for the relationship between digital inclusion and healthy ageing in Chinese context and contributes to a deeper understanding of the solution to ageing population and digital divide.
Similar content being viewed by others
Introduction
Population ageing is one of the most important social trends since the 21st century, which has a huge impact on almost all social fields such as labor force, housing, transportation and medical care. In World Population Prospects 2022, the United Nations pointed that the number and proportion of older adults in almost every country in the world today are increasing, and the growth rate of the population over 65 years old has exceeded that of the population under 65 years old (The United Nations 2022). Furthermore, the United Nations has also adopted “reduce inequalities” as one of the Sustainable Development Goals (SDG), advocating that all policies should be universal in principle and take into account the needs of marginalized groups. As one of the countries with the most serious population ageing phenomenon (Peng 2011), China has nearly 300 million people aged 60 and over, which has entered the moderately ageing society. The acceleration of the ageing process and the fluctuation of population trend bring serious challenges to the population health and medical security in China (Fang et al. 2015). Therefore, how to actively deal with population ageing in China is of great value for promoting the high-quality development of population, economy and society and realizing the strategy of “healthy China” (Luo et al. 2021).
In the face of the increasingly severe phenomenon of population ageing in countries around the world, the World Health Organization proposed the issue of healthy ageing at the end of the 20th century, which refers to the process of developing and maintaining the functional ability of the older adults to achieve their well-being (Michel and Sadana 2017; Rudnicka et al. 2020). Functional ability mainly includes the ability of older adults to meet basic needs, learn, establish and maintain relationships, and contribute to society (Beard et al. 2016). A systematic review further indicates that the realization of healthy ageing is closely related to factors in three dimensions: physical well-being, mental/cognitive well-being and social well-being (Abud et al. 2022), which is consistent with the definition of the three main domains of health by the WHO (WHO 2021). Physical well-being covers physical activity and diet (Chen et al. 2020; Lucas et al. 2018), which emphasizes maintaining good physical ability to promote successful healthy ageing. Mental/cognitive well-being includes self-awareness, outlook/attitude, life-long learning and faith. They promote healthy ageing by enhancing the ability of older adults to adapt to changes, encouraging them to have a good outlook and attitude towards the future, and maintaining good cognitive functions (Ploughman et al. 2012; Amosun and Harris 2020). Social well-being encompasses social support, financial security and community engagement, which achieve healthy ageing by establishing harmonious social relationships, maintaining a good quality of life, and enhancing a sense of purpose (Amosun and Harris 2020). Furthermore, Lu et al. (2021) pointed out that education is the strongest socioeconomic predictor of healthy ageing by comparing the socioeconomic inequality in healthy ageing in the United States, the United Kingdom, China and Japan. Adults with higher level of education tends to have a greater emphasis on health, income level, and occupational status (Wang and Yu 2016), and thus more likely to enjoy a healthier work and life, stronger economic and social security, and more active social participation (Lu et al. 2021), so as to better achieve healthy ageing. Since entering the 21st century, China has also taken the realization of healthy ageing as one of the important national strategies to promote the high-quality development of ageing causes and industries, and has successively promoted the realization of healthy ageing strategies through strengthening health education, improving the medical and health care service system, and further promoting the combination of medical and nursing care (Chen et al. 2019; Chen et al. 2023; Yu 2021).
Digital solutions play a key role in safeguarding the social and economic well-being of older adults (Zhou and Ye 2023). With the rise of data-driven technology represented by artificial intelligence technology, wearable devices, and smartphone applications, it directly promotes the development of global healthcare by facilitating the change of health behavior, tracking the change of health status, and optimizing the interaction of health systems, and can also help realize digital healthy ageing (Gariboldi et al. 2023). Digital inclusion is the process of bridging the digital divide and reducing digital health inequalities, which means that individuals and communities use information and communication technologies without barriers to access to information, can effectively participate in all aspects of knowledge society and economic development, and reap social benefits according to their will and ability (Yang et al. 2022). Current research has demonstrated the positive impact of digital inclusion on the physical, mental and spiritual health of older adults. The use of the Internet and mobile communication technologies in older persons can improve their cognitive abilities (Ordonez et al. 2011), strengthen their relationships with family and friends and reduce loneliness (Blazun et al. 2012), enhance their self-efficacy (Wong et al. 2014), and promote their social participation and integration (Wong et al. 2014). This in turn improves community satisfaction and quality of life, all of which are closely related to healthy ageing. Conversely, healthy ageing prioritizes maintaining health and autonomy (Yu 2020), motivating older adults to engage in novel roles and activities to preserve functional abilities. Advancing healthy ageing not only strengthens their proactive engagement in societal participation but also expands their access to acquiring new skills, knowledge, and resources (Ragnedda et al. 2022), thereby increasing their willingness to engage in digital health. Thus, digital health and healthy ageing continuously reinforce each other, nurturing a mutually beneficial bidirectional relationship.
However, due to low digital health literacy, low confidence and motivation in the use of digital technologies, and low age-suitability of products, older adults are largely digitally marginalized (Gariboldi et al. 2023; Lee and Coughlin 2015). In particular, with the increasing use of digital technologies in the field of healthcare for the old and public health, AI technologies may exacerbate or introduce new forms of age discrimination (World Health Organization 2021). The original intention of the rise of digital health technology is to improve people’s health and well-being, rather than to widen existing health gaps or create new health gaps (Jaworski and Hooper 2023), so improving the digital inclusion of older adults and realizing digital health equity has far-reaching significance in narrowing the social gradient of health and ensuring that all people enjoy the digital health dividend.
So far, the rationale for focusing our investigation on the bidirectional relationship between digital inclusion and healthy ageing is to bridge the noted gap in the literature. The interplay between digital inclusion and healthy ageing represents a pivotal focus in public health and social policy research. Although existing researches emphasize a potential correlation between these constructs, the temporal sequence and reciprocal dynamics remain poorly understood. Especially previous literatures used cross-sectional research designs or relatively small sample sizes (Lu et al. 2022), resulting in the lack of large sample longitudinal data studies on the impact between digital development and population ageing. Moreover, a large number of studies derived from Western contexts (Santini et al. 2020; Danesin et al. 2025), whose socioeconomic structures, cultural norms, and policy regimes differ fundamentally from China’s. This contextual divergence potentially influenced the relationship between digital inclusion and ageing outcomes, limiting the generalizability of existing findings and underscoring the necessity for population-specific investigations. To our knowledge, no study to date has employed a longitudinal design to rigorously model the bidirectional pathways between digital inclusion and healthy ageing in a Chinese cohort, leaving a critical gap in understanding the temporal precedence and mutual reinforcement of these two processes. Clarifying the impact mechanism between digital inclusion and healthy ageing not only provides an important theoretical perspective and policy grip for dealing with population ageing, but also provides a theoretical basis and practical perspective for solving the key pain points of digital health construction and realizing digital health equity. Therefore, this study seeks to contribute to the existing literature by using a cross-lagged panel model to analyze the bidirectional relationship between digital inclusion and healthy ageing among middle-aged and older adults in China based on four waves of CHARLS study. We aim to shed new light on the empirical evidence that supports the realization of healthy ageing and digital health equity in China and other similar contexts.
