
Abstract
Background
Risk-versus-benefit optimization required a quantitative comparison of the two. The latter, directly related to effective diagnosis, can be associated to clinical risk. While many strategies have been developed to ascertain radiation risk, there has been a paucity of studies assessing clinical risk, thus limiting the optimization reach to achieve a minimum total risk to patients undergoing imaging examinations. In this study, we developed a mathematical framework for an imaging procedure total risk index considering both radiation and clinical risks based on specific tasks and investigated diseases.
Methods
The proposed model characterized total risk as the sum of radiation and clinical risks defined as functions of radiation burden, disease prevalence, false-positive rate, expected life-expectancy loss for misdiagnosis, and radiologist interpretative performance (i.e., AUC). The proposed total risk model was applied to a population of one million cases simulating a liver cancer scenario.
Results
For all demographics, the clinical risk outweighs radiation risk by at least 400%. The optimization application indicates that optimizing typical abdominal CT exams should involve a radiation dose increase in over 90% of the cases, with the highest risk optimization potential in Asian population (24% total risk reduction; 306% \({{CTDI}}_{{vol}}\) increase) and lowest in Hispanic population (5% total risk reduction; 89% \({{CTDI}}_{{vol}}\) increase).
Conclusions
Framing risk-to-benefit assessment as a risk-versus-risk question, calculating both clinical and radiation risk using comparable units, allows a quantitative optimization of total risks in CT. The results highlight the dominance of clinical risk at typical CT examination dose levels, and that exaggerated dose reductions can even harm patients.
Plain language summary
The proper practice of radiology (using imaging technology to diagnose and treat diseases) should take into consideration both the risk and benefit to a patient. Such a comparison can be hard because risk and benefit are measured in different ways. The risk includes some amount of radiation exposure to patients which can cause harm, but the benefit could be identifying a medical problem that needs attention. To overcome this obstacle, we developed a mathematical model describing the risk-to-benefit of a medical imaging study. Our modeling exercise found that the clinical benefit outweighs the radiation risk. The finding that benefit of detecting a problem is worth the risk of imaging is contrary to common belief. This study shows that so much emphasis could be put on radiation safety in imaging that avoiding imaging could negatively impact patients’ path of care.
Similar content being viewed by others
Introduction
Decision making in medicine is based on the benefit-to-risk ratio of a planned procedure. In radiology, this is reflected in the application of justification and optimization principles1,2. In particular, justification implies the characterization that the benefit of a radiological procedure outweighs any potential risk, while optimization aims to maximize the benefit over risk, particularly the radiation risk associated with the procedure2. Therefore, the proper practice of radiology should take into consideration the simultaneous and quantitative assessment of both radiation risk and benefit of a procedure. However, this has been a major challenge as the risk and benefit rarely use comparable units3. The need for optimization is particularly relevant in Computed Tomography (CT) as the leading source of radiation exposure per capita in the US4.
To characterize radiation risk, many metrics and surrogates have been developed with different degrees of appropriateness5,6,7. These include Computed Tomography Dose Index (CTDIvol), Effective dose, and Risk Index (RI). CTDIvol and its derivatives (e.g., Size-Specific Dose Estimate and Dose length Product) reflect radiation output in standardized phantoms, and have been used as surrogate metrics of risk in the absence of more representative alternatives. Effective dose offers a more risk-representative, but does not account for patient age and sex. Risk Index (RI), which includes age-, sex-, and tissue-specific risk coefficients, is currently the closest metric to represent the patient radiation burden in CT.
To characterize imaging benefit, one may quantify the benefit of a radiological procedure in term of the anticipated theoretical image quality (e.g., detectability index8,9,10) as a proxy of the potential for a more precise characterization of disease or the lack thereof. Better, imaging benefit can be quantified in terms of the clinical outcome associated with an effective diagnosis11. However, these benefit metrics have different units than those associated with radiation risk and thus cannot be put in perspective with radiation risk and thus used for justification or optimization in purposes. This lack is perhaps the primary reason why optimization of radiological procedures tends to be one-sided and strongly biased towards radiation risk only. One may, however, estimate the likelihood of a misdiagnosis, the reciprocal of the benefit conceptualizing a so-called clinical risk. This enables the comparison of radiation and clinical risk with comparable units, thus allowing optimization of an imaging procedure. This idea was postulated in 20183, but has not yet been demonstrated for a clinical scenario.
