
Abstract
This meta-analysis identified forty-eight unique samples (total number of participants =10,324) which reported rates of smartphone ownership (SO), current, and daily internet usership (IU) among adults with psychiatric disorders between 2004 and 2023. SO increased from 32% in 2012–2013 to 77% in 2020–2021; current IU rose from 65% in 2010–2011 to 87% in 2018–2019; daily IU grew from 30% in 2010–2011 to 58% in 2016–2017. Compared to US national data, the gap has narrowed by 8.9% for SO since 2012 and 10% for current IU since 2010. Individuals who are older, male, less educated, unemployed, and with psychosis diagnosis were at-risk of various digital disengagement. At the macro-level, regional income inequality was also associated with IU. Although the usage and device gaps have been substantially narrowed, continued monitoring is needed to ensure sustained improvements. The highly heterogeneous studies highlighted the need of establishing standardized outcome metrics to enhance cross-study comparability.
Similar content being viewed by others


Introduction
Digital technologies have become a fundamental part of our daily lives. In 2022, internet users constituted around 95.3–97.1% of the national population in the US, UK, and Hong Kong1. The COVID-19 pandemic further underscored the benefits of digital technologies, as restrictions on physical interactions highlighted their potential to enable broad access to services with reduced cost2. Since then, the digitalisation in various aspects of societal function has been a major focus of governments. While digital technologies are frequently promoted as a solution for reducing inequalities3,4, their accessibility and usability remain shaped by entrenched structural and individual barriers5. Disadvantaged populations, particularly patients with psychiatric illnesses, may be disproportionately excluded as they fall behind in digital participation and face a new form of social inequality. The digital divide refers to the disparity in digital access, usage, and outcomes6, which has direct and indirect detrimental impacts on patients with psychiatric illness. Direct impacts relate to the inaccessibility of digital health technologies (DHTs). DHTs aim to provide both physical and mental health care at reduced cost and with wider coverage, attracting significant interest from various national health services7. However, over-emphasis on developing DHTs may neglect the needs of the digitally disengaged population. Indirect impacts pertain to digitalising essential services, such as housing or employment opportunities7, which risk further marginalising digitally disengaged patients.
The digital divide among the psychiatric population can be examined on two levels: the access and the usage gap. The access gap refers to the ‘have’ or ‘have-not’ internet access6. In recent years, due to high internet penetration rate in developed regions, the focus has shifted to the device gap8, which relates to the device they use to access the Internet. Particularly, smartphones have a lower financial cost compared to personal computers, serving as a viable entry point for populations with limited resources9. The usage gap, on the other hand, explores how and why individuals with access use the internet, and focus on the disparities in usage patterns, digital skills, confidence, and acceptance6,8. As digital technologies evolve, becoming more affordable and increasingly user friendly, it can be anticipated that the existing gaps will continue to narrow. However, ongoing monitoring remains crucial to assess the pace and sustainability of this progress. Moreover, what constitutes meaningful participation is likely to shift over time. Beyond measuring general internet use, examining usage patterns, such as frequency and types of online activities, could provide deeper insights into how psychiatric populations adapt to societal digitalisation10. Previous research on internet use (IU) and smartphone ownership (SO) has produced varying results and conflicting conclusions regarding the existence of gaps between psychiatric and general populations11,12, warranting a review to consolidate these findings. Additionally, a static snapshot of IU and SO may not fully capture the evolving nature of the divide. Examining longitudinal changes can reveal whether improvements have been consistent or whether periods of stagnation or regression have occurred. These insights are crucial for informing policy decisions and guiding interventions.
To the best of our knowledge, no prior review has examined the IU gap among psychiatric populations, and only one meta-analysis was conducted in 2016 which focused on mobile phone ownership among individuals with psychosis. The study reported a significantly narrowed gap in mobile phone ownership between patients and the general population13. However, since 2016, technological advancements have been substantial. Smartphones have largely replaced traditional mobile phones and become the predominant mobile device. Merely owning a mobile phone may no longer be sufficient for patients to remain digitally connected within society. For instance, communication has largely transitioned from traditional text messages to social media platforms, and many DHTs now incorporate sophisticated functions that operate exclusively on smartphones. Moreover, the previous meta-analysis modelled temporal trends linearly. This approach may not account for variations in the pace of technological progress during different periods. Thus, an updated and more comprehensive meta-analysis on smartphone ownership (SO) is warranted.
