
Abstract
The American Heart Association has updated the cardiovascular health (CVH) assessment tool, referred to as the Life’s Essential 8 (LE8). Metabolic dysfunction-associated steatotic liver disease (MASLD) is now the most common chronic liver disease worldwide and is linked to an elevated risk of mortality. We aimed to explore the association of LE8 with all cause and cause-specific mortality in MASLD in a prospective cohort study. A total of 10,050 participants with MASLD from the NHANES 2005–2018 dataset were included in the study. LE8 was evaluated by combining four health behaviors and four health factors, with scores of 0–49 categorized as low CVH, 50–79 as moderate CVH, and 80–100 as high CVH. In the fully adjusted model, each one-point increase in the LE8 score corresponded to a 2.7, 2.7, and 1.6% decrease in all-cause, CVD, and cancer mortality risk, respectively, in people with MASLD. Compared to low CVH, being in moderate/high CVH was negatively associated with most mortality outcomes, while health factors lost significant association with cancer mortality.
Similar content being viewed by others

Introduction
In 2023, a consensus of experts and scholars from leading international liver disease societies introduced the term metabolic dysfunction-associated steatotic liver disease (MASLD) to replace the previously used nonalcoholic fatty liver disease (NAFLD)1,2,3. MASLD is a clinicopathological condition characterized by the presence of hepatic steatosis and at least one cardiometabolic risk factor (CMRF) in the absence of other causes of steatosis, highlighting its strong association with metabolic disorders1. MASLD represents the most prevalent chronic liver disease globally and serves as a primary driver of liver-related complications, including cirrhosis, liver transplantation, and hepatocellular carcinoma4. Recent epidemiologic evidence suggests that about one in three adults in the U.S. is affected by MASLD5,6. In addition, MASLD is a multisystem disease. A meta-analysis that included 129 cohort studies demonstrated that MASLD is associated with a variety of adverse health outcomes, including cardiovascular disease (CVD), multiple cancers, chronic kidney disease, and various metabolic disorders7. Prospective cohort studies consistently indicate that MASLD independently increases all-cause mortality compared with control populations8,9. Lifestyle modifications targeting metabolic disorders remain central to MASLD prevention and treatment10.
Cardiovascular risk assessment and intervention are pivotal in managing MASLD. Individuals with MASLD face a markedly elevated risk of cardiovascular disease (CVD), which is the leading cause of death in the MASLD population11,12,13. Maintaining optimal cardiovascular health (CVH) likely plays a crucial role in preventing excess mortality among individuals with MASLD. In 2022, the American Heart Association (AHA) updated the CVH assessment tool, known as the Life’s Essential 8 (LE8) score14. The LE8 integrates four health behaviors and four health factors, offering a novel approach to CVH evaluation at both the population and individual levels. Recent observational clinical studies have demonstrated that LE8, is linked to the incidence of various diseases, including CVD and NAFLD15,16. Furthermore, higher CVH has been shown to correlate with lower all-cause mortality in the general population17. However, whether LE8 is associated with all-cause and disease-specific mortality in people with MASLD remains unclear. Given the high burden of CVD in MASLD and its contribution to premature mortality, investigating the relationship between LE8 and mortality in individuals with MASLD could clarify the importance of achieving optimal CVH in mitigating premature mortality.
In this study, we utilized a nationally representative, prospective cohort from the National Health and Nutrition Examination Survey (NHANES) to examine the association between cardiovascular health (CVH) assessed by the Life’s Essential 8 (LE8) score and mortality in individuals with MASLD. In addition, we explored the dose-responsive or nonlinear association between LE8 and mortality in the MASLD population and whether it remained stable across sociodemographic characteristics. These findings suggest that adherence to a higher CVH plays a key role in preventing excess mortality in individuals with MASLD, offering valuable insights for the clinical management of MASLD.