The purpose of this study was to develop a mathematical model to estimate a total risk index considering the radiation risk and clinical benefit of a CT imaging procedure undergoing abdominal exam. The model was tested on a population of one million digital twins simulating the clinical cancer scenario of detecting liver cancer. The study assessed a total risk as functions of the radiation burden, the prevalence of the disease, the false positive rate, the expected life-expectancy loss for an incorrect diagnosis, and the radiologist interpretative performance. The results highlight that, for all demographics, the clinical risk outweighs radiation risk by at least 400%, and that optimizing typical abdominal CT exams should involve a radiation dose increase in over 90% of the cases. At typical CT examination dose levels, clinical risk is highly dominant, and exaggerated dose reductions can even harm patients.
Methods
Total risk formalism
In this study, the total risk (\({R}_{t}\)) associated with a CT procedure is characterized as the additive risk of radiation risk (\({R}_{r}\)) and clinical risk (\({R}_{c}\)):
The radiation risk is defined as
where \(p\) is the prevalence of the considered disease in a CT population calculated as the ratio of patients diagnosed with the considered disease and patients undergoing a CT exam after referral for symptoms that might be associated with the same pathology; \({RI}\) is the risk index as described by Li et al. calculated by applying to each organ the age-, sex-, and tissue-specific lifetime attributable risk of cancer incidence coefficients reported in BEIR VII publication12,13; \(s\) is the 5-year survival rate for a new cancer as reported by the National Cancer Institute Surveillance, Epidemiology, and End Results Program (NCI-SEER), recorded as 68.7% at the time of the manuscript preparation14; and \(\beta\) is the false positive to true positive ratio for the detection of the investigated pathology. The \(\left(1+\beta \right)\) factor implies that, in case of a false positive, the patient will probably undergo a further CT examination during his path or care.
The clinical risk is defined as
The \(\left(1-\beta \right)\) factor implies the clinical risk is null under a false positive result, whereas the parameter \(\alpha\) describes the expected life-expectancy loss for an incorrect diagnosis as the predicted years of survival for a correct diagnosis minus the predicted years of survival for an incorrect diagnosis. The \(\alpha\) parameter was calculated per each race, sex, and age group based on the survival rates for different tumor stages reported by the NCI-SEER program14.
Combining Eqs. (1), (2), and (3), the resulting total risk is estimated as
Equation (4) provides the total risk associated with a radiological procedure including factors for the radiation burden for different age and sex, the prevalence of the disease, the false positive rate, and the expected life-expectancy loss for an incorrect diagnosis including the effects of age, sex, and race.
Extension of total risk concept to cancer cases
In case of an oncological disease, the stage of the cancer is indicated with \(k\), where \(k=0\) indicates no tumor, and \(k=1,\,2,\,3\) are related to localized, regional, and distant stages, respectively. Therefore, \({p}_{k}\) represents the prevalence of each tumor stage in a clinical CT population with \({p}_{0}\) being the prevalence of non-tumor cases, and \({\alpha }_{k}\) represents the expected life-expectancy loss for the incorrect diagnosis per each tumor stage with \({\alpha }_{0}=0\) and \({\alpha }_{k}\) is the predicted years of survival for stage k minus the predicted years of survival for stage \(k+1\).