Furthermore, contemporary models theorise that the digital divide is shaped by deeply rooted structural inequalities and individual-level vulnerabilities. According to Van Dijk’s Resources and Appropriation theory, personal categories (e.g., age, gender, health/ability, etc.) and positional categories (e.g., education, household, nation) determine individuals’ temporal, material, mental, social and cultural resources, which in turn influence their access and use of digital technologies5. Apart from socio-demographic and socio-economic determinants of the divide that have been examined extensively in non-psychiatric populations8, illness chronicity and severity have been identified as illness specific barriers in psychiatric populations in previous studies13. Particularly, patients with psychosis have been highlighted to have lower levels of digital engagement compared to other severe mental illnesses14. Beyond individual barriers, the digital divide, understood as a dimension of social inequality, is closely interlinked with other systematic inequities. Macro-level determinants including regional disparities in information communication technology (ICT) infrastructures, social policy environments, as well as regional income inequality interact with the micro-level factors (individual and illness-related barriers)15. Indeed, prior research has indicated that higher regional income inequality significantly predicted lower internet usage16. Psychiatric populations, who are often socio-economically disadvantaged, may be disproportionately impacted by these systematic inequalities, and their intersecting vulnerabilities can further entrench their position on the disadvantaged side of the digital divide5. Addressing both societal and individual factors could better inform social policies directions and development of targeted interventions to further reduce the digital divide.
This is the first meta-analysis to investigate internet use and smartphone ownership in the psychiatric population. This review first examined the trend of SO, current and daily IU rates over the years among psychiatric populations. Then, potential factors relating to SO, current and daily IU were explored. Lastly, the device and digital usage gap between the psychiatric and general populations was investigated by comparison with national data. By addressing these areas, we hope to contribute to the broader discourse of the digital divide and support the efforts to reduce and improve equity in societies.
Results
The database search identified 2307 results, of which 48 studies were found to be eligible for this review, yielding a total sample size of 10, 324 (Fig. 1).

n = number of studies. Included and excluded studies extracted from PubMed, Medline, PsycInfo, Scopus, Web of Science on smartphone ownership and internet use among psychiatric populations, with reasons for exclusion.
The mean age was 41.9 (median = 44, range = 27.7-69.5) (k = 45), 53.7% of the sample were identified as male (k = 47), 61.2% achieved education equivalent to or above high school (k = 32), 34.6% were engaged in open employment or had student status (k = 26), and 38.8% had a diagnosis of psychosis (k = 46). The studies were conducted across 17 countries/regions, 19 (39.6%) studies were from World Health Organisation (WHO Region of the Americas, 19 (39.6%) studies were from the WHO European Region, 6 (12.5%) studies were from the WHO Western Pacific Region, 1 (2.1%) was in the WHO African Region, and 1 (2.1%) was across multiple regions. Thirty-one studies (64.6%; n = 7045) reported the rate of current IU while 21 (43.8%; n = 3990) reported daily IU rates from 2004 to 2021, 27 (56.3%) studies (n = 5431) reported the rate of SO from 2012 to 2023 (Table 1).
Longitudinal patterns of smartphone ownership and internet use
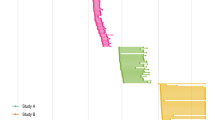
The pooled rate of current IU increased from 65% (95% CI = 52–76%) in 2010–2011 to 87% (95% CI = 72–94%) in 2018–2019 (Fig. 2a), daily IU rose from 30% (95% CI = 26–35%) in 2010–2011 to 58% (95% CI = 41–72%) in 2016–2017 (Fig. 2b). Additionally, SO increased from 32% (95% CI = 14–58%) in 2012–2013 to 77% (95% CI = 50–92%) in 2020–2021 (Fig. 2c). Significant bi-yearly sub-group differences were observed for all three outcomes (p < 0.001), with high heterogeneity (I2 = 95.5–96.3%; τ 2 = 0.67–1.34). From 2010 to 2019, there was a marked increase in current IU within the psychiatric population, nearly catching up the general population. However, a possible drop was observed after 2018–2019 in the psychiatric population only while the US general population continued to increase. A similar trend was also observed for daily IU, though the rate remained much lower than that of the current IU (Fig. 3a). An accelerated growth in SO was noted in the psychiatric population, with the SO rate becoming comparable to the general US population by 2024. Nevertheless, since 2020, the rate of SO within the psychiatric populations may have experienced a slight drop and plateaued, while the general US population continued to see a steady increase (Fig. 3b). The leave-one-out sensitivity analysis did not reveal any samples that were influential to the pooled rates (Supplementary Figs. 1 & 2). By excluding studies with low quality, the sensitivity analysis revealed that the estimated rates were minimally affected (Supplementary Figs. 3 & 4). Funnel Plots and Egger’s regression test detected no publication bias except for the rate of SO in 2016-2017 (Supplementary Figs. 5 & 6).