Digital inclusion
Digital inclusion has emerged as a critical societal goal amidst global digital transformation, with its absence—digital exclusion—posing a particular threat to the health and well-being of older adults. Digital divide traditionally refers to the gap in adequate physical access to information communication technology and infrastructure (Lythreatis et al. 2022). When this access gap leads to individuals’ inability to participant fully in digital society compounded by a lack of digital skills and opportunities, it culminates in digital exclusion—a state of societal marginalization arising from limited or insufficient internet access (Ge et al. 2025). Consequently, digital inclusion is the proactive process and desired outcome of overcoming digital divide and preventing digital exclusion, ensuring both effective digital access and meaningful participation in the digital society.
Scholarly conceptualizations of digital inclusion itself can be broadly categorized into two complementary perspectives, which carry distinct implications for academic measurement and policy practice. The behavior-oriented perspective, exemplified by Lu et al. (2022), defines digital inclusion as the absence of inequality in the access and used of information and communication technologies. This view prioritizes measurable actions and availability, directing research towards indicators like Internet penetration rate, device ownership, and usage frequency. In contrast, the outcome-oriented perspective, articulated by Seifert et al. (2021), emphasizes the ultimate goal of social participation, defining digital inclusion as the state where individuals are not excluded from societal domains dominated by digital technologies. This standpoint shifts the focus from mere Internet usage to tangible consequences of digital engagement, advocating for policy measures that ensure digital services lead to improved health outcomes, social connection and civic engagement. Furthermore, the multi-dimensional conceptual model of information society inequality proposed by De Haan (2004) contributes to better clarify the relationship between various influencing factors of digital inclusion. This model classifies these factors into individual factors (e.g., age, education, cognitive ability) and structural factors (e.g., education system, labor market demands, policy frameworks), which interact to create imbalances in resources, and in turn drive the process of digital exclusion. For older adults, this dynamic is particularly pronounced, as digital exclusion can exacerbate existing social and health disparities (Barnett et al. 2021), while bridging digital divide can help reduce health inequities on a global scale and promote digital inclusion (Lu et al. 2022).
Therefore, enhancing digital inclusion for older adults is not merely a technical challenge but a multifaceted societal imperative, and synthesizing the behavioral and outcome perspectives is of vital significance. Policies should not only ensure access but also foster the digital skills and design the inclusive environments necessary to translate digital engagement into tangible benefits for healthy ageing. This integrated approach is fundamental to modernizing social governance and ensuring that the digital dividend is universally shared.
Healthy ageing
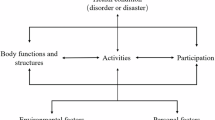
The conceptual evolution of the World Health Organization’s “Healthy Ageing” reflects a profound theoretical shift from a biomedical focus to a holistic and person-centered paradigm. Healthy ageing was proposed by WHO at the 40th World Health Assembly in 1987, which refers to the process of developing and maintaining the functions required for healthy life in old age (Beard et al. 2016). The concept of healthy ageing breaks through the traditional negative view of population ageing and puts forward new methods and ideas to solve this problem. On this basis, a significant theoretical expansion occurred in 2002 with the introduction of the “active ageing” concept, which incorporated the social environment as a critical determinant of the ageing experience and emphasized improving the quality of life of older adults (WHO 2002). This marked a pivotal move beyond individual physiology towards a socio-ecological understanding. The 2015 World report on ageing and health represents the most integrative theoretical framework to date (WHO 2015). It synthesizes prior concepts by explicitly integrating the dynamic interplay between intrinsic capacity (the composite of individuals’ physical and mental attributes), functional ability (the ability to perform activities valued by individuals), and the environment (encompassing social, policy, and physical contexts). This framework theoretically redefines healthy ageing not as the absence of disease, but as the process of developing and maintaining functional capacity that enables well-being of older adults. It establishes that functional capacity is an emergent property of the interaction between individuals and their environment, providing a comprehensive systems-level lens through which to view population ageing and guide public health action (Beard et al. 2016).
Furthermore, previous studies have shown that factors such as better health conditions (Nguyen et al. 2020), higher education level (Lu et al. 2021), more regular lifestyles (Caballero et al. 2017), higher socioeconomic status (Wu et al. 2020), and higher level of income (Lu et al. 2021) are crucial to the realization of healthy ageing. In recent years, the combination of healthy ageing and various fields has made remarkable progress, especially in the field of digitalization. Smart sensors, wearable devices and artificial intelligence technology are used to monitor the physiological data (such as heart rate, blood pressure, blood sugar) and activities of older adults in real time, providing personalized health management and early warning services. This technology can not only help older adults find health problems in time, but also respond quickly in emergency situations to ensure the safety of them (Chen et al. 2023). In addition, the research on healthy ageing and psychological factors began to shift from the external environment to the psychological motivation of older adults and the subjective willingness to achieve healthy ageing. Research shows that healthy ageing depends not only on an individual’s health goals and motivations, but also on the effort they put into achieving those goals. By implementing interventions such as task prompting and emotion regulation, efforts to mobilize on healthy behaviors in older adults can be promoted (Hess et al. 2021).
Digital inclusion and healthy ageing
Social capital theory (SCT) provides a powerful framework for understanding how resources embedded within social networks can be accessed and mobilized to facilitate collective action and enhance individual well-being (Halpern 2005). According to SCT, social capital comprises three distinct while interconnected dimensions: structural capital, relational capital, and cognitive capital (Nahapiet and Ghoshal 1998). Structural capital refers to the overall pattern and network configuration of social relations, such as the connections, rules and procedures between individuals. Relational capital is defined as the quality of interpersonal relationships formed through long-term interaction, such as trust, obligation, recognition and reciprocal norms. And cognitive capital is the shared codes, languages, narratives, and values within a group (Nahapiet and Ghoshal 1998).
On the one hand, the development of digital health provides a new technological path and perspective for the realization of healthy ageing, which requires health system and social change (Danesin et al. 2025). Based on SCT, digital inclusion acts as a catalyst for healthy ageing by empowering older adults to build and mobilize social capital. At structural level, digital platforms expand the scale and diversity of older adults’ social networks, increasing the frequency and durability of interactions with their family, friends and community members. And at relational level, frequent and effective online communication helps to maintain and deepen relational social capital through fostering trust and reinforcing norms of reciprocity. When facing health challenges, the trusted network can swiftly provide emotional support and practical assistance. When it comes to cognitive level, internet access allows older adults to engage with mainstream cognitive social capital, such as acquiring digital health literacy and understanding online service protocols, thereby bridging the value and knowledge gap with younger generations (Danesin et al. 2025). Therefore, improving the digital inclusion of older adults and reducing their social inequality in digital technology can better solve the dilemma of population ageing.
On the other hand, healthy ageing emphasizes the importance of health and independence (Yu 2020), which encourages older adults to take on new roles and activities in order to maintain their functional capacity. And healthy ageing facilitates digital inclusion by enhancing older adults’ capacity to accumulate and utilize social capital. The high levels of physical, cognitive and psychological function emphasized by healthy ageing are fundamental prerequisites for active social participation and capital accumulation. For example, good cognitive and physical function enables older adults to learn how to use digital devices and engage in online social interactions (Ragnedda et al. 2022). And positive psychological state and social role identity motivate them to actively maintain relationships, for which digital tools are highly efficient. Hence, promoting the realization of healthy ageing of older adults can also enhance their subjective initiative of social participation, increase their opportunities to acquire new skills, knowledge and information (Ragnedda et al. 2022), and then increase their initiative to use digital health technology, so as to better contribute to the realization of digital inclusion and digital health equity.