\({\beta }_{k}\) represents the false positive to true positive ratio for the detection of the stage \(k\) of the considered tumor. \({\beta }_{k}\) can be inferred from the Receiver Operating Characteristic curve (ROC) via a simply polynomial fit as
where \({ROC}\left({\gamma }_{k}\right)={x}^{{\gamma }_{k}}\) or \({{AUC}}_{k}={\int }_{0}^{1}{x}^{{\gamma }_{k}}{dx}\), resulting in
From Eqs. (5) and (6) it follows that
Finally, Eqs. (4) and (7) together yield:
The values of\(\,{p}_{k},\,{\alpha }_{k}\), \({\beta }_{0},\) and \({{AUC}}_{k}\) can be retrieved from literature, historical record, and any other validated source.
Demonstration to a digital twin liver cancer population
To demonstrate the feasibility of the described model in clinical practice, Eq. (8) was applied to a population of one million cases simulating a liver cancer scenario. The demographic information was taken from the publicly available 2019 Census Population Estimates by Age, Sex, Race, and Hispanic Origin15. In particular, The United States Census Bureau presents race and ethnic categories as separate questions, and data are collected based on self-identification. The patient population was simulated in eight different cohorts with genders of male and female, and races/ethnicities of white, Black, Hispanic, and Asian. The total population sample size allowed the inclusion of a considerable number of cases in each group. For each simulated patient, the age was randomly sampled from a uniform distribution, which spanned the age range of the individual demographic groups. Because the study involved only simulated digital twins, IRB approval was not required.
Concerning patient body habitus, for each of the eight separate demographic cohorts, the waist diameter in centimeters was randomly sampled per patient from a truncated normal distribution with mean and standard deviation based on their demographic information (age, sex, and race). The waist circumferences means and their standard errors were obtained from the publicly available Center for Disease Control and Prevention Anthropometric Reference Data for Children and Adults: United States 2015–201816. The standard errors of the means were converted to standard deviations that, together with the means, were multiplied by \(1/\pi\) to obtain the sampling distribution of diameter. The normal distributions were truncated to 0 for the lower bound, and the 95th percentile value plus 15 cm for the upper bound.
The CT scanner radiation output was obtained per each simulated case in terms of volume CTDI (\({{CTDI}}_{{vol}}\)). The administered \({{CTDI}}_{{vol},0}\) was calculated using the well-established exponential relationship between patient diameter and \({{CTDI}}_{{vol}}\), and applying the fitting coefficients extracted from a clinical population of 735 patients undergoing abdominopelvic CT with a maximum upper bound \({{CTDI}}_{{vol}}\) of 50 mGy7. Table 1 reports the number of cases, age, waist diameter, and utilized CTDIvol for the simulated population per sex and race/ethnicity group.
The cancer incidence and expected life expectancy in terms of 5-year survival rate for each case per different sex, race/ethnicity, age, and stage of diagnosis was extracted from the NCI-SEER. The total risk (\({R}_{t,0}\)) was calculated for a typical false positive to true positive ratio of \({\beta }_{0}=5 \%\) and it was assumed that each case received an average radiologist interpretative performance of \({{AUC}}_{0}=0.75\) for a hypothetical lesion without any changes in radiation dose beyond routine practice17.
To explore the potential use of the framework for imaging optimization (radiation dose minimization), 2000 imaging conditions were simulated for each patient while varying \({{CTDI}}_{{vol}}\) from 0.1 and 200 mGy with 0.1 mGy increments. Per each \({{CTDI}}_{{vol}}\) value, the anticipated area under the receiver operating characteristic curve (AUC) was calculated by applying an expected asymptotic relationship between \({{CTDI}}_{{vol}}\) and image quality18 as:
where \(q\) represents an image quality surrogate of diagnostic quality (e.g., detectability index, or signal to noise ratio)18,19, and \({erf}\) is the error function. Expecting \({q}^{2}\propto {{CTDI}}_{{vol}}\), Eq. (9) was re-written as
where \(t\) represents a parameter returning the arbitrary \({{AUC}}_{0}\) when \({{CTDI}}_{{vol}}={{CTDI}}_{{vol},0}\)
where \({inverf}\) is the inverse function of \({erf}\). For this study, \(t\left({{AUC}}_{0}=0.75\right)=0.90987\).
