
Abstract
Individuals with a family history of premature coronary heart disease (CHD) have increased cardiac morbidity and mortality, which may motivate them to modify their health behaviours. This analysis examines whether patients with self-reported family history of premature CHD experiencing an acute coronary syndrome (ACS) were more likely to have their risk factors and health behaviours under control at 12 months post ACS. Data from the TEXTMEDS study were used to estimate the association between self-reported family history of premature CHD and blood pressure control, LDL cholesterol control, BMI, exercise and smoking status at 12 months post ACS. The study cohort consisted of 1423 participants (mean age 58.0 ± 10.67, 79.2% male), with 556 (39.1%) reporting a family history of premature CHD, while 867 (60.9%) reported no family history. No evidence from this analysis suggests that patients with knowledge of their family history were more likely to achieve better risk factor control. Novel strategies for risk factor control in this high-risk population is required to improve secondary prevention.
Similar content being viewed by others
Introduction
Coronary heart disease (CHD) is a condition which confers a significant health burden; it is associated with 17.8 million deaths annually and is also the third leading cause of mortality globally1. It is a major cause of mortality among Australians - in 2019 CHD was estimated to underly 11% of all deaths and 42% of all deaths from cardiovascular diseases (CVD)2. Individuals with a family history of CHD are at a higher risk of CVD morbidity and mortality compared to those without a family history throughout their lifetime3. Furthermore, a family history of premature CHD is associated with an increased risk of disease recurrence such as recurrent myocardial infarction after an acute coronary syndrome (ACS)4.
Health-related risk perception refers to an individual’s view on their susceptibility to particular health threats or diseases5. It is regarded by many to be an important factor in individuals’ modification of unhealthy behaviours. Evidence suggests that there is a direct correlation between individual risk perceptions and their behaviours in health6. Previous studies have shown a direct correlation between perception of cardiovascular risk and health behaviours. Cross-sectional data suggest an association between knowledge and preventative actions including exercise, diet and weight management7,8. There is some evidence to indicate that individuals with a family history of premature CHD are aware of their increased risk9. Despite this, associations between family history of disease and risk perception were unclear in many other studies, both in general and for CHD specifically10,11,12. This is particularly true for individuals who are disease-free13. Hence, establishment of the relationship between family history and perception of their cardiovascular risk is an important factor to consider in the management strategies of this population of patients. This analysis aims to investigate if a self-reported family history of premature CHD in the context of a confirmed ACS diagnosis is associated with behavioural and risk factor control changes. The analysis utilises data from TEXTMEDS (Text Messages to Improve Medication Adherence and Secondary Prevention After Acute Coronary Syndrome) randomised clinical trial14.
Results
This study included 1423 participants from the TEXTMEDS study, having excluded one participant due to non-response to family history of premature CHD question. A total of 556 (39.1%) participants reported a family history of premature CHD. The mean age of participants was lower in those with a family history compared with those without (mean age 56 ± 10.83 years v 59 ± 10.44 years) and women in the sample were more likely to have a positive family history as opposed to not having a family history (61.2% v 46.9%) (Table 1). Baseline BMI and rates of obesity were significantly higher in those with a family history. In addition, there was an increased prevalence of sleep apnoea and depression in the family history group. The proportion of participants prescribed antihypertensive and lipid-lowering agents were similar across the two groups, as was adherence of antihypertensives and statins in the 12-month period the primary study took place (Table 1).
Outcomes by family history
A multiple bar chart of the percentage of outcome achievement by family history has been presented (Fig. 1). Initial unadjusted logistic regression models suggested no association between family history status and any of the five outcomes at 12 months (Table 2).

Abbreviations used: FHx family history, CHD coronary heart disease, BP blood pressure, LDL low-density lipoprotein, BMI body mass index.