As one of the most serious public health challenges facing the world today, population ageing will increase the population vulnerability and future health burden of countries around the world (Chen et al. 2024). UN indicated that the number of people aged 65 and above is expected to exceed that of those under 18 by the end of the 2070 s. Currently, China has entered a period of deep population ageing and the degree of ageing is at a medium to high level globally, presenting the characteristics of a large older population, a rapid ageing process and significant urban-rural differences. Researches showed that compared with the US, England and Japan, whose problem of population ageing is also particularly severe, the degree of education and income inequality for healthy ageing in China is significantly higher (Lu et al. 2021). According to official statistics released in January 2025, China’s internet user population surpassed 1.108 billion, among which the group of Internet users aged 60 and above accounted for only 14.1%. As the digitally marginalized population, older adults demonstrate significant deficiencies in digital competencies, informational navigation skills, and technological knowledge acquisition (Cui et al. 2024). In the Blue Book on the Development of Healthy Ageing in China (2023–2024), it is also clearly proposed that digital wisdom means should be more efficient, accurate, and secure in actively responding to population ageing strategies, and improve the social ageing service capacity and social adaptability of older adults (Wang 2024). Therefore, focusing on China to explore the relationship between digital inclusion and healthy ageing can, by analyzing the structural contradictions in the digital transformation of the world’s largest ageing society, reveal the complex interaction mechanism between technological empowerment and ageing social governance in the development process of an ageing society, and provide a transferable practical model for developing and even developed countries around the world to deal with the silver wave.
In conclusion, current research on the reciprocal relationship between digital inclusion and healthy ageing is still limited. On the one hand, literatures focus more on macro policies and case analyses, while there is insufficient micro-empirical evidence for digital development and healthy ageing (Gariboldi et al. 2023). On the other hand, previous studies mainly used cross-sectional research designs or small-sample studies (Lu et al. 2022), lacking large-sample longitudinal data studies. It has significant disadvantages, one is that it will produce bias caused by common methods, the other is that the reliability of causal inference needs to be verified (Podsakoff et al. 2003), and the direction of the relationship between variables in the dynamic time span cannot be defined. It’s extremely imperative to reveal the bidirectional relationship between digital inclusion and healthy ageing.
The present study
The purpose of this study is to explore the relationship between digital inclusion and healthy ageing in older adults in China. First, this study uses four waves of CHARLS data from 2011 to 2018 to empirically test the longitudinal relationship between digital inclusion and healthy ageing. To address the limitations of cross-sectional data analysis, we adopted cross-lagged research design to better clarify the influence mechanism between digital inclusion and healthy ageing, and strengthen causal inference. Secondly, this study takes the middle-aged and older adults in China as the research object, and expands the research perspective of China’s ageing social governance system. The ageing society of different countries has different characteristics. Our research further explores the evidence of population ageing in the Chinese cultural background, and provides reference for promoting the digital healthy ageing to the in-depth development and exploration of the construction of the Chinese-style healthy ageing model. To sum up, based on literature and relevant theories, this study puts forward the following hypothesis:
H1: Digital inclusion can positively predict healthy ageing.
H2: Healthy ageing can positively predict digital inclusion.
H3: There are bidirectional effects between digital inclusion and healthy ageing.
Methods
Sample and data collection
Data were obtained from China Health and Retirement Longitudinal Survey (CHARLS) which is conducted among Chinese individuals and households aged 45 and above in 28 provinces across China and aims to build a high-quality public micro-database. The information collected covers the socio-economic status and health status of multi-dimensional information in order to meet the needs of scientific research on ageing (Cheng et al. 2024; Zhao et al. 2014). The survey was carried out in five waves: 2011(Wave 1), 2013(Wave 2), 2015(Wave 3), 2018(Wave 4) and 2020(Wave 5), covering over 150 counties and 450 communities with a total of near 20,000 participants from over 12,000 households. This dataset provides a valuable resource for interdisciplinary studies addressing ageing-related issues. Comprehensive information regarding the CHARLS dataset is available at the official website: https://charls.pku.edu.cn/.
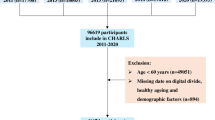
Given that more than 50% of the healthy ageing indicators were not measured in Wave 5, this study utilized data from wave 1 to 4, with the 2011 wave designated as the baseline. The baseline cohort comprised 17,708 participants. And we excluded participants who were lost to follow-up in wave 2 to wave 4 (n = 5,727), those under the age of 45 (n = 248), those with missing data for digital inclusion (n = 129), and those with missing covariate information, including age, gender, education level, residence, marital status, personal income, household registration, smoking status, alcohol consumption, chronic diseases, self-rated health, and depressive symptoms (n = 8,713). The final analytical sample consisted of 2,891 participants (see Fig. 1).

Flow of participants into study sample.
Before each wave of CHARLS survey, every participant would be informed about the content and sign an informed consent form by interviewers. All the survey data are strictly confidential and protected by data security and privacy laws. In addition, each round of CHARLS survey was approved by the Biomedical Ethics Committee of Peking University in accordance with the Declaration of Helsinki (ethical approval number IRB00001052-11015) (Zhao et al. 2023).
Variables
Digital inclusion
Data on digital inclusion were collected through self-reported questionnaires. In CHARLS survey, it was assessed using two questions “Have you used the Internet in the past month” and “How often in the last month did you use the Internet” (Lu et al. 2022; Zhao et al. 2022; Li and Liu 2025). The answers to the former question are “yes” (1 point) and “no” (0 point), while the latter question are “almost daily” (3 points), “almost every week” (2 points) and “not regularly” (1 point). The scores were added together, ranging from 0 to 4.
Healthy ageing
We applied the indicators developed by Ageing Trajectories of Health Longitudinal Opportunities and Synergies (ATHLOS) project to measure healthy ageing (Sanchez-Niubo et al. 2021). It is the most widely used and reliable comprehensive indicators for healthy ageing using harmonized data from 16 cohorts from 38 different countries on six continents (Cheng et al. 2024; Critselis et al. 2020). The ATHLOS scale consist of 31 items for CHARLS and is scored using a unidimensional, two-parameter logistic model (2PLM) of Item Response Theory (IRT), and the endorsement probability of a specific response category is modeled as a function of item discrimination and difficulty, and a person parameter (Sanchez-Niubo et al. 2021), which has been proved to converge successfully with excellent model fit (CFI = 0.99, TLI = 0.99, RMSEA = 0.03) (Sanchez-Niubo et al. 2021; Stepaniak et al. 2024; Li et al. 2022). The scale covers domains on cognition (memory, immediate recall, delayed recall, orientation in time), psychology symptoms (sleeping), vitality (pain, energy, et al.), sensory (eyesight, hearing, et al.), mobility (stooping, lifting, climbing stairs, et al.), activities of daily living (getting in or out of bed, shopping, bathing, et al.), and instrumental activities of daily living (doing housework, managing money, et al.). In this study, we followed Cheng et al. and excluded the making telephone calls and walking speed items from CHARLS since there were not evaluated in wave 1 and wave 4 respectively (Cheng et al. 2024). Ultimately, we added up the scores of all the indicators to obtain the score for healthy ageing, ranging from 0 to 29.