The \({AUC}\) values distribution generated after applying Eq. (10) to the 2000 imaging conditions per each patient was inputted in Eq. (8) to calculate the total risk distribution. The analytical minimum of such distribution represented the theoretical minimum total risk \({R}_{t,\min }\) for the patient with the related \({{CTDI}}_{{vol},\min }\) representing the theoretical radiation dose that should be administered to minimize the overall total risk. Percentage differences between \({R}_{t,\min }\) and \({R}_{t,0}\), and between \({{CTDI}}_{{vol},\min }\) and \({{CTDI}}_{{vol},0}\) were calculated. Finally, the data were stratified in terms of patient age, sex, and race/ethnicity.
Reporting summary
Further information on research design is available in the Nature Portfolio Reporting Summary linked to this article.
Results
Application to typical scanning and clinical condition
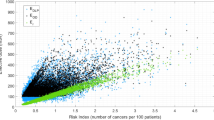
For the case of a typical false positive to true positive ratio of \({\beta }_{0}=5 \%\) and average radiologist interpretative performance of \({{AUC}}_{0}=0.75\), the radiation risk among the whole population ranged between 0.0009 and 0.061 deaths per 100 patients (mean: 0.009; median: 0.008); the clinical risk ranged between 0.00007 and 0.094 deaths per 100 patients (mean: 0.045; median: 0.049); and the total risk ranged between 0.002 and 0.146 deaths per 100 patients (mean: 0.053; median: 0.057). Results aggregated by sex and race are reported in Table 2. Figure 1 shows the distribution of radiation, clinical, and total risk for the whole population. The results show that the overall clinical risk exceeds that of radiation risk for the vast majority of cases. This is more evident for Asian patients because they exhibit higher liver cancer related mortality rates according to NCI-SEER program data.

Distributions of the calculated radiation, clinical, and total risk for the whole population of 1 million patients, assuming typical false positive to true positive ratio of \({\beta }_{0}=5 \%\) and average radiologist interpretative performance of \({{AUC}}_{0}=0.75\). \({{CTDI}}_{{vol}}\) ranged between 1.8 mGy and 50 mGy. The red line represents the median and the blue boxes represent the 1st and 3rd quartile. Values that exceed 1.5 times interquartile length (black whiskers) are in red.
Risk-versus-risk optimization
Concerning the application of the model to estimate the theoretical minimum risk, \({R}_{t,\min }\), Fig. 2 shows two examples of the distributions of radiation, clinical, and total risk with the CTDIvol ranged from 0.1 and 200 mGy with 0.1 mGy increments and AUC values calculated from Eq. (10). In particular, we show case example of patient n. 561,907 and patient n. 101,174, representing the first and third quartile of theoretical risk reductions (first quartile: 15.9%; third quartile: 2.1%). Moreover, Fig. 3 shows the comparison between the distributions of \({{CTDI}}_{{vol},0}\) and \({{CTDI}}_{{vol},\min }\), and the related \({R}_{t,0}\) and theoretical minimum total risk \({R}_{t,\min }\) across the whole population. In this data, \({{CTDI}}_{{vol},\min }\) ranged between 0.1 and 98.2 mGy (mean: 39.8; median: 38.5), and \({R}_{t,\min }\) ranged between 0.0001 and 0.129 deaths per 100 cases (mean: 0.049; median: 0.050). The mean percentage difference between \({{CTDI}}_{{vol},\min }\) and \({{CTDI}}_{{vol},0}\) was 153.9% (median: 141.8%; min: −99.8%; max: 694.7%) and the average total risk reduction across the whole population was 10.5% (median: 7.4%; min: 0.0%; max: 98.3%). Out of the one million patients, we found 93,242 cases in which the administered \({{CTDI}}_{{vol},0}\) was higher than the radiation output required to achieve the minimum risk \(({{CTDI}}_{{vol},\min })\)); for 570 cases, the administered \({{CTDI}}_{{vol},0}\) exactly corresponded to the \({{CTDI}}_{{vol},\min }\); and for the majority of 906,188 cases (90.6%), the administered \({{CTDI}}_{{vol},0}\) was lower than \({{CTDI}}_{{vol},\min }\).