Methods
Study design and population
NHANES is a major health epidemiology program under the direction of the National Center for Health and Statistics (NCHS), aimed at assessing the health and nutritional status of noninstitutionalized populations in the United States. Since 1999, NHANES has collected and characterized participants’ demographic characteristics and health-related information through continuous two-year cycles. To obtain national estimates, NHANES employs a multistage probability sampling design with associated sample weights, adjusting for the complex study structure. Thus, NHANES consists of ongoing, nationally representative, multiethnic cross-sectional surveys. The NCHS Ethics Review Board approved all NHANES protocols, and written informed consent was obtained from all participants.
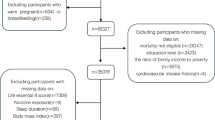
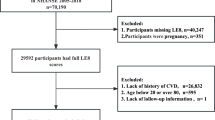
The study population selection flowchart was presented in Fig. 1. Initially, 70,190 participants from NHANES 2005–2018 were included, excluding individuals aged < 20 years (n = 30,441), pregnant women (n = 711), those with viral hepatitis (n = 842), autoimmune hepatitis (n = 7), and excessive alcohol consumption (n = 3,072).Next, we excluded people with missing Fatty Liver Index (FLI) data (n = 5489), FLI less than 60 (n = 15459), not meeting CMRF criteria, missing LE8 (n = 3230), and missing survival information (n = 8). Individuals with missing covariates (n = 876) were also excluded. Ultimately, 10,050 individuals with MASLD were included.

Flowchart of study population selection, NHANES 2005–2018.
Assessment of LE8 score
The LE8 is an integrated cardiovascular health (CVH) assessment metric comprising four health behaviors (diet quality, physical activity, nicotine exposure, and sleep health) and four health factors (body mass index [BMI], blood lipids, blood glucose, and blood pressure)14. Diet quality was assessed according to the Healthy Eating Index-2015 (HEI-2015). The HEI-2015 is a comprehensive tool for evaluating and monitoring the dietary quality of the population, providing a score ranging from 0 to 10018. In brief, the HEI-2015 evaluates nine dietary components for adequate intake (where total fruits, whole fruits, total vegetables, greens and beans, total protein foods, and seafood and plant proteins were assigned scores from 0 to 5, and whole grains, dairy products, and fatty acids were assigned scores from 0 to 10) and four components for moderate intake (refined grains, salt, added sugars, and saturated fats, all assigned scores from 0–10)18. Dietary intake was assessed using two 24-hour dietary recalls (the first conducted in person and the second via a telephone follow-up within 3–10 days), and participants’ energy and nutrient intakes of HEI-2015 components were calculated using the Food and Nutrient Database for Dietary Studies (FNDDS), and food groups were identified using the U.S. Department of Agriculture (USDA) Food Pattern Equivalency Database (FPED)19. The other health behavior score components were derived from self-reported data collected via the NHANES questionnaire15. Physical activity was assessed based on self-reported weekly duration of moderate or vigorous physical activity (min) on the Global Physical Activity Questionnaire. Nicotine exposure was evaluated based on self-reported history of smoking or use of inhaled nicotine delivery systems. Sleep health was evaluated based on the average hours of sleep per night.
BMI was calculated by dividing weight (kg) by the square of height (m), with weight and height measurements determined by trained technicians at mobile examination centers (MECs). Blood lipid scores were assessed based on plasma non-high-density lipoprotein cholesterol (HDL-C) levels. Blood glucose score was assessed by fasting blood glucose (FBG, mg/dL) and hemoglobin A1c (%) levels. Blood pressure scores were assessed by at least three consecutive systolic and diastolic blood pressure values (mmHg) provided by MEC skilled staff.
Each LE8 component was assigned a score from 0 to 100, and the final total score was obtained by adding the scores for each indicator and dividing by eight. Based on LE8 scores, participants were categorized as having low (0–49), moderate (50–79), and high CVH (80–100) CVH14. Specific assignment criteria were presented in Table S1.
