
Abstract
Formalin fixation and paraffin embedding are conventional tissue preservation and processing methods used for histologic diagnosis in over 90% of cases. However, formalin fixation has three disadvantages: (1) slow fixation (16–24 h) hinders intraoperative decision making, (2) slow quenching of enzymatic activity causes RNA degradation, and (3) extensive molecule modification affects protein antigenicity. Applying high-frequency, high-intensity ultrasound to the formalin fixative cuts fixation time to 5–15 min. Fixation of various tissues such as lymph node, brain, breast, and prostate suggests that, compared to the conventional method, implementation of ultrasound retains superior and more uniform tissue morphology preservation. Less protein antigenicity is altered so that rapid immunohistochemical reactions occur with higher sensitivity and intensity, reducing the need for antigen retrieval pretreatment. Better RNA preservation results in stronger signals in in situ hybridization and longer RNA fragments extracted from fixed tissues, probably due to rapid inhibition of endogenous RNase activity. Molecules extracted from ultrasound-fixed tissues are of greater integrity and quantity compared to conventionally fixed tissues, and thus better support downstream molecular analyses. Overall, ultrasound-facilitated tissue preservation can provide rapid and improved morphological and molecular preservation to better accommodate both traditional and molecular diagnoses.
Similar content being viewed by others


Main
Fixation is the first step in tissue preservation for pathological diagnosis. Fixation arrests autolysis and putrefaction, coagulates soluble and structural proteins, fortifies tissues against the deleterious effects of subsequent processing, and facilitates staining. Fixation of tissues can be accomplished by formalin to form cross-links in tissue,1, 2 alcohol and acetone to coagulate and dehydrate tissues,3, 4 cryopreservation to inactivate endogenous enzymes, and microwave energy to thermally denature enzymes and fix tissue.5, 6 The conventional tissue fixation method involves placing tissue samples in 10% neutral-buffered formalin for 16–24 h, followed by overnight (18–24 h) processing. This standard or conventional formalin fixation and paraffin embedding practice has not changed for over 50 years and is used in over 90% of cases in hospitals and clinical settings because it provides superior morphological details and high consistency under various conditions, and offers simple and economical processing and handling.
For the past 30 years, dynamic changes in molecular biology have accelerated technological advancements in medical practice. Application of immunohistochemistry, in situ hybridization, fluorescent in situ hybridization, polymerase chain reaction (PCR), reverse transcription (RT)-PCR, in situ PCR, laser capture microdissection,7 cDNA and tissue microarrays8, 9 have revolutionized pathological diagnosis. Initially, molecular techniques were limited to fresh or frozen tissues because conventional formalin fixation modifies macromolecules, altering protein antigenicity and rendering proteins and DNA/RNA difficult to extract for further molecular testing.10, 11, 12 The slow, time-consuming process of formalin fixation also causes RNA fragmentation by enzymatic degradation, obstructing RNA-based diagnosis. Frozen sections, on the other hand, maintain relatively poor morphology, insufficient for a definitive pathologic diagnosis.13 Frozen tissues also require large and expensive storage facilities, which make their use prohibitive for most medical practices. Since no preservation method currently provides both superior morphology and a high quantity of soluble macromolecules suitable for molecular analysis, conventional formalin-fixed and paraffin-embedded tissue is most widely used for histological diagnosis, while frozen tissue is mainly used for molecular diagnosis.
An affordable technology capable of rapid macromolecular preservation for superior morphology, and better preservation of RNA and protein integrity, would be a significant advancement in medical research and practice. Different approaches have been studied in an effort to enhance the quality of histology, antigen preservation, and fixation speed. Alternative fixatives,3, 4 modified fixation procedures,11 application of microwave,6, 14 or combinations of microwave and ultrasound15 have been tested. Ultrasound, per se, does not preserve tissue, but is often used for tissue disaggregation because of its high tissue-penetration properties. Thus, ultrasound may be used in combination with fixatives to increase tissue penetration dramatically and, consequently, the speed of fixation.
Ultrasound was first applied to fixation solutions by Buchmuller's group in Germany in the 1950s as a means of improving the efficiency of tissue fixation.16 Since the 1960s, a few groups have reported using ultrasound to increase the speed of fixation17 and processing18, 19 and to accelerate immunoassay20, 21 and staining.22 Most of these studies used commercially available ultrasound generators and involved the use of low-frequency ultrasound (approximately 40 kHz), which led to controversial results and frequent tissue damage.15, 18 For the past 20 years, there have been few studies on the use of ultrasound in tissue preservation.
We found that to apply successfully ultrasound to rapid tissue processing without tissue damage, it was critical to maintain ultrasound at high frequency and high intensity, and to control the total energy applied to the tissue. Our prototype employs an adjustable high-intensity (3 to 22 W/cm2) acoustic power and specific high frequency of a 1.6–1.7 MHz ultrasound generator to avoid the tissue destruction that occurs with low-frequency ultrasound. This report presents a series of histological data to demonstrate that ultrasound-facilitated formalin fixation is a faster and better method of tissue fixation. Compared to conventional methods, ultrasound fixation achieves not only rapid tissue–formalin cross-linking, but also rapid quenching of endogenous protease and nuclease activities, resulting in improved histomorphology and superior preservation of protein antigen and nucleic acid integrity. Since the ultrasound fixation technique is still under development and needs further validation, as an initial effort, we focus here on the assessment of morphological preservation (H&E morphology, immunohistochemistry, and in situ hybridization) and extracted molecules in formalin- fixed tissues with and without implementation of ultrasound.
