
Abstract
Background
Global warming exacerbates heatstroke, increasing its severity and associated health risks, including fatal kidney damage. Predicting post-heatstroke organ injury remains difficult, delaying timely medical intervention. This study aims to identify potential blood biomarkers that reflect organ stress and recovery status following heatstroke.
Methods
Plasma samples (n = 12) from clinically diagnosed classical (non-exertional) heatstroke patients were collected at diagnosis and recovery. Two-dimensional gel electrophoresis was used to analyze protein expression, identifying 359 protein spots. Selected proteins showing differential expression were validated by Western blotting.
Results
Here, five proteins—alpha-1 antitrypsin, alpha-1 microglobulin/bikunin precursor, apolipoprotein A-IV, clusterin, and complement component 2—show significant changes between the two timepoints. These proteins are linked to inflammatory, coagulation, and lipid metabolism pathways. Alpha-1 antitrypsin, alpha-1 microglobulin, and complement component 2 may reflect the resolution of inflammation, while apolipoprotein A-IV and clusterin indicate renal stress. The alpha-1 microglobulin–IgA complex may exert anti-inflammatory effects. Complement component 2, an initiator of the complement cascade, has not been previously reported to be associated with heat stress.
Conclusions
The findings suggest that these proteins may serve as blood biomarkers to assess heatstroke severity and monitor recovery. Their clinical application could improve early detection of organ damage and guide intervention strategies.
Plain language summary
Heatstroke is becoming more common due to rising global temperatures. It can cause serious damage to organs such as the kidneys, but doctors often struggle to predict how well someone will recover. We looked at blood samples from people with heatstroke occurring during hot conditions, rather than that caused by strenuous physical activity, to find proteins that change during heatstroke and recovery. We found five specific proteins that may show whether a patient is recovering or still at risk of organ damage. These proteins could serve as early warning signals in the blood, helping doctors to respond sooner and more effectively. This research could lead to a simple blood test that could help monitor patients with heatstroke, making treatment safer and more personalized in the future.
Similar content being viewed by others

Introduction
Global warming, as one of the main factors that causes environmental deterioration, is also threatening the health of the human population worldwide. Thereinto, heatstroke is the most hazardous condition directly contributing to its morbidity and severity1. Classic (non-exertional) heatstroke (CHS) and exertional heatstroke (EHS) are two primary types of heatstroke. CHS results from prolonged exposure to high temperatures, posing significant risks, especially for vulnerable populations like the elderly and those with pre-existing health conditions, including acute or chronic illnesses. On the other hand, EHS, linked to strenuous physical activity in hot conditions, occurs rapidly, primarily affecting young and healthy individuals, notably athletes2,3. In recent years, the incidence of heatstroke has escalated globally, particularly posing a significant threat to teenagers and manual labourers such as farmers and firefighters. EHS is becoming increasingly prevalent among young and physically active individuals4,5, while CHS continues to present significant risks across a broader demographic, including teenagers and manual laborers6. Thus, the rising number of CHS heatstroke cases calls for heightened attention from the medical community.
Heatstroke symptoms include high core body temperature, altered mental status, rapid pulse, muscle cramps, nausea, vomiting, and, in severe cases, loss of consciousness. Diagnosis is typically based on a rapid increase in core body temperature above 40 °C (104 °F) and evaluating central nervous system (CNS) dysfunction7. While heatstroke causes thermoregulatory failure, dehydration, and electrolyte imbalance, it can progress to systemic inflammation, coagulopathy, and eventually lead to CNS lesions and multiorgan damage8,9,10. Among the consequences of heatstroke, the most affected organ is often the brain, with over 70% of patients experiencing lasting cerebellar damage affecting balance and coordination9,11. Besides, renal lesions are also critical, with acute kidney injury (AKI) developing in about one-third of cases. This can further lead to chronic renal damage, multiorgan complications, and high mortality12,13. Other complications include life-threatening conditions like acute respiratory distress syndrome, disseminated intravascular coagulation (DIC), hepatic injury, hypoglycemia, rhabdomyolysis, and seizures14,15,16. Currently, the long-term sequelae of heatstroke in young people are also particularly concerning. The emerging understanding of long-term sequelae, including neurological17, cardiovascular, renal18, immune, and metabolic dysfunction19, highlights the importance of prevention, prompt treatment, and ongoing monitoring for young heatstroke survivors.
Prompt and effective treatment is essential to reduce the severity and likelihood of post-heatstroke complications. Managing heatstroke prioritizes protecting the airway, breathing, and circulation, with rapid whole-body cooling as the primary treatment. Proper rehydration without overcorrecting sodium levels would follow. Even after primary treatment, continual monitoring, early detection and appropriate management of post-heatstroke conditions are crucial for improving outcomes in heatstroke-induced damage such as systemic inflammatory responses (SIRS)20, multi-organ dysfunction, acute kidney injury, etc. depending on the patient’s condition, a supplementary assessment of organ injury may be conducted, and anti-inflammatory and anticoagulant drugs may be administered10,21. Medications like Dantrolene and high-dose benzodiazepines may also help manage acute symptoms, though further research is needed10,22. Nevertheless, limited early detection and intervention strategies for post-heatstroke organ damage and its progression remain major obstacles. Moreover, predicting the impact of heatstroke is further complicated in elderly individuals and those with pre-existing health conditions such as cardiovascular diseases, diabetes and chronic neurological diseases23,24.
Therefore, understanding the mechanisms underlying heatstroke conditions and identifying molecular targets for early risk evaluation and timely therapy in post-heatstroke conditions is essential. Proteomics, a powerful tool for investigating disease-protein relationships through studying protein expression, structure, function, interactions, and modifications, has been pivotal in heatstroke research. Past biomarker studies, primarily using rodent models, focused on organ-specific damage, due to its complexity, often resemble those in infectious and inflammatory diseases like sepsis25,26,27. For instance, high mobility group box 1 (HMGB1), a key player in sepsis-related organ failure, was first identified in EHS patients and later validated in rat models as a marker for heatstroke-induced liver injury28,29. Key neuroinflammatory proteins, including IL-1β30, hippocalcin (HPAC)31, argininosuccinate synthetase (ASS1), HMGB2, and vimentin32, regulate heatstroke-induced neuroinflammation and hypothalamic effects. Meanwhile, various inflammation-related enzymes, glycoproteins, and TNF-related factors play a role in EHS-induced AKI33. Besides, well-known apoptosis regulators, including aquaporin 4 (AQP4), caspases, and Bcl-2 family members, mediate heatstroke-related cell death34,35. Clinical studies commonly employ immunoassays and clinical tests to illustrate the correlation between inflammation, coagulation, and heatstroke. Cytokines (TNFα, IL-6, IL-2R, IL-4) and chemokines (IL-8) indicate multi-organ dysfunction and resistance to cooling therapies36, and coagulation-related proteins (thrombomodulin-α, antithrombin III) drive fibrinolysis and late-stage organ failure37,38. Moreover, common clinical indicators like D-dimer and fibrinogen degradation products (FDP) are also closely linked to AKI and its life-threatening complication of rhabdomyolysis (RM) in heatstroke39,40. Typically, myoglobin release from muscle during inflammation and coagulopathy is also able to predict renal damage with a long-term tracking capability26. Additionally, low albumin levels have been proposed as a predictor of heatstroke patients’ risk for DIC41. One study, closely related to ours, examined serum exosome proteomics and highlighted differences between mild and severe heatstroke patients, linking them to acute phase reactions42. Unsurprisingly, numerous biomarkers observed that indicate heatstroke may overlap with those of other inflammatory and organ failure diseases. Hence, to address current deficiencies, an optimized biomarker panel, aligning with clinical evaluation criteria, is crucial in predicting the onset of heatstroke-induced organ damage and aiding more targeted treatment decisions while effectively tracking heatstroke severity. Inspired by past studies, our study shifts the focus toward long-term physiological adaptations, emphasizing the need for markers that reflect recovery and help track heatstroke severity.
