
Abstract
The current diagnostic gold standard for metabolic dysfunction-associated steatohepatitis (MASH) requires invasive biopsy to assess steatosis, inflammation, and ballooning. While MRI-based proton density fat fraction (PDFF) and MR elastography address steatosis and fibrosis, non-invasive methods for evaluating hepatic inflammation remain lacking. This study developed a diffusion MRI (dMRI)-based MR cytometry technique to map liver cellular properties, including MRI-derived cell size (excluding fat content) and cell density. Validation through histology-driven simulations and ex vivo MRI of fixed human liver specimens demonstrated that stromal regions exhibit smaller MRI-derived cell sizes and higher cell densities than both normal and fatty tissues. An in vivo feasibility study, conducted on healthy subjects (n = 5) and MASH patients (n = 5) using a clinical 3 T MRI system, further showcased the potential of MR cytometry to characterize pathological changes in liver microstructure.
Similar content being viewed by others


Introduction
The development of non-invasive diagnostic techniques for metabolic dysfunction-associated steatohepatitis (MASH), particularly for distinguishing MASH from simple steatosis1, has gained significant interest due to the shortcomings of liver biopsy2. As the global obesity epidemic continues to rise, the prevalence of MASH—a severe form of Metabolic dysfunction-associated steatotic liver disease (MASLD) —has increased. In 2015, an estimated 16.5 million individuals in the U.S. (5% of the population) were affected by MASH, a figure projected to reach 27 million (7.67%) by 20303. The ability to differentiate MASH from simple steatosis is critical for patient management, especially following the recent FDA approval of resmetirom (Rezdiffra) for treating MASH with stage 2 or 3 fibrosis.
While individuals with simple steatosis alone are generally thought to have a relatively benign long-term prognosis, up to a quarter of these patients may develop MASH, which can progress to cirrhosis4, a potent risk factor for the development of hepatocellular carcinoma (HCC). Currently, MASH is diagnosed and staged through biopsy using three components, including steatosis, lobular inflammation, and ballooning. As with any chronic liver disease, fibrosis staging is important from a therapeutic and diagnostic standpoint. However, biopsy is invasive, costly, and subject to sampling variability, prompting the need for reliable non-invasive alternatives. Existing non-invasive imaging methods, such as MRI-based proton density fat fraction (PDFF) and MR elastography (MRE), have been shown to quantify steatosis5 and fibrosis6, respectively. T1 mapping using MRI has been reported to be a valuable tool for assessing liver inflammation7, however, T1 relaxation times are affected by many other factors, such as steatosis8, fibrosis9, and iron overload10, making it difficult to attribute changes solely to inflammation. The availability of a reliable non-invasive tool to assess the inflammatory stage of MASLD (i.e., MASH) is urgently needed in clinical practice, particularly in light of the recent FDA approval of resmetirom (Rezdiffra) for the treatment of MASH with stage 2–3 fibrosis.
Inflammation in MASH is marked by infiltration of small immune cells, such as T lymphocytes, neutrophils, and natural killer cells, which have smaller sizes (< 15 um)8,11,12 compared to hepatocytes (15–30 um)13,14, the chief functional cells in the liver. This infiltration increases local cell density15 and decreases the average cell sizes, offering an opportunity to assess inflammation by quantifying differences in cell size and cell density. Currently, such information is obtainable only via biopsy. A non-invasive imaging approach to quantify these pathological changes could significantly improve diagnostic capabilities.
Significant efforts have been made to develop noninvasive imaging methods that characterize biological tissues at the cellular level. Diffusion MRI (dMRI) is a promising technique that examines the restriction and hindrance of water molecules diffusing in biological tissues, providing unique insight into tissue microstructure. However, conventional dMRI, particularly the widely-used apparent diffusion coefficient (ADC), reflects averaged diffusion properties across all structures and length scales, yielding ambiguous microstructural information. Recently, a class of advanced dMRI methods has been developed to tackle this limitation. Specifically, these methods use multi-compartment biophysical models and acquisitions with multi-b and multi-diffusion times to estimate mean cell size and density, such as VERDICT(vascular, extracellular, and restricted diffusion for cytometry in tumors)16, IMPULSED (imaging microstructural parameters using limited spectrally edited diffusion)13,17,18,19, JOINT (IMPULSED combined with transcytolemmal water exchange)19, and POMACE (pulsed and oscillating gradient MRI for assessment of cell size and extracellular space)20. Because these methods non-invasively characterize microstructural information at the cellular level, we have termed this class of techniques MR cytometry. To date, MR cytometry is almost exclusively utilized for cancer imaging21. Recently, we were the first to adapt and implement MR cytometry in healthy human and rodent livers in vivo13,21, demonstrating the feasibility of mapping liver microstructures. Consequently, we propose a new concept suggesting that MR cytometry can quantify pathological changes in the average cell size and cell density in MASH, and therefore complement PDFF and MRE, and potentially reducing the need for biopsy. The primary objectives of this study were to determine if MRI-derived cell size and density can serve as biomarkers of inflammation and to assess the ability of MR cytometry to measure these changes in vivo in MASH patients.
Results
Histology-based simulations confirmed pathological variations in cell size and density
As shown in Fig. 1, the fitted average stroma cell sizes are significantly smaller than those in steatosis and normal liver tissues at all SNR levels (10, 20, and 50). The fitted average stroma cell densities are significantly higher than those in steatosis and normal liver tissues, with variations increasing at lower SNRs.