Diagnosis of MASLD
MASLD was defined as the presence of at least one cardiometabolic risk factor (CMRF) in addition to SLD, with exclusion of other causes of steatosis (e.g., heavy alcohol consumption [> 30 g/day in men and > 20 g/day in women], chronic viral hepatitis, or autoimmune liver disease)20. The presence of CMRF was determined by the presence of at least one of the following factors: overweight/obesity/central obesity, hyperglycemia, hypertension, elevated plasma triglyceride (TG) levels (≥ 1.7 mmol/l or on lipid-lowering therapy), and lowered serum high-density lipoprotein cholesterol (HDL-C) (≤ 1 mmol/l in men or ≤ 1.3 mmol/l in women or on lipid-lowering therapy)1. SLD was assessed using the Fatty Liver Index (FLI), with a value ≥ 60 indicating the presence of hepatic steatosis. FLI is a well-established noninvasive screening algorithm with good accuracy (0.84) based on BMI, waist circumference (WC), gamma-glutamyl-transferase (GGT), and TG calculations21. Numerous clinical studies have shown that FLI is an effective diagnostic marker for hepatic steatosis in MASLD22. Additionally, we employed another widely used diagnostic marker for SLD, the USFLI, in sensitivity analyses to validate the stability of the results23. The USFLI is a noninvasive assessment tool developed using NHANES, with a diagnostic AUC of 0.80 based on age, race/ethnicity, WC, GGT, fasting insulin, and FBG levels24.
Mortality data collection
Mortality data were obtained through December 31, 2019, by prospective matching with the National Death Index database. The outcomes of our study included all-cause, cardiovascular disease (CVD), and cancer-related mortality in the MASLD population. All-cause mortality included all types of mortality. CVD mortality was derived from codes associated with deaths from cardiac and cerebrovascular diseases, including I00-I09, I11, I13, I20-I51, and I60-I69. Cancer-related mortality was obtained according to codes C00-C97.
Covariates
We considered a range of potential covariates, including age, sex (male or female), race/ethnicity (non-Hispanic White, Mexican American, non-Hispanic Black, other Hispanic, or other race), educational attainment (less than high school, high school, or greater than high school diploma), household income-to-poverty ratio, marital status (single or non-single), and history of cardiovascular disease (CVD) (yes/no)15,17. Sociodemographic characteristics of participants were retrieved from the NHANES demographic file. CVD history (self-reported presence of angina, congestive heart failure, stroke, coronary heart disease, or heart attack) was collected via responses to questions on the medical condition questionnaire.
Statistical analysis
All analyses were appropriately weighted to account for the complex study design of NHANES. Data handling and analysis were performed using Empower Stats (X&Y Solutions, Inc., Boston, MA) and R 4.2.3. A two-sided P value < 0.05 was considered statistically significant. For baseline analyses, we categorized the MASLD population by CVH status (low, moderate, and high CVH) as assessed by LE8. Continuous variables were expressed as mean ± standard error and tested by weighted ANOVA, and categorical variables were expressed as number (percentage) and tested by weighted chi-square analysis. Kaplan-Meier (KM) survival curves were employed to explore time-dependent survival differences in the MASLD population by CVH status and to examine survival differences over time between groups using the log-rank test. Multivariate Cox proportional hazards regression models were used to explore the association of LE8 (continuous variable) and different CVH statuses (categorical variable) with all-cause and cause-specific mortality in the MASLD population and calculated hazard ratio [HR] and 95% confidence interval25. We constructed several models with varying degrees of adjustment. The crude model did not adjust for any covariates, model 1 adjusted for age, sex, and race/ethnicity, and model 2 was a fully adjusted model that additionally adjusted for education level, PIR(Polyisocyanurate Foam), marital status, and CVD history based on model 1. Fully adjusted restricted cubic spline (RCS) modeling and smoothed curve fitting were employed to explore nonlinear or dose-response associations between LE8 and mortality in individuals with MASLD. Fully adjusted stratified analyses (adjusting for all covariates other than subgroup variables) were used to explore whether these associations remained stable across subgroups and to identify potential effect modifiers through interaction analyses. In sensitivity analyses, the USFLI was used to diagnose SLD, verifying the reliability of the results.