This study used two-dimensional gel electrophoresis (2-DE) proteomics to investigate early-stage heatstroke-induced organ complications. Unlike bottom-up proteomics, 2-DE analyzes intact proteins, detecting isoforms and post-translational modifications (PTMs) that mass spectrometry alone may miss43. Despite its potential, 2-DE is rarely applied to heatstroke research due to challenges in obtaining reproducible, high-resolution images. With recent advancements in our lab’s 2-DE protocol44, its application in studying clinical diseases has become significantly more feasible25,45. To the best of our knowledge, this study presents the first application of 2-DE in investigating heatstroke in humans. The plasma proteome of heatstroke patients is examined at heatstroke diagnosis and during recovery to identify potential biomarkers and molecular targets for early therapeutic interventions. It is aimed at addressing the need for long-term tracking of post-heatstroke conditions.
In this study, we report a five-protein biomarker panel: alpha-1 antitrypsin (A1AT), alpha-1 microglobulin/bikunin precursor (AMBP/A1M), apolipoprotein A-IV (APOA4), clusterin, and complement component 2 (C2), which reflects condition improvement and potential renal stress following heatstroke. Notably, C2 has not previously been linked to heat stress. Moreover, the coexistence of A1M with its IgA-bound form suggests anti-inflammatory potential. These proteins are associated with two key pathways: the complement and coagulation cascade and lipid metabolism. The findings from this research are expected to contribute significantly to the management of individuals recovering from heatstroke, potentially leading to improved patient outcomes.
Methods
Sample collection
Plasma samples (n = 12) from six clinically diagnosed classic heatstroke (CHS) patients were collected at Juntendo University Hospital in 2020. Patients suspected of heat-related injury were included in the study if their serum creatinine levels exceeded 1.0 mg/dL and they had no prior history of chronic renal failure (CRF). All patients who met the inclusion criteria during the study period were male. Patient selection was consecutive and not based on sex. Next, acute kidney injury (AKI) was diagnosed when the estimated glomerular filtration rate based on cystatin C (eGFRcys) was below 60 mL/min/1.73 m2. Recovery was defined as the normalization of abnormal laboratory findings (e.g., serum creatinine and urine volume) and clinical symptoms. Twelve plasma samples were collected from six patients at two distinct time points: upon diagnosis (at patient presentation to the emergency room) and during recovery, typically 4–7 days post-diagnosis (Table 1). The plasma samples were transported in liquid nitrogen, then aliquoted and stored at −80 °C until proteomic analysis. The sample processing thereafter was conducted in a randomized order to mitigate the influence of the batch effect. This study was approved by the ethical committee of Tokyo Institute of Technology under the approval number 2022291, and written informed consent from all human subjects attending was also acquired.
Sample size justification
This exploratory proteomics study aimed to identify previously unreported biomarkers linked to recovery from heatstroke. Six patients were enrolled, with paired plasma samples collected at diagnosis and recovery to reduce interindividual variability and better capture changes over time. This pilot study represents, to the best of our knowledge, the first use of two-dimensional electrophoresis (2-DE) in human heatstroke research. The sample size aligns with typical preliminary proteomics research, which often includes 5–10 samples per group. The findings will help estimate effect sizes and variability, guiding statistical planning for future larger studies. Therefore, the current sample size is suitable for the discovery phase and lays the groundwork for later validation.
Pre-treatment of plasma samples
The 2-DE analysis procedure was optimized in our lab for blood samples and successfully applied in previous studies, specifically designed to identify and analyze low-abundance proteins in clinical samples25. To prepare plasma samples for 2-DE, a pre-treatment step to remove major proteins and impurities is performed. Each plasma aliquot following the randomized treatment order was removed from −80°C storage and thawed on ice. Fifty microliters of aliquots of human plasma were used for each experiment. The samples were then diluted with Buffer A (Agilent) and filtered through a 0.45 μm Cellulose Acetate Costar-SpinX centrifuge tube filter (Sigma-Aldrich, CLS8163). Each plasma sample was treated with Aurum Serum Protein Mini Kit (Bio-Rad) twice to effectively deplete albumin and IgG. Then, the Multiple Affinity Removal Spin Cartridge Human-14 (Agilent) was utilized to enhance the enrichment of lower-abundance proteins. This cartridge works by depleting 14 highly abundant proteins from the sample, including albumin, IgG, IgA, IgM, transferrin, haptoglobin, antitrypsin, fibrinogen, α2-macroglobulin, α1-acid glycoprotein, apolipoproteins, apolipoprotein A-I, apolipoprotein A-II, complement C3 and transthyretin. The resulting elution samples were then concentrated through a Viviaspin concentrator (2-3k, Cytiva) and further desalted and purified by using a 2-D Clean-Up Kit (Cytiva). Finally, the protein pellets were dissolved in the Destreak rehydration solution (Cytiva) before 2-DE.
Protein separation by two-dimensional electrophoresis (2-DE)
To ensure equal amounts of protein samples were loaded onto 2-DE, a 2-D Quant Kit (Cytiva) was used for calibration curve-based quantification. Additionally, the wavelength was measured using a UV–VIS spectrophotometer (UV-1280, Shimadzu), and the concentration was calculated based on the calibration curve conducted using gradient bovine serum albumin (BSA) concentrations. In total, 15 µg of each patient’s protein sample was applied for 2-DE. Briefly, Immobiline DryStrips (7 cm, pH 3-10 NL, Cytiva) were rehydrated at room temperature for at least 16 hours with the samples. The first-dimension separation of isoelectric focusing was conducted on the Ettan IPGphor 3 IEF System (Cytiva), in four steps: (i) 0–300 V, 1 h; (ii) 300—1000 V, 30 min; (iii) 1000–5000 V, 1.5 h, and (iv) 5000 V, 36 min. The strips were then incubated with dithiothreitol (DTT) and iodoacetamide (IAA) for reduction and alkylation. For the second-dimension separation, NuPAGE 4–12% Bis–Tris Z00m Gel (Thermo Fisher Scientific) was used. The electrophoresis was run at 200 V, 2.0 A, and 300 W for around 45 ± 5 min before the gels were stained with SYPRO Ruby Protein Gel Stain (Thermo Fisher Scientific), and stored in ultrapure water at 4 °C.
To visualize the protein spots on the gels, an image scanner Typhoon FLA 9500 (GE Healthcare) was used. Finally, the scanned images were analyzed by MelanieTM 2D gel analysis software (Version 9.0, SIB Swiss Institute of Bioinformatics).
Statistical analysis
All spots and in all gels were aligned and analyzed using Melanie 9.0, with parameters set at a minimum matching rate of 75% (Smooth = 3, Saliency = 47.7, Min Area = 29). The percentage volume (%vol) of each spot was obtained and used for statistical analysis. All statistical analysis was performed using R Studio (Version 2024.04.1 + 748). The raw spots %vol were first log-transformed to account for non-normality in the data before subsequent analysis. In particular, paired t-tests were performed on the results of six patients. The volcano plot was conducted based on the original percentage volume fold change and minus log 10 of the p-values. T-values from the test models were also obtained, and the local false discovery rate (lFDR) was applied for multiple testing corrections to verify significant differences between groups. The validation volcano plot was conducted based on the original percentage volume fold change and minus log 10 of the lFDR corrected p-values. The significance screening was conducted based on a threshold of p-value < 0.05, along with fold change > 0.5 and <−0.5; while the validation plot used the lFDR <0.2 for all protein spots observed. Box plots were subsequently created for each significant protein spot to visualize the changes between/among groups.
Trypsin digestion
After screening out the protein spots of interest, Melanie software was used to locate and confirm the target spots’ positions. Then, an automatic spot picker, EttanTM Spot Picker (Cytiva), was used to excise the gel spots. The gel fractions were stored in ultrapure water at 4 °C until trypsin digestion.