Fitted cell sizes (top row) and densities (bottom row) from histology-based simulated diffusion signals for normal liver tissues, steatosis, and stroma (a combination of inflammatory cells and fibrosis) at three different SNR levels (10, 20, and 50, from left to right). *P < 0.05, **P < 0.01, ***P < 0.001, and ****P < 0.0001 as measured by one-way analysis of variance (ANOVA) with Bonferroni correction.
Ex vivo MR cytometry characterized different pathological conditions
Figure 2 shows β-Catenin stained histologic sections and corresponding MRI and histology-derived maps of cell size and cellularity (i.e., density) of two human liver samples, including a sample with moderate steatosis (Fig. 2A) and a sample with MASH (Fig. 2B). Strong membranous β-catenin staining showed significant morphological differences among different liver pathological conditions (Fig. 2C–E). Most cells in normal liver tissues are hepatocytes (Fig. 2C), which are bigger than stroma cells (a mixture of inflammatory cells and fibrosis) (Fig. 2E). In fatty liver areas, the accumulation of abnormal amounts of fat in hepatocytes results in either a single large fat vacuole or several smaller ones that occupy the greater part of the cell, pushing the nucleus to the periphery (Fig. 2C). β-catenin does not stain membranes of stroma cells (Fig. 2E). Therefore, the average cell size of stroma could not be estimated from β-catenin histological sections directly. Instead, it was calculated from the nucleus size, assuming a constant nuclear-cytoplasmic ratio of 1:122. By comparing the number of nuclei from H&E images, stroma tissues have a higher cellularity than normal liver tissues. These findings are supported by maps of MRI and histology-derived cell size and cellularity. MRI-derived cell sizes have similar values compared to those derived from histology, while MRI-derived cellularities are larger than histology-derived cellularities. The outlines of tissue samples as measured by MRI and histology are almost the same (Fig. 2F-I).

β-Catenin stained histological pictures (A–E) and corresponding MRI (F, H) and histology-derived maps (G, I) of cell size and cellularity from two human liver specimens, including a sample with moderate steatosis and a sample with MASH.
Histology-derived cell sizes, cellularities, fat fractions, and MRI-derived cell sizes and cellularities of different liver pathologies and conditions were summarized using Box-and-whisker plots (Fig. 3). Our MR measurements suppressed fat signals, so the area of fat vacuoles was deducted from the area of cells when calculating the cell size on histological sections. Therefore, histology-derived cell sizes for fatty areas (the average fat fraction ~13%) are smaller than those for normal liver (the average fat fraction ~6%). Both histology and ex vivo MR cytometry reveal that stroma has significantly smaller cell sizes and higher cellularities than normal liver and steatosis. A combination of MRI-derived cell size and cell density differentiates stroma well from steatosis and normal liver tissues (Fig. 4).

Box-and-whisker plots of histology-derived cell sizes (A), cellularities (B), and fat fractions (C) and MRI-derived cell sizes (D) and cellularities (E) for liver ROIs with different pathologies. For all the Box-and-whisker plots, the 25th–75th percentiles are blocked by the box, the red bands inside the box are the mean values, and the whiskers mark the SD. *P < 0.05, **P < 0.01, ***P < 0.001, and ****P < 0.0001 as measured by one-way analysis of variance (ANOVA) with the Bonferroni correction.

Note that blank spots on the parametric maps represent imaging voxels that do not show apparent diffusion time dependency due to either poor signal-to-noise ratios or being dominated by fluids (e.g., blood vessels). The binary threshold map highlights imaging voxels with cell size < 10 µm and cell density > 30 × 104/mm3 in red and displays all other voxels in green. The red dots are hypothesized to visualize the severity of inflammation.
In vivo MR cytometry quantified microstructures in healthy subjects and MASH patients
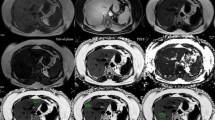
Figures 4 and 5 show maps of MRI-derived cell size, cell density, and fat fraction from a single slice for each subject overlaid on T2W anatomical images. For the five healthy subjects, the average fitted cell sizes and cell densities range from 15 to 20 µm and 20 to 25 x 104/mm3, aligning with previously reported sizes and densities for human hepatocytes14,23. In the five MASH patients, the average fitted cell sizes are slightly smaller, and the average fitted cell densities are higher compared to healthy subjects. Additionally, the standard deviations of cell size and cell density are greater in MASH patients than in healthy subjects. These variations are depicted in the histograms in Supplementary Figs. 5 and 6, which show a wider distribution of cell sizes and a longer tail in the cell density distribution for MASH patients, suggesting a more diverse microenvironment in MASH-affected livers. To quantify these differences, we categorized all imaging voxels into two groups based on thresholds for cell size and cell density (e.g., cell size = 10 µm and cell density = 30 x 104/mm3). Figure 6 illustrates the average perfusion-free signal decay and their fittings for regions defined by these thresholds, indicating an apparent diffusion time dependency in the diffusion signal decays. We defined the fraction of imaging voxels with cell sizes smaller than 10 µm and cell densities higher than 30 x 104/mm3 as the Small Dense Cell Fraction (SDCF). The SDCF is significantly higher in MASH patients than in healthy subjects, as shown in Fig. 7 and Table 1.