Results
Baseline characteristics
A total of 10,050 participants with MASLD were included, with a mean age of 50.3 years and a mean LE8 score of 60.6. Only 448 (4.46%) participants were in high CVH status. As CVH status increased, the MASLD population was younger, had a higher PIR, and was likely to be male, Mexican American/Other Hispanic/Other race, non-single, greater than a high school diploma, and without a history of CVD. Scores for LE8, LE8 health behaviors, LE8 health factors, and all LE8 components increased significantly with increasing levels of CVH (all p < 0.0001) (Table 1).
Association of LE8 with mortality in the MASLD population
After a median follow-up of 88 months (interquartile range 48–130 months), 1082 patients with MASLD died, with 354 and 260 CVD- and cancer-related deaths, respectively. KM survival analyses demonstrated a significant increase in all-cause, CVD, and cancer-related time-dependent survival probabilities in the MASLD population with increasing levels of CVH (all log-rank test p-values < 0.0001) (Fig. 2A–C).

KM survival analysis. A: LE8 and all-cause mortality; B: LE8 and CVD mortality; C: LE8 and cancer mortality.
In the fully adjusted model, each incremental increase in LE8 score was associated with a 2.7% reduction in all-cause mortality (HR = 0.973; 95% CI: 0.965–0.981; p < 0.0001). Compared to low CVH, participants with MASLD at both moderate and high CVH were associated with significantly lower all-cause mortality (moderate CVH: HR = 0.564; high CVH: HR = 0.330; p for trend < 0.0001). Similar associations were found between LE8 health behaviors/health factors and all-cause mortality in the MASLD population, with increases in health behaviors and health factors associated with 1.8% and 0.9% reductions in all-cause mortality per score, respectively (both p < 0.01) (Table 2). LE8, health behaviors, and health factor scores were also all significantly negatively associated with CVD mortality (LE8: HR = 0.973; health behaviors: HR = 0.990; and health factors: HR = 0.980). Compared to low CVH, most individuals with MASLD at moderate/high CVH had significantly lower CVD mortality, except for health behaviors in those with high CVH status (p = 0.084) (Table 3). LE8 and health behavior scores were inversely associated with cancer-related mortality in the MASLD population (LE8: HR = 0.984; health behavior: HR = 0.982), while health factors were not significantly associated with cancer mortality. Compared to low CVH, high CVH status for both LE8 and health behaviors was associated with significantly lower cancer mortality (p for trend both < 0.05) (Table 4).
RCS analysis
RCS analyses showed linear dose-response associations of LE8 and health behaviors with all-cause mortality in the MASLD population (p for nonlinear 0.5704 and 0.618, respectively), whereas health factors were nonlinearly associated with all-cause mortality (p for nonlinear = 0.0043, inflection point = 56.2) (Fig. 3A–C). LE8 was nonlinearly associated with CVD mortality in the MASLD population (p for nonlinear = 0.0156, inflection point = 60), whereas both health behaviors and health factors were linearly associated with CVD mortality (p for nonlinear 0.5551 and 0.3486, respectively) (Fig. 3D–F). Both LE8 and health behaviors were linearly associated with cancer mortality (p for nonlinear 0.2861 and 0.0551, respectively), whereas health factors were not associated with cancer mortality (Fig. 3G–I).

RCS analysis of the association of LE8, health behaviors, and health factors with all-cause, CVD, and cancer mortality in the MASLD population. A: LE8 and all-cause mortality; B: health behaviors and all-cause mortality; C: health factors and all-cause mortality; D: LE8 and CVD mortality; E: health behaviors and CVD mortality; F: health factors and CVD mortality; G: LE8 and cancer mortality; H: health behaviors and cancer mortality; I: health factors and cancer mortality.
Stratified analysis
Interaction analyses indicated that race/ethnicity and PIR significantly influenced the association between LE8 and all-cause mortality in the MASLD population (p for interaction = 0.012 and 0.013, respectively), with a more pronounced association observed in non-Hispanic Black, non-Hispanic White, and other racial populations, as well as in those with a PIR > 3(Fig. 4). However, the association between LE8 and CVD (Fig. 5) and cancer mortality (Fig. 6) in the MASLD population remained stable across all subgroups (all p for interaction > 0.05).

