
Abstract
Post-traumatic stress disorder (PTSD) is a debilitating condition with serious implications for mental and physical health. Although previous studies have documented PTSD prevalence and short-term trajectories, detailed examination of long-term symptom patterns remains limited, especially in large cohorts. This study investigates 20-year PTSD symptom trajectories in World Trade Center responders, constituting one of the largest and longest studies of PTSD to date. We aimed to answer the following questions. How stable are symptoms? What is the average trajectory? What are atypical trajectories? How quickly do symptoms improve and worsen? Does symptom course differ across demographics or predict functional impairments or mental health care utilization? Data include 81,298 observations from 12,822 responders. Symptoms were stable in the short term but changed significantly over two decades, peaking over a decade after exposure and declining modestly thereafter. Demographic differences in average trajectories were small. The median time before symptoms improved was 8–10 years for PTSD cases (median = 8.88; 95% confidence interval, 8.01–9.79). Most experienced improvement after a decade but approximately 10% reported elevated symptoms two decades after trauma. Changes in symptoms predicted higher functional impairments and mental health care utilization. Our findings highlight the enduring impact of PTSD among World Trade Center responders, with substantial variability in individual trajectories. Despite overall modest declines, a subset remained highly symptomatic, underscoring the need for continued treatment. These results emphasize the importance of long-term monitoring and highlight the need for tailored treatment strategies for trauma-exposed populations.
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 12 digital issues and online access to articles
$79.00 per year
only $6.58 per issue
Buy this article
- Purchase on SpringerLink
- Instant access to the full article PDF.
USD 39.95
Prices may be subject to local taxes which are calculated during checkout





Similar content being viewed by others


Data availability
Data not provided in the Article because of space limitations are not publicly shared due to ethical considerations. Study participants provided consent for their data to be analyzed only by study personnel. To respect the autonomy and privacy of the study participants, the data underlying the reported results will be made available to qualified investigators whose proposed use of the data has been approved by an internal review committee and the Institutional Review Board at Stony Brook University. This access will be granted up to 4 years after publication of this study, following rigorous de-identification of sensitive information. Requests for data access will be reviewed and a response will be provided within 60 days of submission.
Code availability
The analysis code is publicly available at https://osf.io/p7sx2/.
References
Davis, L. L. et al. The economic burden of posttraumatic stress disorder in the United States from a societal perspective. J. Clin. Psychiatry 83, 21m14116 (2022).
Jordan, H. T. et al. Persistent mental and physical health impact of exposure to the September 11, 2001 World Trade Center terrorist attacks. Environ. Health 18, 12 (2019).
Lowell, A. et al. 9/11-Related PTSD among highly exposed populations: a systematic review 15 years after the attack. Psychol. Med. 48, 537–553 (2018).
Cone, J. E. et al. Chronic probable PTSD in police responders in the World Trade Center health registry ten to eleven years after 9/11. Am. J. Ind. Med. 58, 483–493 (2015).
Galatzer-Levy, I. R., Huang, S. H. & Bonanno, G. A. Trajectories of resilience and dysfunction following potential trauma: a review and statistical evaluation. Clin. Psychol. Rev. 63, 41–55 (2018).
Able, M. L. & Benedek, D. M. Severity and symptom trajectory in combat-related PTSD: a review of the literature. Curr. Psychiatry Rep. 21, 58 (2019).
Feder, A. et al. Risk, coping and PTSD symptom trajectories in World Trade Center responders. J. Psychiatric Res. 82, 68–79 (2016).
Pietrzak, R. et al. Trajectories of PTSD risk and resilience in World Trade Center responders: an 8-year prospective cohort study. Psychol. Med. 44, 205–219 (2014).
Lee, D. J. et al. The 20-year course of posttraumatic stress disorder symptoms among veterans. J. Abnorm. Psychol. 129, 658–669 (2020).
Solomon, Z. et al. Predictors of PTSD trajectories following captivity: a 35-year longitudinal study. Psychiatry Res. 199, 188–194 (2012).
Rosellini, A. J. et al. Recovery from DSM-IV post-traumatic stress disorder in the WHO World Mental Health surveys. Psychol. Med. 48, 437–450 (2018).
Marmar, C. R. et al. Course of posttraumatic stress disorder 40 years after the Vietnam war: findings from the National Vietnam Veterans Longitudinal Study. JAMA Psychiatry 72, 875–881 (2015).
Morina, N. et al. Remission from post-traumatic stress disorder in adults: a systematic review and meta-analysis of long term outcome studies. Clin. Psychol. Rev. 34, 249–255 (2014).