Note that blank spots on the parametric maps represent imaging voxels that do not show apparent diffusion time dependency due to either poor signal-to-noise ratios or being dominated by fluids (e.g., blood vessels). The binary threshold map highlights imaging voxels with cell size < 10 µm and cell density > 30 × 104/mm3 in red and displays all other voxels in green. The red dots are hypothesized to visualize the severity of inflammation. MASH livers exhibit scattered or intense red dots throughout the liver.

The average perfusion-free signal decay and their fittings for regions split by thresholds of cell size at 10 µm and cell density at 30 × 104/mm3, for 5 subjects with MASH.

Box-and-whisker plots of voxel fractions with cell size < 10 µm and cell density > 30 x 104/mm3 for healthy subjects and MASH patients. For all the Box-and-whisker plots, the 25th–75th percentiles are blocked by the box, the red bands inside the box are the mean values, and the whiskers mark the SD. *P < 0.05, **P < 0.01, ***P < 0.001, and ****P < 0.0001 as measured by one-way analysis of variance (ANOVA) with Bonferroni correction.
Discussion
In this work, we proposed a novel concept where changes in cell size and cell density (or cellularity in 2D) can serve as biomarkers of inflammation, a critical diagnostic component for MASH, using a noninvasive imaging method known as MR cytometry. Through histological analysis of fixed human liver specimens, including those with steatohepatitis, steatosis, and normal liver tissue, we demonstrated that cell size and cell density can effectively differentiate between these pathological conditions. These findings are consistent with previous studies reporting that inflammatory cells are typically smaller (< 15 um)8,11,12 than hepatocytes (15–30 um)13,14, and cell density could serve as a biomarker for identifying inflammation the liver24. Histology-based simulations further confirmed that these differences in cell size and cell density can be quantified when the SNR exceeds 10, with reliability decreasing as SNR diminishes. Our in vivo pilot study demonstrated the feasibility of MR cytometry in both healthy subjects and MASH patients using clinical 3 T scanners lasting less than 12 min. Distinct distributions of cell size and cell density were observed between the two groups. Notably, the SDCF did not correlate with the fat fraction in MASH patients (Pearson’s tau correlation coefficients = 0.01, p-value = 0.98), suggesting that the SDCF may provide additional information beyond fat fractions and could be associated with inflammation, although further validation in a larger cohort of MASH patients is required.
It is essential to understand the effects of other diagnostic features (steatosis, fibrosis, and ballooning), as well as other pathologies such as iron overload, on MR cytometry-derived cell size, cell density, and SDCF in MASH livers. In the case of steatosis, a single large fat vacuole or several smaller ones occupy the greater part of the cell and push the nucleus to the periphery. In this scenario, water diffusion inside the cell is restricted by a smaller space, which is approximately the difference between the cell volume and the fat volume. The MRI-derived cell size represents the average size of the compartment in which water molecules are restricted, so the average restriction size of fatty liver tissue as measured by MR cytometry is much smaller than the actual size of fatty cells. Furthermore, fat may have a direct impact on the diffusion MRI signals, even though the diffusion MRI signals are collected with fat suppression. However, it is fortunate that fat diffusion is two orders of magnitude smaller than water diffusion25. As a result, lipid molecules move a small distance (<< 1 um) within the diffusion times (5–70 ms) used by MR cytometry and experience ‘free diffusion’ inside hepatocytes. With the maximum b value (1 ms/µm2) that was used in this study, the unsuppressed fat signal decays by approximately 1%, and can be included as a constant term in the liver signal model.
Ballooning is a form of hepatocyte death. It is defined as rounded hepatocyte enlargement > 1.5–2 times the normal diameter with loss of the usual polygonal shape of the cell and usually containing pale staining cytoplasm, variably sized cytoplasmic vacuoles, and frequently Mallory Denk bodies. However, such cell enlargement may not be detected by MR cytometry with diffusion times ranging from 5 to 70 ms.
Fibrosis is characterized by the excessive accumulation of extracellular matrix proteins including collagen and involves hepatic stellate cells (~ 13 µm)26,27 as well as infiltrating T cells (~ 6-10 µm)28,29. This condition is expected to reduce the average cell size and increase cell density. Our MASH patients #1 and #3, who have a fibrosis stage of 3, exhibit much higher SDCF (~ 9%) compared to the other three MASH patients with similar inflammation scores. There is evidence that a modest degree of iron overload is associated with more advanced liver injury in MASH30.
Iron overload decreases the T2 relaxation time of the liver significantly, which could potentially lead to a low SNR (< 20) in diffusion signals for patients with iron overload. To enhance SNR and achieve reliable data fitting, diffusion signals can be averaged over a small window (e.g., 3 x 3 window), which could boost SNR by approximately 3 times. We acknowledge that compromising on the spatial resolution of MRI-derived parametric maps is acceptable since the existence and severity of MASH are of more diagnostic importance than information on the spatial distribution of MASH. Iron overload can cause local variations in T2, particularly between intra- and extracellular spaces. To reduce model complexity, we assumed homogeneous T2 relaxation across the liver in this study, consistent with several other multi-compartment diffusion MRI models proposed for solid tissues16,20. This simplification allows MR cytometry to use a single echo time (TE), enabling a total scan time of less than 12 min for liver imaging, which is practical for clinical applications. In our recent studies on the impact of T2 on MR cytometry in tumors (with cell sizes ranging from 10–15 µm)31, we observed that T2 differences between intra- and extracellular spaces have minor effects on cell size estimation. However, these differences can either overestimate or underestimate the intracellular volume fraction, depending on whether the intracellular T2 is longer or shorter than the extracellular T2. While we have proposed a multi-echo-time imaging protocol to achieve accurate intracellular volume fraction estimation, this approach significantly increases scan time. It is also important to note that iron overload is not the diagnostic feature of MASH, evidence suggests that a modest degree of iron overload is typically associated with more advanced liver injury in MASH. As our focus is on detecting MASH at early stages, severe iron overload is less likely to be a confounding factor.