a Forest plot of pooled estimates of current internet user rates. Red squares indicate rates from individual studies, while black diamonds represent the pooled estimates for each period and the overall analysis. b Forest plot of pooled estimates of daily internet user rates. Red squares indicate rates from individual studies, while black diamonds represent the pooled estimates for each period and the overall analysis. c Forest plot of pooled estimates of smartphone ownership rates. Red squares show the rates from individual studies, and black diamonds depict the pooled estimates for each period and the overall analysis.

a Internet user rate across 2004–2021. Each bubble represents the internet user rate of an individual study, with point size proportional to sample size. Red points represent the World Health Organisation (WHO) African Region, green the European Region, blue the Region of the Americas, purple the Western Pacific Region, and grey an undefined region. The grey line shows the internet user trend of the general United States population (International Telecommunication Union1 data, adapted by authors), while the pink and orange lines represent the pooled daily and current internet user trends of the psychiatric sample, respectively. b Smartphone ownership rate across 2012–2023. Each bubble represents the smartphone ownership rate of an individual study, with point size proportional to sample size. Red points represent the WHO African Region, green the European Region, blue the Region of the Americas, purple the Western Pacific Region, and grey an undefined region. The grey line shows the trend of the general United States population (International Telecommunication Union1 data, adapted by authors). The orange line represents the trend of the psychiatric sample.
The exploratory meta-regression on the pandemic effect on digital engagement showed no significant association between the COVID-19 pandemic and current or daily IU, but a significant negative association were observed with SO (Estimate = −2.13, SE = 0.92, p < 0.01; Supplementary Table 2), though there were only two studies from 2020 onwards for current and daily IU and six for SO. Additionally, the sensitivity analysis conducted by excluding 2020-2021 studies revealed that the pooled SO rate decreased slightly from 70% (95% CI = 60% – 78%) to 68% (95% CI = 57–77%) (Supplementary Fig. 7), indicating that the observed decline may not entirely driven by the studies in the COVID-19 period. However, due to the limited studies after 2020 for current and daily IU, this sensitivity analysis was not performed on these outcomes. Table 1
Predictors of digital engagement
For socio-demographic predictors, being male was significantly associated with lower rates of current, daily IU and SO. Older age was significantly associated with lower current IU and SO but not daily IU. Conversely, attaining a high school education was significantly associated with higher rates of current, daily IU and SO. Employment status was significantly associated with lower rates of current and daily IU but higher SO (Table 2). Risk of multicollinearity was insignificant for these predictors (VIF < 2). The multivariate regression model revealed that only attainment of high school education was significantly associated with higher rate of SO, current and daily IU. In addition, being male was also associated with higher daily IU. However, the models had small sample sizes (k = 15–22), and particularly the SO (τ² = 2.40) and daily IU models (τ² = 2.71) exhibited high heterogeneity (Supplementary Table 3).
For clinical predictors, having psychosis was significantly associated with lower current, daily IU and SO. For structural predictors, residing in a region with a higher Gini Index was significantly associated with a lower rate of current and daily IU but only a trend toward significance with higher rate of SO (p = 0.063; Table 2). The regional differences were also examined. The meta-regression revealed that WHO European regions had significantly lower SO rate than WHO Region of Americas (Supplementary Table 4). Subgroup analyses further supported this finding, showing a significant regional difference in SO (Supplementary Fig. 11). However, no significant differences were observed between regions for current and daily IU in either the meta-regression (Supplementary Table 4) or subgroup analyses (Supplementary Figs. 12 & 13).
Discussion
This is the first proportional meta-analysis of current and daily internet use (IU) and smartphone ownership (SO) among psychiatric populations from 2004 to 2023, including 48 unique samples with a total of 10,324 psychiatric populations across 17 regions. Current IU in psychiatric populations increased from 60% in 2010–2011 to 87% in 2018–2019, while SO rose from 32% in 2012–2013 to 77% in 2020–2021. Using US national data as a benchmark, psychiatric populations had nearly caught up with the general population in terms of current IU and SO by 2019. A possible decline was observed during 2020–2023, though additional data were required to confirm this finding. The findings also revealed older, male, less educated individuals and patients with psychosis were at-risk subpopulations of digital disengagement. Being employed were less likely to use the internet but more likely to be smartphone owners. Residing in regions with higher Gini Index were less likely to use the internet.