Materials and methods
We follow the general protocols and methods for tissue handling, fixation, processing, embedding, sectioning, H&E staining, immunoreactions, and quality assurance assessments routinely utilized in the Hematopathology, Neuropathology and Genitourinary Pathology laboratories of the Armed Forces Institute of Pathology.
Tissue Preparation
Surgically removed human biopsy tissues, including tonsils from four patients, three lymph node specimens, two lung specimens, two soft tissues, one brain specimen, and 23 prostate biopsies, were obtained from the Walter Reed Army Medical Center within 1–2 h of excision. A total of 58 post-mortem human tissue samples, including breast, pancreas, spleen, liver, brain, and 11 other types of tissues from 13 autopsies were collected within 15–32 h after death. Fresh tissue samples were sectioned into five slices, each 5 mm thick. Three tissue slices were conventionally fixed in 200 ml of 10% neutral-buffered formalin at room temperature, one slice for 30 min, one for 6 h, and one for 22 h. Two tissue slices were fixed with the same amount of buffered formalin with ultrasound irradiation of either 15–30 min at 3–8 W/cm2 or 5–10 min at 8–20 W/cm2. Tissues fixed for a shorter time were left in 75% ethanol until the sample fixed for 22 h was ready to be processed (see Table 1). The fixed slices were then dehydrated in graded ethanol, cleared in xylene, and infiltrated in paraffin in an automatic tissue processor (Tissue Tek, Miles Scientific, Naperville, IL, USA) for 18 h overnight. Paraffin sections were cut at 4–5 μm and stained with H&E. Three certified pathologists independently evaluated the histology of the tissue samples.
Ultrasonic Apparatus: Characteristics and Application
Any ultrasound generator of high frequency and high intensity as specified later in this section might be adapted to achieve similar results. The high-frequency, high-intensity ultrasonic apparatus used in this study is a prototype designed and developed by the first author (WSC) and built by Bio-Quick Inc. (Silver Spring, MD, USA). It consists of a 1.6–1.7 MHz ultrasonic generator with an adjustable intensity output of 3–22 W/cm2. The ceramic transducers were specially designed to disperse ultrasound energy rather than focus on a single point. This prototype was designed for research purposes with a single transducer for individual tissue samples. The tissue to be studied was aligned with the transducer at a distance of 3–5 cm, depending on the tissue size. Ultrasound irradiation was applied continuously to the tissue as the transducer and tissue were immersed in 200 ml of formalin (10% in neutral buffer). Ultrasound energy was monitored by a UW-3 ultrasound wattmeter (Bio-Tek Instruments Inc., Winooski, VT, USA). The temperature increase in tissue and buffer was in proportion to the length of ultrasound irradiation, but was limited to 10°C for 40-min irradiation.
Immunohistochemistry
Fixed tissue sections were stained with commercially available antibodies according to the modified ABC method.23, 24 Tissue sections were deparaffinized, rehydrolized, and rinsed in PBS with or without pretreatment by microwave or pepsin-antigen retrieval, as specified for each antibody. The sections were then blocked with 10% horse and goat serum for 15 min to reduce nonspecific background. Primary antibodies CD20 (1:400), CD3 (1:500), CD45 (1:250), Bcl-2 (1:100), cytokeratin AE1/AE3 (1:400), and immunoglobulin kappa and lambda (1:100K) chains were purchased from DAKO, Carpinteria, CA, USA, while CD5 (1:100) was obtained from Vision BioSystems Inc., Norwell, MA, USA, and alpha-methylacyl-CoA racemase (1:200) from Zeta Co., Sierra Madre, CA, USA. As listed in Table 1, for long immunohistochemistry staining, sections were incubated sequentially with primary antibody for 18 h at room temperature, biotinylated secondary antibody for 30 min at 40°C, 0.3% hydrogen peroxide for 5 min at 40°C, and ABC complex for 30 min. Short immunohistochemistry staining was similar to long immunohistochemistry procedures, except that sections were incubated with the primary antibody, secondary antibody, and ABC complex for 10, 5, and 5 min, respectively. Antibody binding sites were visualized using 3,3′-diaminobenzidine as the chromogenic substrate, and tissue sections were lightly counterstained with hematoxylin. Appropriate multitissue controls were used with each reaction as external positive and negative controls. Negative controls for immunohistochemistry reactions used serum to substrate primary antibodies. The quality of immunohistochemistry staining was graded on five scales from (−) to (++++): (−) indicates lack of staining; (+) indicates weak staining in a small percentage of positive cells; (++) indicates weak staining in the majority of positive cells; (+++) indicates moderate staining in the majority of positive cells; and (++++) indicates strong staining in all positive cells.
mRNA In Situ Hybridization
Tissue sections were deparaffinized as described for immunohistochemistry, and subjected to enzymatic or microwave antigen retrieval pretreatment prior to hybridization. Synthetic oligonucleotide probes specific for mRNA of kappa and lambda immunoglobulin were labeled with fluorescein isothiocyanate (FITC) (sequences provided by BioGenex, San Ramon, CA, USA). The FITC-labeled probe was applied to the section, which was secured by a cover slip and denatured at 100°C for 5 min in a steamer. Slides were allowed to cool and hybridize with the probe at room temperature for 1 h. Sections were given two 3-min washes in 2 × SSC, incubated for 30 min with monoclonal mouse anti-FITC, followed by two 3-min washes in PBS. The slide section was incubated with biotinylated secondary antibody for 30 min at room temperature, followed by two 3-min washes in PBS, and then incubated with streptavidin-biotinylated peroxidase for 30 min. After PBS washing, the slide was treated with 5-bromo-4-chloro-3-indolyl phosphate/nitroblue tetrazolium (BCIP/NBT) reagents16 for color development. Appropriate positive and negative controls provided by BioGenex were used with each reaction.