A moderate to weak linear correlation (Pearson’s tau correlation coefficients = 0.58 and 0.39, for cell size and cellularity, respectively, both with p < 0.0001) between MRI and histology measurements was observed (Supplementary Fig. 4). The correlations between MRI and histology measurements are affected by several concurrent factors. Both MRI and histology have biases when measuring the average cell size and cellularity in biological tissues. For MRI measurements, the range of cell sizes that can be measured by MR cytometry depends on how far water molecules diffuse, which is a function of diffusion time and water diffusion coefficient. For the effective diffusion times (5–70 ms) used in this study, MR cytometry is sensitive to cell sizes from about 5–20 µm (the root-mean-square-displacement of water at body temperature). Also, large cells contribute more to the average MRI-derived cell size than small cells because the overall diffusion signals from all the cells are volume-weighted. The relation of the average MRI-derived cell size depends on the distribution of cell sizes and does not equal to the true average cell size. Secondly, the water exchange effects for diffusion measurements with relatively long diffusion times (e.g., > 10 ms) have been included in our signal model, which has been demonstrated to reduce the error of fitted \({v}_{{in}}\) when the water exchange is slow. However, with faster water exchange, our signal model still underestimates \({v}_{{in}}\) 19 and thus underestimates the cell density. In addition, as mentioned earlier in 2.5, the formula used to calculate the cellularity ignores the impact of fat, leading to an overestimation of cellularity for fatty liver tissues. For histology measurements, first, tissue shrinkage occurs during histology preparation and the fact that the tissue section rarely passes through the center of the cell, leading to an underestimation of cell size. Secondly, the imperfect co-registration between MRI and histology may also contribute to the moderate correlation between the two measurements. Although the homemade tissue sample holder guarantees both the MR images and histological sections were obtained from the same location, tissue shrinkage/distortion occurs during the histology preparation. The 2D shape registration used in this study allows two outlines of the same specimen in the MR image and histologic section match with each other, but it may still generate errors when transforming ROIs inside the specimen from histology to MRI due to the complexities of modeling tissue deformation. In addition, the histological section is much thinner than the MR image slice thickness. Taking all these factors into account, we are not surprised to obtain an either moderate or weak correlation between MRI and histology-derived cell sizes and cellularities. More important than evaluating the accuracy of MRI measurements, the key finding of this study is that MR cytometry can detect and quantify pathological changes in liver microstructure that are confirmed by histology.
Fat fraction values measured using Philips’ PDFF product (mDIXON Quant) were used to calculate the MRI-derived cell density, estimated as \((1-{f}_{{fat}})\times {6v}_{{in}}/\pi {d}^{3}\). Given that the fat distribution appears relatively homogeneous across the MASH liver, as demonstrated by our in vivo data, and that our primary focus is on the relative difference in cell density, any potential bias in fat fraction measurements has a minor impact on our findings.
Our in vivo MR cytometry generated five parametric maps (\({f}_{{IVIM}},{d}\), \({v}_{{in}}\), \({\rm{AD}}{{\rm{C}}}_{{ex}},\,{\tau }_{{in}}\)). In this study, we focused only on \(d\) and \({v}_{{in}}\) because our central hypothesis is that imaging voxels dominated by inflammation have small cell sizes and high cell densities. Additionally, the fitted \(d\) has been shown in our previous computer simulations32, in vitro cell experiments33,34, and in vivo animal studies18 to be estimated more reliably than other fitted parameters. \({\rm{AD}}{{\rm{C}}}_{{ex}}\) provides similar information as the ADC values obtained by conventional PGSE acquisitions with a relatively long diffusion time. In a recent study19, \({\tau }_{{in}}\) has been shown to be an indicator of water exchange between intra and extra-cellular spaces using computer simulations and in vitro cell experiments. However, the accuracy and precision of \({\tau }_{{in}}\) need further investigation. \({f}_{{IVIM}}\) has been investigated for assessing liver fibrosis35. It could potentially be combined with MRI-derived cell size and cell density for a comprehensive characterization of MASH. However, this is beyond the scope of this study.
Validating the accuracy of MR cytometry-derived microstructural properties in livers with and without MASH presents significant challenges. Currently, no other in vivo techniques have been reported to measure liver microstructural properties, such as cell size and density, aside from our work. Obtaining regions at the early stage of MASH from transplanted livers is nearly impossible. While liver biopsies allow quantitative analysis of liver microstructure, they only represent small samples (1–2 mg), making direct comparisons between biopsy-derived scores and MRI results difficult. For example, in this study, SDCF values did not correlate well with inflammation scores obtained from liver biopsies.
A practical alternative involves conducting histology and MR cytometry on fixed human specimens, as well as performing histology-based computer simulations, as demonstrated in this study. Animal models that encapsulate key pathological features of human MASH also provide valuable insights. Importantly, the ultimate goal is to identify inflammation-induced changes in cell size and density. Thus, the repeatability of MR cytometry-derived measurements of cell size and density is more critical than their absolute accuracy. Establishing cutoff values for cell size and density to differentiate inflammation from simple steatosis requires larger clinical studies involving subjects with MASH or simple steatosis.