The digital divide between psychiatric and general populations has narrowed substantially over the years. Current IU rates (87%) peaked in 2018–2019, while SO (79%) peaked in 2016–2017. The increased affordability of technology and the rise in popularity of smartphones may have contributed to this trend. For instance, the affordability of fixed broadband improved with a 2.7% drop in Gross National Income per capita price worldwide and a 4.5% drop in the US alone from 2008 to 201717. Notably, the Canadian smartphone price index showed a remarkable 56.7% drop in prices from 2015 to 202118. These comparable SO rates of the psychiatric and general population support previous research suggesting that smartphones are a viable entry point to close the device and usage gap for disadvantaged populations9. However, our meta-analyses suggested that the rate of daily IU appeared drastically lower than the rate of current IU, with nearly one-third of the current IU were not engaging daily. Although the number of studies assessing daily IU at each bi-yearly subgroup were limited, this preliminary finding points to potential barriers beyond accessibility and affordability, such as a lack of skills and interest19. Thus, the psychiatric populations may remain vulnerable to the usage gap. Therefore, simply categorising individuals into internet users and non-users may not effectively assess the digital divide. This highlights the need to constantly refine metrics of digital participation to better reflect meaningful engagement in the everchanging digital landscape.
Additionally, although more studies are needed to verify the findings, our meta-analyses suggested a potential decline in daily and current IU and SO after 2019, despite continued growth in the general population. A possible explanation is the impacts of COVID-19. Pandemic restrictions, such as lockdowns and social distancing measures, may have reduced access to some of the key resources of digital access for the psychiatric population, including public facilities offering free Internet20, and to social networks that provide internet and device support. Our exploratory analysis partially supported this explanation, as the pandemic dummy variable was associated with lower SO rate, though the significance was not observed in current and daily IU, possibly due to the limited number of post-2020 studies for these outcomes. Sensitivity analysis excluding 2020-2021 studies yield a slightly dropped pooled estimate for SO. The pandemic restrictions may have isolated individuals with limited digital skills from support needed to maintain digital engagement. A study in the UK during the pandemic found that patients with severe mental illness (SMI) reported lower internet knowledge compared to the general public 14.These results suggested the vulnerability of the psychiatric population to fall back into poorer digital access and usage during sudden societal changes, warranting further monitoring of the divide and underscores the need for enhanced support to improve digital adaptability and independence among the vulnerable population.
The current study also identified several individual, clinical, and macro-level socioeconomic factors associated with current, daily IU and SO. Consistent with findings from non-psychiatric populations, older adults and individuals with lower educational levels were less likely to use the internet or own smartphones21,22. Conversely, digital disengagement was more common among men. One possible reason may be the lower perceived social benefits of digital technology. Previous research has shown that men with psychiatric disorders are less likely to seek help23, which may reduce their motivation to engage digitally. Being employed was significantly associated with higher smartphone ownership but lower likelihood of current and daily internet use, highlighting unique challenges faced by the psychiatric population. This paradox may suggest that, although employed individuals could afford smartphones, many may work in blue-collar occupations, requiring them to work long hours in physically demanding tasks24, leaving limited opportunities or motivations to develop digital skills. Hence, smartphone ownership does not necessarily translate to active digital engagement. Future research on the relationships between the types of occupation and SO and IU are needed. When accounting for multiple socio-demographic variables simultaneously, only educational level remained a significant predictor for current IU and SO, while higher educational level and being male were associated with higher daily IU. However, given the small number of studies with complete sociodemographic data and high residual heterogeneity, the models were underpowered, and no firm conclusions should be drawn. Future studies with more comprehensive assessments of socio-demographic factors and their relationship with digital engagement are needed to clarify these associations.
Clinically, having psychosis was negatively associated with SO, current and daily IU. This corroborated with previous evidence that patients with psychosis had poorer digital skills19. Impaired cognitive functioning and negative symptoms, such as amotivation and asociality, may impaired their ability to develop digital skills and reduce their interest in social interaction and help-seeking behaviors25, leading to digital disengagement, even in the most basic forms. Notably, the lowest rate of current IU was reported in community rehabilitation placement users with long-term psychosis26, who were likely to represent those with more severe and chronic forms of illness among psychiatric populations. Thus, while telehealth and digital interventions are promising avenues for mental healthcare delivery, they may not reach the subgroups most in need without tailored strategies to address cognitive and motivational barriers, warranting reconsideration in the role of DHTs in the overall healthcare model.
On a macro-level, income inequality was significantly associated with current and daily internet use but not smartphone ownership. Regions with a higher Gini Index, exhibited less IU, suggesting that in areas with greater income inequality, internet access may be perceived as a privatized asset, discouraging use among disadvantaged individuals. For example, as of 2024, the US, a region with relatively high Gini Index, continues to struggle to provide affordable internet connectivity to disadvantaged populations27. In contrast, regions with a lower Gini Index, such as those in Europe, have made efforts to provide reliable and free public internet access28, which may encourage IU without necessarily increasing SO or private internet subscriptions. This may partly explain the regional differences identified where SO was lower in the European regions compared to the Americas. These results highlighted the impacts of government social policies on the digital divide and reinforced “Internet for all” as a viable solution to mitigate the usage gap. However, policymakers should also consider ongoing technological advancements that may potentially raise the threshold of meaningful digital participation, necessitating individuals to own personal devices with constant internet access to remain socially and economically relevant. Furthermore, while the Gini Index reflects overall income inequality, it does not capture the specific distribution between wealthy and low-income populations. This limitation may partly explain why significant associations were observed for IU but not SO, as SO may depend more strongly on the proportion of disadvantaged individuals lacking resources rather than generalized inequality measures. Future research may consider examining regional income distribution and individuals’ socio-economic status to provide better predictors of smartphone ownership.