Covariate
This study systematically addressed potential confounders associated with both digital inclusion and healthy ageing. Based on prior literature (Lu et al. 2022; Zhang et al. 2023; Cheng et al., 2024; Wang et al., 2024; Wang et al., 2025), we adjusted for a range of covariates, including sociodemographic characteristics, health-related behaviors, and health outcomes. Sociodemographic characteristics consist of age (1 = under 60, 2 = greater than or equal to 60), gender (1 = male, 2 = female), education level (1 = primary school or below, 2 = junior high, 3 = senior high or vocational, 4 = college or above), residence (1 = rural, 2 = urban), marital status (1 = married, 2 = unmarried), household registration (1 = agricultural, 2 = non-agricultural, 3 = unified resident registration), and personal income (1 = income present, 2 = no income). Health-related behaviors encompassed smoking status (1 = smoker, 2 = never smoked) and alcohol consumption (1 = drinker, 2 = never drunk). Health outcomes included self-rated health (1 = excellent, 2 = very good, 3 = good, 4 = fair, 5 = poor), chronic disease conditions (hypertension, dyslipidemia, diabetes or high blood sugar, cancer or malignant tumor, chronic lung diseases, liver disease, heart attack, stroke, kidney disease, stomach or other digestive disease, emotional, nervous, or psychiatric problems, memory-related disease, arthritis or rheumatism, and asthma), the number of chronic diseases (1 = none, 2 = one, 3 = more than one) and depression (1 = rarely or none, 2 = some or a little of the time, 3 = occasionally or a moderate amount of the time, 4 = most or all of the time). All covariates were assessed at baseline wave to reduce model complexity (Wang et al. 2025).
Statistical analyses
Continuous variables were described by means (standard deviations) and categorical variables were expressed as frequencies (percentages) to comprehensively summarize the characteristics of research sample. To investigate the bidirectional relationship between digital inclusion and healthy ageing among Chinese older adults, a cross-lagged panel model was developed with sequential adjustment for covariates. More precisely, standardized coefficients were reported for four models. Model 1 is an autoregressive model designed to test the stability of digital inclusion and healthy ageing from wave 1 to wave 4. Model 2 is a crude cross-lagged panel model without adjustments that include all the autoregressive paths and cross-lagged paths to analyze the bidirectional relationship between digital inclusion and healthy ageing. Model 3 adjusted for age and gender based on Model 2. And Model 4 additionally accounted for marital status, self-rated health, smoke, drink, the number of chronic diseases and depression, alongside age and gender. Model fit was assessed using the comparative fit index (CFI), the Tucker-Lewis index (TLI), the root mean square error of approximation (RMSEA), and standardized root mean square residual (SRMR). Acceptable model fit was defined by CFI > 0.90, TLI > 0.90, RMSEA < 0.06, and SRMR < 0.06 (Hu and Bentler 1999). Furthermore, we conducted subgroup analyses to examine potential variations in the associations. Participants were stratified by key characteristics, including gender, marital status, education level, residence, and personal income. To further assess the robustness of our findings, we conducted a series of sensitivity analyses following established methodologies (Li and Liu 2025; Wang et al. 2025). First, we individually controlled for 14 specific chronic conditions in place of the aggregate chronic disease count used in the primary model (Model 4). Second, to address potential bias from incomplete responses of healthy ageing, we employed multiple imputation, generating and analyzing several complete datasets to compare with the original results. Using a fully conditional specification approach, five imputed datasets were generated with 10 iterations per imputation. And logistic regression was used to conduct independent statistical analysis on each imputed dataset. Finally, we included digital exclusion as an alternative variable, which was defined based on two questions: (1) Have you used the internet in the past month; (2) Does your residence have broad-band internet connection. Responding “no” to either question was categorized as digitally excluded (coded as 0), otherwise as nondigitally excluded (coded as 1). All statistical analyses were conducted using Mplus version 8.3 and SPSS 27.0, and maximum likelihood robust estimator was used. All p-values were two-sided, and the significance level was 0.05.
Results
Baseline characteristics
Table 1 summarizes the baseline characteristics of the study participants. In the total sample, 47.5% were male, 32.1% had attained at least a primary education, and 81.9% resided in rural areas. In terms of social demographics, 82.1% were married and 81.0% had agricultural household registration. Regarding health-related lifestyle behaviors, 61.3% were non-smokers and 67.2% did not consume alcohol. With respect to health status, 24.5% reported good self-rated health, 43.4% experienced little or no depressive symptoms, and 31.0% had no chronic diseases.
Bidirectional relationship between digital inclusion and healthy ageing
Our study examined the relationship between digital inclusion and healthy ageing by constructing cross-lagged panel models, and it shows a satisfying fit to the data: RMSEA = 0.035, CFI = 0.985, TLI = 0.950, SRMR = 0.023. The standardized coefficients of autoregressive and cross-lagged path are presented in Table 2. In model 1, we incorporated digital inclusion and healthy ageing from wave 1 to 4. The autoregressive effects of both variables were significant, indicating that the variables were stable among the four time points. In model 2, we included cross-lagged path on the basis of controlling the autoregressive effect. The results revealed that the predictive effects of digital inclusion on healthy ageing were all significant from wave 1 to 4 (β = 0.049, p < 0.001; β = 0.037, p < 0.01; β = 0.086, p < 0.001). And the predictive effects of healthy ageing on digital inclusion were also significant from wave 1 to 4 (β = 0.057, p < 0.01; β = 0.048, p < 0.01; β = 0.043, p < 0.01) as shown in Fig. 2. This suggested the presence of bidirectional increase effects between them. In model 3 we included age and gender as the covariate, and in model 4 marital status, self-rated health, smoke, drink, the number of chronic diseases and depression were also included. The results showed that the cross-lagged effects remain robust (see Table 2).

Cross-lagged models between digital inclusion and healthy ageing in model 2.
Subgroup analysis
A multi-group analysis grouped by gender, marital status, education level, residence, and personal income was conducted to examine differences in the cross-lagged panel model. We constructed constrained models respectively based on different grouping criteria, assumed that the coefficient of cross-lagged paths among each subgroup were equal, and compared them with the unconstrained models to test whether there were any differences. The results indicated that there was no significant difference among different gender groups (\(\Delta {\chi }^{2}\) = 11.776, \(\Delta {df}\)=6, p = 0.067å 0.05), marital status groups (\(\Delta {\chi }^{2}\,\)= 4.467, \(\Delta {df}\)=6, p = 0.6137å 0.05), residence groups (\(\Delta {\chi }^{2}\) = 7.086, \(\Delta {df}\)=6, p = 0.313å 0.05), and personal income group (\(\Delta {\chi }^{2}\) = 5.313, \(\Delta {df}\)=6, p = 0.5043å 0.05). However, different education level groups illustrated significant difference (\(\Delta {\chi }^{2}\,\)= 35.129, \(\Delta {df}\)=18, p = 0.009 < 0.01).
Sensitivity analysis
To ensure the robustness of our findings, we conducted multiple sensitivity analyses (see Table 3). First, when controlling for 14 specific chronic diseases at baseline rather than the total count, all cross-lagged path estimates retained statistical significance (Model 5). Second, results remained consistent when multiple imputation was applied to handle missing data, supporting the reliability of the original associations (Model 6). Finally, re-estimating the models using digital exclusion as the independent variable yielded substantively unchanged results, further confirming the stability of our conclusions (Model 7).