Nucleic Acid and Protein Extraction from Fixed Tissue Sections
Four to eight 5-μm sections were cut from each paraffin block and placed in a 1.5-ml microcentrifuge tube. For RNA extraction, 800 μl of Hemo-De (Fisher, Pittsburgh, PA, USA) was added to each tube and vortexed until the paraffin was visibly dissolved. After centrifugation, the pellet was washed with 400 μl absolute ethanol, then resuspended in a buffer containing 20 mM Tris (pH 7.4), 20 mM EDTA, 1% SDS, and 1 mg/ml proteinase K (Sigma, St Louis, MO, USA) at 0.5 ml/tube. The tissue was then incubated in a 55°C water bath for 6 h to solubilize cellular proteins. The tissue lysate was treated twice with TRIzol LS (Life Technologies, Gaithersburg, MD, USA) to extract RNA, following the manufacturer's recommendations. After DNase I treatment, the extracted RNA was resuspended in 25 μl of molecular-grade water until RT-PCR reaction. For protein extraction, the deparaffinized tissue pellet was resuspended in 60 μl of protein extraction buffer 1D (Bio-Quick, Inc, Silver Spring, MD, USA) in a 1.5-ml tube, and protein was extracted according to the manufacturer's recommendation.
SDS-PAGE and Western Blot
Proteins extracted from paraffin blocks were first denatured at 100°C for 5 min and then separated by electrophoresis with a 4–15% gradient PAGE gel. For Western blot, the protein was transferred onto PVDF membrane (Bio-Rad, Hercules, CA, USA). After washing in TBS (Bio-Rad) and blocked overnight with 3% gelatin–TBS buffer, the membranes were incubated in TBS-diluted anticytokeratin monoclonal antibody (1:5000) for 3 h, followed by 2 h of incubation with 1:50 000 diluted secondary antibody, alkaline phosphatase-conjugated goat anti-mouse IgG. The signal was developed using the AP Color Development System (Promega, Madison, WI, USA). The silver stain procedure followed product instructions (Bio-Rad).
RT-PCR Analysis
The RNA extracted from conventional formalin-fixed and ultrasound-fixed tissues was reverse-transcribed into cDNA with a reaction kit (Invitrogen Life Technologies, Carlsbad, CA, USA) in a reaction tube, following the manufacturer's instructions. Two sets of specific primer pairs for β-actin, 548 bp (5′-GTGGGGCGCCCCAGGCACCA-3′ and 5′-CTCCTTAATGTCACGCACGATTTC-3′) and 156 bp (5′-CCACACCTTCTACAATGAGC-3′ and 5′-ACAGCCTGGATAGCAACGTA-3′), were used for the PCR amplification, at a concentration of 15 pmol per primer. The PCR reaction was run for 40 cycles. The PCR products were separated on a 2% agarose gel and stained with ethidium bromide before photography.
Results
Implementing ultrasound in conjunction with formalin fixation of tissue reduces fixation time from approximately 16 h to 5–15 min, while tissue morphology is the same quality as that achieved by conventional formalin fixation. In addition, macromolecules are better preserved with the aid of fast ultrasound fixation. Tissue preservation by formalin fixation with ultrasound and without ultrasound (conventional fixation) was evaluated on the basis of tissue morphology, immunohistochemistry, in situ hybridization staining, and the integrity and antigenicity of molecules extracted from fixed tissues. Gross examination of tissue sections after ultrasound fixation revealed a firm texture with good tissue integrity and no appreciable shrinkage. Microscopic detail was well retained. Paraffin-embedded, ultrasound-fixed tissue was stable and no visible morphological difference presented after 5 years of storage at room temperature.
Morphological Preservation of Tissue by Conventional and Ultrasound Fixation
H&E-stained sections of lymphoid tissue fixed by formalin for various lengths of time, with and without ultrasound, are shown in Figure 1. Without ultrasound, shorter formalin fixation resulted in underfixed tissues. In all, 30 min of conventional formalin fixation resulted in unsatisfactory preservation of tissue, with cracking and shrinkage, nuclear chromatin condensation, cellular distortion, and epithelial dissociation from basement membranes characteristic of underfixed tissues (Figure 1a). After 6–8 h of conventional formalin fixation (Figure 1b), tissue showed mild swelling and rupture of cells, mild nuclear chromatin condensation, and mild cellular distortion. With the aid of ultrasound, tissues fixed for 15 and 30 min (Figure 1d and e) displayed no morphological differences (no structural distortion, collapse, or alteration of chromatin intensity) compared to tissues conventionally fixed for 22 h (Figure 1c). The color balance in ultrasound-fixed tissue was pleasant, with a slightly more pronounced eosinophilia than in conventionally fixed tissue. The 15-min ultrasound-fixed section showed slightly more eosinophilia staining than the 30-min ultrasound-fixed section. Erythrocytes were intact and no erythocytolysis occurred in ultrasound-fixed sections. This experiment indicates that applying ultrasound drastically reduced a 22-h conventional fixation to about 15 min.