One limitation of this study is the sample size. Although the overall sample size was relatively large, not all analyses had sufficient studies to achieve statistical power. For the bi-yearly subgroup analyses, there were three subgroups with less than three studies for current and daily IU, and two subgroups for SO. Therefore, caution in interpretation is warranted for these subgroup analyses. Moreover, only about half of the psychiatric patients reported daily IU, it was the least frequently measured across studies and was not assessed consistently across all time periods. Future research on digital inclusion among both general and disadvantaged populations should include daily IU as a standardized metric to enable more accurate and meaningful assessments of the usage gap in the evolving digital landscape. Furthermore, due to insufficient reporting across included studies, only multivariate meta-regressions on socio-demographic factors were conducted exploratively. The interaction between individual socio-demographic, illness-related, and macro-level socioeconomic factors was not explored. Additionally, only a very small number of studies were available post-2020 (2 studies for current and daily IU, and 6 studies for SO), making the exploratory analyses of the pandemic effects and post-pandemic trends underpowered. Findings related to potential post-COVID declines should be interpreted with caution until more post-pandemic data become available and future studies should continue to monitor the digital engagement trends to identify any possible widening of the divide.
Secondly, the included studies suffered from high methodological heterogeneity, particularly in operational definitions and timeframes used to assess “current” internet users. Measurement periods varied widely, ranging from weekly to yearly intervals, and some studies categorised users without clearly specifying the reference period. Such inconsistencies in strictness of criteria may make the outcomes vulnerable to inflation or underestimation, thereby obscuring true temporal trends. This lack of standardization underscores a broader concern regarding the constituents of a meaningful timeframe for assessing digital participation. Establishing consensus on internet usage is critical for ensuring comparability of findings across studies which warrants further investigation.
Thirdly, the regional distribution of studies was highly uneven, with only three conducted in Asia, one in Africa, and none in Southeast Asia. Although subgroup analyses were performed to explore regional effects and account for outcome heterogeneity, the limited representation of several regions resulted in underpowered analyses. This imbalance restricted the generalisability of the findings and highlighted the need for more geographically diverse research. Notably, this review utilized national data from the United States as a benchmark for comparison. While most of the included studies were conducted within the US, employing this reference to evaluate findings from studies conducted in other regions may introduce comparability bias. In particular, the digital divide also existed on a regional level due to differences in ICT infrastructures29, and developing regions may be more vulnerable to the divide. We performed subgroup analyses restricted to U.S.-only studies to measure the changes in digital engagement within the same national reference frame. Although limited by small sample sizes, these analyses similarly reflected a narrowing of the digital divide since 2014 for both current internet use and smartphone ownership (Supplementary Figs. 16 & 17), which were largely consistent with the overall temporal trends. Nonetheless, this approach cannot fully account for cross-regional differences. Furthermore, we did not perform subgroup comparisons with healthy subjects by demographic characteristics (e.g., age or gender). The included sample was on average middle-aged with balanced gender distribution, making comparisons with the general population a reasonable benchmark. Therefore, future research should explore subgroup-specific digital divides, such as in older age groups to address the intersectionality between multiple disadvantaged status and develop region-specific benchmarks spanning multiple geographic areas to improve the robustness and generalizability of findings.
Fourthly, other variables, such as cognitive functioning, housing situation and income level, have been identified in prior research as factors influencing digital engagement but could not be examined in this meta-analysis due to insufficient reporting across included studies26,30,31. Although efforts were made to extract data on socio-economic status and living situation, these variables were rarely available and often unstandardized, which may partly explain the high residual heterogeneity observed in our analyses. Besides, while different psychiatric diagnoses may influence digital engagement, our analysis primarily distinguished between individuals with and without psychosis, as it was the most consistently reported diagnostic category across included studies. Other diagnoses, such as affective disorders or substance use disorders, were less frequently or inconsistently documented, making reliable analyses infeasible. Finally, only fundamental evaluation of the internet usage gap rather than examining specific online activities were reviewed in this study. It is possible that psychiatric populations differ from the general population not only in access but also in how they use the internet. Future research could examine specific types of internet use to provide a more nuanced understanding of the usage gap and to inform targeted interventions.