Discussion
This study represents the first large-scale longitudinal investigations into the bidirectional relationship between digital inclusion and healthy ageing among middle-aged and older adults in China. Our findings advance the understanding of how digital inclusion and healthy ageing mutually reinforce each other over time, while highlighting critical disparities across socioeconomic and demographic groups. These results carry significant theoretical, practical, and policy implications for addressing population ageing and advancing digital health equity, and provides new evidence and understanding of the relationship between digital inclusion and healthy ageing in the Chinese context. The results of descriptive statistical analysis showed that the level of healthy ageing of middle-aged and older adults in China generally shows a downward trend, which is consistent with the research conclusion of Lu et al. (2022). At the same time, they also found that there is no significant linear or non-linear relationship between the age of middle-aged and older adults in China and healthy ageing, which is exactly the opposite of the situation in the United States, the United Kingdom and Japan. This further indicates that the connotation of healthy ageing should not only emphasize physical health, cognitive health and social health also need to be given due attention (Abud et al. 2022), which is also consistent with the definition of the connotation of health by WHO. Current research on healthy ageing mainly focuses on meeting basic needs, activity capabilities and mental health, while research on functional capabilities such as decision-making, establishing and maintaining relationships, and contributing to society is relatively lacking (Zhao et al. 2023). Our research conforms to the development trend of the digital age, exploring the bidirectional relationship between digital inclusion and healthy ageing, which is of great value for comprehensively promoting the functional capabilities of older adults.
To further test the bidirectional predictive relationship between digital inclusion and healthy ageing, we used a four-wave cross-lagged analysis, and cross-lagged panel analyses robustly confirm a reciprocal relationship between digital inclusion and healthy ageing, supporting the “virtuous cycle” hypothesis. This bidirectional linkage underscores the need to reconceptualize digital inclusion not merely as a tool for healthy ageing but as an integral component of the ageing process itself (Gariboldi et al. 2023). Notably, the relationship exhibits marked heterogeneity on education level. Existing research indicates that individuals with lower education levels derive disproportionately greater benefits from digital inclusion, suggesting that digital technologies may partially mitigate socioeconomic disparities in ageing outcomes, which challenges assumptions about technology exacerbating inequalities (Jaworski and Hooper 2023). This aligns with Lu et al.‘s (2021) emphasis on education as a socioeconomic determinant of healthy ageing, and reveals that targeted digital interventions could serve as compensatory mechanisms for disadvantaged groups. Existing research demonstrates that moderate Internet engagement offers multifaceted health benefits for older adults facing chronic conditions. Scholars have identified that online health information accessibility serves as a key mechanism through which digital connectivity enhances older adults’ quality of life (Hu et al. 2024; Choi and DiNitto 2013). This technological engagement not only facilitates better chronic disease management but also fosters cognitive resilience by strengthening digital literacy confidence, thereby promoting greater independence in daily functioning (Cilli et al. 2023). Furthermore, digital platforms act as social bridges that enhance intergenerational connectivity, with studies indicating significant positive correlations between Internet use and both psychological well-being and mental health outcomes (Zhao et al. 2022; Marcus et al. 2009). Therefore, the cumulative evidence suggests that strategic Internet adoption can simultaneously address physical health challenges while nurturing social-emotional wellness in ageing populations.
The three major aspects of healthy ageing are individual health, overall health and human environment health (Wu et al. 1997). This study finds that digital inclusion can promote the realization of healthy ageing from all the three aspects, and integrates and develops the conclusions of the above research. In addition, digital exclusion creates digital health inequalities that contribute to other socioeconomic inequalities (Pérez-Amaral et al. 2021), so it is imperative to identify ways to increase digital inclusion among older adults. A very typical example is the serious underrepresentation of middle-aged and older adults among technology developers, which makes it difficult for the legitimate concerns of older adults to be fully taken into account, further exacerbating digital health inequalities (Lee and Coughlin 2015). The promotion of healthy ageing can improve the cognitive and physical functions of older adults, reduce social isolation, and improve social connections (Merchant et al. 2021), thus improving the participation of the middle-aged and older adults in society, increasing their opportunities to acquire new skills, knowledge and information, and then improving their digital inclusion, bridging the digital divide, and realizing digital health equity (Adler-Milstein 2021). This is consistent with the conclusion of this study, that healthy ageing can better promote the digital inclusion of older adults and achieve digital healthy ageing. Furthermore, while the observed cross-lagged path coefficients are statistically significant, their modest magnitude warrants substantive meaningfulness. It’s worthing noting that in complex longitudinal models involving multifaceted societal-level constructs like digital inclusion and healthy ageing, even small coefficients can be theoretically and practically meaningful (Ferguson 2009). The cross-lagged effect identified represent the predicted change over a two-year or three-year internal, and the persistence of these bidirectional effects across multiple waves suggests a potential for cumulative impact over long term (Ferguson 2009). Small but steady annual gains in functional ability can compound into substantively significant differences in health trajectories over a decade driven by digital engagement.
Implications
This study provides valuable insights into the governance practices of population ageing. Theoretically, it establishes a reciprocal dynamic between digital inclusion and healthy ageing in older adults, creating an empirically-grounded conceptual framework that addresses both ageing society challenges and digital health disparities. By systematically demonstrating how these dimensions mutually reinforce each other, the research provides novel explanatory mechanisms for developing integrated solutions to population ageing while achieving digital health equity.
At the level of practical governance, it is necessary for government management departments and older adults to pay more attention to digital healthy ageing. As digital health becomes more widely used in the field of knowledge and practice to develop and use digital technologies to improve health (Crawford & Serhal, 2020), it also plays a more important role in achieving healthy ageing of older adults. For example, the S-Health mobile app launched by the Vietnamese government and the 5 G mobile app for Ageing launched by the Thai government aim to promote the health level of older adults through mobile application technology. In the 14th Five-Year Plan for Healthy Ageing, the Chinese government has also clearly pointed out that it will innovate the ways of providing health services for older adults, and encourage the use of information technologies to expand the space and content of services such as medical treatment, nursing and rehabilitation. Therefore, in the future, multiple departments should be committed to building a digital inclusive healthy ageing system, improve the digital inclusion of older adults from the aspects of digital health literacy improvement, digital health technology transformation, digital health education (Gariboldi et al. 2023), and enhance the sense of digital acquisition of older adults. Moreover, they can also build a comprehensive digital inclusive healthy ageing system from various aspects such as policies, technologies and services to promote the comprehensive well-being of older adults and realize digital health equity. At the same time, the ageing policy design should implement the people-oriented concept, and build an all-age friendly digital inclusive society through multi-subject consultation and co-governance (Chu et al. 2022). In addition, older adults should also give full play to their subjective initiative, actively participate in social exchanges, take the initiative to improve digital health literacy (Choukou et al. 2022), better integrate into the development of digital health society, and take practical actions to improve the level of healthy ageing and digital society participation of individuals, so as to achieve the improvement of health status and life expectancy.
Limitation and future directions
First, the CHARLS data used in this study were all from the questionnaire responses of Chinese middle-aged and older adults, and these data may still have problems such as subjectivity and social cancellation bias (Cao and Ji 2024). Furthermore, population weights were not utilized to adjust the representativeness of the sample. Although CHARLS database fully considered the randomness of sample selection and sample weights during the sampling survey, the deleted sample size due to the excessive missing values may also lead to a reduction in the representativeness of the samples. In addition, due to the limitations of the CHARLS database, although there have been five waves of data research, the results of the latest fifth wave in 2020 are missing a large number of indicators related to healthy ageing. Therefore, this study only included four waves of research data from 2011 to 2018. Major public health emergencies in 2020 have had a significant impact on the health of older adults and may affect their level of healthy ageing. Future studies could explore this mechanism through public health modeling.