Currently, dedicated efforts are underway to investigate the quantitative relationships between MRI-derived cell size and density and varying pathologies using animal models, study the reproducibility of MR cytometry across a larger number of individuals, and evaluate the ability of MR cytometry to differentiate MASH from simple steatosis in large subject cohorts.
In summary, we have demonstrated that MR cytometry can quantify changes in cell size and density associated with inflammation through a combination of computer simulations and ex vivo experiments. Our preliminary in vivo studies have shown the feasibility of MR cytometry in both healthy subjects and those with MASH, using clinical 3 T scanners within a 12 min imaging protocol. Furthermore, this study provides initial evidence supporting the hypothesis that MRI-derived measures of cell size and density could improve the noninvasive differentiation of inflammation from fatty and normal liver tissues. This technique holds promise as a complementary tool to existing noninvasive methods, such as PDFF and MRE, contributing to the development of a comprehensive, noninvasive diagnostic approach for MASH.
Methods
Theory of MR cytometry
Within the framework of Temporal Diffusion Spectroscopy (TDS), MR cytometry17,18,33 uses a limited number of diffusion measurements obtained at clinically achievable b values and diffusion times (i.e., from 5 to 70 ms). This technique models the extravascular microenvironment of solid tissues by segmenting it into intra- and extracellular compartments. These compartments are differentiated based on the varying diffusion time-dependence of the ADC, enabling estimation of microstructural parameters, such as mean cell size \(d\) and intracellular volume fraction \({v}_{{in}}\) by approximating the restricted intracellular space as a sphere. Within each imaging voxel, the MRI-derived cell size corresponds to the average diameter of spheres with equivalent volumes to the restricted intracellular spaces, particularly the space excluding fat contents in fatty liver tissue. For clarity, all references to MRI-derived cell size in the following text will specifically refer to the equivalent cell size excluding the fat content. The critical factor in applying MR cytometry is determining whether the size of restricted intracellular space can be sensitized by water diffusion within the clinically achievable diffusion times. In liver tissues, cell sizes of interest typically range from 5 µm to 30 µm (e.g., hepatocytes ~ 15–30 µm, inflammatory cells ~ 5–15 µm). These sizes correspond to diffusion times of 5–70 ms, which can be readily achieved using a combination of OGSE (oscillating gradient spin echo) and PGSE (pulsed gradient spin echo) measurements on clinical MRI scanners. This allows for the assessment of liver microstructure by measuring water diffusion rates across multiple time scales. Therefore, the JOINT method was used in the current work which combines PGSE and OGSE acquisitions and more importantly, it considers the influences of transcytolemmal water exchange to provide a more robust estimation of mean cell size and cell density19.
However, implementing MR cytometry in the liver presents unique challenges due to the tissue’s high perfusion rate and blood volume fraction. Signal dephasing in the vasculature and increased cell membrane permeability in liver disease36 can further complicate measurements. To address these issues, we extended the biophysical model to minimize interferences from blood perfusion and water exchange between intra- and extracellular compartments34, resulting in more accurate estimations of cell size and cell density (details provided in the supplemental materials21).
Validation using histology-based simulations
This study utilizes a Finite Difference (FD) method37 to simulate diffusion signals for compartmental tissue structures derived from segmented histological images using MATI, an in-house diffusion MRI simulation toolbox. Examples of segmentations for normal, steatotic, and stromal (inflammatory and fibrotic) liver tissues are provided in Supplementary Fig. 1. The tissue structures consist of three impermeable compartments, including fat vacuoles, restricted intracellular spaces excluding fat content, and extracellular spaces. Diffusivities for intracellular spaces excluding fat content and extracellular spaces are 1.53 and 2 μm2/ms, respectively. The proton density of intracellular spaces excluding fat content and extracellular spaces was set to homogeneous, while that of fat vacuoles was set to zero, ensuring that they function solely as restrictive barriers. Homogeneous T2 relaxation times were set for all three compartments for simplicity. The PGSE and OGSE acquisition parameters are the same as those in the in vivo MR cytometry protocol described in section 2.4. For each pathology, six segmented histological images (2000 x 2000 pixels with a resolution of 0.5 x 0.5 µm2 per pixel) were used to generate six sets of diffusion data. Rician noise at three SNR levels (10, 20, and 50) were added to the simulated diffusion signals. cytometry analysis was conducted afterwards.
Validation using ex vivo MR cytometry and histology analysis
Six human liver tissue samples, including normal liver (n = 3) and samples with MASH (n = 3), with weights ranging from 1 to 15 grams were obtained from the Western Division of the Cooperative Human Tissue Network at Vanderbilt University Medical Center. All the samples were immersed in 10% neutral buffered formalin for one week and then transferred to PBS solution for 24 h before MR imaging. Each sample was embedded in a 3D-printed holder (Supplementary Fig. 2) with 4% agarose for MRI measurements. This specially-designed sample holder has evenly spaced slots with a slot width of 0.5 mm (the width of a razor blade) and 5 mm between slots. The 4% agarose-filled slots can be easily identified on MR images, which serve as landmarks for accurate slice coregistration between histology and MRI-derived parametric maps. Both H&E and β-catenin (a cell membrane marker) stainings were performed to visualize nuclei and cell boundaries, respectively, on histology images to estimate hepatocyte sizes and cellularities (number of nuclei cross-sections per mm2).