In conclusion, our findings suggest that the gap in internet usage and device ownership between the general population and psychiatric populations has substantially narrowed but may have widened since 2020, calling for continued monitoring of the gaps. Moreover, research on digital inclusion should shift focus on the patterns of internet use as a discrepancy between current and daily internet usage within the psychiatric population was observed. Individual factors including older age, male, lower education, diagnosis of psychosis and employment were found to be related with digital disengagement with varied directions. At macro-level, regional income inequality was also associated with internet use. Our results highlighted a complex relationship between these factors and the digital divide over time. Thus, it would be crucial to establish a standardized core outcome set for assessment of digital divide encompassing key socio-demographic factors (e.g., age, gender, living status, marital status or other social network indicators), socio-economic indicators (e.g., educational level, employment status, occupational type, income, standardized poverty measures), clinical variables (e.g., standardized diagnostic reporting, illness severity, cognitive functioning), and digital engagement metrics (e.g., digital usage patterns, device ownership, self-reported digital skills such as the Essential Digital Skills survey19). This would facilitate cross-study comparisons and comprehensive understanding of the digital divide, in support of the United Nation (UN) initiative to monitor and evaluate the maturity level of digital health in countries and institutions, implement digital health strategies and inform future policy development15.
Methods
Literature Search and Selection Criteria
This review was pre-registered on PROSPERO (ID: CRD42024542674) and adhered to the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) guidelines32 (Supplementary Table 1). A systematic search of PubMed, MEDLINE, PsycINFO, Scopus, and Web of Science was performed from database inception to 22 October 2024. The search strategy was designed to capture studies addressing the digital divide, internet use, and smartphone ownership in psychiatric populations. For the digital divide, we used the terms “digital divide”, “digital inequality”, “digital gap”, “technology inequality”, “digital disparities”, and “digital exclusion”. For internet use, we included “internet use”, “internet usage”, and “internet access.” For smartphone ownership, we included “smartphone ownership” and “smartphone access”. For psychiatric populations, search terms included “mental illness”, “mental disorder”, “psychiatric illness”, “psychiatric disorder”, “psychiatric disabilities”, “severe mental illness”, “schizophrenia”, “psychosis”, “bipolar”, “major depressive disorder”, “anxiety disorder”, “obsessive-compulsive disorder”, “mood disorder”, “substance use disorder”, “trauma-stressor related disorder”, and “eating disorder”. Within each conceptual group, terms were combined using the Boolean operator OR, and the resulting sets were combined using AND to form the final search string. Paper screening, data extraction, and quality assessment were conducted independently by two researchers (CTW Wong, HLJ Li), and disagreements were resolved through discussion with the research team.
Only peer-reviewed articles that were quantitative studies, published in English, and with separate categorical measurements on the rate of internet users (IU), smartphone owners (SO), or access among adults (aged over 18) diagnosed with any psychiatric illnesses were included. A smartphone is defined as a mobile phone with apps and internet capabilities. Studies were excluded if they, (1) did not measure SO and IU as categorical variables; (2) no separate information were reported for individuals with psychiatric illnesses; (3) involved samples with problematic internet use or internet abuse; or (4) were abstract, poster, qualitative studies, case reports, or reviews. For longitudinal studies with multiple follow-up studies, the study with the clearest definition and measurement period of IU and/or SO was chosen.
Data extraction and risk of bias assessment
The following information was systematically extracted from each study: (1) study and sample characteristics: sample size, study region, age, gender, educational level, employment, data collection period, and diagnosis; and (2) the rate and measurement period of SO and IU. When data collection period was not provided, the year used for national data comparison in the study, or the year of journal acceptance was extracted instead. The rates were extracted separately for different psychiatric diagnoses and study regions where possible. To reflect clearly the temporal relationship of the data, past users/owners were categorised as non-users or non-owners. IU was extracted along with their measurement period, IU was classified as current IU (non-daily internet usage, including user in the last 3 months, 12 months, monthly and weekly user) or daily IU, as the latter indirectly represented familiarity and regular usage of the internet that is distinct from simply having used the internet (Supplementary Table 5). The access rate of smartphones was used as equivalent as SO when SO was not provided. Gini Indices of the regions for the year closest to the midpoint of included study data collection year were obtained from the World Bank33. The Gini Index measures income inequality, where a higher index indicates higher degrees of inequality34. The quality of the studies included in the current review was assessed using the Joanna Briggs Institute (JBI) checklist35 (Supplementary Table 6). The included studies were ranked according to their quality.