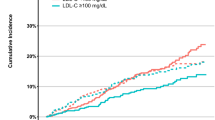
In the final model for achieving target blood pressure, history of hypertension was the only covariate independently associated with the outcome. In the adjusted model, no association was found between family history and achieving blood pressure target at 12 months (adjusted odds ratio (aOR) = 0.92, 95% CI = 0.68, 1.24). Smoking, drinking, marital status, physical disability, baseline HDL cholesterol, lipid agent use, diabetes and hyperlipidaemia were associated with achieving LDL cholesterol target. In the adjusted model no association was found between family history and achieving LDL cholesterol target (aOR = 0.92, 95% CI = 0.70, 1.21). In the final model for achieving target BMI, ethnicity, employment, baseline HDL cholesterol, baseline triglyceride, hypertension, diabetes, hyperlipidaemia, sleep apnoea and obesity were independent predictors. In the adjusted model there was no association between family history and achieving BMI < 25 (aOR = 0.99, 95% CI = 0.59, 1.64). The final model for achieving exercise target, included BMI, alcohol consumption, employment, education, marital status, prior cardiovascular events, hypertension, obesity, depression, chronic kidney disease and SF12 quality of life physical health scores. In the final adjusted model, no association was found between family history and exercise target (aOR = 1.29, 95% CI = 0.97, 1.73). The final model for achieving non-smoking target included education level, marital status and depression and no association was found for family history and non-smoking at 12 months (aOR = 0.88, 95% CI = 0.59, 1.31) (Table 2). Similar findings were found on all four outcomes excluding smoking when analysed with a continuous regression model. Multiple comparison adjustment was not performed due to the exploratory nature of this analysis that required further hypothesis testing had there been clinically significant outcomes.
Discussion
In this secondary analysis of the TEXTMEDS study, we found no association between family history of CHD and risk factor control (blood pressure, LDL cholesterol, BMI, exercise, smoking) at 12 months after their ACS. We found that roughly a third of the cohort who have had an ACS had a family history of premature CHD. Participants with a family history of premature CHD were younger and more likely to be female but were otherwise like those without a family history of CHD, with comparable levels of hypertension, hyperlipidaemia, exercise, BMI and smoking.
Our findings suggests that knowledge of family history may not influence behaviour change with respect to cardiovascular risk factors in patients with a recent ACS, despite the expectation that patients with knowledge of their family history perhaps should perceive their risk to be higher. The absence of an improvement in risk factor control compared to the participant group without a family history after baseline adjustment is consistent with some prior studies studying the association of only family history or only prior ACS to behavioural changes. In study populations with a family history of premature CVD, cross-sectional and case-control data examined by Ton et al. found that approximately half of the siblings and offspring of patients that suffered from CHD believed their risk of CHD to be equal to or less than the general population11. Ter Hoeve demonstrated that in patients with a past ACS controllable risk factors e.g. cholesterol, BMI were often underestimated, with external factors being an emphasis e.g. stress, work as the cause of their ACS; even in those who identified controllable risk factors as a major contributor, rates of programme participation to control these factors remained suboptimal15. Andersson et al. explored the effects that a personal experience of disease or a family history of CVD may have on a variety of risk factors i.e. smoking, exercise, BMI levels16. While a difference was seen in smoking, as a result of a personal experience to illness, there were no differences observed due to family history. Elis et al. investigated cross-sectional data consisting of mostly young adults, and results showed that smoking and exercise habits remain unchanged between groups with and without a family history of CVD17.
Risk perception from a family history, similarly, did not associate itself with risk factor and behaviour management. Imes and Lewis’ systematic review consisting of 25 studies between 1986 and 2012 of mostly cross-sectional studies concluded that both an awareness of family history and the perception of one’s own risk for CVD was not sufficient to drive health behaviour changes to a significant level10. This was true for both smoking and exercise, where Hunt’s study found that apart from the youngest cohort of participants interviewed (around age 23), those with a family history of CVD, while aware of their increased risk, did not think that reducing smoking and increasing exercise was of more importance to them18. Also mentioned in the systematic review was Kavanagh’s study; attempts at adhering to exercise and weight loss regimes were suboptimal at 50% or lower in participants who had a first degree relative with premature CHD19. Tavares, Oliveira and Lopes’ study consisting of questionnaires delivered to individuals within the Portuguese general population further failed to show any dissimilarity in care-seeking and health behaviour between individuals with and without a family history20. Studies investigating differences in the same biological factors evaluated in this study according to the presence of family history reported no significant differences in the achievement of systolic blood pressure, diastolic blood pressure and LDL cholesterol targets21,22.