Distributions of radiation, clinical, and total risk with the CTDIvol ranged from 0.1 and 200 mGy for patient n. 561,907 and patient n. 101,174, corresponding to the cases for which the first and third quartile theoretical risk reduction was achieved.

Comparison between the distributions of \({{CTDI}}_{{vol},0}\) and \({{CTDI}}_{{vol},\min }\), and the related \({R}_{t,0}\) and theoretical minimum total risk \({R}_{t,\min }\) across the whole population. The red line represents the median and the blue boxes represent the 1st and 3rd quartile. Values that exceed 1.5 times interquartile length (black whiskers) are in red.
Figure 4 shows the theoretical minimum total risk for age, sex, and race/ethnicity for the whole population. The jaggedness of the trends is reflective of the expected life-expectancy loss data that are categorized for race/ethnicity, age, and sex14. Figure 5 shows the percentage difference between the theoretical minimum total risk \({R}_{t,\min }\) and \({R}_{t,0}\) versus age for difference sex and race/ethnicity. Figure 6 shows the percentage difference between the administered \({{CTDI}}_{{vol},0}\) and the radiation output required to achieve the minimum risk \(({{CTDI}}_{{vol},\min })\)) versus age for different sex and race/ethnicity. As reported in Table 3, the Asian female group had the highest total risk reduction potential (−26.6%), whereas the Hispanic male group had the lowest (−4.7%).

Theoretical minimum total risk versus age for the whole population (left), male patients (center), and female patients (right). Different colors are different races/ethnicities.

Percentage difference between the theoretical minimum total risk \({R}_{t,\min }\) and \({R}_{t,0}\) versus age for the whole population (left), male patients (center), and female patients (right). Different colors are different races/ethnicities.

Percentage difference between the administered \({{CTDI}}_{{vol},0}\) and the radiation output required to achieve the minimum risk \(({{CTDI}}_{{vol},\min })\)) versus age for the whole population (left), male patients (center), and female patients (right). Different colors are different races/ethnicities.
Discussion
In this study, we implemented and demonstrated a mathematical model to characterize the interplay between radiation risk and clinical benefit in CT in terms of a risk-versus-risk optimization strategy. Such a framework allows a complete depiction of the total risk associated with an imaging procedure including both the radiation and the clinical risk. To our knowledge, this is the first attempt to define a method that can quantitatively optimize a radiological procedure including its benefit component. We tested the model to a population of one million digital twins simulating a liver cancer scenario. Our estimation in terms of radiation risk are consistent with other studies estimating lifetime attributable cancer mortality risks associated with CT procedures7,20,21. In the absence of data describing the clinical risk associated with radiological procedures, our approach provides a theoretical methodology to put the imaging benefit in terms that can be related to radiation risk.
When the model was applied to a scenario reproducing routine scanning condition and typical radiologist interpretative performance (false positive to true positive ratio of \({\beta }_{0}=5 \%\), and \({{AUC}}_{0}=0.75\)) for a hypothetical liver cancer lesion17, the results highlighted the dominance of clinical risk. In particular, the clinical risk was found to largely outweigh the radiation risk by a factor of 4 to 5 (Fig. 1, Table 2). This is so in spite of the fact that we used a relatively large radiation dose levels for our modeled imaging scenarios (or CTDIvol of up to 50 mGy), higher than many current low-dose CT practices. This dominance of clinical risk over radiation risk was consistent across population groups, ranging from fourfold in female Hispanic to over ninefold in female Asian patients highlighting the need to incorporate patient demographic in the radiological procedure risk-to-benefit assessment. This is contrary to common assumption about radiation risk that dominates the common understanding of CT safety. Our results in fact emphasize how the over-exaggerated and obsessive understanding of radiation dose, as most recently reflected in the Centers for Medicare and Medicaid Service ruling22, can impact patient safety negatively.