Ex vivo imaging protocol
MRI acquisitions were performed using a Varian/Agilent 4.7 T scanner (Palo Alto, California, USA). For PGSE experiments, diffusion gradient duration/separation were δ/Δ = 3/11 and 3/31 ms. OGSE acquisitions used a frequency of 50 Hz with δ / Δ = 20/25 ms. For STEAM experiments, diffusion gradient duration/separation were δ/Δ = 3/71 ms. Five b-values (0, 250, 500, 750, and 1000 s/mm2 were used. Other imaging parameters were: slice thickness = 1 mm, slice numbers either 3 or 5 depending on the size of samples, in plane resolution = 0.5 x 0.5 mm, TR = 2 s, and TE = 55 ms.
Co-registration between histology and ex vivo MRI
A 3-step approach was performed to co-register histology and ex vivo MR images.
Step 1. Two continuous 5 µm sections were obtained from the surface of each paraffin-embedded tissue block and were stained with H&E and β-catenin, respectively. Note that our customized tissue holder allows that all the MR imaging slices were collected from the surface plane of each paraffin-embedded tissue block (Supplementary Fig. 2).
Step 2. All the stained slides were scanned using an Apero Versa 200 slide scanner at 20x to generate high-resolution digital images (0.5 x 0.5 µm2 per pixel). A total of 60 regions-of-interest (ROIs) representing different liver pathologies, including fatty liver tissues (N = 15), stroma (N = 32), and normal liver tissues (N = 13), were drawn on the β-catenin-stained pictures by a liver pathologist (M.K.W). The high-resolution histological images were divided into small sub-images of size 1000 x 1000 pixels. Cellular parameters, such as average cell sizes, cellularities, and fat fractions, were recorded using in-house algorithms written in Matlab.
Step 3. Histological images were registered to MR images using a combination of Iterative Closest Point (ICP)-based rigid transformation included in the Matlab Computer Vision Toolbox and 2D shape nonrigid registration (matlab codes available from http://fr.mathworks.com/matlabcentral/profile/authors/3793616-mohammad-rouhani), which captures both global and local alignment and deformation. ROIs drawn on the histological sections were then transformed to MRI-derived parametric maps using T2W MR images as bases. For each ROI, cellular properties (e.g., cell size and cellularity) derived from histology and IMPULSED were summarized and compared.
In vivo feasibility experiment
The human imaging study was approved by the Institutional Review Board at Vanderbilt University Medical Center (IRB# 231331). Ten subjects were recruited including five healthy subjects and five biopsy-proven MASH patients, with the MASH activity score provided in Table 1. Informed consent to participate in the study were obtained from all the ten subjects.
MR imaging was performed using a Philips Ingenia CX 3 T scanner with a dStream TorsoCardiac coil. A PGSE sequence with δ / Δ = 12/74 ms was used to collect diffusion data at a relatively long diffusion time (70 ms). Shorter diffusion times were achieved using a cosine-modulated trapezoidal OGSE sequence with gradient frequencies of 25 and 50 Hz. Five b values (0, 250, 500, 750, and 1000 s/mm2) were used for PGSE with Δ = 74 ms and 25 Hz OGSE acquisitions. For 50 Hz OGSE acquisitions, four b values (0, 100, 200, and 300 s/mm2) were used. Other imaging parameters were TR / TE = 2000 / 93 ms; in-plane resolution = 4 × 4 mm; 5 slices; slice thickness = 10 mm; NEX = 2; respiratory-gated, single shot EPI; SENSE factor=2; fat suppression with SPAIR. The total scan time ≈ 12 min. The SNRs of b0 images (images acquired without diffusion weighting) are at least 20. Typical imaging parameters were employed for liver PDFF imaging, including 6 echoes, TR = 7.8 ms, and a flip angle of 3° to avoid significant T1 bias, utilizing Philips’ PDFF product (mDIXON Quant). The fat fraction maps were reconstructed directly by the Philips scanner.
MR cytometry analysis
The OGSE and PGSE diffusion data were processed following the pipeline shown in Supplementary Fig. 3. Briefly, all diffusion data underwent four steps, including preprocessing (including registration and denoising), model selection, removal of blood perfusion, and derivation of microstructural maps. For the last step, the constraints for fitting parameters were based on physiologically relevant values21,32: 0 ≤ \(d\) ≤ 30 µm, 0 ≤ \({v}_{{in}}\) ≤ 1, 0 ≤ \({D}_{{in}}\) ≤ 3.0 µm2/ms, 0 ≤ \({{\rm{ADC}}}_{{ex}}\) ≤ 3.0 µm2/ms, and 0 ≤ \({\tau }_{{in}}\) ≤ 1000 ms. Initial values for each fitting parameter were randomly selected from their ranges. All the data processing was performed using a MATLAB-based in-house software package that is available online (https://github.com/jzxu0622/mati). However, we focused only on MRI-derived \(d\) and \({v}_{{in}}\) in this study with detailed explanations provided in the discussion.