Conversely, studies involving an intervention targeting at improving risk factor control specifically in individuals with family history demonstrated efficacy. Goldfarb et al. conducted a systematic review and meta-analysis on primary screening and intervention of cardiac disease in individuals with a family history of cardiac disease, which suggested that active intervention in these individuals may be effective for risk factor or health behaviour modification23. Similarly, a text message randomised controlled trial undertaken by Ruffin et al. targeting individuals’ familial risk of six common diseases including CHD showed modest changes in lifestyle factors with increases in exercise and diet habits24. However, these positive studies consisted of a targeted effort to increase risk perception in the specific population with a family history, rather than just evaluating the sole effect of family history on health behaviour and risk factor control over time. On the other hand, this can also mean that familial risk is possibly a contributing factor to an individual’s amenability to modify their own lifestyle choices.
The underlying reason behind this lack of association between family history and risk factor control is likely to be multifactorial and complex. One of the possible explanations may be that the interpretation of what a family history of CHD entails can differ between the general public and that of clinicians. Family members of premature CHD patients may attempt to find dissimilarities between their lifestyles and attribute premature CHD to these external factors, rather than an intrinsic tendency to develop CHD25. It is also possible that the degree of risk perceived from having prior adverse cardiovascular events is similar or greater than that from a family history, which can result in no appreciable differences in risk factor control between the two groups of participants26. It is also possible that inherently, risk factor control is more difficult to achieve in these individuals in which poor control of these risk factors is what contributed originally to a family history of premature CHD. It is worth noting that an inability, rather than an unwillingness to control risk factors may be relevant in participants with a family history; factors such as socioeconomic disadvantage is associated with poorer risk factor management27,28, and this may contribute to a higher frequency of premature CHD in family members.
The main strength in the current study is that the data was obtained from a randomised clinical trial with uniformly collected data points on risk factor outcomes for all participants at 12 months. These data were collected from multiple states within Australia, making the results more generalisable within the country. A limitation of this study is that family history is obtained by self-report and hence may have been over or under-reported, however we are interested in patients who know their family history so self-reporting is appropriate in this case. There were missing data at the 12-month follow-up timepoint which resulted in exclusion of individuals in the final data analysis. This was 14.7% for blood pressure, 18.8% for LDL cholesterol, 15.4% for exercise and 18.3% for BMI (Supplementary Tables 2–6). Comparison of individuals with and without missing values suggested that the former group of individuals were less likely to be employed or receive higher education. They were also more associated with comorbidities at baseline such as physical disability, diabetes, sleep apnoea and depression. This may introduce selection bias into the final model which could have affected the results. A further sensitivity analysis was conducted where each missing value for each outcome were imputed and replaced with a negative outcome which showed no changes in the results. In-depth interviews would be useful for future studies to fully understand whether family history acts as a catalyst to improve cardiovascular risk factors through risk factor control and lifestyle behaviours.
This study found evidence that among patients who have experienced an ACS, a family history of premature CHD is not associated with differences in the control of cardiovascular risk factors a year post ACS. Given the high lifetime risk that a history of premature CHD is associated with, further research is needed to understand how to improve the cardiovascular risk factor management and control of this group. Monitoring and managing risk factors are important in all ACS patients and particularly important in those with a family history of premature CHD due to their elevated risk.
Methods
The TEXTMEDS study recruited 1424 participants as described within the primary study protocol paper29. Briefly, the primary study was a single-blind randomised controlled trial of patients after an episode of ACS. Patients either received usual secondary prevention care according to the treating clinician (control) or received additional weekly text messages with medication and lifestyle advice for the time period of a year. The primary study discovered that medical adherence did not improve as a result of the additional intervention but had small effects on BMI and dietary habits.
As per the primary study, patients were screened from metropolitan and rural hospitals and medical centres across five states in Australia with a confirmed diagnosis of an ACS on admission to the hospital. This was defined as follows:
-
1.