Bui, E. et al. Course of posttraumatic stress symptoms over the 5 years following an industrial disaster: a structural equation modeling study. J. Trauma. Stress 23, 759–766 (2010).
Livingston, N. A. et al. Longitudinal assessment of PTSD and illicit drug use among male and female OEF-OIF veterans. Addict. Behav. 118, 106870 (2021).
Zvolensky, M. J. et al. Post-disaster stressful life events and WTC-related posttraumatic stress, depressive symptoms, and overall functioning among responders to the World Trade Center disaster. J. Psychiatric Res. 61, 97–105 (2015).
Ginzburg, K., Ein-Dor, T. & Solomon, Z. Comorbidity of posttraumatic stress disorder, anxiety and depression: a 20-year longitudinal study of war veterans. J. Affect. Disord. 123, 249–257 (2010).
Blanchard, E. B. et al. Psychometric properties of the PTSD Checklist (PCL). Behav. Res. Ther. 34, 669–673 (1996).
Berlin, K. S., Williams, N. A. & Parra, G. R. An introduction to latent variable mixture modeling (part 1): overview and cross-sectional latent class and latent profile analyses. J. Pediatr. Psychol. 39, 174–187 (2014).
Skogstad, L., Heir, T., Hauff, E. V. & Ekeberg, Ø. Post-traumatic stress among rescue workers after terror attacks in Norway. Occup. Med. 66, 528–535 (2016).
Thormar, S. B. et al. The mental health impact of volunteering in a disaster setting: a review. J. Nerv. Ment. Dis. 198, 529–538 (2010).
Gandek, B. et al. Cross-validation of item selection and scoring for the SF-12 Health Survey in nine countries: results from the IQOLA Project. J. Clin. Epidemiol. 51, 1171–1178 (1998).
Ware, J. E., Kosinski, M. & Keller, S. D. A 12-Item Short-Form Health Survey: construction of scales and preliminary tests of reliability and validity. Med. Care 34, 220–233 (1996).
Fujita, F. & Diener, E. Life satisfaction set point: stability and change. J. Pers. Soc. Psychol. 88, 158–164 (2005).
Mann, F. D., DeYoung, C. G. & Krueger, R. F. Patterns of cumulative continuity and maturity in personality and well-being: evidence from a large longitudinal sample of adults. Pers. Individ. Dif. 169, 109737 (2021).
Waszczuk, M. A. et al. Polygenic prediction of PTSD trajectories in 9/11 responders. Psychol. Med. 52, 1981–1989 (2022).
Mann, F. D. et al. A novel approach to model cumulative stress: area under the s-factor curve. Soc. Sci. Med. 348, 116787 (2024).
Mann, F. D., Cuevas, A. G. & Krueger, R. F. Cumulative stress: a general ‘s’ factor in the structure of stress. Soc. Sci. Med. 289, 114405 (2021).
Perrin, M. A. et al. Differences in PTSD prevalence and associated risk factors among World Trade Center disaster rescue and recovery workers. Am. J. Psychiatry 164, 1385–1394 (2007).
Bromet, E. J. et al. DSM-IV post-traumatic stress disorder among World Trade Center responders 11–13 years after the disaster of 11 September 2001 (9/11). Psychol. Med. 46, 771–783 (2016).
Wisnivesky, J. P. et al. Persistence of multiple illnesses in World Trade Center rescue and recovery workers: a cohort study. Lancet 378, 888–897 (2011).
Hagh‐Shenas, H., Goodarzi, M. A., Dehbozorgi, G. & Farashbandi, H. Psychological consequences of the Bam earthquake on professional and nonprofessional helpers. J. Trauma. Stress 18, 477–483 (2005).
Hobfoll, S. E. et al. Five essential elements of immediate and mid-term mass trauma intervention: empirical evidence. Psychiatry 70, 283–315 (2007).
Hawn, S. E. et al. Conceptualizing traumatic stress and the structure of posttraumatic psychopathology through the lenses of RDoC and HiTOP. Clin. Psychol. Rev. 95, 102177 (2022).
Bauer, D. J. & Curran, P. J. Distributional assumptions of growth mixture models: implications for overextraction of latent trajectory classes. Psychol. Methods 8, 338–363 (2003).
Bauer, D. J. & Curran, P. J. The integration of continuous and discrete latent variable models: potential problems and promising opportunities. Psychol. Methods 9, 3–29 (2004).
Bauer, D. J. Observations on the use of growth mixture models in psychological research. Multivar. Behav. Res. 42, 757–786 (2007).