For the ex vivo comparisons with histology, cellularity (the number of cells in a unit cross-section area) was calculated as \(2\,\times \,{\left(\frac{3{v}_{{in}}}{2\pi }\right)}^{\frac{2}{3}}/{d}^{2}\) by assuming that livers consist of spherical cells densely-packed on a face-centered-cube grid38,39. Theoretically, the cellularity should be expressed as \(2\,\times \,{\left(\frac{3(1-{f}_{{fat}}){v}_{{in}}}{2\pi }\right)}^{\frac{2}{3}}/{d}^{2}\), where \({f}_{{fat}}\) is the fat fraction. The reason is that in our signal model, \({v}_{{in}}\) represents the ratio of intracellular water volume to the total water volume, which is much smaller than the total cell volume in the presence of fat. However, formalin fixation can alter the distribution and appearance of fat in tissues and lead to a loss of lipids, making it challenging to quantify the lipid content in fixed human specimens using either MRI or histology. For the in vivo experiment, \({D}_{{in}}\) was fixed at 1.58 mm2/s. Fixing \({D}_{{in}}\) has been shown to effectively improve the fitting of other parameters when the diffusion time range and signal-to-noise-ratio are limited17. The cell density was estimated as \((1-{f}_{{fat}})\times {6v}_{{in}}/\pi {d}^{3}\), under the assumption that the cells are spherical in shape. The fat fraction was measured by a standard mDixon method available on Philips MRI scanners.
The primary hypothesis of this study is that MR cytometry can accurately quantify changes in non-fat cell size and cell density associated with inflammation. To test this, imaging voxels were divided into two groups based on specific thresholds for MRI-derived non-fat cell size and cell density. The group characterized by smaller cell sizes and higher densities likely corresponds to inflammatory cells, while the other group is associated with fatty hepatocytes. In this study, voxels with cell size < 10 µm and cell density > 30 × 104/mm3 are hypothesized to be dominated by inflammation. Additionally, the ratio of voxels between these two groups is referred to as the Small Dense Cell Fraction (SDCF).
Statistical analysis
Group differences in i) MRI-derived parameters among different types of liver tissues at different SNR levels; ii) histology and MRI-derived parameters among different types of liver tissues; and iii) MRI-derived SDCF between healthy subjects and MASH patients, were summarized using means and standard errors of the means and compared using one-way analysis of variance (ANOVA) with Bonferroni correction. The correlations between histology and MRI-derived cell sizes, and cellularities, were assessed using Pearson’s tau correlation coefficient.
Data availability
All simulation, ex vivo, and in vivo data are available upon reasonable request.
Code availability
The toolbox for MRI cytometry analysis is available at https://github.com/jzxu0622/mati.
References
Kleiner, D. E. et al. Design and validation of a histological scoring system for nonalcoholic fatty liver disease. Hepatol. Baltim. Md 41, 1313–1321 (2005).
Beers, B. E. V., Daire, J.-L. & Garteiser, P. New imaging techniques for liver diseases. J. Hepatol. 62, 690–700 (2015).
Younossi, Z. M. et al. Global epidemiology of nonalcoholic fatty liver disease—Meta-analytic assessment of prevalence, incidence, and outcomes. Hepatology 64, 73 (2016).
Bebawi, E., Takla, M. & Leonard, J. Nonalcoholic fatty liver disease. CMAJ 195, E909–E909 (2023).
Nonalcoholic Fatty Liver Disease: MR Imaging of Liver Proton Density Fat Fraction to Assess Hepatic Steatosis | Radiology. https://pubs.rsna.org/doi/abs/10.1148/radiol.12120896?journalCode=radiology.
Venkatesh, S. K., Yin, M. & Ehman, R. L. Magnetic Resonance Elastography of Liver: Technique, Analysis and Clinical Applications. J. Magn. Reson. Imaging JMRI 37, 544–555 (2013).
Trout, A. T. et al. Corrected T1 Mapping in Children and Young Adults With Autoimmune Liver Disease: Correlation With Histology. Am. J. Roentgenol. 220, 901–902 (2023).
Tigner, A., Ibrahim, S. A. & Murray, I. V. Histology, White Blood Cell. in StatPearls (StatPearls Publishing, Treasure Island (FL), 2024).
Klaus, J. B. et al. MRI Dixon Fat-Corrected Look-Locker T1 Mapping for Quantification of Liver Fibrosis and Inflammation-A Comparison With the Non-Fat-Corrected Shortened Modified Look-Locker Inversion Recovery Technique. Invest. Radiol. 59, 754–760 (2024).
Alkhouri, N. et al. Decreases in cT1 and liver fat content reflect treatment-induced histological improvements in MASH. J. Hepatol. S0168-8278, 02559–5 (2024).
JCI - Liver inflammation and fibrosis. https://www.jci.org/articles/view/88881.
Cano, R. L. E. & Lopera, H. D. E. Introduction to T and B lymphocytes. in Autoimmunity: From Bench to Bedside [Internet] (El Rosario University Press, 2013).
Jiang, X., Xu, J. & Gore, J. C. Mapping hepatocyte size in vivo using temporal diffusion spectroscopy MRI. Magn. Reson. Med. 84, 2671–2683 (2020).
Liver Cell - an overview | ScienceDirect Topics. https://www.sciencedirect.com/topics/immunology-and-microbiology/liver-cell.
Vaughan-Jackson, A. et al. Density dependent regulation of inflammatory responses in macrophages. Front. Immunol. 13, 895488 (2022).
Panagiotaki, E. et al. Noninvasive quantification of solid tumor microstructure using VERDICT MRI. Cancer Res. 74, 1902–1912 (2014).