Stratified analysis of the association between LE8 and all-cause mortality in the MASLD population.

Stratified analysis of the association between LE8 and CVD mortality in the MASLD population.

Stratified analysis of the association between LE8 and cancer mortality in the MASLD population.
Sensitivity analysis
The association of le8 with mortality in the masld population remained stable across subgroups of BMI and comorbidities (including diabetes, hypertension, and hyperlipidemia) (p for interaction all > 0.05) (Figure S1–3) Sensitivity analyses using the USFLI to diagnose MASLD yielded broadly consistent results, reinforcing the stability of the conclusions. Similarly, health factors remained non-significantly associated with cancer mortality in MASLD (Table S2–4).
Discussions
This national prospective cohort study, utilizing baseline data from NHANES 2005–2018 and follow-up through December 31, 2019, this national prospective cohort study demonstrated that the AHA’s recently updated LE8 scores were negatively associated with all-cause, CVD, and cancer mortality among the MASLD population, whereas health behaviors and health factors were individually and significantly associated with most of the mortality outcomes, except that health factors and cancer mortality lost significant associations. Maintaining moderate or high CVH was generally associated with significantly lower mortality compared to low CVH. Most of the associations demonstrated a dose-response relationship, except for health factors and all-cause mortality, and LE8 and CVD mortality, which exhibited nonlinear relationships. Race/ethnicity and PIR significantly influenced the association between LE8 and all-cause mortality in the MASLD population, while other associations remained stable across subgroups. These findings suggest that LE8-quantified CVH is independently associated with prognosis in the MASLD population, indicating that adherence to higher CVH is generally associated with reduced mortality among individuals with MASLD. Guiding individuals towards healthy lifestyle and health factor modifications using the LE8 assessment can help prevent excess mortality in the MASLD population and highlights the potential impact of sociodemographic factors.
The LE8 score is a composite measure of cardiovascular health (CVH) proposed and updated by the American Heart Association (AHA)14. The LE8 score integrates eight elements: healthy diet, physical activity, smoking (nicotine exposure), sleep health, healthy weight, and healthy levels of lipids, blood glucose, and blood pressure. It is designed to comprehensively measure and monitor CVH, while promoting improvements in both individual and population health14. The clinical application of the LE8 assessment offers several key benefits. First, it offers physicians a comprehensive, systematic tool for assessing a patient’s CVH status. By considering these eight elements together, physicians can more accurately evaluate cardiovascular risk and develop tailored prevention and treatment programs26. Secondly, the LE8 assessment helps guide patients to make healthy lifestyle adjustments. By understanding their scores on various elements and health behaviors/health factors, individuals can be more targeted to improve their lifestyle habits, such as adjusting dietary structure, increasing physical activity, and improving sleep quality, thereby reducing the risk of CVD and the associated disease burden. In addition, LE8 assessment can be used for epidemiologic studies and public health interventions in large populations. Scoring LE8 in diverse populations allows for an understanding of differences in CVH status across regions, age groups, and genders, providing a scientific basis for developing targeted public health policies27. An important finding was that the association of LE8 with all-cause mortality in the MASLD population was influenced by two important demographic factors, race/ethnicity and PIR. Indeed, extensive epidemiologic studies have demonstrated significant demographic and socioeconomic status (SES) variability in CVH as assessed by LE8 and may explain the association between SES and certain diseases28,29,30,31. Thus, the AHA’s updated LE8 scores offer new perspectives and methodologies for quantitative studies of CVH providing both theoretical and practical support for disease prevention through adherence to higher CVH levels. The two most recent studies one explored the association of le8 with the odds of masld and the other explored the association of le8 with CVD prevalence and mortality in NAFLD populations. These two studies differ from our study exploring the association of le8 with mortality in the masld population. First, masld is the new nomenclature for NAFLD somewhat differentiating it from the diagnosis of NAFLD. In addition, our study comprehensively explored the respective effects of the health behaviors and health factors components of le8 on mortality in masld, which has not been explored in previous studies32,33.