Second, the cross-lagged panel model is used in this study to avoid the drawbacks of cross-sectional design. However, considering that longitudinal data itself is a kind of multi-level data, the sources of variable variation can be naturally classified into between-person level and within-person level, while CLPM confuses the two distinct levels of effects (Hamaker 2023), leaving the blend of effects uninterpretable. In future research, more sophisticated longitudinal research designs can be taken into consideration, such as latent growth curve model, latent change score model, random intercept cross-lagged panel model, to further improve the quality of research data.
Third, although Ageing Trajectories of Health Longitudinal Opportunities and Synergies (ATHLOS) has provided reliable indicators for measuring healthy ageing using CHALRS database, due to the limitations of secondary data, this study referred to previous studies and deleted making telephone calls and walking speed items because they were not considered in at least two rounds of surveys. Furthermore, ATHLOS also provides indicators of healthy ageing for the ageing databases of other countries (like Health and Retirement Study in the US, English Longitudinal Study of Ageing in the UK, Survey of Health, Ageing and Retirement in Europe). However, some dimensions that were not measured in CHARLS database while measured in other databases could not be deeply examined in this study, such as verbal fluency, processing speed, and numeracy. All of these issues may cause incomplete measurement of healthy ageing to a certain extent. Future studies could consider enriching more dimensions to measure the healthy ageing status older adults more comprehensively.
Fourth, the aim of this study is to provide new empirical evidence for the bidirectional relationship between digital inclusion and healthy ageing, which conduct preliminary exploration for the investigation of this relationship. On this basis, future studies can be enriched by incorporating mediation and moderation models. For example, explore the mediation role of social participation and digital health literacy, as well as the influence of e-skill self-efficacy as a boundary condition.
Conclusion
Based on the four-wave longitudinal data from the CHARLS database, this study empirically examined the bidirectional predictive relationship between digital inclusion and healthy ageing among middle-aged and older adults in China. The results illustrated that digital inclusion significantly positively predicts healthy ageing, and healthy ageing can also positively predict digital inclusion. There is a virtuous circle relationship between them. This study highlights the importance of digital inclusion in promoting healthy ageing and provides a theoretical foundation for addressing population ageing. It emphasizes the need for government to focus on digital health for older adults. Various governments are already implementing digital health initiatives. Future efforts should focus on building a comprehensive digital inclusive healthy ageing system, improving digital literacy among older adults, and implementing people-oriented policies for an age-friendly and digitally inclusive society. Older adults are also encouraged to actively participate in digital health society and improve their healthy ageing and digital participation levels.
Data availability
The data sets generated and analyzed in this study are available from the corresponding author upon reasonable request.
References
Abud T, Kounidas G, Martin KR, Werth M, Cooper K, Myint PK (2022) Determinants of healthy ageing: a systematic review of contemporary literature. Aging Clin Exp Res 34(6):1215–1223. https://doi.org/10.1007/s40520-021-02049-w
Adler-Milstein J (2021) From digitization to digital transformation: policy priorities for closing the gap. JAMA 325(8):717–718. https://doi.org/10.1001/jama.2020.27014
Amosun S, Harris F (2020) What next now that you are sixty?”–Preliminary exploration of the self-reported aspirations of community-dwelling older persons in the Western Cape Province, South Africa within the active aging framework. Physiother Theory Pract 36(7):791–798. https://doi.org/10.1080/09593985.2018.1508262
Barnett P, Goulding L, Casetta C, Jordan H, Sheridan-Rains L, Steare T, Williams J, Wood L, Gaughran F, Johnson S (2021) Implementation of telemental health services before COVID-19: Rapid umbrella review of systematic reviews. J Med Internet Res 23(7):e26492. https://doi.org/10.2196/26492
Beard JR, Officer A, De Carvalho IA, Sadana R, Pot AM, Michel JP, Lloyd-Sherlock P, Epping-Jordan JE, Peeters GMEE, Mahanani WR, Thiyagarajan JA, Chatterji S (2016) The world report on ageing and health: a policy framework for healthy ageing. Lancet 387(10033):2145–2154. https://doi.org/10.1016/S0140-6736(15)00516-4
Blazun H, Saranto K, Rissanen S (2012) Impact of computer training courses of reduction of loneliness of elder people in Finland and Slovenia. Comput Hum Behav 28(4):1202–1212. https://doi.org/10.1016/j.chb.2012.02.004
Caballero FF, Soulis G, Engchuan W et al. (2017) Advanced analytical methodologies for measuring healthy ageing and its determinants, using factor analysis and machine learning techniques: the ATHLOS project. Sci Rep-UK 7:43955. https://doi.org/10.1038/srep43955
Cao X, Ji S (2024) Bidirectional relationship between self-rated health and the big five personality traits among Chinese adolescents: A two-wave cross-lagged study. Hum Soc Sci Commun 11:200. https://doi.org/10.1057/s41599-024-02699-x
Chen CR, Ding SC, Wang J (2023) Digital health for aging populations. Nat Med 29(7):1623–1630. https://doi.org/10.1038/s41591-023-02391-8
Chen K, de Schrijver E, Sivaraj S et al. (2024) Impact of population aging on future temperature-related mortality at different global warming levels. Nat Commun 15(1):1796. https://doi.org/10.1038/s41467-024-45901-z
Chen L, Ye MZ, Kahana E (2020) A self-reliant umbrella: Defining successful aging among the old-old (80+) in Shanghai. J Appl Gerontol 39:242–249. https://doi.org/10.1177/0733464819842500
Chen PJ, Li FZ, Harmer P (2019) Healthy China 2030: moving from blueprint to action with a new focus on public health. Lancet Public Health 4(9):E447–E447. https://doi.org/10.1016/S2468-2667(19)30160-4
Chen SM, Li LY, Jiao LR, Wang C (2023) Long-term care insurance and the future of healthy aging in China. Nat Aging 3(12):1465–1468. https://doi.org/10.1038/s43587-023-00540-9
Cheng Y, Chen ZL, Wei Y, Gu N, Tang SL (2024) Examining dynamic developmental trends: the interrelationship between age-friendly environments and healthy aging in the Chinese population: Evidence from China Health and Retirement Longitudinal Study, 2011–2018. BMC Geriatr 24(1):429. https://doi.org/10.1186/s12877-024-05053-7
Choi NG, DiNitto DM (2013) The Digital divide among low-income homebound older adults: internet use patterns, eHealth literacy, and attitudes toward Computer/Internet use. J Med Internet Res 15(5):e93. https://doi.org/10.2196/jmir.2645