Excised gel fractions underwent in-gel trypsin digestion according to the procedure reported previously45. Briefly, gel pieces were first transferred into ProteoSave® SS 1.5 mL microtubes (MS-4215M, Sumitomo Bakelite) and incubated in ABC/ACN solution (200 mM ammonium bicarbonate, ABC [NH4HCO3, pH 8.1], 50% acetonitrile, ACN) for 15 min at room temperature. Afterwards, the solution was substituted with a reduction reagent (25 mM ABC [pH 8.1], 100 mM DTT), and kept at 60 °C for 30 min. Then, an alkylation reagent (25 mM ABC [pH 8.1], 100 mM IAA) was also applied to the gel pieces and incubated in the dark for 30 min at room temperature. After washing the gel pieces with 25 mM ABC at room temperature for 5 min, the gel fractions were dehydrated using 100% ACN and desiccated before the addition of trypsin solution. To prepare the trypsin solution, Trypsin Gold (Promega) was used at a concentration of 20 μg/mL in a solution containing 0.2 mM HCl, 40 mM ABC (pH 8.1), 5 mM CaCl2, and 10% ACN. The solution was then added to the gel fraction and incubated at room temperature for 5 min. The trypsin supernatant was then removed and replaced with the same dissolving solution without trypsin. The mixture was incubated overnight at 37 °C. On the second day, trypsin-digested gel fractions were sequentially processed rinse using ultrapure water (Wako Pure Chemical Industries), 0.1% trifluoroacetic acid (TFA) in 60% ACN, 0.1% TFA in 80% ACN, and 0.1% TFA in 100% ACN to extract all peptide and protein products. The resultant samples were concentrated to a reduced volume using an evaporator (Convenience store evaporator C10 light, Biochromato), followed by the use of C18-tips (SPE C-TIP T300 C18 type, 10 µL tip, Nikkyo Technos) to eliminate excess salts. Subsequently, all protein samples were desiccated and reconstituted in 0.1% TFA and 2% ACN in ultrapure water in preparation for liquid chromatography–tandem mass spectrometry (LC–MS/MS) detection.
Protein identification
The following LC–MS/MS procedure was performed at the National Institute for Materials Science (NIMS, Tsukuba, Japan) using a Benchtop Quadrupole-Orbitrap Mass Spectrometer (Thermo Scientific Q Exactive MS system) with NIMS Proteome Discoverer 2.4 (Thermo Fisher) for analysis. The in-gel digested samples were injected into the inlet system equipped with a C18 column (100 µm diameter × 150 mm length, packed with 3 µm C18 particles). The separation process utilized a gradient mobile phase, comprising mobile phase A (0.1% trifluoroacetic acid in distilled water) and mobile phase B (100% acetonitrile), with a gradient ranging from 5% to 45%. The column temperature was maintained at 35 °C, and the flow rate was set at 500 nL/min for a duration of 20 min per sample. Following the liquid chromatography separation, the samples underwent ionization through electrospray ionization (ESI) before being directed to the mass spectrometer for mass measurements.
LC–MS/MS-acquired data were processed using MASCOT (Version 2.5.1, Matrix Science, United Kingdom) against the Swiss-Prot database (SwissProt 2023_01) with trypsin as the digestion enzyme. The specified parameters included a precursor ion mass range of 350–5000 m/z, a fragment tolerance of 0.02 Da, and a precursor mass tolerance of 10.0 PPM. Two missed cleavage sites were allowed, and carbamidomethylation of Cys residues was set as a fixed modification, while Met oxidation was considered a variable modification. Identified proteins underwent filtering to achieve a false discovery rate (FDR) of 0.01. Further refinement excluded keratin proteins as potential contaminants. The protein annotation with the highest ranking of MASCOT score, along with its matching molecular weight and isoelectric point as observed on the 2-DE images, was determined and subjected to verification and network analysis.
Western Blotting verification
To validate the identified target protein biomarkers in this study, Western Blotting (WB) was conducted. At least three patient samples were selected randomly to be used to verify the target proteins of interest. The use of positive control for normalization is omitted in this experiment. This is because the commonly used positive control for blood sample-based WB experiments, transferrin, could be altered due to inflammation46, which could compromise its utility. Although no normalization was applied, the same total protein amount was loaded based on accurate quantification for each experimental batch.
Plasma samples were first diluted 20-fold in Buffer A (Agilent), and the concentration was determined using the 2D-Quant Kit. Then, protein samples were separated on either 7.5/12.5% sodium dodecyl sulfate-polyacrylamide gel (SDS-PAGE), with 10–20 μg of protein per sample. Then, the prepared samples were dissolved in 5× sample buffer (0.05% bromphenol blue, 10% glycerol, 10 mM DTT, 10% SDS and dissolved in 0.25 M Tris-HCl [pH 6.8]) in a 4:1 fold (sample volume: 5× sample buffer volume) and heated at 95 °C to denature for 5 min. Precision Plus ProteinTM WesternCTM Standards (Bio-Rad) were used as a protein standard.
Separated proteins were then transferred to a polyvinylidene difluoride (PVDF) membrane at 200 V, 0.12 A for an hour at room temperature using an SD Semi-Dry Electrophoretic Transfer Cell (Bio-Rad, Trans-Blot®). The blot was then probed for the proteins of interest. All primary antibodies were validated according to the manufacturers’ datasheets and used for detection in human plasma samples. The antibodies and their respective working dilutions are as follows: Anti-alpha1-antitrypsin antibody (ab207303, Abcam) was used at a 1:5000 dilution [datasheet: https://www.abcam.co.jp/products/primary-antibodies/alpha-1-antitrypsin-antibody-epr17087-50-ab207303.pdf]; Anti-alpha1 microglobulin (protein AMBP/A1M) antibody (PA5-119665, Invitrogen) was used at a 1:1000 dilution [datasheet: https://www.thermofisher.com/order/genome-database/dataSheetPdf?producttype=antibody&productsubtype=antibody_primary&productId=PA5-119665&version=Local]; Anti-apolipoprotein A-IV antibody (MA5-31355, Invitrogen) was used at a 1:700 dilution [datasheet: https://www.thermofisher.com/order/genome-database/dataSheetPdf?producttype=antibody&productsubtype=antibody_primary&productId=MA5-31355&version=Local]; Anti-complement component 2 (C2) antibody (ab209900, Abcam) and anti-apolipoprotein J (clusterin) antibody (PA5-86452, Invitrogen) were each used at a 1:1000 dilution [C2 datasheet: https://www.abcam.co.jp/products/primary-antibodies/c2-antibody-epr17979-ab209900.pdf; Clusterin datasheet: https://www.thermofisher.com/order/genome-database/dataSheetPdf?producttype=antibody&productsubtype=antibody_primary&productId=PA5-86452&version=Local]. A blocking buffer consisting of 5% skim milk (Fujifilm) in TBS-T (0.1% Tween-20) was used for antibody dilution and membrane blocking. All dilutions followed the manufacturer’s recommendations unless otherwise specified. This blocking buffer was also used for pre-blocking for 1 h before overnight primary antibody incubation at 4 °C. Secondary antibody staining was then performed using HRP Goat Anti-Rabbit IgG (65-6120, Invitrogen) (for clusterin), Anti-IgG (H + L chain) Rabbit pAb-HRP (485, MBL) (for A1AT and protein AMBP/A1M), HRP Goat Anti-Mouse IgG (H&L) (ab205719, Abcam) (for APOA4), and Goat Anti-Rabbit IgG H&L (HRP) (ab6721, Abcam) (for C2) for an hour at room temperature. The blots were washed three times using 1× TBS-T. Detection of protein bands was done using Merck Immobilon Western Chemiluminescent HRP substrate (Fisher Scientific). The blot was visualized using the LuminoShotTM 400Jr system (Takara) under an exposure time of 5 min, and the expression intensity of the bands was analyzed and compared using ImageJ. The mean percentage change of all five target proteins was calculated as the recovery-to-diagnosis ratio, with diagnosis (D) set at 100%. This standardization enables a clear comparison of protein level fluctuations.