Despite its theoretical significance, there remains limited real-world evidence on the clinical relevance of LE8 in MASLD. Several observational studies have suggested that LE8 is associated with the prevalence and longitudinal incidence of NAFLD in the general population. Wang et al. analyzed 3,588 participants from NHANES 2017–2018 indicating that LE8 was negatively associated with the odds of NAFLD in U.S. adults, with an increase in LE8 per 10 points associated with a 33% lower prevalence15. A prospective cohort study of 3,266 adults without NAFLD at baseline found that individuals with low and intermediate CVH had a significantly higher incidence of NAFLD compared to those with high CVH34. Another prospective cohort study from UK Biobank demonstrated that adherence to a healthy lifestyle (based on BMI, smoking, alcohol consumption, sleep, physical activity, and diet) and moderate/high CVH (compared to low CVH) were both associated with a reduced incidence of severe NAFLD35. However, it remains unclear whether adherence to higher LE8 scores is associated with improved clinical outcomes in the MASLD population.
Several prospective cohort studies have demonstrated that LE8 is negatively associated with all-cause and/or factor-specific mortality in the general population, and that higher CVH is associated with a significantly lower risk of mortality. In a prospective cohort study, Yi et al. included 23,110 adults from NHANES 2005–2014 demonstrating that an increase in LE8 per 10 points was associated with 14% and 19% reductions in all-cause and CVD mortality, respectively, and that being in high CVH (compared with low CVH) reduced all-cause and CVD mortality by 40% and 54%, respectively17. Another study utilizing NHANES 2005–2018 reached similar conclusions and showed that high CVH (compared to low and moderate CVH) explained 33.4% and 42.9% of the reduction in all-cause and CVD mortality, respectively36. Xing et al. included 16,011 CVD-free young adults aged 18–40 years from the Kailuan prospective cohort demonstrating that both baseline CVH and longitudinal CVH change were independently associated with all-cause mortality37. These protective effects were especially pronounced in populations with high polygenic risk scores for CVD38. Other prospective cohort studies have reached similar conclusions, further highlighting the strong potential of maintaining high CVH (as assessed by LE8) in preventing mortality in the general population39,40,41. In addition, adherence to a high CVH may also be associated with a more intuitive extension of life expectancy. Compared to low CVH, those at high CVH lived an average of 8.9 years longer at age 50 regardless of gender42. Similarly, both moderate and high CVH (compared to low CVH) were associated with increased life expectancy free of chronic disease (CVD, diabetes, cancer, and dementia) at age 50 years, whereas high CVH may also reduce life expectancy inequalities due to SES43. In addition its benefits for the general population, cumulative prospective cohort studies have shown that high CVH is associated with reduced mortality in people with specific diseases, including cancer survivors, diabetes, chronic kidney disease, and CVD32,44,45,46. Our study provides new evidence highlighting the public health importance of adherence to high CVH, as assessed by LE8, in preventing mortality in individuals with MASLD, the most common chronic liver disease worldwide.
Adopting a favorable lifestyle remains the cornerstone of management for individuals with MASLD.A substantial body of clinical high-quality evidence suggests that maintaining LE8 healthy behaviors, including high dietary quality, physical active, non-smoking, and appropriate sleep duration, are individually and/or jointly associated with reduced mortality in individuals with NAFLD. Weight loss achieved through lifestyle interventions, such as a healthy diet and physical activity/exercise, has been associated with improved histologic features and regression of fibrosis in NAFLD47. Fibrosis is the most important prognostic factor in NAFLD48, and it is conceivable that these major delays or ameliorations in disease progression may have contributed to the observed reduction in mortality49. Although the clinical relevance of maintaining a healthy lifestyle in MASLD is still underexplored, the clinical course of MASLD closely mirrors that of NAFLD, suggesting that conclusions from NAFLD studies may be applicable to MASLD12,50. LE8 health factors include maintaining a normal BMI and ideal blood lipid, blood glucose, and blood pressure status, abnormalities of which all play an important role in the pathogenesis of MASLD and are key clinical features of MASLD as CMRF51. Notably, our findings suggest that LE8 health factors are not consistently and significantly associated with mortality in the MASLD population, suggesting that maintaining healthy behaviors may have a more dominant role in the prevention of mortality due to specific diseases such as cancer.