Acute myocardial infarction defined by the Third Universal Definition of myocardial infarction30 OR
-
2.
Admitted to hospital with symptoms consistent with cardiovascular ischaemia but not meeting requirements of the criteria above and one of (a) angiography suggestive of CHD (narrowing of at least one coronary artery greater than 50%) (b) prior coronary artery bypass graft surgery (c) prior percutaneous coronary intervention.
Additional inclusion criteria were based on participants’ ability to give consent, possession of a mobile device capable of text function, adequate command of English, as well as a life expectancy of more than 6 months. This analysis includes participants from TEXTMEDS who provided data regarding a family history of premature CHD. Consent has been obtained from the participants at the time of the primary study for the data collected to be discussed and/or published in peer-reviewed journals.
Statistical power
We consider an improvement of 10% to be clinically significant. To detect a relative risk ratio of 10% meeting the blood pressure target from a baseline of 70% in those without a family history to 77% of those with a family history, the main study of 1423 participants will have 85% power.
Data collection
Data collection has been previously described29. In summary, data were collected at baseline and follow-up assessments were at 6 months and 12 months. The baseline and 12-month visits were conducted in-person, while the 6-month visit was conducted via telephone. Baseline family history of premature CHD was defined as a diagnosis of CHD in at least one first degree male relative under the age of 55, or one first degree female relative under the age of 65 years31.
In this study the outcomes are achieving target blood pressure, LDL cholesterol, body mass index (BMI) and smoking status at 12 months. The data for these five outcomes were not collected at the 6-month follow-up appointments. Thresholds defining risk factor control were blood pressure lower than 140/90 mmHg, LDL cholesterol concentration lower than 1.8 mmol/L and BMI lower than 25 kg/m2; these are based on the standard definition of hypertension, optimal LDL cholesterol levels for patients with past cardiovascular events and the definition of overweight as follows:
Hypertension: grade 1—140–159 mmHg systolic or 90–99 mmHg diastolic, grade 2— 160–179 mmHg systolic or 100–109 mmHg diastolic, grade 3—180 mmHg systolic or 110 mmHg diastolic and above32.
LDL cholesterol: For patients with past ACS, the recommended LDL-C goal is ≤1.8 mmol/L (≤70 mg/dL) while commenced on anti-lipid/statin therapy33,34.
BMI: Based on current WHO definition of overweight (BMI ≥ 25)35.
GPAQ (Global Physical Activity Questionnaire) score ≥ 600 MET-minutes per week was used to identify participants who were exercising regularly. A GPAQ score of 600 is equal to 75 min of vigorous activity, 150 min of moderate activity or an equivalent combination of both reaching 600 MET-minutes per week36.
Statistical method
Data analysis has been performed on R version 4.3.1. Family history and each outcome of interest was compared initially with unadjusted Welch Two Sample t tests and Pearson’s Chi-squared tests. Statistically relevant baseline factors within the TEXTMEDS study dataset were identified for each outcome of interest using univariate logistic regression (Supplementary Tables 2–6). The statistical method of LASSO (Least Absolute Shrinkage and Selection Operator) was then utilised to further identify and narrow down relevant covariates37. To summarise briefly, this statistical method selects only for covariates that can better predict each of the outcomes being investigated in our study. The covariates that remain within the model after the LASSO method were then included and adjusted for within the final model for each outcome. The final model for each outcome was adjusted by age, sex, intervention in the primary study, baseline value for each outcome and the covariates that were identified using LASSO. In addition, analyses were conducted using the continuous outcome variables in a regression model for all outcomes except smoking status.
This project was approved by the Western Sydney Local Health District Human Research Ethics Committee (approval HREC2012/12/4.1 [3648] AU RED HREC/13/WMEAD/15); the primary study has been listed on the Australian New Zealand Clinical Trials Registry (ACTRN12613000793718).
Data availability
Data are available on request and approval by the TEXTMEDS investigators.
Code availability
Code for the data analysis is available on request and approval by the corresponding authors.