Comparison of morphology preservation in tissues fixed for varying lengths of time, with and without ultrasound. H&E-stained sections of lymph nodes formalin-fixed by routine method for 30 min (a), 6 h (b), 22 h (c), and with ultrasound for 15 min (d) and 30 min (e). All fixed tissues were processed by standard overnight protocols. Original magnification × 40 and × 800.
As they lack collagen, brain tissues are very delicate. Brain sections submerged in formalin and fixed with the assistance of ultrasound remained intact and retained histologic and morphologic qualities equal or superior to conventional fixation, as shown in Figure 2. With H&E staining, neuropils and neurons were visible, and nuclear details in cerebellar granular cells and Purkinje cells were well preserved. There was not much difference in staining and morphology between brain tissues ultrasound-fixed for 15 min and those conventionally fixed overnight. Immunohistochemistry detection of glial and neural antigens after proteolytic pretreatment in ultrasound-fixed brain tissue had more intense immunoreactivity and sharper staining, with greater cellular protein detail and definitions than with conventional fixation. Immunohistochemistry staining with neurofilament monoclonal antibody indicated that neuron fibers in ultrasound-fixed sections were less fragmented than in conventionally fixed sections. This experiment seems to suggest that ultrasound-facilitated formalin fixation may result in better tissue preservation.

Comparison of the preservation of morphological details in brain tissues undergoing conventional 16- to 24-h overnight fixation, and 10–15 min of ultrasound fixation. Fixed tissues are subject to 16–18 h of automated tissue processing. H&E-stained sections indicated better morphologic characteristics in ultrasound-fixed tissue (b) than in conventionally fixed tissue (a). Original magnification × 400. Immunohistochemistry detection with NFP antibody indicated stronger immunohistochemistry staining and less neuron fiber fragmentation in ultrasound-fixed tissue (d) than in conventionally fixed tissue (c). Original magnification × 100.
Nuclear Morphology in Tissues Preserved by Conventional and Ultrasound Fixation: A Blind Study
In all, 5-mm biopsies from 23 fresh prostatectomy specimens were formalin-fixed as 5-mm-thick sections, with 72–96 h of conventional and 5 min of ultrasound-facilitated formalin fixation. This blind study compared the nuclear morphology of the corresponding radical prostatectomies. Nuclear histology was compared to the corresponding slide of the prostatectomy. Nuclei were graded according to the WHO/Mostofi grading system. In the H&E-stained sections (Figure 3), nuclear morphology, including size, shape, and chromatin distribution, was identical in tissue with or without ultrasound treatment.

Comparison of H&E staining of clinical cases (as in Table 1) of prostate tissues fixed with conventional method (a–c) and ultrasound-facilitated method (d–f). Original magnification × 200. a, d: case 1, benign; b, e: case 11, tumor of grade I; c, f: case 8, different grading in 10% of cells.
As summarized in Table 2, 14 out of 23 samples consisted of benign glands; nine were malignant. Nuclear morphology is sensitive to the duration of formalin fixation. As reported previously, shorter fixation caused nuclear artificial changes that simulate a lower nuclear grading.25, 26 Except in one case where 10% of the prostatectomy showed a nuclear appearance of higher grade, grading of ultrasound-fixed tissue was the same as that determined from conventional formalin-fixed and paraffin-embedded tissue. This study indicates that nuclear appearance is almost identical following 5-min ultrasound fixation or 72-h conventional formalin fixation.
Ultrasound Fixation Greatly Improves Tissue Protein Antigenic Properties, Immunohistochemistry Studies
Fat-abundant breast tissue is difficult to fix by conventional methods. Recently, it was reported that underfixed breast tissues resulted in a very faint and less specific ER immunohistochemistry staining, even after antigen retrieval treatment.27, 28, 29 Figure 4 shows specific ER staining of similar intensity in breast specimens fixed by 5-min ultrasound fixation and 24-h conventional formalin fixation. This experiment indicates that, for breast tissue, 5-min ultrasound fixation achieves results similar to 24-h conventional fixation.

Estrogen receptor immunohistochemistry of breast tissues (× 400) fixed by (a) 24-h routine formalin fixation and (b) 5-min ultrasound-facilitated formalin fixation.
Ultrasound fixation also substantially increases protein antigenic reactivity and reduces the need for antigen retrieval treatment before immunohistochemistry staining, as summarized in Table 3 and shown in Figure 5. Tissues were underfixed by 30-min conventional fixation or slightly overfixed by 22-hour conventional fixation, so that their immunohistochemistry staining was less intense than that of the 6-h fixed tissue. In comparison, 15-min ultrasound-fixed tissue produced better morphology and protein antigen preservation than 30-min ultrasound-fixed tissue. With antigen retrieval, CD5 antibodies took hours to react with conventionally fixed tissue, but only 10 min with ultrasound-fixed tissue. With antigen retrieval and short immunohistochemistry staining protocols, CD5 staining was not observed on conventionally fixed lymph node, but was strong on 15-min ultrasound-fixed tissue. Without antigen retrieval pretreatment, using overnight long immunohistochemistry staining protocols (see Materials and methods), CD5 signal was not visible on the 22-h conventionally fixed tissue, but was observable on 30-min ultrasound-fixed tissue and very intense on 15-min ultrasound-fixed tissue. Furthermore, without antigen retrieval, positive CD5 stain was observable on 15-min ultrasound-fixed tissue with short immunohistochemistry reaction protocol. These data indicate that the efficiency of immunohistochemistry staining was significantly increased on ultrasound-fixed tissues.