Our study had several significant strengths. It was a nationally representative prospective cohort study with a large, multiethnic sample, ensuring generalizability and reliability of results. Our findings provide new insights into the important clinical relevance of LE8 in mortality risk assessment and prevention in MASLD. These results demonstrate importance of maintaining ideal CVH status to improve clinical outcomes in MASLD and are expected to provide new ideas and approaches for mortality prevention in the MASLD population. However, our study had some limitations. First, the assessment of health behaviors in LE8 was primarily based on participant self-report, which may be subject to recall bias. The NHANES self-report questionnaire has been used in a large number of NHANES studies with acceptable accuracy and consistency. In addition, we call for future studies to validate these findings using more accurate assessment methods. However, previous clinical studies using NHANES have assessed the reliability of these methods. The diagnosis of MASLD relied on noninvasive markers rather than imaging, which may affect accuracy. The FLI has been shown to be an accurate diagnostic alternative for SLD, and numerous studies have used it to diagnose MASLD, demonstrating its reliability. Additionally, we conducted a sensitivity analysis using the USFLI, reinforcing the reliability of these findings. Second, NHANES did not collect participant changes in le8 components during follow-up, and thus could not assess the association of cumulative changes in le8 during follow-up with mortality in the masld population. We are acutely aware of this limitation, and thus our findings only suggest that higher baseline scores of le8 are associated with a reduced risk of mortality in the MASLD population, and we were unable to explore the effect of cumulative changes in le8 (e.g., remaining stable, decreasing, or increasing) over the follow-up period on mortality in the MASLD population. This important research gap needs to be addressed by further research.
Conclusions
In a national prospective cohort study, LE8 was found to be negatively associated with all-cause, CVD, and cancer mortality in individuals with MASLD. Health behaviors and factors were significantly associated with most mortality outcomes, except for health factors and cancer mortality. These findings suggest that adherence to higher CVH plays a crucial role in preventing excess mortality in MASLD, particularly among specific racial groups and those with higher PIR. The LE8 assessment of CVH supports targeted modifications to health behaviors and factors, which can help prevent mortality in patients with MASLD, especially those with suboptimal CVH status.
Data availability
This study analyzed publicly available datasets and can be found at https: //www.cdc.gov/nchs/nhanes.
References
Rinella, M. E. et al. A multisociety Delphi consensus statement on new fatty liver disease nomenclature. J. Hepatol. 79 (6), 1542–1556 (2023).
Rinella, M. E. et al. A multisociety Delphi consensus statement on new fatty liver disease nomenclature. Ann. Hepatol. 29 (1), 101133 (2024).
Rinella, M. E. et al. A multisociety Delphi consensus statement on new fatty liver disease nomenclature. Hepatology 78 (6), 1966–1986 (2023).
Miao, L., Targher, G., Byrne, C. D., Cao, Y. Y. & Zheng, M. H. Current status and future trends of the global burden of MASLD. Trends Endocrinol. Metab. (2024).
Kalligeros, M. et al. Prevalence of steatotic liver disease (MASLD, MetALD, and ALD) in the United States: NHANES 2017–2020. Clin. Gastroenterol. Hepatol. 22 (6), 1330–1332e1334 (2024).
Lee, B. P., Dodge, J. L. & Terrault, N. A. National prevalence estimates for steatotic liver disease and subclassifications using consensus nomenclature. Hepatology 79 (3), 666–673 (2024).
Chan, K. E. et al. Longitudinal outcomes Associated with metabolic dysfunction-associated steatotic liver disease: a meta-analysis of 129 studies. Clin. Gastroenterol. Hepatol. 22 (3), 488–498e414 (2024).