References
Brown, J. C., Gerhardt, T. E. & Kwon, E. in StatPearls (StatPearls Publishing Copyright © 2024, StatPearls Publishing LLC., 2024).
Australian Institute of Health and Welfare. Heart, stroke and vascular disease: Australian facts. https://www.aihw.gov.au/reports/heart-stroke-vascular-diseases/hsvd-facts/contents/all-heart-stroke-and-vascular-disease/coronary-heart-disease (2023).
Bachmann, J. M., Willis, B. L., Ayers, C. R., Khera, A. & Berry, J. D. Association between family history and coronary heart disease death across long-term follow-up in men: the Cooper Center Longitudinal Study. Circulation 125, 3092–3098 (2012).
Wahrenberg, A. et al. Cardiovascular family history increases the risk of disease recurrence after a first myocardial infarction. J. Am. Heart Assoc. 10, e022264 (2021).
Ferrer, R. & Klein, W. M. Risk perceptions and health behavior. Curr. Opin. Psychol. 5, 85–89 (2015).
Sheeran, P., Harris, P. R. & Epton, T. Does heightening risk appraisals change people’s intentions and behavior? A meta-analysis of experimental studies. Psychol. Bull. 140, 511–543 (2014).
Al Hamarneh, Y. N., Crealey, G. E. & McElnay, J. C. Coronary heart disease: health knowledge and behaviour. Int J. Clin. Pharm. 33, 111–123 (2011).
Zaman, M. J. et al. Socio-economic distribution of cardiovascular risk factors and knowledge in rural India. Int J. Epidemiol. 41, 1302–1314 (2012).
Patel, M. J. M. D. et al. Implications of family history of myocardial infarction in young women. Am. Heart J. 154, 454–460 (2007).
Imes, C. C. & Lewis, F. M. Family history of cardiovascular disease, perceived cardiovascular disease risk, and health-related behavior: a review of the literature. J. Cardiovasc. Nurs. 29, 108–129 (2014).
Ton, T. G. et al. Knowledge, perception, and behaviors of relatives of people with premature heart disease: a systematic literature review. Circulation 124, 958–964 (2011).
Wang, C. et al. Family history assessment: impact on disease risk perceptions. Am. J. Prev. Med. 43, 392–398 (2012).
Acheson, L. S. et al. Family history and perceptions about risk and prevention for chronic diseases in primary care: a report from the family healthware impact trial. Genet. Med. 12, 212–218 (2010).
Chow, C. K. et al. Text messages to improve medication adherence and secondary prevention after acute coronary syndrome: the TEXTMEDS randomized clinical trial. Circulation 145, 1443–1455 (2022).
Ter Hoeve, N. et al. Know your numbers: risk factor perceptions and lack of control in patients after an acute coronary syndrome. Eur. J. Prev. Cardiol. 27, S87 (2020).
Andersson, P., Sjöberg, R. L., Ohrvik, J. & Leppert, J. The effects of family history and personal experiences of illness on the inclination to change health-related behaviour. Cent. Eur. J. Public Health 17, 3–7 (2009).
Elis, A. et al. Family history of cardiovascular disease does not predict risk-reducing behavior. Eur. J. Cardiovasc. Prev. Rehabil. 15, 325–328 (2008).
Hunt, K., Davison, C., Emslie, C. & Ford, G. Are perceptions of a family history of heart disease related to health-related attitudes and behaviour?. Health Educ. Res. 15, 131–143 (2000).
Kavanagh, T., Shephard, R. J., Hamm, L. F., Mertens, D. J. & Thacker, L. Risk profile and health awareness in male offspring of parents with premature coronary heart disease. J. Cardiopulm. Rehabil. 20, 172–179 (2000).
Tavares, P., Oliveira, A. & Lopes, C. Family history of coronary heart disease, health care and health behaviors. Rev. Port. Cardiol.30, 703–710 (2011).
Slattery, M. L. et al. Family health history and health behaviors in Alaska native and American Indian people. J. Health Care Poor Underserved 20, 678–694 (2009).