Comparison of CD5 immunohistochemistry on formalin-fixed lymph node tissues without microwave-antigen retrieval, by routine 22 h (a), ultrasound 15 min (b), and ultrasound 30 min (c). In all, 15-min ultrasound-fixed tissue (b) has much stronger CD5 immunoreactivity than 30-min ultrasound-fixed tissue (c). No immunohistochemistry stain observed in routine 22-h fixed tissue (a). Original magnification × 100.
Ultrasound fixation increases the sensitivity of color staining (H&E) or immunostaining. Under conditions listed in Table 3, ultrasound fixation generated stronger CD5 immunohistochemistry intensity than corresponding conventional fixation. In Figure 6, as the concentration of anticytokeratin antibody was diluted from 1:400 to 1:20 000, the immunohistochemistry intensity on ultrasound-fixed tissue was similar to that of conventionally fixed tissue with a 1:400 antibody dilution, indicating a 50-fold increase in immunohistochemistry sensitivity, and a 50-fold reduction in antibody usage.

Ultrasound-facilitated formalin fixation improved immunohistochemistry sensitivity. Immunohistochemistry intensity on 15-min ultrasound-fixed lung tissue with anticytokeratin antibody dilution of 1:20 000 is similar to that of conventional 16- to 18-h fixed tissue with antibody at 1:400 dilution.
Ultrasound Fixation Greatly Improves Tissue RNA Preservation, In Situ Hybridization Studies
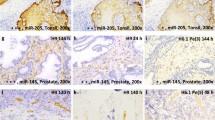
Synthetic oligonucleotide specific to kappa light chain immunoglobulin mRNA was hybridized to fixed tonsil sections and visualized with anti-kappa antibody (Figure 7e–h). Immunohistochemistry staining against kappa light chain antigens is shown for comparison. The immunohistochemistry signals for kappa light chain were weak in 30-min conventionally fixed sections, but strong in the 6- and 22-h conventionally fixed sections and also in the 15-min ultrasound-fixed section, consistent with what we observed of immunohistochemistry staining (Figure 5). However, no in situ hybridization staining was observed in either 30-min (Figure 7a) or 6-h (Figure 7b) fixed tonsils without ultrasound (Figure 7e and f). Tonsil fixed for 22 h (Figure 7g) without ultrasound showed only sporadic mRNA staining signals in plasma cells along the peripheral margin, and none in the central portion. This edge staining is consistent with results from previous reports.30, 31, 32 In contrast, 15-min ultrasound-fixed tonsil (Figure 7h) demonstrated intensive, specific mRNA staining of plasma cells in the germinal center as well as the peripheral edge, producing sharp, well-defined cytoplasm signals in plasma cells and germinal center cells, with an evenly distributed in situ hybridization signal across the histologic section. The pattern and distribution of mRNA hybridization signal (Figure 7h) in ultrasound-fixed tissue matched the distribution of the anti-kappa immunohistochemistry (Figure 7d).

Comparison of immunohistochemistry and in situ hybridization of tonsil tissues formalin fixed with and without ultrasound. Immunohistochemistry for kappa light chain antigen (a–d) and in situ hybridization for kappa light chain mRNA (e–h). Tonsils fixed for 6 h (b and f) show specific immunohistochemistry staining of kappa light chain antigen but no kappa light chain mRNA signals. Tonsils fixed for 22 h (c and g) show sporadic mRNA staining along the peripheral edges. In all, 15-min ultrasound-fixed tonsils (d and h) demonstrate strong, specific mRNA staining of plasma cells in the germinal center and the peripheral edge, corresponding to immunohistochemistry signals. Original magnification × 20.
Ultrasound Fixation Improves the Preservation of Macromolecules, Molecular Analyses
Proteins in extracted solutions from fixed tissues were analyzed by SDS-PAGE and Western blot. Coomassie blue staining (Figure 8a) and Western blot against a universal cytokeratin protein (Figure 8b) or a cancer marker alpha-methylacyl-CoA racemase33, 34 protein (Figure 8c) indicated that a much greater amount of total and specific proteins was detected in extract from frozen prostate tissue and ultrasound-fixed tissue than from conventionally fixed tissue. These results are consistent with our immunohistochemistry data, suggesting that protein antigenicity is more severely masked in conventionally fixed tissue than in ultrasound-fixed tissue.

Comparison of SDS-PAGE of proteins extracted from prostate tissues: (1) 12–16 h conventional formalin fixation; (2) 5-min ultrasound-facilitated formalin fixation; and (3) frozen. (a) Coomassie blue staining, (b) Western blot by anti-keratin AE1/AE3 antibody; and (c) Western blot by anti-alpha-methylacyl-CoA racemase antibody.
RT-PCR was utilized to evaluate mRNA integrity in extract from formalin-fixed tissues with and without ultrasound (Figure 9). Equal amounts of total RNA from ultrasound-fixed and conventionally fixed tissues was reverse-transcribed to cDNA, then amplified with primers specific for a 548 bp fragment of beta-actin. The 548-bp-long fragment was only amplified from extracts of ultrasound-fixed tissue, but not from conventionally fixed tissue, while the short 156-bp fragment was amplified from extracts of both tissues. The controls using total RNA extracts without reverse transcription did not show any PCR products, indicating that the amplicons were from RNA not DNA. This observation indicated that the integrity of mRNA was much better preserved in ultrasound-fixed specimens than in conventionally fixed tissues. Similarly, DNA molecules are well preserved in ultrasound-fixed tissue and readily generate PCR amplicons of over 1300 bp (data available). These results are consistent with our in situ hybridization data, suggesting that more RNAs remain intact and less degradation occurs in ultrasound-fixed tissue than in conventionally fixed tissue.