Xu, J. et al. Magnetic resonance imaging of mean cell size in human breast tumors. Magn. Reson. Med. 83, 2002–2014 (2020).
Jiang, X. et al. In vivo imaging of cancer cell size and cellularity using temporal diffusion spectroscopy. Magn. Reson. Med. 78, 156–164 (2017).
Jiang, X., Devan, S. P., Xie, J., Gore, J. C. & Xu, J. Improving MR cell size imaging by inclusion of transcytolemmal water exchange. NMR Biomed. 35, e4799 (2022).
Reynaud, O. et al. Pulsed and oscillating gradient MRI for assessment of cell size and extracellular space (POMACE) in mouse gliomas. NMR Biomed. 29, 1350–1363 (2016).
Jiang, X., Li, H., Devan, S. P., Gore, J. C. & Xu, J. MR cell size imaging with temporal diffusion spectroscopy. Magn. Reson. Imaging 77, 109–123 (2021).
Turgeon, M. L. Clinical hematology: theory and procedures. in 67 (Lippincott Williams & Wilkins, 2005).
Wilson, Z. E. et al. Inter-individual variability in levels of human microsomal protein and hepatocellularity per gram of liver. Br. J. Clin. Pharmacol. 56, 433–440 (2003).
Quantitative digital pathology enables automated and quantitative assessment of inflammatory activity in patients with autoimmune hepatitis - PubMed. https://pubmed.ncbi.nlm.nih.gov/38524918/.
Steidle, G., Eibofner, F. & Schick, F. Quantitative diffusion imaging of adipose tissue in the human lower leg at 1.5 T. Magn. Reson. Med. 65, 1118–1124 (2011).
Tsuchida, T. & Friedman, S. L. Mechanisms of hepatic stellate cell activation. Nat. Rev. Gastroenterol. Hepatol. 14, 397–411 (2017).
Kordes, C., Sawitza, I., Götze, S., Herebian, D. & Häussinger, D. Hepatic stellate cells contribute to progenitor cells and liver regeneration. J. Clin. Invest. 124, 5503–5515 (2014).
Zhang, M. & Zhang, S. T Cells in Fibrosis and Fibrotic Diseases. Front. Immunol. 11, 1142 (2020).
T cell migration in microchannels densely packed with T cells | Scientific Reports. https://www.nature.com/articles/s41598-019-43569-w.
Dongiovanni, P., Fracanzani, A. L., Fargion, S. & Valenti, L. Iron in fatty liver and in the metabolic syndrome: a promising therapeutic target. J. Hepatol. 55, 920–932 (2011).
Jiang, X. et al. Joint estimation of compartment-specific T2 relaxation and tumor microstructure using multi-TE IMPULSED MRI. Magn. Reson. Med. 93, 96–107 (2025).
Li, H., Jiang, X., Xie, J., Gore, J. C. & Xu, J. Impact of transcytolemmal water exchange on estimates of tissue microstructural properties derived from diffusion MRI. Magn. Reson. Med. 77, 2239–2249 (2017).
Jiang, X. et al. Quantification of cell size using temporal diffusion spectroscopy. Magn. Reson. Med. 75, 1076–1085 (2016).
Time-Dependent Influence of Cell Membrane Permeability on MR Diffusion Measurements - Li - 2016 - Magnetic Resonance in Medicine - Wiley Online Library. https://onlinelibrary.wiley.com/doi/full/10.1002/mrm.25724.
Li, Y. T. et al. Liver intravoxel incoherent motion (IVIM) magnetic resonance imaging: a comprehensive review of published data on normal values and applications for fibrosis and tumor evaluation. Quant. Imaging Med. Surg. 7, 59–78 (2017).
Kaplowitz, N. Mechanisms of liver cell injury. J. Hepatol. 32, 39–47 (2000).
Xu, J., Does, M. D. & Gore, J. C. Numerical study of water diffusion in biological tissues using an improved finite difference method. Phys. Med. Biol. 52, N111–N126 (2007).
Xu, J., Does, M. D. & Gore, J. C. Sensitivity of MR Diffusion Measurements to Variations in Intracellular Structure: Effects of Nuclear Size. Magn. Reson. Med. Off. J. Soc. Magn. Reson. Med. Soc. Magn. Reson. Med. 61, 828–833 (2009).
An Efficient Computational Approach to Characterize DSC-MRI Signals Arising from Three-Dimensional Heterogeneous Tissue Structures | PLOS ONE. https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0084764.
Acknowledgements
This work was funded by NIH grants R01 CA109106, CA269620, R01DK135950, and CA270731.
Author information
Authors and Affiliations
Contributions
X.J., M.J.I., M.K.W., J.X. and J.C.G. contributed to the design of the experiments, X.J. performed and evaluated the MRI experiments. M.K.W drew the ROIs of different liver pathologies and oversight the histological analysis. M.L. and X.Y. designed and produced the sample holder. M.J.I. and G.P. oversight the patient recruitment. X.J. wrote the manuscript. M.J.I., M.K.W., M.L., X.Y, J.X. and J.C.G. contributed to the manuscript. All authors have read and approved the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Jiang, X., Washington, M.K., Izzy, M.J. et al. Noninvasive assessment of liver inflammation in metabolic dysfunction associated steatohepatitis using MR cytometry. npj Imaging 3, 17 (2025). https://doi.org/10.1038/s44303-025-00080-4
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s44303-025-00080-4