Choukou MA, Sanchez-Ramirz DC, Pol M, Uddin M, Monnin C, Syed-Abdul S (2022) COVID-19 infodemic and digital health literacy in vulnerable populations: A scoping review. Digit Health 8:1–13. https://doi.org/10.1177/20552076221076927
Chu, Nyrup CH, Leslie R, Shi K, Bianchi JM, Lyn A, McNicholl A, Khan M, Rahimi S, GrenierA S, Meeks S (2022) Digital ageism: Challenges and opportunities in artificial intelligence for older adults. Gerontologist 62(7):947–955. https://doi.org/10.1093/geront/gnab167
Cilli E, Ranieri J, Guerra F et al. (2023) Digital affinity and cognitive reserve: Salience for resilient aging in pandemic. Gerontol Geriatric Med 9:233372142311627. https://doi.org/10.1177/23337214231162773
Crawford A, Serhal E (2020) Digital health equity and COVID-19: the innovation curve cannot reinforce the social gradient of health. J Med Internet Res 22(6):e19361. https://doi.org/10.2196/19361
Critselis E, Panaretos D, Sánchez-Niubò A, Giné-Vázquez I, Ayuso-Mateos JL, Caballero FF, de la Fuente J, Haro JM, Panagiotakos D (2020) Ageing trajectories of health-longitudinal opportunities and synergies (ATHLOS) Healthy Ageing Scale in adults from 16 international cohorts representing 38 countries worldwide. J Epidemiol Commun H 74(12):1043–1049. https://doi.org/10.1136/jech-2020-214496
Cui YP, He YS, Xu XL, Zhou LL, Nutakor JA, Zhao LQ (2024) Cultural capital, the digital divide, and the health of older adults: a moderated mediation effect test. BMC Public Health 24(1):302. https://doi.org/10.1080/10400435.2025.246257410.1186/s12889-024-17831-4
Danesin L, Pucci V, Vidoret A, Mondini S, Arcara G, Montemurro S, Burgio F (2025) Promoting healthy aging using new digital solutions in Italy: A scoping review. Assist Technol 37(5):332–357. https://doi.org/10.1080/10400435.2025.2462574
De Haan J (2004) A multifaceted dynamic model of the digital divide. It & Society 1(7):66–88
Fang EF, Scheibye-Knudsen M, Jahn HJ, Li J, Ling L, Guo HW, Zhu XQ, Preedy V, Lu HM, Bohr VA, Chan WY, Liu YL, Ng TB (2015) A research agenda for aging in China in the 21st century. Ageing Res Rev 24:197–205. https://doi.org/10.1016/j.arr.2015.08.003
Ferguson CJ (2009) An effect size primer: A guide for clinicians and researchers. Prof Psychol-Res Pr 40(5):532–538. https://doi.org/10.1037/a0015808
Gariboldi MI, Chen M, Wei Y, Xu S, Galea G, Lee SW (2023) Towards digital healthy ageing: The case of Agatha and priorities moving forward. Lancet Reg Health-W 35:100649. https://doi.org/10.1016/j.lanwpc.2022.100649
Ge H, Li JS, Hu HL, Feng TT, Wu X (2025) Digital exclusion in older adults: A scoping review. Int J Nurs Stud 168:105082. https://doi.org/10.1016/j.ijnurstu.2025.105082
Halpern D (2005) Social capital. Cambridge: Polity
Hamaker EL (2023) The Within-Between Dispute in Cross-Lagged Panel Research and How to Move Forward. Psychol Methods. https://doi.org/10.1037/met0000600
Hess TM, Freund AM, Tobler PN (2021) Effort mobilization and healthy aging. J Gerontol B-Psychol 76(Supplement2):S135–S144. https://doi.org/10.1093/geronb/gbab030
Hu L, Bentler PM (1999) Cutoff criteria for fit indexes in covariance structure analysis: conventional criteria versus new alternatives. Struct Equat Model 6(1):1–55. https://doi.org/10.1080/10705519909540118
Hu YN, Yang YK, Gao Y, Zhao LY, Chen L, Sui WZ, Hu JQ (2024) The impact of chronic diseases on the health-related quality of life of middle-aged and older adults: The role of physical activity and degree of digitization. BMC Public Health 24(1):2335. https://doi.org/10.1186/s12889-024-19833-8
Jaworski BK, Hooper MW (2023) Advancing digital health Equity: Directions for behavioral and social science research. Transl Behav Med 13(3):132–139. https://doi.org/10.1093/tbm/ibac088
Lee C, Coughlin JF (2015) PERSPECTIVE: Older Adults’ adoption of Technology: An integrated approach to identifying determinants and barriers. J Prod Innovat Manag 32(5):747–759. https://doi.org/10.1111/jpim.12176
Li HM, Zeng YX, Gan L, Tuersun Y, Yang J, Liu J, Chen JY (2022) Urban‑rural disparities in the healthy ageing trajectory in China: a population‑based study. BMC Public Health 22(1):1406. https://doi.org/10.1186/s12889-022-13757-x
Li ZB, Liu HJ (2025) Bidirectional association between internet use and depressive symptoms among middle‐aged and older adults in China: A cross-lagged model of proactive health behavior as the mediating role. Depress Anxiety 2025(1). https://doi.org/10.1155/da/9391682
Lu WT, Pikhart H, Sacker A (2021) Comparing socio-economic inequalities in healthy ageing in the United States of America, England, China and Japan: Evidence from four longitudinal studies of ageing. Ageing Soc 41(7):1495–1520. https://doi.org/10.1017/S0144686X19001740
Lu XR, Yao Y, Jin YZ (2022) Digital exclusion and functional dependence in older people: Findings from five longitudinal cohort studies. EClinicalMedicine 54:101708. https://doi.org/10.1016/j.eclinm.2022.101708
Lucas HM, Lozano CJ, Valdez LP, Manzarate R, Lumawag FAJ (2018) A grounded theory of successful aging among select incarcerated older Filipino women. Arch Gerontol Geriatr 77:96–102. https://doi.org/10.1016/j.archger.2018.04.010
Luo YA, Su BB, Zheng XY (2021) Trends and challenges for population and health during population aging - China, 2015-2050. China CDC Weekly 3(28):593–598. https://doi.org/10.46234/ccdcw2021.158
Lythreatis S, Singh SK, El-Kassar AN (2022) The digital divide: A review and future research agenda. Technol Forecast Soc 175:121359. https://doi.org/10.1016/j.techfore.2021.121359
Marcus BH, Ciccolo JT, Sciamanna CN (2009) Using electronic/computer interventions to promote physical activity. Brit J Sport Med 43(2):102–105. https://doi.org/10.1136/bjsm.2008.053744
Merchant RA, Tsoi CT, Tan WM, Lau W, Sandrasageran S, Arai H (2021) Community-Based Peer-Led intervention for healthy ageing and evaluation of the ‘HAPPY’ program. J Nutr Health Aging 25(4):520–527. https://doi.org/10.1007/s12603-021-1606-6
Michel JP, Sadana R (2017) Healthy aging” concepts and measures. J Am Med Dir Assoc 18(6):460–464. https://doi.org/10.1016/j.jamda.2017.03.008
Nahapiet J, Ghoshal S (1998) Social capital, intellectual capital, and the organizational advantage. Acad Manag Rev 23:242–266. https://doi.org/10.5465/amr.1998.533225
Nguyen H, Wu YT, Dregan A, Vitoratou S, Chua KC, Prina AM (2020) Multimorbidity patterns, all-cause mortality and healthy aging in older English adults: Results from the English Longitudinal Study of Aging. Geriatr Gerontol Int 20(12):1126–1132. https://doi.org/10.1111/ggi.14051
Ordonez TN, Yassuda MS, Cachioni M (2011) Elderly online: Effects of a digital inclusion program in cognitive performance. Arch Gerontol Geriatr 53(2):216–219. https://doi.org/10.1016/j.archger.2010.11.007
Peng XZ (2011) China’s demographic history and future challenges. Science 333(6042):581–587. https://doi.org/10.1126/science.1209396
Pérez-Amaral T, Valarezo A, López R, Garín-Muñoz T (2021) Digital divides across consumers of internet services in Spain using panel data 2007–2019. Narrowing or not? Telecommun Policy 45(2):102093. https://doi.org/10.1016/j.telpol.2020.102093