Kip, K. E., McCreath, H. E., Roseman, J. M., Hulley, S. B. & Schreiner, P. J. Absence of risk factor change in young adults after family heart attack or stroke: the CARDIA Study. Am. J. Prev. Med. 22, 258–266 (2002).
Goldfarb, M. et al. Screening strategies and primary prevention interventions in relatives of people with coronary artery disease: a systematic review and meta-analysis. Can. J. Cardiol. 31, 649–657 (2015).
Ruffin, M. T. T. et al. Effect of preventive messages tailored to family history on health behaviors: the Family Healthware Impact Trial. Ann. Fam. Med. 9, 3–11 (2011).
Hunt, K., Emslie, C. & Watt, G. Lay constructions of a family history of heart disease: Potential for misunderstandings in the clinical encounter?. Lancet 357, 1168–1171 (2001).
Grauman, Å, Viberg Johansson, J., Falahee, M. & Veldwijk, J. Public perceptions of myocardial infarction: do illness perceptions predict preferences for health check results. Prev. Med. Rep. 26, 101683 (2022).
Leng, B., Jin, Y., Li, G., Chen, L. & Jin, N. Socioeconomic status and hypertension: a meta-analysis. J. Hypertens. 33, 221–229 (2015).
Anekwe, C. V. et al. Socioeconomics of obesity. Curr. Obes. Rep. 9, 272–279 (2020).
Chow, C. K. et al. TEXT messages to improve MEDication adherence and Secondary prevention (TEXTMEDS) after acute coronary syndrome: a randomised clinical trial protocol. BMJ Open 8, e019463 (2018).
Thygesen, K. et al. Third universal definition of myocardial infarction. Eur. Heart J. 33, 2551–2567 (2012).
Wahrenberg, A. et al. Family history of coronary artery disease is associated with acute coronary syndrome in 28,188 chest pain patients. Eur. Heart J. Acute Cardiovasc. Care 9, 741–747 (2020).
Gabb, G. What is hypertension? Aust. Prescr. 43, 108–109 (2020).
Atar, D. et al. New cardiovascular prevention guidelines: How to optimally manage dyslipidaemia and cardiovascular risk in 2021 in patients needing secondary prevention?. Atherosclerosis 319, 51–61 (2021).
Sakuma, M. et al. Optimal target of LDL cholesterol level for statin treatment: challenges to monotonic relationship with cardiovascular events. BMC Med. 20, 441 (2022).
World Health Organization. SuRF Report 2 (World Health Organization, 2005).
World Health Organization. (ed Prevention of Noncommunicable Diseases Department) Global Physical Activity Questionnaire (GPAQ) Analysis Guide (20 Avenue Appia, 1211 Geneva 27, Switzerland, 2021).
Tibshirani, R. Regression shrinkage and selection via the lasso. J. R. Stat. Soc. Ser. B Stat. Methodol.58, 267–288 (1996).
Acknowledgements
J.R. is funded by a National Health and Medical Research Council (NHMRC) Investigator Grant (GNT2007946). C.C. is funded by a NHMRC Investigator grant (APP1195326).
Author information
Authors and Affiliations
Contributions
C.C. led the conception of the research topic. D.J. conducted the data transformation and analysis, with extensive assistance from H.M., S.M. and D.Q. D.J. drafted the manuscript, with edits and reviews from all authors. C.C., J.R., H.K., G.H., D.B., J.A., R.B., D.C., N.C., M.F., C.J., N.K., A.M., M.M., R.P., P.S., C.H., P.T., S.S., A.V. and S.J. was part of the team that conceived, designed and delivered the primary TEXTMEDS study of which the dataset of this study came from.
Corresponding authors
Ethics declarations
Competing interests
Author C.C. is an Associate Editor at npj Cardiovascular Health. C.C. was not involved in the journal’s review of, or decisions related to, this manuscript.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Jeng, D.YH., Min, H., Marschner, S. et al. Family history of premature CHD and risk factor control in patients with a recent ACS. npj Cardiovasc Health 2, 37 (2025). https://doi.org/10.1038/s44325-025-00060-y
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s44325-025-00060-y