Statistical Analysis
Meta-analyses were conducted to examine the bi-yearly temporal trends for SO, current and daily IU among psychiatric populations. Studies were allocated to bi-yearly intervals using the midpoint of each study’s data collection period to ensure sufficient sample size and account for rapid technological changes. Random-effects models were applied to the meta-analyses of proportions, with logit transformation used to stabilise variance and improve the normality assumptions. A normal approximation interval based on summary measures was used to estimate the confidence interval (CI)36. Meta-analyses were performed with data when at least 2 studies were available for an outcome and period. The Cochran’s Q, Tau² and I2 statistics were used to estimate heterogeneity between studies, with high heterogeneity indicated by an I2 > 75%. The robustness of results was tested by performing sensitivity analyses using the leave-one-out method and removing studies of low quality (ranking in the lower 75% quartile of quality score) to evaluate the changes in effect size in current IU and SO. Funnel plots and Egger’s test were used to assess publication bias in current IU and SO. As the data for daily IU was relatively limited and concentrated within certain periods, sensitivity analysis and publication bias tests were not conducted.
Temporal trends were visualized by plotting bi-yearly pooled rates with locally weighted linear regression (LOESS) smoothing37. Following the methodology of a previous meta-analysis13, as most included studies were conducted in the US, the corresponding US national data retrieved from International Telecommunication Union1 was utilised as a benchmark for comparing SO and current IU. Since no equivalent national data were available on daily IU, comparisons were only made against current IU to examine the differences between having used the internet and regular internet use. To validate the changes in the usage and ownership gaps within the same national reference frame, sensitivity analyses were performed on US-only studies.
Separate meta-regressions were performed for age, gender, educational level, employment status, Gini index, and presence of psychosis on SO, current and daily IU, with year of data collection as controlled variable. The potential interrelated effects of sociodemographic variables (i.e., age, gender, employment status and educational level) were explored through multivariate meta-regression. Explorative meta-regression analyses were also conducted on the pandemic effects (pre-2020 vs post-2020), and WHO regional differences on the outcomes while controlling for the year of data collection. Sensitive analysis was conducted by excluding 2020-2021 studies when possible. Regional sub-group meta-analyses further complemented the results on regional differences in the outcomes.
All analyses were performed with R (version 4.4.2), using the R package “metafor”36.
Data Availability
The datasets generated and/or analyzed during the current study are not publicly available, as they comprise extracted data from both open-access and subscription-based published studies. However, they are available from the corresponding author upon reasonable request.
Code availability
No custom code was used in the analysis but the R scripts used in the current study is available on reasonable request from the corresponding author.
References
International Telecommunication Union. World Telecommunication/ICT Indicators Database - Individuals using the Internet (% of population) (IT.NET.USER.ZS). (2025).
Alfano, V. & Ercolano, S. The efficacy of lockdown against COVID-19: a cross-country panel analysis. Appl. Health Econ. Health Policy 18, 509–517 (2020).
United Nations. Sustainable Development Goals. (2015).
United Nations Department of Economic and Social Affairs. The Sustainable Development Goals Report 2025. (2025).
van Dijk, J. A. G. M. Closing the Digital Divide: The Role of Digital Technologies on Social Development, Well-Being of All and the Approach of the Covid-19 Pandemic. (2020).
Van Dijk, J. The Deepening Divide: Inequality in the Information Society. (SAGE Publications, Inc., 2455 Teller Road, Thousand Oaks California 91320 United States). https://doi.org/10.4135/9781452229812. (2005).
Badr, J., Motulsky, A. & Denis, J.-L. Digital health technologies and inequalities: a scoping review of potential impacts and policy recommendations. Health Policy 146, 105122 (2024).
Lythreatis, S., Singh, S. K. & El-Kassar, A.-N. The digital divide: a review and future research agenda. Technol. Forecast. Soc. Change 175, 121359 (2022).
Tsetsi, E. & Rains, S. A. Smartphone Internet access and use: extending the digital divide and usage gap. Mob. Media Commun. 5, 239–255 (2017).
Wadman, R. et al. Patterns of internet use in people diagnosed with severe mental illness: qualitative interview study. J. Med. Internet Res. 27, e55072 (2025).
Marbin, D. et al. Use of digital technologies by users of psychiatric inpatient services in Berlin, Germany: a cross-sectional patient survey. BMJ Open 13, e067311 (2023).
Žaja, N. et al. Internet use among patients with schizophrenia and depression. Int. J. Environ. Res. Public. Health 19, 5695 (2022).
Firth, J. et al. Mobile phone ownership and endorsement of “mHealth” among people with psychosis: a meta-analysis of cross-sectional studies. Schizophr. Bull. 42, 448–455 (2016).
Spanakis, P. et al. Use of the internet and digital devices among people with severe mental Ill health during the COVID-19 pandemic restrictions. Front. Psychiatry 12, (2021).