2-DE Western Blotting verification
One of the protein spots of interest observed in 2-DE initially appeared to have a high molecular weight. However, LC–MS/MS identification revealed it as the low molecular weight AMBP protein/A1M (Table 2). This observation has led to the hypothesis that protein AMBP/A1M may also exist in complex molecular forms of A1M-IgA. To further confirm the existence of the A1M-IgA complex and A1M (protein AMBP) co-expression, as well as their regulation of expression levels from the heatstroke condition to recovery, 2-DE-based WB was conducted on randomly selected patient no.4. The procedure for conducting 2-DE was the same as previously described, except that the step to deplete major proteins using affinity columns was omitted. After electrophoresis, proteins on the 2-DE gel were subjected to WB using the same procedure as before. The primary antibody used was anti-α-1 microglobulin at a 1:1000 dilution, followed by its corresponding secondary antibody as previously used. The blot was then visualized via LuminoShotTM 400Jr system, and the expression of each protein spot was analyzed using Melanie 9.0.
Protein network
STRING database (https://string-db.org) was used to generate a protein-protein interaction network for the significant proteins identified in this study. Accession numbers from UniProt were used as input. The interaction maintained a default confidence level at a score of 0.4, while the 3D protein structures were incorporated into the bubble-like nodes. The identified proteins were also classified using PANTHER (Version 18.0, https://www.pantherdb.org) to classify proteins according to their biological processes, cellular components, and possible pathways (unclassified were filtered). The biological processes of the target proteins involved were represented in a pie chart created using Microsoft Excel.
Statistics and reproducibility
All statistical analyses were performed using R Studio (Version 2024.04.1 + 748), as detailed in the “Statistical analysis” section above. Briefly, paired t-tests were applied to log-transformed 2-DE protein spot intensities from six matched patient samples (n = 6 pairs). Effect sizes were calculated using Cohen’s dz, with 95% confidence intervals estimated via the noncentral t-distribution. Multiple testing correction was performed using the local false discovery rate (lFDR), and significance thresholds were defined by both p-value and fold change criteria. Biological replicates were defined as independent patient plasma samples. A total of 12 samples (6 diagnosis, 6 recovery) were analyzed by 2-DE, with one gel performed per sample. Protein spots of interest were picked across multiple gels for LC–MS/MS identification. Western blotting was conducted on at least three independent patient samples per target protein for replication purposes. Although normalization controls were omitted due to variability in transferrin under inflammatory conditions, total protein loading was equalized using precise quantification. All procedures followed standardized protocols, and no samples or data points were excluded. All replicates are reported.
Results
Five proteins reflecting recovery conditional changes from heatstroke
A total of 12 plasma samples, comprising diagnosis (D) and recovery (R) groups from six heatstroke patients, were subjected to 2-DE analysis (Fig. 1). A total of 359 spots were detected using Melanie software. To determine protein spots that changed significantly between the diagnosis and recovery groups, each spot’s %vol was analyzed using a paired t-test. In the screening criteria using p-value < 0.05 and a fold change greater than 0.5 or less than −0.5, five protein spots (no. 2 [p = 0.01296], no. 109 [p = 0.00259], no. 183 [p = 0.0110], no. 220 [p = 0.00540] & no. 237 [p = 0.04518]) were identified as significantly different between the two groups (Fig. 2a, Supplementary Fig. 1). When local false discovery rate correction was applied, four of these spots (no. 2 [lFDR = 0.0635], no. 109 [lFDR = 0.0001399], no. 183 [lFDR = 0.03982], no. 220 [lFDR = 0.0564611]) remained significant (lFDR < 0.1), while spot no. 237 has been excluded (Supplementary Fig. 2). While lFDR adjustment accounts for multiple comparisons, reducing the likelihood of false positives, spot no. 237 was still included in the subsequent analysis. To confirm its relevance, the trend changes for spot 237 were later validated using WB to verify its significance. Figure 2b shows the position of these five proteins on the 2-DE image, where they are dispersed, suggesting they are different proteins. Results of LC–MS/MS (Table 2 and Supplemental Data 1) revealed that these five protein spots as alpha-1-antitrypsin (A1AT, spot no. 183, P01009) and protein AMBP/A1M (no. 2, P02760); apolipoprotein A-IV (APOA4, no. 220, P06727), complement component 2 (C2, no. 109, P06681), and clusterin (no. 237, P10909).

a The 12 images from human plasma samples were categorized into two groups: diagnosis (D) and recovery (R). b The gel image of 46-D1 illustrates the molecular weight of the marker (10–220 kDa) and pI range (3–10). Complete original gel images are available in Supplementary Data 3.

a Main volcano plot of D against R with a minimum threshold of p < 0.05, fold-change range except [−0.5,0.5]. b The distribution of screened-out significant spots on the gel. The gel image presents 56-D6 with 359 spots matched and squared. The significant spots were squared in green with spot ID labelled aside. c Box plots for all up-regulated and down-regulated spots of interest. On the x-axis, the label D refers to the diagnosed group, and R refers to the recovery group. D and R were paired with the same patient in color lines. Significance levels were marked between groups on the plots. * lFDR < 0.05; **lFDR < 0.005, *** lFDR < 0.0005.
Among these five proteins, three showed increased expression (spot no. 109, no. 220 & no. 237), while two showed decreased expression (spot no. 2 & no. 183) during recovery compared to diagnosis (Fig. 2c). The intensities of significant spots in patient samples were compared in 3D to visualize differences by Melanie 9.0 (Supplementary Fig. 3). Five noteworthy protein spots in patient plasma were identified and annotated through database matching (Table 2 and Supplemental Data 1). The five annotated proteins from patient plasma include two that were down-regulated: alpha-1-antitrypsin (A1AT) and protein AMBP/A1M; and three up-regulated proteins: apolipoprotein A-IV (APOA4), complement component 2 (C2), and clusterin (also known as apolipoprotein J).
Western Blotting analysis involved five protein targets, where their changes are verified as consistent with the results of 2-DE. This includes two down-regulated proteins, A1AT and protein AMBP/A1M, as well as two upregulated proteins, clusterin, APOA4 and C2 (Fig. 3). Based on the quantitative intensity comparison results, individual variability was observed in all tests, even though this observation may be attributed to variations in experimental batches and/or inconsistencies in sample preparation (Fig. 3f). Intriguingly, the fold-change tends to resemble among patients in two upregulated proteins, A1AT and protein AMBP/A1M (Fig. 3a, b, f), despite the presence of high variability in individuals. For C2, the regulation trend could be validated in three out of four randomly selected patient samples across time points (Fig. 3e), with the sample from patient no. 5 showing an inverse trend to that of 2-DE. This phenomenon may be due to possible PTMs of the C2 protein itself in this patient. WB measures the whole protein of C2, whereas the C2 spot on 2-DE represents a specific proteoform of C2. However, it is also possible that additional factors, such as sample handling, contribute to this discrepancy, and thus further investigation is needed.

a Alpha-1 antitrypsin (A1AT). b Protein AMBP/A1M. c Clusterin. The primary antibody binds to the alpha chain of clusterin. d Apolipoprotein A-IV (APOA4). e Complement component 2. From a–d, each lane was loaded with 10 µg of patient plasma and separated on a 12.5% SDS-PAGE. For e a 20 µg plasma sample was used per lane, separated on a 7.5% SDS-PAGE. Modification was done for C2 for enhanced separation and transfer efficiency of high molecular weight proteins. f Mean percentage change of five target proteins (relative to D-Diagnosis as 100%). The mean percentage change for all five target proteins was calculated using the ratio R/D (Recovery/Diagnosis), where D is set as the reference at 100%. The error bars represent the standard error, with larger values indicating greater individual variability in the alterations of a specific protein. The full Western blot images can be found in Supplementary Figs. 4–8.