Joseph, K. S., Mehrabadi, A. & Lisonkova, S. Confounding by indication and related concepts. Curr. Epidemiol. Rep. 1, 1–8 (2014).
Wager, S. & Athey, S. Estimation and inference of heterogeneous treatment effects using random forests. J. Am. Stat. Assoc. 113, 1228–1242 (2018).
Chernozhukov, V. et al. Double/debiased machine learning for treatment and structural parameters. Econom. J. 21, C1–C68 (2018).
Pietrzak, R. H. et al. The burden of full and subsyndromal posttraumatic stress disorder among police involved in the World Trade Center rescue and recovery effort. J. Psychiatric Res. 46, 835–842 (2012).
Dasaro, C. R. et al. Cohort profile: World Trade Center Health Program General Responder Cohort. Int. J. Epidemiol. 46, e9 (2017).
Robins, L. N. et al. Diagnostic Interview Schedule for the DSM-IV (DIS-IV) (Washington Univ. School of Medicine, 2000).
First, M. B. et al. Structured Clinical Interview for DSM-IV Axis I Disorders–Patient Edition (version 2) (Biometric Research Institute, 1995).
Ware, Jr, J. E. & Sherbourne, C. D. The MOS 36-item short-form health survey (SF-36): I. Conceptual framework and item selection. Med. Care 30, 473–483 (1992).
Hunter, J. E. & Schmidt, F. L. Methods of Meta-Analysis: Correcting Error and Bias in Research Findings (Sage, 2004).
Pinheiro, J. et al. Package ‘nlme’. Linear and nonlinear mixed effects models. R package version 3: 274 (2017).
Bates, D., Mächler, M., Bolker, B. & Walker, S. Fitting linear mixed-effects models using lme4. J. Stat. Softw. 67, 1–48 (2015).
Proust-Lima, C. et al. Package ‘lcmm’. R package version 2.1.0 (2023).
Benjamini, Y. & Hochberg, Y. Controlling the false discovery rate—a practical and powerful approach to multiple testing. J. R. Stat. Soc. Series B Methodol. 57, 289–300 (1995).
Erler, N. S., Rizopoulos, D. & Lesaffre, E. M. E. H. JointAI: joint analysis and imputation of incomplete data in R. J. Stat. Softw. 100, 1–56 (2021).
Monson, C. M. et al. Change in posttraumatic stress disorder symptoms: do clinicians and patients agree? Psychol. Assess. 20, 131–138 (2008).
Therneau, T. & Lumley, T. R Survival Package. R package version 3.7.0 (2013).
Kassambara, A. et al. Package ‘survminer’. Drawing survival curves using ‘ggplot2’. R package version 0.3.1 (2017).
Hothorn, T. et al. Package ‘lmtest’. Testing linear regression models. https://cran.r-project.org/web/packages/lmtest/lmtest.pdf R package version 0.9.40 (2022).
Zeileis, A. et al. Package ‘sandwich’. R package version 3-0.03 (2021).
Acknowledgements
Data collection was funded by CDC 2011‐200‐39361 (awarded to B.J.L.), U01OH011864 (awarded to R.K. and M.A.W.) and the SUNY Research Foundation. F.D.M. was awarded and partially funded by R21AG074705‐01. We thank the WTC responders from the General Responder Cohort whose participation was integral to this work.
Author information
Authors and Affiliations
Contributions
F.D.M. analyzed the data in consultation with R.K. F.D.M. drafted the manuscript. B.J.L., R.K. and M.A.W. obtained funding for the study. M.A.W., S.A.P.C., S.F., C.J.R., B.P.M., J.E.S., E.J.B. and B.J.L. provided critical revisions and approved the final version of the Article.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Peer review
Peer review information
Nature Mental Health thanks Shane Adams, Clare Henn-Haase and Christopher Layne for their contribution to the peer review of this work.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Extended data
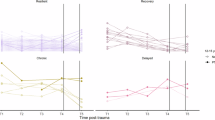
Extended Data Fig. 1 Observed trajectories of PTSD symptoms for WTC responders.
Top left panel, individual trajectories are plotted for the full sample. The remaining panels plot subsamples of n = 500 observations without replacement with dashed gray lines indicating quadratic trends and orange regions denoting 95% confidence bands.
Extended Data Fig. 2 Average predicted trajectories of PTSD symptoms from quadratic and cubic mixed effects models.
The top and bottom panels plot average quadratic and cubic trends, respectively. Blue “X”s indicates annual means and dashed vertical lines denote plus and minus 2 times the standard error of the mean. Sample sizes and descriptive statistics are reported in Table 1.