Assessing the relevance of the mathematical model in the design of optimization strategies, we simulated, 2000 imaging conditions (\({{CTDI}}_{{vol}}\) varying from 0.1 and 200 mGy) per patient, resulting in 2000 different AUC values. Utilizing the distributions of the related radiation, clinical, and total risks, the theoretical minimum total risk \({R}_{t,\min }\) was estimated per patient. The optimum dose level (\({{CTDI}}_{{vol},\min }\)) was found be higher than the starting \({{CTDI}}_{{vol},0}\) in over 90% of the cases implying that, for these procedures, increasing the scanner output could have in fact reduced the overall risk to the patient (Figs. 2, and 3, Table 3). This advantage of increased dose was age-, sex-, and race-dependent, with the highest potential for risk optimization is in the Asian population, with 24% theoretical total risk reduction on average corresponding to a 306% increase in \({{CTDI}}_{{vol}}\); whereas, the Hispanic group showed the lowest average hypothetical total risk reduction of 5% with an 89% scanner output increase.
In the described scenario, it is important to highlight that patient demographic information influence both radiation and clinical risk. In particular, the patient size dictates the scanner X-ray output in exams performed with automated tube current modulation. Moreover, the risk index is calculated by applying age- and sex-specific lifetime attributable risk of cancer incidence coefficients to each organ resulting in a decreasing radiation risk for older patients. Lastly, the clinical risk incorporates the difference between the predicted years of survival for correct and incorrect diagnosis which is also age-, sex-, and race-specific. Such a difference in survival for correct and incorrect diagnosis largely outweighs the stochastic radiation risk resulting in clinical risk dominating the resulting total risk.
Our findings are consistent with what the International Commission of Radiation Protection recommended in publication 135: “Optimization is generally concerned with maintaining the quality of the diagnostic information provided by the examination commensurate with the medical purpose while, at the same time, seeking to reduce patient exposures to radiation to a level as low as reasonably achievable. Image quality or, more generally, the diagnostic information provided by the examination (including the effects of postprocessing) must also be evaluated. […] In some cases, optimization may result in an increase in dose.”23. This statement represented a paradigm shift in the traditional CT optimization approach that is either based on radiation dose only, or incorporates image quality without quantitatively assessing the resulting clinical outcome24. Our model, instead, proposes a comparison of radiation and clinical risk with comparable units allowing a complete depiction of the total risk associated with a CT procedure and a comprehensive risk-to-benefit assessment.
Our methodology can be considered not only for optimization of imaging procedures but also from the perspective of radiation protection justification. The justification of a medical procedure is meant to be patient-specific, though not always, as in the case of COVID-19 diagnosis or cancer screening where population aggregates have been used25,26. The model introduced in this study can help to better inform the justification of an exam both for the single individual and for a population (e.g., an exam might be justified for an ethnic group and sex, but not for another).
This study had a few limitations. First, while we equated radiation and clinical risks through identical units, they are associated with different timeframes: the risk related to radiation exposures is associated with the adverse effects in years and decades, whereas the clinical risk is associated with the specific pathology progression that tends to have shorter timespans. The proposed model should be extended to include differing time horizons. Second, our study focused on only one clinical task associated with liver cancer. The framework can be extended to other diagnostic tasks. To do so, one can designate a “most difficult task” as the limiting task of a protocol, thus ordain the optimization process for imaging of that body part. Third, the described method does not include many potential additional or ancillary clinical variables that are patient specific and may weigh in when deciding the appropriateness of an imaging procedure. Fourth, this study did not associate any uncertainties to the calculated quantities. Currently, only models describing radiation risk uncertainties are available, and it has been reported that the averaged relative error for risk index in abdominopelvic examinations is 0.27. Future studies can aim to assess the overall total risk uncertainties. Lastly, the false positive to true positive ratio of \({\beta }_{0}=5 \%\), and \({{AUC}}_{0}=0.75\) were chosen to describe typical radiologist interpretative performance on a typical, relevant cancer detection task. Although these are reasonable assumptions17, different practices can be represented by different\(\,{\beta }_{0}\) and \({{AUC}}_{0}\) values, thus leading to different results. Nevertheless, the validity of the proposed model is not impacted by the specific interpretative performance and can be applied to any set of targeted false positive to true positive ratio and area under the ROC curve.