RT-PCR of beta-actin mRNA from pulmonary carcinoma with primer sets A (for amplicons of 548-bp) and B (for amplicons of 156-bp). F: traditional formalin-fixed and paraffin-embedded tissue; U: ultrasound-facilitated formalin-fixed tissue; FC: F without reverse transcription; UC: U without reverse transcription; C: water only; M: DNA marker.
Discussion
This paper seeks to demonstrate that implementation of high-frequency, high-intensity ultrasound to formalin fixation procedures not only greatly accelerates conventional formalin fixation, but also achieves superior overall tissue preservation in morphology (Figures 1, 2 and 3), immunoreactivity (Figures 4, 5, 6 and 7), and macromolecular integrity (Figures 7, 8 and 9). The improved preservation of protein antigenicity in ultrasound-fixed tissues results in increased immunohistochemistry intensity, sensitivity, and reduction or elimination of the need for antigen enhancement pretreatment (Figures 5 and 6). Greater amounts of proteins and nucleic acids, with improved integrity, can be extracted from ultrasound-fixed tissues than from conventionally fixed tissues to support general molecular analysis (Figures 8 and 9). Previous reports have shown that morphological nuclear grading on radical prostatectomy specimens25, 26 and the specificity and intensity of ER staining on breast tissues27, 28, 29 are sensitive to formalin fixation time. Our results (Figures 3 and 4) clearly show that 5-min ultrasound-facilitated formalin fixation achieved the same degree of formalin fixation as conventional methods lasting 16 h or more. Although ultrasound can be used to facilitate penetration of other fixatives as well, we have chosen to retain formalin as the fixative because, overall, it is the most widely used fixative for clinical tissue preservation.
The high-frequency, high-power ultrasound specified in this report enhances biochemical reactions and accelerates fixative penetration into tissue, while avoiding the tissue damage caused by low-frequency ultrasound and the excessive heat generated by other physical modalities such as microwave. The ultrasound transducer produces a strong, directional ultrasonic stream in fixatives capable of pushing aside a glass section slide, yet the microscopic structure of a 5-μm-thick tissue section mounted on the glass slide is not disrupted after continuous exposure to this force for 10–20 min. No structural distortion has been observed in ultrasound-fixed tissues (Figure 1), even in the most delicate brain tissue and after proteolytic enzyme pretreatment (Figure 2). By comparison, identical tissue sections are destroyed after a 10-s exposure to 40 kHz ultrasound in a water bath.
In general, ultrasonic irradiation facilitates mobilization of molecules and accelerates chemical reactions. As documented in the literature,35, 36 the effects of ultrasound on tissue include: (1) thermal effects causing an increase in temperature and rate of mass transport, (2) mechanical effects causing cell membrane permeability changes and/or cell membrane rupture, and (3) chemical effects causing free radical formation and consequent biochemical reactions in tissue. In our laboratory, ultrasound irradiation caused only a limited increase in tissue and solution temperature (less than 10°C after 40 min of irradiation). Considering that ultrasound fixation requires only 5–15 min, we believe that the accelerating effect of ultrasound-facilitated formalin fixation is probably due to increased cellular penetration to overcome the ‘fixed surface tissue perfusion barrier’ and to accelerated chemical interactions.
In water solution, over 99% of formaldehyde exists in hydrated methylene glycol form, which by itself is not a fixative.1, 36 The reversion of the predominantly nonfixative ethylene glycol to the fixative formaldehyde depends on the latter forming bonds with the tissue molecules. But the cross-linking reaction between formaldehyde and amino acids or nucleic acids is very slow.1 This explains why it takes 13 h for skim milk to harden when it is mixed with 35% formaldehyde, but only 30 min to reach the same hardness with ultrasound sonication.37 The increased hardening rate is a clear indication of accelerated formaldehyde reaction with proteins, since the possibility of penetration as a limiting step is eliminated.
In most pathology laboratories, the fixative used is 10% formalin. Subsequent processing usually includes a period in alcohol; thus, tissues are effectively ‘double fixed’ in both formalin and alcohol. Underfixation, such as 30-min conventional formalin fixation (Figures 1a and 7a), causes structural distortion due to the loss of soluble components, or tissue shrinkage caused by subsequent alcohol treatment. Alcohols fix tissues by dehydrating, denaturing, and coagulating tissue proteins without modification of molecular structure.3, 11 Tissues underfixed after formalin treatment may undergo rapid dehydration when exposed to ethanol, causing significant tissue shrinkage, distortion, and suboptimal preservation of morphology. As in prior ER immunohistochemistry studies,27 weak immunohistochemistry staining was observable in underfixed tissue only in peripheral regions, indicating that some of the proteins in these regions were preserved to some degree. Loss of immunoreactivity in underfixed tissue (Figure 7a and Table 3) is probably caused by alcohol precipitating of unfixed tissue proteins, resulting in excessive sensitivity to proteolytic enzyme or microwave antigen retrieval pretreatment.3, 5, 38 Tissues with 6-h conventional formalin fixation showed a stronger immunohistochemistry signal after antigen retrieval treatment than tissues with 22-h fixation, suggesting that the latter produces overfixation that is difficult to reverse fully by antigen retrieval.