Extended Data Fig. 3 Observed scores and predicted trajectories for individual responders diagnosed with PTSD from parametric and generalized mixed effect models.
Observed scores (blue circles) from 20 responders with a lifetime diagnosis of PTSD and 15 or more observations are plotted with predicted trends from a linear mixed effect model (dashed red line) and a generalized mixed effect model with Gamma distribution and log link (dashed black line).
Extended Data Fig. 4 Average predicted trend in PCL scores from the preferred generalized mixed effect model stratified by baseline year of data collection, the number of completed assessments, and the average interval between assessments.
a, Each line depicts the average predicted trend for responders who completed their baseline assessment during a given year. b, Each line depicts the average predicted trend for responders who completed different numbers of assessments. c, Each line depicts the average predicted trend for responders with different average intervals of time between assessments. In all panels, shaded regions depicting 95% confidence bands.
Extended Data Fig. 5 Distributions of changes in observed PCL scores across increasing time lags stratified by baseline PCL score.
Given intercept-slope correlations, plots were stratified by observed PCL scores at in-take. Created using the ‘ggridges’ package, density plots of observed changes in PCL scores (x axis) across increasing time lags (y axis) are plotted and grouped by observed PCL scores at first visit (top label of each panel).
Extended Data Fig. 6 Average predicted trajectory of PTSD symptoms by demographic factors.
a, Age-group differences in the average predicted trajectory. b, Sex differences in the average predicted trajectory. c, Race/ethnicity differences in the average predicted trajectory. d, Occupational differences in the average predicted trajectory. In all panels, shaded regions denote 95% confidence bands. Effects of demographic factors on levels of symptoms (that is, intercepts) are statistically significant at two-tailed FDR-adjusted q-values < 0.05 using the Benjamini–Hochberg procedure, and effects on rates of change (that is linear and quadratic slopes) are not statistically significant (q-values > 0.10).
Extended Data Fig. 7 Average predicted trajectory of PTSD symptoms by traumatic exposures.
Average predicted trajectories are depicted for responders who arrived early or late to the WTC following the 9/11 attacks (a), who did or did not witness the collapse of the Twin Towers (b), reported being caught in the dust cloud (c), exposed to blood or bodily fluids (d), exposed to human remains (e), slept at Ground Zero (f), knew someone who was injured (g), and knew someone who died (that is, experienced traumatic bereavement; h). In all panels, shaded regions denote 95% confidence bands. The effects of each traumatic exposures on levels of symptoms (that is, intercepts) are statistically significant at FDR-adjusted q-values < 0.001 using the Benjamini–Hochberg procedure, and the effects of each traumatic exposures on rates of change (that is, linear and quadratic slopes) are not statistically significant (q-values > 0.10).
Extended Data Fig. 8 Prediction of functional impairments in 2022 by deciles of predicted change in PTSD symptoms.
Circles denote adjusted risk ratios from robust quasi-Poisson regressions predicting impairment in mental function and physical function, indicated by a mental component score (MCS < 40) or physical component score (PCS < 40) derived from the SF-12 more than one standard deviation below the normed average, controlling for the effects of demographic factors and baseline PTSD symptom severity (Supplementary Tables 13 and 14). Vertical bars denote 95% confidence intervals calculated using heteroscedasticity-consistent (HC1) standard errors.
Extended Data Fig. 9 Prediction of mental health care services in 2022 by deciles of predicted change in PTSD symptoms.
Circles denote linear regression coefficients predicting log transformed expenditures (a) and relative risk ratios from robust quasi-Poisson regressions (b,c), adjusted for the effects of demographic factors and baseline PTSD symptom severity (Supplementary Tables 15–17). Vertical bars denote 95% confidence intervals calculated using heteroscedasticity-consistent (HC1) standard errors.
Supplementary information
Supplementary Information (download PDF )
Supplementary methods, Tables 1–18 and Figs. 1–12.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Mann, F.D., Waszczuk, M.A., Clouston, S.A.P. et al. A 20-year longitudinal cohort study of post-traumatic stress disorder in World Trade Center responders. Nat. Mental Health 3, 789–802 (2025). https://doi.org/10.1038/s44220-025-00419-1
Received:
Accepted:
Published:
Version of record:
Issue date:
DOI: https://doi.org/10.1038/s44220-025-00419-1
This article is cited by
-
Polygenic Risk and Exposure Severity Predict Trajectories of PTSD: A Prospective Cohort Study
Molecular Psychiatry (2025)