World Health Organization. Global Strategy on Digital Health 2020-2025. (World Health Organization, Geneva, 2021).
Fuchs, C. The Role of Income Inequality in a Multivariate Cross-National Analysis of the Digital Divide. Soc. Sci. Comput. Rev. https://doi.org/10.1177/0894439308321628. (2008).
International Telecommunication Union. ICT Price Baskets, historical data series. (2024).
Statistics Canada. Smart phone price index, monthly. Government of Canada https://doi.org/10.25318/1810020901-ENG (2021).
Spanakis, P. et al. Measuring the digital divide among people with severe mental ill health using the essential digital skills framework. Perspect. Public Health 144, 21–30 (2022).
Ramsetty, A. & Adams, C. Impact of the digital divide in the age of COVID-19. J. Am. Med. Inform. Assoc. 27, 1147–1148 (2020).
Hwang, H. & Nam, S. The digital divide experienced by older consumers in smart environments. Int. J. Consum. Stud. 41, 501–508 (2017).
Tappen, R. M., Cooley, M. E., Luckmann, R. & Panday, S. Digital Health Information Disparities in Older Adults: a Mixed Methods Study. J. Racial Ethn. Health Disparities 9, 82–92 (2022).
Oliver, M. I., Pearson, N., Coe, N. & Gunnell, D. Help-seeking behaviour in men and women with common mental health problems: cross-sectional study. Br. J. Psychiatry 186, 297–301 (2005).
Luciano, A. & Meara, E. The employment status of people with mental illness: National survey data from 2009 and 2010. Psychiatr. Serv. Wash. DC 65, 1201–1209 (2014).
Skrobinska, L., Newman-Taylor, K. & Carnelley, K. Psychosis and help-seeking behaviour-A systematic review of the literature. Psychol. Psychother. 97, 583–605 (2024).
Tobitt, S. & Percival, R. Switched on or switched off? A survey of mobile, computer and Internet use in a community mental health rehabilitation sample. J. Ment. Health 28, 4–10 (2019).
Federal Communications Commission. Affordable Connectivity Program (ACP) Fact Sheet. (2024).
European Union. Shaping Europe’s digital future. (2025).
United Nations. Widening Digital Gap between Developed, Developing States Threatening to Exclude World’s Poorest from Next Industrial Revolution, Speakers Tell Second Committee. (2023).
Choi, N. G. & DiNitto, D. M. The digital divide among low-income homebound older adults: internet use patterns, eHealth literacy, and attitudes toward computer/internet use. J. Med. Internet Res. 15, e2645 (2013).
Depp, C. A., Harmell, A. L., Vahia, I. V. & Mausbach, B. T. Neurocognitive and functional correlates of mobile phone use in middle-aged and older patients with schizophrenia. Aging Ment. Health 20, 29–35 (2016).
Moher, D., Liberati, A., Tetzlaff, J. & Altman, D. G. & The PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 6, e1000097 (2009).
The World Bank. The World Bank. (2012).
Subramanian, S. V. Income inequality and health: what have we learned so far? Epidemiol. Rev. 26, 78–91 (2004).
Joanna Briggs Institute. Checklist for systematic reviews and research syntheses. (2017).
Schwarzer, G., Carpenter, J. R. & Rücker, G. Meta-Analysis with R. https://doi.org/10.1007/978-3-319-21416-0 (Springer, Cham, Switzerland, 2015).
Cleveland, W. S. & Devlin, S. J. Locally weighted regression: an approach to regression analysis by local fitting. J. Am. Stat. Assoc. 83, 596–610 (1988).
Acknowledgements
This study was partly funded by the General Research Fund of the University Grants Committee of Hong Kong (Reference number 17106021) awarded to Sherry Kit Wa Chan.
Author information
Authors and Affiliations
Contributions
C.T.W.W. and S.K.W.C. are the chief investigators who conceptualised, designed the review protocol and developed the search strategy. C.T.W.W. and L.H.J.L. conducted systematic literature search and paper screening. C.T.W.W. conducted data extraction with L.H.J.L. and Y.S.V.C. C.T.W.W., H.K.H.T., W.T., C.L., and H.Z. conducted data analysis. C.T.W.W., H.K.H.T. and S.K.W.C. were responsible for writing the original draft and result visualisation. All authors revised and finalized the manuscript. All authors approved the content of the manuscript. All authors had full access to all the data in the study and had final responsibility for the decision to submit for publication.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Wong, C.T.W., Tsui, H.K.H., Li, H.L.J. et al. A Global meta-analysis of digital divide in psychiatric population from 2004 to 2023. npj Digit. Med. 9, 26 (2026). https://doi.org/10.1038/s41746-025-02203-y
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41746-025-02203-y