We believe that ultrasound-facilitated formalin fixation results in more uniform fixation and/or the formation of cross-linking throughout the entire tissue. Without the aid of ultrasound, no in situ hybridization signal appeared on 30-min or 6-h conventionally fixed tissues (Figure 7e and f). Sporadic in situ hybridization signals in peripheral regions were observed until the tissue was fixed for 22 h (Figure 7g), in accordance with previous mRNA studies.30, 31, 32 This fact seems to suggest that RNAs in central regions take longer to fix and are thus more vulnerable to RNase-induced degradation. In contrast, 5–15 min of ultrasound-facilitated formalin fixation achieves good preservation in both protein antigenicity (Figures 2b, 3d, 7d) and nucleic acid uniformly throughout the tissue (Figure 7h). Previous studies have concluded that subsequent alcohol treatment is insufficient to terminate endogenous RNase activity,16 and the formation of cross-linking is related to the quenching of RNase activity during formalin fixation.39, 40 Our observations suggest that ultrasound overcomes the ‘fixed surface tissue perfusion barrier’ and accelerates the cross-linking reaction to inactivate RNase. Our RT-PCR analysis also confirmed that mRNA integrity was much improved in ultrasound-fixed tissues, so that RNA of 548 bp was obtained in ultrasound-fixed but not in conventionally fixed tissues. Since an mRNA fragment over 500 bp long is sufficient for the construction of gene libraries and molecular profiling,12 ultrasound-facilitated fixation is superior to conventional fixation for molecular analysis.
In conclusion, high-frequency, high-intensity ultrasound significantly reduces the time of formalin fixation from overnight to 5–15 min, probably through ultrasound-elevated formaldehyde tissue penetration and cross-linking reaction. Compared to the conventional method, ultrasound-facilitated formalin fixation retains more uniform tissue morphology and improved macromolecule preservation. Molecule extracts from ultrasound-fixed tissue can be used directly for downstream molecular analysis. Finally, ultrasound-fixation is a safe and technically simple process applicable to many contemporary molecular techniques, and to small- and large-scale automation.
References
Fox CH, Johnson FB, Whiting J, et al. Formaldehyde fixation. J Histochem Cytochem 1985;33:845–853.
French D, Edsall JT . The reaction of formaldehyde with amino acids and proteins. Adv Protein Chem 1945;2:277–335.
Battifora H, Kopinski M . The influence of protease digestion and duration of fixation on the immunostaining of keratins. A comparison of formalin and ethanol fixation. J Histochem Cytochem 1986;34:1095–1100.
Kaku T, Ekem JK, Lindayen C, et al. Comparison of formalin- and acetone-fixation for immunohistochemical detection of carcinoembryonic antigen (CEA) and keratin. Am J Clin Pathol 1983;80:806–815.
Login GR, Schnitt SJ, Dvorak AM . Rapid microwave fixation of human tissues for light microscopic immunoperoxidase identification of diagnostically useful antigens. Lab Invest 1987;57:585–591.
Leong AS, Duncis CG . A method of rapid fixation of large biopsy specimens using microwave irradiation. Pathology 1986;18:222–225.
Bonner RF, Emmert-Buck M, Cole K, et al. Laser capture microdissection: molecular analysis of tissue. Science 1997;278:1481–1483.
Schena M, Shalon D, Davis RW, et al. Quantitative monitoring of gene expression patterns with a complementary DNA microarray. Science 1995;270:467–470.
Kononen J, Bubendorf L, Kallioniemi A, et al. Tissue microarrays for high-throughput molecular profiling of tumor specimens. Nat Med 1998;4:844–847.
Werner M, Chott A, Fabiano A, et al. Effect of formalin tissue fixation and processing on immunohistochemistry. Am J Surg Pathol 2000;24:1016–1019.
Srinivasan M, Sedmak D, Jewell S . Effect of fixatives and tissue processing on the content and integrity of nucleic acids. Am J Pathol 2002;161:1961–1971.
Emmert-Buck MR, Strausberg RL, Krizman DB, et al. Molecular profiling of clinical tissue specimens: feasibility and applications. Am J Pathol 2000;156:1109–1115.
Wada N, Imoto S, Hasebe T, et al. Evaluation of intraoperative frozen section diagnosis of sentinel lymph nodes in breast cancer. Jpn J Clin Oncol 2004;34:113–117.
Morales A, Essenfeld H, Essenfeld E, et al. Continuous-specimen-flow, high-throughput, 1-hour tissue processing. A system for rapid diagnostic tissue preparation. Arch Pathol Lab Med 2002;126:583–590.
Yasuda K, Yamashita S, Shiozawa M, et al. Application of ultrasound for tissue fixation: combined use with microwave to enhance the effect of chemical fixation. Acta Histochem Cytochem 1992;25:237–244.
Buchmuller K . The dependence on frequency in utilization of ultrasonics for histological technic. Strahlentherapie 1954;95:316–325 [in German].
Drakhli EI . Methods of using ultrasonics in a quick histological treatment of tissues. Arkh Patol 1967;29:81–82 [in Russian].
Shmurun RI . Methods for the rapid preparation of paraffin blocks. Arkh Patol 1992;54:46–47 [in Russian].
Obertyshev VG . Ultrasonic express paraffin handling of histological specimens. Sud Med Ekspert 1987;30:56–58 [in Russian].
Chen R, Weng L, Sizto NC, et al. Ultrasound-accelerated immunoassay, as exemplified by enzyme immunoassay of choriogonadotropin. Clin Chem 1984;30:1446–1451.