Protein AMBP/A1M exhibits multifaceted downregulation following recovery
One of the significantly down-regulated protein spots was identified as protein AMBP (spot no. 2). This spot is positioned at a higher molecular weight location on the 2-DE gel image (>200 kD) (Fig. 2b). However, in the result of LC-MS/MS, the theoretical molecular weight was 39 kD (Table 2). Upon WB validation using anti-α-1 microglobulin antibody, the band corresponding to this theoretical molecular weight of AMBP (approximately 34 kDa) also displayed a downregulation. The band corresponding to a molecular weight of more than 200kDa, as seen on 2-DE, was not detected (Supplementary Fig. 5). This is thought to be due to the reduced transfer efficiency in conventional WB for proteins with higher molecular weight.
Hence, in order to effectively track and confirm the changes in the high molecular states of protein AMBP/A1M, instead of WB following SDS-PAGE, protein samples were separated via 2-DE, following WB (2-DE-WB). In the results of 2-DE WB (Fig. 4a and Supplementary Fig. 9), spots in three regions were detected (250, 130, and 34 kDa). The detection of both spots around 250 kDa and 34 kDa may indicate the co-expression of protein AMBP/A1M high molecular states as A1M-IgA complex and A1M monomeric states. Furthermore, their expression levels were observed to be downregulated collectively from the heatstroke condition to recovery (Fig. 4b). A novel finding regarding post-translational modifications (PTMs) of A1M monomeric states revealed multiple independent spots exhibiting varied regulatory changes. Because the PTMs of A1M spots showed significant changes in isoelectric point (pI) without noticeable differences in molecular weight, it is hypothesized that phosphorylation may occur in the monomeric states of A1M. Among these, three spots were identified: two downregulated and one showing clear upregulation. However, the overall trend of A1M spot integrity changes remained consistent with a down-regulation trend. Further investigation into the post-translational modification changes of A1M and confirmation of this phenomenon’s reproducibility in other patients are both required.

a 2-DE-WB results presented multiple target bands. b The column plot indicated the volume comparison among all observed spots on the gel image. Patient No. 4 was selected at random for comparison, where all discernible spots exhibiting significant binding signals were assessed. Among all spots, the monocular states of A1M (~34 kD) were represented by multiple independent spots, visualized in 3D form generated using MelanieTM software. Colored arrows on the bar chart indicate the trend of regulation based on volume changes observed from diagnosis to recovery states. Each sample was treated with 15 µg of protein after undergoing a clean-up step. Complete original gel images are available in Supplementary Fig. 9.
The protein network shows protein relations and two pathways that might regulate heatstroke
To further understand the protein–protein interactions of the five observed proteins and to elucidate the pathophysiology of heatstroke progression from diagnosis to recovery, protein network analysis was conducted using STRING. This is based on a database containing the latest published results of the co-expression relationships and high co-mention frequency for each protein. The interactions between five proteins are shown in Fig. 5a. The five target proteins are linked by six edges, displaying an average node degree of 2.4. C2 was clustered separately from the other four proteins. The average local clustering coefficient was 0.8, with a PPI enrichment p-value of 1.56e − 07, indicating the network has significantly more interactions than expected by chance. More specifically, this suggests that the protein clusters formed by A1AT, APOA4, clusterin, and protein AMBP/A1M are biologically connected to each other as a group and have more interactions among themselves than a random set of proteins of the same size and degree distribution drawn from the genome. Distinctively, the co-expression relationship has been found in both A1AT and protein AMBP/A1M to all three other proteins, excluding C2. Thus, C2 may play an independent previously unreported function in directing disease recovery apart from the cluster of A1AT, protein AMBP/A1M, APOA4, and clusterin. Next, through GO term analysis utilizing both PANTHER and STRING, it can be generalized that the five target proteins primarily participate in regulatory processes (Fig. 5c and Supplementary Table 2). The shared theme among these functional terms pertains to their involvement in cellular secretory and transport processes, as well as their contribution to structural and communication functions within and between cells. These proteins collectively play pivotal roles in preserving the integrity and functionality of cells and tissues.

The varying thickness of lines connecting protein nodes signifies the strength of data support for the respective protein–protein interactions. a Protein network derived from the annotation of five identified proteins. b Expanded network incorporating target proteins and their predicted functional partners. c Pie chart illustrating biological processes based on GO-terms, generated from the annotation of the initial five target proteins.
Subsequently, in order to explore the potential pathways associated with the target proteins, the K-means clustering function was employed on the existing five target protein nodes using the default parameter of three clusters (Fig. 5b). This function enables incorporating additional nodes representing predicted functional partners into the network. The resulting network graphic comprises ten nodes connected by 31 edges, exhibiting an average node degree of 6.2 (with an average local clustering coefficient of 0.932). All additional predicted functional partner proteins were included based on a score exceeding 0.999. The KEGG pathway database matching initially identified the complement and coagulation cascades as the pathway for three out of five target proteins (C2, clusterin, and A1AT) (Supplementary Table 1). An additional pathway related to cholesterol metabolism was discovered based on the enrichment of connections, linking APOA4 to other apolipoprotein family members. These two pathways held the top two ranks in counts within the matched network list, suggesting a possible relationship with heatstroke progression.
Discussion
Global warming intensifies heatstroke, a serious health threat with potentially fatal consequences, especially for vulnerable populations such as the elderly, who face thermoregulatory challenges, and manual labourers, who are at risk from prolonged heat exposure. Regarding risk factors, although acute illness and dehydration are commonly associated with exertional heatstroke (EHS), they also significantly contribute to classic heatstroke (CHS), particularly in the elderly or those with chronic comorbidities due to impaired thermoregulation and reduced fluid intake47,48. Currently, younger individuals are also increasingly affected by heatstroke, drawing growing attention worldwide. Children and adolescents, in particular, are at higher risk due to their developing physiology, making them more vulnerable to heat-related illnesses5. Increased time spent outdoors, coupled with climate change and worsening air pollution, further elevates the exposure of vulnerable populations to extreme heat and respiratory issues4. Furthermore, the long-term sequelae of heatstroke in young people, such as neurological17, cardiovascular, renal18, immune, and metabolic dysfunction19, underscore the need for prevention, timely treatment, and sustained follow-up. Therefore, raising awareness about the condition and ensuring timely medical intervention are vital for reducing its impact3. From this study, a proteomics-based analysis of CHS patient plasma identified significant changes in five proteins from diagnosis to recovery, revealing both upregulation and downregulation patterns, providing insights into potential biomarkers for heatstroke recovery. Alpha-1 antitrypsin (A1AT) inhibits enzymes like elastase and trypsin, plays a role in tissue repair, and protects against enzymatic damage49. Though not directly linked to inflammation associated with heat stress, it is involved in immune regulation and anti-inflammatory processes in autoimmune and chronic diseases50,51. This study revealed a significant decrease in A1AT levels post-heatstroke, indicating reduced inflammation as protease activity and A1AT immune-modulating properties return to normal after recovery.
Protein AMBP, a precursor of A1M, plays a key role in antioxidant and tissue protection mechanisms, particularly in oxidative stress and inflammation52. Its anti-inflammatory effects and role in early-stage tissue damage have rendered it a widely studied potential biomarker53., especially in acute kidney injury (AKI)54,55. Meanwhile, the acute phase protein, A1M, has also been studied as a potential biomarker for AKI due to its ability to bind and neutralize free hemoglobin and heme, preventing early oxidative damage56. One study highlighted the downregulation of AMBP in kidney injury from EHS rat models, further underscoring its potential as a key biomarker for kidney injury33. Given its significant up-regulation in the early stages of AKI and down-regulation in the severe stages, the AMBP/A1M protein may serve as a marker for tracking the progression of AKI. While this study’s subjects showed no clinical signs of AKI, monitoring A1M levels may still be valuable, as significant changes can indicate a kidney condition with high efficiency. Apart from its monocular properties, A1M also forms complexes with IgA, influencing inflammation in various diseases57,58. In this study, both AMBP/A1M and A1M-IgA were downregulated during heatstroke recovery. 2-DE-WB confirmed their potential role in alleviating heatstroke, with A1M monomers appearing as multiple spots, indicating possible phosphorylation during recovery.