Ploughman M, Austin MW, Murdoch M, Kearney A, Fisk JD, Godwin M, Stefanelli M (2012) Factors influencing healthy aging with multiple sclerosis: a qualitative study. Disabil Rehabil 34(1):26–33. https://doi.org/10.3109/09638288.2011.585212
Podsakoff PM, Mackenzie SB, Lee JY, Podsakoff NP (2003) Common method biases in behavioral research: A critical review of the literature and recommended remedies. J Appl Psychol 88(5):879–903. https://doi.org/10.1037/0021-9010.88.5.879
Ragnedda M, Ruiu ML, Addeo F (2022) The self-reinforcing effect of digital and social exclusion: The inequality loop. Telemat Inform 72:101852. https://doi.org/10.1016/j.tele.2022.101852
Rudnicka E, Napierała P, Podfigurna A, Meczekalski B, Smolarczyk R, Grymowicz M (2020) The World Health Organization (WHO) approach to healthy ageing. Maturitas 139:6–11. https://doi.org/10.1016/j.maturitas.2020.05.018
Sanchez-Niubo A, Forero CG, Wu YT et al. (2021) Development of a common scale for measuring healthy ageing across the world: results from the ATHLOS consortium. Int J Epidemiol 50(3):880–892. https://doi.org/10.1093/ije/dyaa236
Santini S, Galassi F, Kropf J, Stara V (2020) A digital coach promoting healthy aging among older adults in transition to retirement: Results from a qualitative study in Italy. Sustainability-Basel 12(18):7400. https://doi.org/10.3390/su12187400
Seifert A, Cotten SR, Xie B (2021) A double burden of exclusion? Digital and social exclusion of older adults in times of COVID-19. J Gerontol B-Psychol 76(3):E99–E103. https://doi.org/10.1093/geronb/gbaa098
Stepaniak U, Grosso G, Polak M, Gradowicz-Prajsnar B, Kozela M, Bobak M, Sanchez-Niubo A, Stefler D, Haro JM, Pajak A (2025) Association between dietary (poly) phenol intake and the ATHLOS Healthy Ageing Scale in the Polish arm of the HAPIEE study. Geroscience. 47:3241–3253 https://doi.org/10.1007/s11357-024-01275-0
The United Nations (2022) World Population Prospects 2022. The United Nations, New York
Wang HL, Yu YW (2016) Increasing health inequality in China: An empirical study with ordinal data. J Econ Inequal 14(1):41–61. https://doi.org/10.1007/s10888-015-9315-1
Wang HM (2024) Blue Book on the Development of Healthy Ageing in China (2023–2024). Peking University, Beijing
Wang JF, Cui QM, Xu X, Yang G (2025) Bidirectional association between grip strength and cognitive function in Chinese older adults: a nationwide cohort study. BMC Public Health 25(1). https://doi.org/10.1186/s12889-025-23079-3
Wang YG, Wu ZG, Duan LZ, Liu SJ, Chen RZ, Sun T, Wang J, Zhou JH, Wang HX, Huang P (2024) Digital exclusion and cognitive impairment in older people: Findings from five longitudinal studies. BMC Geriatr 24(1):406. https://doi.org/10.1186/s12877-024-05026-w
Wong YC, Chen HL, Lee V et al. (2014) Empowerment of senior citizens via the learning of information and communication technology. Ageing International 39(2):144–162. https://doi.org/10.1007/s12126-013-9185-4
World Health Organization (2002) Active ageing: a policy framework. World Health Organization, Geneva
World Health Organization (2015) World report on ageing and health. World Health Organization, Geneva
World Health Organization (2021) Global report on ageism. World Health Organization Demographic Change and Healthy Ageing, Geneva
World Health Organization. Constitution of the World Health (online). Available at: https://www.who.int/about/who-we-are/constitution. Accessed February 14, 2021
Wu YT, Daskalopoulou C, Terrera GM et al. (2020) Education and wealth inequalities in healthy ageing in eight harmonised cohorts in the ATHLOS consortium: a population-based study. Lancet Public Health 5(7):E386–E394. https://doi.org/10.1016/s2468-2667(20)30077-3
Wu ZG, Zhou JY, Feng XJ et al. (1997) Dictionary of Population Science. Southwestern University of Finance and Economics Press
Yang H, Chen HT, Pan TS, Lin YR, Zhang Y, Chen HL (2022) Studies on the digital inclusion among older adults and the quality of life-A Nanjing example in China. Front Public Health 10:811959. https://doi.org/10.3389/fpubh.2022.811959
Yu Y (2021) Healthy ageing in urban China: Governing the ageing population. Geogr J 187(1):28–38. https://doi.org/10.1111/geoj.12372
Zhang JJ, Jia XQ, Li YY, Li HB, Yang Q (2023) The longitudinal bidirectional association between sarcopenia and cognitive function in community-dwelling older adults: Findings from the China Health and Retirement Longitudinal Study. J Glob Health 13:04182. https://doi.org/10.7189/jogh.13.04182
Zhao IY, Ho MH, Tyrovolas S, Deng SY, Montayre J, Molassiotis A (2023) Constructing the concept of healthy ageing and examining its association with loneliness in older adults. BMC Geriatr 23(1):325. https://doi.org/10.1186/s12877-023-04019-5
Zhao LY, Zhang K, Gao Y, Jia ZH, Han SY (2022) The relationship between gender, marital status and depression among Chinese middle-aged and older people: Mediation by subjective well-being and moderation by degree of digitization. Front Psychol 13:923597. https://doi.org/10.3389/fpsyg.2022.923597
Zhao YH, Hu YS, Smith JP, Strauss J, Yang GH (2014) Cohort Profile: The China Health and Retirement Longitudinal Study (CHARLS). Int J Epidemiol 43(1):61–68. https://doi.org/10.1093/ije/dys203
Zhou JH, Ye XX (2023) Aging population and digital inclusive finance, a natural experiment from China. Plos One 18(11):e0287292. https://doi.org/10.1371/journal.pone.0287292
Acknowledgement
This work was supported by the National Natural Science Foundation of China under grants 72474022, 72574023, 71974011 and 72174022, “BIT think tank” Promotion Plan of Science and Technology Innovation Program of Beijing Institute of Technology under grants 2024CX14017 and 2025CX13015, and Beijing Social Science Foundation under grant 25JCC131.
Author information
Authors and Affiliations
Contributions
TA, TY, WH, and JW were involved in conception, data analysis, and paper drafting. JN and ZT helped with data collection and substantial revisions. All authors reviewed the manuscript.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethical approval
This study utilizes open secondary data obtained from the China Health and Retirement Longitudinal Survey (CHARLS). CHARLS received approval from the Biomedical Ethics Committee of Peking University in 2011 in accordance with the Declaration of Helsinki (approval number: IRB00001052-11015). In alignment with our institutional policy, this research does not require separate ethical approval.
Informed consent
The secondary data used originates from CHARLS. All CHARLS participants provided signed informed consent during the initial data collection phase prior to their involvement in the survey.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Yang, T., Wang, T., Deng, W. et al. Bidirectional relationship between digital inclusion and healthy ageing among Chinese older adults: a four-wave cross-lagged study. Humanit Soc Sci Commun 13, 311 (2026). https://doi.org/10.1057/s41599-025-06486-0
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1057/s41599-025-06486-0