Conclusion
A mathematical framework to describe total risk in CT was implemented and robustly tested in a simulated dataset of 1,000,000 CT studies reproducing a clinical liver cancer detection scenario. Framing risk-to-benefit assessment as a risk-versus-risk question, calculating both clinical and radiation risk using comparable units, allows a quantitative depiction of total risks in CT. Yielding differing results across patient age and race stratifications, the results highlighted the dominance of clinical risk at typical CT examination dose levels and that, in the current practice, there is room for increase in radiation dose to the benefit of the patient. Further, exaggerated dose reductions beyond current levels can even harm patients. Care should be exercised that any dose reduction should not be done at the expense of quality patient care, and the mathematical model demonstrated in this study can aid in quantitative individualized justification and optimization of imaging exams.
Data availability
All data generated and analyzed in the study (source data) are publicly available via the CERN’s Zenodo repository (https://doi.org/10.5281/zenodo.13715861)27. Particularly, the dataset includes the data summarized in all the tables and the figures reported in this manuscript. Any publication of results obtained with this dataset should reference this paper. Moreover, the demographic and anatomical information taken from the 2019 Census Population Estimates15 and from the Center for Disease Control and Prevention Anthropometric Reference Data for Children and Adults: United States 2015–201816, are publicly available. Any further information about data calculation and analysis is available from the corresponding author on reasonable request.
References
Basic Safety Standards. GSR part 3. International Atomic Energy Agency, Vienna 3, 471 (2014).
Icrp. The 2007 Recommendations of the International Commission on Radiological Protection. ICRP Publication 103. Annals of the ICRP 37, 9–34. (2007).
Samei, E. et al. Medical imaging dose optimisation from ground up: expert opinion of an international summit. J. Radiol. Prot. 38, 967–989 (2018).
NCRP. NCRP. National Council on Radiation Protection and Measurements. Medical Radiation Exposure of Patients in the United Stated (2019), (2019). NCRP Report no. 184. 2019. Report No.: ISBN: 9781944888169.
McCollough C., et al. AAPM report n.96. The Measurement, Reporting, and Management of Radiation Dose in CT, The Report of AAPM Task Group 23. College Park, MD; 2008.
Valentin, J. Managing patient dose in multi-detector computed tomography(MDCT). ICRP Publication 102. Ann. ICRP 37, 1–79 (2007).
Ria, F. et al. Comparison of 12 surrogates to characterize CT radiation risk across a clinical population. Eur. Radiol. 31, 7022–7030 (2021).
Cheng, Y. et al. Validation of algorithmic CT image quality metrics with preferences of radiologists. Med. Phys. 46, 4837–4846 (2019).
Cheng, Y., Smith, T. B., Jensen, C. T., Liu, X. & Samei, E. Correlation of algorithmic and visual assessment of lesion detection in clinical images. Acad. Radiol. 27, 847–855 (2020).
Smith, T. B., Solomon, J. & Samei, E. Estimating detectability index in vivo: development and validation of an automated methodology. J. Med. Imaging 5, 1–9 (2017).
Icrp. Radiation protection in medicine. ICRP Publication 105. Ann. ICRP. 2007.
Li, X. et al. Patient-specific radiation dose and cancer risk estimation in CT: part II. Application to patients. Med. Phys. 38, 408–419 (2011).
Health Risks from Exposure to Low Levels of Ionizing Radiation: BEIR VII Phase 2. (Washington, D.C.: National Academies Press, 2006).