Apolipoprotein A-IV (APOA4) plays a crucial role in the regulation of lipid metabolism and transport, particularly in association with blood lipoprotein59. Early-stage elevation of APOA4 has been recognized in kidney-related diseases like chronic kidney disease (CKD) and diabetes for an extended period, making it a novel therapeutic target and early marker for renal injuries60,61. The current study appears to be the first to report APOA4 association with heatstroke, observing its upregulation post-recovery, suggesting heatstroke may trigger inflammation and abnormal fat metabolism, potentially impacting kidney health. Hence, APOA4 could serve as a biomarker for monitoring delayed kidney damage following heatstroke.
Clusterin, also known as apolipoprotein J, is a glycoprotein expressed in various tissues and bodily fluids62. It is typically known as a chaperone, regulating protein folding and preventing aggregation under stress, similar to heat shock proteins (HSPs)63,64. Clusterin’s protective role is seen in kidney tissue remodelling and in clearing misfolded proteins in hypoxic kidney cells65. When recovering from heat stress, the elevation of clusterin levels in the patient may indicate its involvement in averting protein aggregation and safeguarding the kidneys from heat stress. Hence, this observation also holds potential implications for evaluating the risks of subsequent kidney complications.
Complement component 2 (C2), as a vital part in the immune response, activates during the complement cascade to form the C3 convertase enzyme, with C2 deficiency linked to immunodeficiency66. Previous studies have established that complement cascade activation is a primary contributor to multiple organ dysfunction syndrome (MODS) in patients, not only in inflammatory diseases such as sepsis but also in heat-related illnesses67. While C2’s role is considered less crucial than C3 in inflammatory diseases and organ injuries68,69, this study found C2 significantly upregulated during heatstroke recovery, suggesting restored complement cascade activity and potential involvement in abnormal blood coagulation under stress.
Among the proteins described above, the co-expression of several proteins is also an intriguing aspect that deserves attention. The co-expression of A1AT, AMBP/A1M, and their interaction with proprotein convertase subtilisin/kexin-9 (PCSK9) in regulating plasma low-density lipoprotein (LDL) levels has been confirmed70, with a coordinated up-regulation observed in down syndrome (DS) fetuses71. This subsequent study reported trends opposite to those observed in our research, with A1AT and AMBP/A1M being downregulated, while clusterin was upregulated, suggesting that these markers may collectively track health conditions, specifically in the context of heatstroke recovery in our study. Furthermore, A1AT and APOA4 also showed inverse expression, as seen in ovarian cancer studies72, making A1AT, AMBP/A1M, clusterin, and APOA4 potential biomarkers for monitoring heatstroke recovery and assessing renal stress.
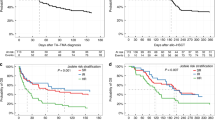
The present study also highlights the involvement of the complement and coagulation cascades in heatstroke, with C2 initiating complement activation, clusterin regulating membrane attack complex (MAC) inhibition, and A1AT influencing coagulation. Since heatstroke can lead to a systemic inflammatory response, the abnormal blood clotting involved in the activation of the blood coagulation pathway due to inflammatory signals is often plausible. These may further lead to multi-organ dysfunction and late-onset organ failure after heatstroke. In addition, kidneys, highly susceptible to heatstroke after the CNS, regulate cholesterol excretion, so dysfunction can impact cholesterol metabolism73. In CKD and heatstroke-induced AKI, lipid metabolism disruptions may lead to elevated cholesterol. The identification of APOA4 in this study suggests potential cholesterol metabolism abnormalities, offering insights into potential long-term kidney issues from heatstroke. Further investigation into cholesterol homeostasis in the kidney is essential, as heatstroke-induced abnormalities may exacerbate pathophysiological damage in renal tubules (e.g., proximal tubules74), where cholesterol is primarily handled. From an additional clinical perspective, retrospective evaluation of serum creatinine and eGFR revealed that five out of six patients met AKI criteria at diagnosis, yet standard markers indicated full recovery in three cases (Table 1). Interestingly, diverse clinical presentations and recovery patterns were observed, even in patients who did not meet AKI criteria or showed apparent recovery, sustained elevations of APOA4 and clusterin suggested ongoing renal stress at the proteomic level. This implies that heat stress-induced kidney injury or subclinical strain may persist beyond the resolution seen in conventional measures. Rather than contradicting existing clinical standards, our findings suggest that integrating multi-biomarker panels could complement routine assessments, offering a more nuanced and sensitive tool for long-term monitoring and potentially guiding protective strategies in the aftermath of heatstroke.
This study’s small sample size of six male patients with heatstroke highlights the need for larger-scale investigations, particularly those incorporating diverse populations varying in age, sex, and pre-existing conditions. Expanding the cohort and including comparative analyses between different types of heatstroke will help validate consistent protein alterations, such as AMBP/A1M and complement C2, across various forms of heat stress. Additionally, future studies should integrate a broader spectrum of clinical, biological, physical, and psychological parameters to refine early prediction models of organ damage, especially kidney injury, and to enhance the precision of individualized therapeutic strategies. These findings should also be interpreted with caution, as some protein changes may reflect subclinical stress rather than definitive evidence of injury or protection. Therefore, incorporating serial measurements and additional biomarkers, such as myoglobin, will be essential for better understanding renal responses during and after heatstroke. Exploring the synergistic roles of biomarkers involved in inflammation, oxidative stress, and kidney recovery will be critical in advancing knowledge of heatstroke pathophysiology. Ultimately, these efforts could support the development of predictive tools and long-term monitoring strategies to improve clinical outcomes in heatstroke management.
Conclusion
This study employed a 2-DE-based proteomics approach to identify multiple biomarkers from non-invasive plasma samples for potential post-heatstroke complications. These biomarkers are apolipoprotein A-IV (APOA4), complement component 2 (C2), clusterin, alpha-1 antitrypsin (A1AT) and protein AMBP/A1M. Several of these biomarkers suggested the involvement of complement and coagulation pathways, along with cholesterol metabolism, in the pathophysiology of heatstroke. Furthermore, utilizing a biomarker panel consisting of these five proteins could aid in monitoring inflammation recovery from heatstroke and assist in early-stage stress prediction for potential organ injuries, including those affecting the kidneys. Utilizing these biomarkers collectively, rather than individually, could potentially enhance the robustness of conditional tracking and the evaluation of post-heatstroke complications. This study has enhanced our understanding of heatstroke-induced progression, making it essential for improving patient outcomes and optimizing healthcare resources. Last but not least, this research is also expected to serve as a fundamental component of preventive medicine guidance and contribute significantly to overall public health and well-being.
Data availability
All data supporting the conclusions of this research are available as follows: Raw LC-MS/MS data: All raw mass spectrometry files (LC-MS/MS) are provided in the Supplementary data (Supplemental data 1.xlsx), in accordance with MIAPE (Minimum Information About a Proteomics Experiment) quality standards. The mass spectrometry proteomics data have been deposited to the ProteomeXchange Consortium via the PRIDE75 partner repository with the dataset identifier PXD054006 and 10.6019/PXD054006. 2-DE image analysis data: Raw 2D-gel images, as well as the numerical output exported from Melanie 9.0 used for quantification, are included in Supplementary data (Supplementary Data 2.xlsx and Supplementary Data 3.pdf) and meet MIAPE-Gel recommendations. Western blot (WB) data: All analyzed WB and 2DE-WB images, and quantified data are available in Supplementary data (Supplementary Information.pdf, Supplementary Data 2.xlsx). The original, unedited WB images are provided in Supplementary Figs. 4–8. The original gel images for the 2DE-WB experiments are included in Supplementary Fig. 9.