Podkletnova I, Alho H . Ultrasound-amplified immunohistochemistry. J Histochem Cytochem 1993;41:51–56.
Nishimura R, Nakao I, Shikata N, et al. Improved lipid visualization with a modified osmium tetroxide method using ultrasonic treatment and intensification with imidazole or triazole. Biotech Histochem 1995;70:28–32.
Hsu SM, Raine L, Fanger H . Use of avidine–biotin–peroxidase complex (ABC) in immunoperoxidase techniques: a comparison between ABC and unlabeled antibody (PAP) procedures. J Histochem Cytochem 1981;29:577–580.
Chu WS, Aguilera NS, Wei MQ, et al. Anti-apoptotic marker, Bcl-X(L), expression on Reed-Sternberg cells of Hodgkin's disease using a novel monoclonal marker, YTH-2H12. Hum Pathol 1999;30:1065–1070.
Zhou M, Hayasaka S, Taylor JM, et al. Lack of association of prostate carcinoma nuclear grading with prostate specific antigen recurrence after radical prostatectomy. J Urol 2001;166:2193–2197.
Jorgensen T, Yogesan K, Tveter KJ, et al. Nuclear texture analysis: a new prognostic tool in metastatic prostate cancer. Cytometry 1996;24:277–283.
Goldstein NS, Ferkowicz M, Odish E, et al. Minimum formalin fixation time for consistent estrogen receptor immunohistochemical staining of invasive breast carcinoma. Am J Clin Pathol 2003;120:86–92.
Arber DA . Effect of prolonged formalin fixation on the immunohistochemical reactivity of breast markers. Appl Immunohistochem Mol Morphol 2002;10:183–186.
Lee H, Douglas-Jones AG, Morgan JM, et al. The effect of fixation and processing on the sensitivity of oestrogen receptor assay by immunohistochemistry in breast carcinoma. J Clin Pathol 2002;55:236–238.
Nuovo GJ, Richart RM . Buffered formalin is the superior fixative for the detection of HPV DNA by in situ hybridization analysis. Am J Pathol 1989;134:837–842.
Tournier I, Bernuau D, Poliard A, et al. Detection of albumin mRNAs in rat liver by in situ hybridization: usefulness of paraffin embedding and comparison of various fixation procedures. J Histochem Cytochem 1987;35:453–459.
Harper SJ, Pringle JH, Gillies A, et al. Simultaneous in situ hybridisation of native mRNA and immunoglobulin detection by conventional immunofluorescence in paraffin wax embedded sections. J Clin Pathol 1992;45:114–119.
Jiang Z, Woda BA, Rock KL, et al. P504S: a new molecular marker for the detection of prostate carcinoma. Am J Surg Pathol 2001;25:1397–1404.
Kuefer R, Varambally S, Zhou M, et al. Alpha-methylacyl-CoA racemase: expression levels of this novel cancer biomarker depend on tumor differentiation. Am J Pathol 2002;161:841–848.
Suslick KS . The chemical effects of ultrasound. Sci Am 1989;260:80–86.
Riesz P, Kondo T . Free radical formation induced by ultrasound and its biological implications. Free Radic Biol Med 1992;13:247–270.
Stephanis CG, Hatiris JG, Mourmouras DE . Acceleration of formaldehyde reactions with proteins due to ultrasound. Ultrason Sonochem 1998;5:33–35.
Williams JH, Mepham BL, Wright DH . Tissue preparation for immunocytochemistry. J Clin Pathol 1997;50:422–428.
Rait VK, O'Leary TJ, Mason JT . Modeling formalin fixation and antigen retrieval with bovine pancreatic ribonuclease A. I. Structural and functional alterations. Lab Invest 2004;84:292–299.
Rait VK, Xu L, O'Leary TJ, et al. Modeling formalin fixation and antigen retrieval with bovine pancreatic ribonuclease A. II. Interrelationship of cross-linking, immunoreactivity, and heat treatment. Lab Invest 2004;84:300–306.
Acknowledgements
We thank Ms Bonnie L Casey for her excellent editorial assistance in the preparation of this manuscript. This work was supported in part by an NIH/NCI Grant 1R21 CA091166 (to WSC) and an ARP/AFIP Grant UBKL (to WSC).
Author information
Authors and Affiliations
Corresponding author
Additional information
The opinions expressed in this article are the personal views of the authors and are not to be construed as representing the views of the Department of the Army, Air Force, Navy or the Department of Defense.
Rights and permissions
About this article
Cite this article
Chu, WS., Furusato, B., Wong, K. et al. Ultrasound-accelerated formalin fixation of tissue improves morphology, antigen and mRNA preservation. Mod Pathol 18, 850–863 (2005). https://doi.org/10.1038/modpathol.3800354
Received:
Revised:
Accepted:
Published:
Issue date:
DOI: https://doi.org/10.1038/modpathol.3800354
Keywords
This article is cited by
-
DNA isolated from formalin-fixed paraffin-embedded healthy tissue after 30 years of storage can be used for forensic studies
Forensic Science, Medicine and Pathology (2021)
-
Biobanking in Precision Medicine
Current Pharmacology Reports (2018)
-
Molecular Pathology and Pre-Analytic Variables: Impact on Clinical Practice From a Breast Pathology Perspective
Current Pathobiology Reports (2018)
-
Towards a mechanistic understanding of the human subcortex
Nature Reviews Neuroscience (2017)
-
Systematic comparison of tissue fixation with alternative fixatives to conventional tissue fixation with buffered formalin in a xenograft-based model
Virchows Archiv (2012)