National Cancer Institute Surveillance E, and End Results Program. SEER*Explorer: An interactive website for SEER cancer statistics. Surveillance Research Program, National Cancer Institute; 2023 Apr 19. 2023 https://seer.cancer.gov/statistics-network/explorer/.
Census.gov. 2019 Population Estimates by Age, Sex, Race and Hispanic Origin: Census.gov; 2020 https://www.census.gov/newsroom/press-kits/2020/population-estimates-detailed.html.
Fryar CDC, M.D.; Gu, Q.; Afful, J.; Ogden, C.L. Anthropometric reference data for children and adults: United States, 2015–2018. Washington, DC: National Center for Health Statistics; 2021.
Mileto, A. et al. CT detectability of small low-contrast hypoattenuating focal lesions: iterative reconstructions versus filtered back projection. Radiology 289, 443–54 (2018).
Rolland, J. P. & Barrett, H. H. Effect of random background inhomogeneity on observer detection performance. J. Opt. Soc. Am. A. 9, 649–58 (1992).
Barrett, H. H., Myers, K. J., Hoeschen, C., Kupinski, M. A. & Little, M. P. Task-based measures of image quality and their relation to radiation dose and patient risk. Phys. Med. Biol. 60, R1 (2015).
Zewde, N., Ria, F. & Rehani, M. M. Organ doses and cancer risk assessment in patients exposed to high doses from recurrent CT exams. Eur. J. Radiol. 149, 110224 (2022). (February).
Bosch de Basea Gomez, M. et al. Risk of hematological malignancies from CT radiation exposure in children, adolescents and young adults. Nat. Med. 29, 3111–9 (2023).
Excessive radiation dose or inadequate image quality for diagnostic computed tomography (CT) in adults (Facility IQR), CMS1074v1 (2023).
Vañó, E. et al. ICRP Publication 135: diagnostic reference levels in medical imaging. Ann. ICRP 46, 1–144 (2017).
McCollough, C. H. & Leng, S. Use of artificial intelligence in computed tomography dose optimisation. Ann. ICRP 49, 113–25 (2020).
Ria F. et al. A comparison of COVID-19 and imaging radiation risk in clinical patient populations. J. Radiol Prot. 40, 1336–1345 (2020).
Rubin, G. D. et al. The role of chest imaging in patient management during the COVID-19 pandemic: a multinational consensus statement from the Fleischner Society. Radiology 296, 172–80 (2020).
Ria F. Optimization of abdominal CT based on a model of total risk minimization by putting radiation risk in perspective with imaging benefit. Zenodo. https://doi.org/10.5281/zenodo.13715861 (2024).
Acknowledgements
This work was funded in part by NIH/NIBIB P41EB028744 and in part by NIH/NIBIB R44EB031658.
Author information
Authors and Affiliations
Contributions
F.R.: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Visualization, Writing – original draft, Writing – review & editing. A.R.Z.: Conceptualization, Data curation, Formal analysis, Methodology, Writing – review & editing. R.L.: Conceptualization, Data curation, Formal analysis, Methodology, Writing – review & editing. A.E.: Data curation, Formal analysis, Methodology, Writing – review & editing. E.A.: Methodology, Formal analysis, Writing – review & editing. E.S.: Conceptualization, Supervision, Investigation, Methodology, Visualization, Writing – review & editing.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Peer review
Peer review information
Communications Medicine thanks Martin Fiebich, Colin J. Martin and the other, anonymous, reviewer(s) for their contribution to the peer review of this work. Peer reviewer reports are available.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Ria, F., Zhang, A.R., Lerebours, R. et al. Optimization of abdominal CT based on a model of total risk minimization by putting radiation risk in perspective with imaging benefit. Commun Med 4, 272 (2024). https://doi.org/10.1038/s43856-024-00674-w
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s43856-024-00674-w
This article is cited by
-
Enhancing diagnostic information in abdominal computed tomography (CT) images through optimized image enhancement techniques
Physical and Engineering Sciences in Medicine (2025)