References
Vicedo-Cabrera, A. M. et al. The burden of heat-related mortality attributable to recent human-induced climate change. Nat. Clim. Change 11, 492–500 (2021).
Epstein, Y. & Yanovich, R. Heatstroke. N. Engl. J. Med. 380, 2449–2459 (2019).
Forsyth, N. & Solan, T. It’s getting hot in here: heat stroke in children and young people for paediatric clinicians. Paediatr. Child Health 32, 471–475 (2022).
Currie, J. & Deschênes, O. Children and climate change: introducing the issue. Future Child. 26, 3–9 (2016).
Anderko, L., Chalupka, S., Du, M. & Hauptman, M. Climate changes reproductive and children’s health: a review of risks, exposures, and impacts. Pediatr. Res. 87, 414–419 (2020).
Bouchama, A. et al. Classic and exertional heatstroke. Nat. Rev. Dis. Prim. 8, 8 (2022).
Cantrill, S. V. Chapter 79—Heat Stroke. In Critical Care Secrets (Fourth Edition) (eds Parsons, P. E. & Wiener-Kronish, J. P.) 501–505 (Mosby, Philadelphia, 2007).
Hemmelgarn, C. & Gannon, K. Heatstroke: thermoregulation, pathophysiology, and predisposing factors. Compend-. Contin. Educ. Vet. 35, E4 (2013).
Lawton, E. M., Pearce, H. & Gabb, G. M. Review article: Environmental heatstroke and long-term clinical neurological outcomes: a literature review of case reports and case series 2000-2016. Emerg. Med. Australas. 31, 163–173 (2019).
Morris, A. & Patel, G. Heat Stroke. In StatPearls (StatPearls Publishing Copyright © 2023, StatPearls Publishing LLC., Treasure Island (FL) ineligible companies. Disclosure: Gaurav Patel declares no relevant financial relationships with ineligible companies, 2023).
Miyamoto, K. et al. Heatstroke-induced late-onset neurological deficits in mice caused by white matter demyelination, Purkinje cell degeneration, and synaptic impairment in the cerebellum. Sci. Rep. 12, 10598 (2022).
Thongprayoon, C. et al. Impact of acute kidney injury on outcomes of hospitalizations for heat stroke in the United States. Diseases 8, 28 (2020).
Goto, H., Kinoshita, M. & Oshima, N. Heatstroke-induced acute kidney injury and the innate immune system. Front. Med. 10, 1250457 (2023).
Pease, S. et al. Early organ dysfunction course, cooling time and outcome in classic heatstroke. Intensive Care Med 35, 1454–1458 (2009).
Hifumi, T. et al. Prognostic significance of disseminated intravascular coagulation in patients with heat stroke in a nationwide registry. J. Crit. Care 44, 306–311 (2018).
Iba, T., Helms, J., Levi, M. & Levy, J. H. Inflammation, coagulation, and cellular injury in heat-induced shock. Inflamm. Res. 72, 463–473 (2023).
Yoneda, K. et al. How can heatstroke damage the brain? A mini review. Front. Neurosci. 18, 1437216 (2024).
Adnan Bukhari, H. A systematic review on outcomes of patients with heatstroke and heat exhaustion. Open Access Emerg. Med. 15, 343–354 (2023).
Kruijt, N. et al. Exertional heat stroke and Rhabdomyolysis: a medical record review and patient perspective on management and long-term symptoms. Sports Med. - Open 9, 33 (2023).
Zeller, L., Novack, V., Barski, L., Jotkowitz, A. & Almog, Y. Exertional heatstroke: clinical characteristics, diagnostic and therapeutic considerations. Eur. J. Intern. Med. 22, 296–299 (2011).
Asmara, I. G. Y. Diagnosis and management of heatstroke. Acta Med. Indones. 52, 90–97 (2020).
Hostler, D., Northington, W. E. & Callaway, C. W. High-dose diazepam facilitates core cooling during cold saline infusion in healthy volunteers. Appl. Physiol. Nutr. Metab. 34, 582–586 (2009).
Leon, L. R. & Bouchama, A. Heat stroke. Compr. Physiol. 5, 611–647 (2015).
Hopp, S., Dominici, F. & Bobb, J. F. Medical diagnoses of heat wave-related hospital admissions in older adults. Prev. Med. 110, 81–85 (2018).
Hayashi, N. et al. Multiple biomarkers of sepsis identified by novel time-lapse proteomics of patient serum. PLoS ONE 14, e0222403 (2019).
Iba, T., Connors, J. M., Levi, M. & Levy, J. H. Heatstroke-induced coagulopathy: biomarkers, mechanistic insights, and patient management. eClinicalMedicine 44, 101276 (2022).
Schlader, Z. J., Davis, M. S. & Bouchama, A. Biomarkers of heatstroke-induced organ injury and repair. Exp. Physiol. 107, 1159–1171 (2022).
Tong, H. S. et al. Early elevated HMGB1 level predicting the outcome in exertional heatstroke. J. Trauma 71, 808–814 (2011).
Tong, H. et al. HMGB1 activity inhibition alleviating liver injury in heatstroke. J. Trauma Acute Care Surg. 74, 801–807 (2013).
Zhang, Z. T. et al. NLRP3 ablation enhances tolerance in heat stroke pathology by inhibiting IL-1β-mediated neuroinflammation. J. Neuroinflamm. 18, 128 (2021).
Ji, J., Hong, X., Su, L. & Liu, Z. Proteomic identification of hippocalcin and its protective role in heatstroke-induced hypothalamic injury in mice. J. Cell Physiol. 234, 3775–3789 (2019).
Xv, F. et al. Quantitative proteomics provided insights into the protective effects of heat acclimation on the rat hypothalamus after exertional heatstroke. J. Integr. Neurosci. 23, 116 (2024).
Wen, F. L. et al. Proteomics analyses of acute kidney injury biomarkers in a rat exertional heat stroke model. Front. Physiol. 14, 1176998 (2023).
Chao, C. M. et al. Proteomic analysis of hypothalamic injury in heatstroke rats. Proteomics 15, 1921–1934 (2015).
Li, X. et al. Acquired heat acclimation in rats subjected to physical exercise under environmental heat stress alleviates brain injury caused by exertional heat stroke. Brain Res. 1811, 148393 (2023).
Broessner, G. et al. Case report: severe heat stroke with multiple organ dysfunction - a novel intravascular treatment approach. Crit. Care 9, R498–501 (2005).
Matsumoto, H. et al. Successful treatment for disseminated intravascular coagulation (DIC) corresponding to phenotype changes in a heat stroke patient. J. Intensive Care 7, 2 (2019).
Ohbe, H. et al. Treatment with antithrombin or thrombomodulin and mortality from heatstroke-induced disseminated intravascular coagulation: a nationwide observational study. Semin. Thromb. Hemost. 45, 760–766 (2019).
Wang, C. et al. Association of D-dimer and acute kidney injury associated with rhabdomyolysis in patients with exertional heatstroke: an over 10-year intensive care survey. Ren. Fail. 43, 1561–1568 (2021).
Iwaniec, J. et al. Acute phase response to exertional heat stroke in mice. Exp. Physiol. 106, 222–232 (2021).
Zeng, Q. et al. Nomogram for predicting disseminated intravascular coagulation in heatstroke patients: a 10 years retrospective study. Front. Med. ((Lausanne)) 10, 1150623 (2023).
Li, Y. et al. Proteomic profiling of serum exosomes reveals acute phase response and promotion of inflammatory and platelet activation pathways in patients with heat stroke. PeerJ. 11, e16590 (2023).
Tholey, A. & Becker, A. Top-down proteomics for the analysis of proteolytic events—methods, applications and perspectives. Biochim. Biophys. Acta Mol. Cell Res. 1864, 2191–2199 (2017).
Wong, S. Y., Hashim, O. H. & Hayashi, N. Development of high-performance two-dimensional gel electrophoresis for human hair shaft proteome. PLoS ONE 14, e0213947 (2019).
Wong, S. Y., Kato, S., Rodenburg, F., Tojo, A. & Hayashi, N. Longitudinal proteomics study of serum changes after allogeneic HSCT reveals potential markers of metabolic complications related to aGvHD. Sci. Rep. 12, 14002 (2022).
Claise, C. et al. Low transferrin levels predict heightened inflammation in patients with COVID-19: new insights. Int. J. Infect. Dis. 116, 74–79 (2022).
Subudhi, A. W., Askew, E. W. & Luetkemeier, M. J. DEHYDRATION. In Encyclopedia of Human Nutrition (Second Edition) (ed Caballero, B.) 518-526 (Elsevier, Oxford, 2005).
Patel, J. et al. Critical illness aspects of heatstroke: a hot topic. J. Intensive Care Soc. 24, 206–214 (2023).
Lechowicz, U., Rudzinski, S., Jezela-Stanek, A., Janciauskiene, S. & Chorostowska-Wynimko, J. Post-translational modifications of circulating alpha-1-antitrypsin protein. Int. J. Mol. Sci. 21, 9187 (2020).
Köhnlein, T. & Welte, T. Alpha-1 antitrypsin deficiency: pathogenesis, clinical presentation, diagnosis, and treatment. Am. J. Med. 121, 3–9 (2008).
Sun, R. et al. Alpha-1 antitrypsin in autoimmune diseases: Roles and therapeutic prospects. Int. Immunopharmacol. 110, 109001 (2022).
Ahmed, S., Ahmed, A. & Rådegran, G. Plasma tumour and metabolism related biomarkers AMBP, LPL and Glyoxalase I differentiate heart failure with preserved ejection fraction with pulmonary hypertension from pulmonary arterial hypertension. Int. J. Cardiol. 345, 68–76 (2021).
Vyssoulis, G. P. et al. Alpha-1 microglobulin as a new inflammatory marker in newly diagnosed hypertensive patients. Am. J. Hypertens. 20, 1016–1021 (2007).
Kristiansson, A. et al. α(1)-Microglobulin (A1M) protects human proximal tubule epithelial cells from heme-induced damage in vitro. Int. J. Mol. Sci. 21, 5825 (2020).
Hansson, M. et al. Cystatin C and α-1-microglobulin predict severe acute kidney injury in patients with hemorrhagic fever with renal syndrome. Pathogens 9, 666 (2020).
Åkerström, B. & Gram, M. A1M, an extravascular tissue cleaning and housekeeping protein. Free Radic. Biol. Med. 74, 274–282 (2014).
FLOWER, D. R. The lipocalin protein family: structure and function. Biochem. J. 318, 1–14 (1996).
Bergwik, J., Kristiansson, A., Allhorn, M., Gram, M. & Åkerström, B. Structure, functions, and physiological roles of the lipocalin α1-microglobulin (A1M). Front. Physiol. 12, 645650 (2021).
Wang, F. et al. Apolipoprotein A-IV: a protein intimately involved in metabolism. J. Lipid Res. 56, 1403–1418 (2015).
Kollerits, B. et al. Apolipoprotein A-IV concentrations and clinical outcomes in haemodialysis patients with type 2 diabetes mellitus—a post hoc analysis of the 4D Study. J. Intern. Med. 272, 592–600 (2012).
Kronenberg, F. Apolipoprotein L1 and apolipoprotein A-IV and their association with kidney function. Curr. Opin. Lipido. 28, 39–45 (2017).
Rodríguez-Rivera, C., Garcia, M. M., Molina-Álvarez, M., González-Martín, C. & Goicoechea, C. Clusterin: always protecting. Synthesis, function and potential issues. Biomed. Pharmacother. 134, 111174 (2021).
Poon, S. et al. Mildly acidic pH activates the extracellular molecular chaperone clusterin. J. Biol. Chem. 277, 39532–39540 (2002).
Wyatt, A. R., Yerbury, J. J. & Wilson, M. R. Structural characterization of clusterin-chaperone client protein complexes. J. Biol. Chem. 284, 21920–21927 (2009).
Alnasser, H. A. et al. Requirement of clusterin expression for prosurvival autophagy in hypoxic kidney tubular epithelial cells. Am. J. Physiol. Ren. Physiol. 310, F160–F173 (2016).
Laich, A., Patel, H., Zarantonello, A., Sim, R. B. & Inal, J. M. C2 by-pass: Cross-talk between the complement classical and alternative pathways. Immunobiology 227, 152225 (2022).
Nakamura, Y. et al. Complement activation in patients with heat-related illnesses: soluble CD59 is a novel biomarker indicating severity of heat-related illnesses. Crit. Care Explor. 4, e0678 (2022).
Garred, P., Tenner, A. J. & Mollnes, T. E. Therapeutic targeting of the complement system: from rare diseases to pandemics. Pharm. Rev. 73, 792–827 (2021).
Bode, M. et al. Complement component C3 as a new target to lower albuminuria in hypertensive kidney disease. Br. J. Pharm. 180, 2412–2435 (2023).
Melendez, Q. M. et al. Identification of novel proteins interacting with proprotein convertase subtilisin/kexin 9. Int. J. Biomed. Investig. 3, 1–10 (2020).
Kolialexi, A. et al. Application of proteomics for the identification of differentially expressed protein markers for Down syndrome in maternal plasma. Prenat. Diagn. 28, 691–698 (2008).
Timms, J. F. et al. Discovery of serum biomarkers of ovarian cancer using complementary proteomic profiling strategies. Proteom. Clin. Appl. 8, 982–993 (2014).
Pan, X. Cholesterol metabolism in chronic kidney disease: physiology, pathologic mechanisms, and treatment. Adv. Exp. Med. Biol. 1372, 119–143 (2022).
Zager, R. A., Burkhart, K. M., Johnson, A. C. & Sacks, B. M. Increased proximal tubular cholesterol content: implications for cell injury and “acquired cytoresistance”. Kidney Int. 56, 1788–1797 (1999).
Perez-Riverol, Y. et al. The PRIDE database resources in 2022: a hub for mass spectrometry-based proteomics evidences. Nucleic Acids Res. 50, D543–d552 (2022).
Acknowledgements
Thanks to Prof. Toshiaki Iba’s group from Juntendo University for support with sample collection and supply. Additionally, appreciation to Mr. Shinya Hattori from the National Institute for Materials Science (NIMS) for collaborating on LC–MS/MS conduction for protein identification. Furthermore, this work was supported by “Advanced Research Infrastructure for Materials and Nanotechnology in Japan (ARIM)” of the Ministry of Education, Culture, Sports, Science and Technology (MEXT) (Grant Reference Nos. 16K11421 and 22K09191). Proposal Number JPMXP1224NM0063.
Author information
Authors and Affiliations
Contributions
J.J. (JiayiJin) conducted all experiments, analyzed data, and wrote the initial paper draft. S.Y.W. (SingYingWong) assisted with paper review and revisions, and provided experimental guidance. K.K. (KentaKondo) contributed to reviewer–response revisions and supplied clinical data. T.I. (ToshiakiIba), as clinical professor, offered clinical insights and provided patient samples. N.H. (NobuhiroHayashi) conceived and designed the study as corresponding author, negotiated contracts, optimized paper narrative per journal guidelines, and refined academic tone.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Peer review
Peer review information
Communications Medicine thanks Thiago Gomes Heck and the other, anonymous, reviewer(s) for their contribution to the peer review of this work. [A peer review file is available].
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Jin, J., Wong, S.Y., Kondo, K. et al. Proteomics-based monitoring of heatstroke recovery identifies molecular signatures of organ stress. Commun Med 5, 382 (2025). https://doi.org/10.1038/s43856-025-01075-3
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s43856-025-01075-3