Song, R., Li, Z., Zhang, Y., Tan, J. & Chen, Z. Comparison of NAFLD, MAFLD and MASLD characteristics and mortality outcomes in United States adults. Liver Int. 44 (4), 1051–1060 (2024).
Han, E. et al. Mortality in metabolic dysfunction-associated steatotic liver disease: a nationwide population-based cohort study. Metabolism 152, 155789 (2024).
Chan, W. K. et al. Metabolic dysfunction-associated steatotic liver disease (MASLD): a state-of-the-art review. J. Obes. Metab. Syndr. 32 (3), 197–213 (2023).
Lee, H. H. et al. Metabolic dysfunction-associated steatotic liver disease and risk of cardiovascular disease. Gut 73 (3), 533–540 (2024).
Targher, G., Byrne, C. D. & Tilg, H. MASLD: a systemic metabolic disorder with cardiovascular and malignant complications. Gut 73 (4), 691–702 (2024).
Mellemkjær, A., Kjær, M. B., Haldrup, D., Grønbæk, H. & Thomsen, K. L. Management of cardiovascular risk in patients with metabolic dysfunction-associated steatotic liver disease. Eur. J. Intern. Med. 122, 28–34 (2024).
Lloyd-Jones, D. M. et al. Life’s essential 8: updating and enhancing the American heart association’s construct of cardiovascular health: a presidential advisory from the American heart association. Circulation 146 (5), e18–e43 (2022).
Wang, L., Yi, J., Guo, X. & Ren, X. Associations between life’s essential 8 and non-alcoholic fatty liver disease among US adults. J. Transl. Med. 20 (1), 616 (2022).
Ning, N. et al. American heart association’s new ‘life’s essential 8’ score in association with cardiovascular disease: a national cross-sectional analysis. Public Health 225, 336–342 (2023).
Yi, J., Wang, L., Guo, X. & Ren, X. Association of life’s essential 8 with all-cause and cardiovascular mortality among US adults: a prospective cohort study from the NHANES 2005–2014. Nutr. Metab. Cardiovasc. Dis. 33 (6), 1134–1143 (2023).
Krebs-Smith, S. M. et al. Update of the healthy eating index: HEI-2015. J. Acad. Nutr. Diet. 118 (9), 1591–1602 (2018).
Vilar-Gomez, E. et al. High-quality diet, physical activity, and college education are associated with low risk of NAFLD among the US population. Hepatology 75 (6), 1491–1506 (2022).
Ciardullo, S., Carbone, M., Invernizzi, P. & Perseghin, G. Exploring the landscape of steatotic liver disease in the general US population. Liver Int. 43 (11), 2425–2433 (2023).
Bedogni, G. et al. The fatty liver index: a simple and accurate predictor of hepatic steatosis in the general population. BMC Gastroenterol. 6, 33 (2006).
Carli, F. et al. Fatty liver index (FLI) identifies not only individuals with liver steatosis but also at high cardiometabolic risk. Int. J. Mol. Sci. 24 (19). (2023).
Liu, Y. & Chen, M. Dietary and lifestyle oxidative balance scores are independently and jointly associated with nonalcoholic fatty liver disease: a 20 years nationally representative cross-sectional study. Front. Nutr. 10, 1276940 (2023).
Ruhl, C. E. & Everhart, J. E. Fatty liver indices in the multiethnic United States National Health and Nutrition Examination Survey. Aliment. Pharmacol. Ther. 41 (1), 65–76 (2015).
国家区域医疗中心建设 中国卫生 (11):12. (2023).
Koyawala, N. et al. A clinician’s guide to addressing cardiovascular health based on a revised AHA framework. Am. J. Cardiovasc. Dis. 13 (2), 52–58 (2023).
Lloyd-Jones, D. M. et al. Status of cardiovascular health in US adults and children using the American heart association’s new life’s essential 8 metrics: Prevalence estimates from the National Health and Nutrition Examination Survey (NHANES), 2013 through 2018. Circulation 146 (11), 822–835 (2022).
Williams, A. et al. Association of socioeconomic status with life’s essential 8 varies by race and ethnicity. J. Am. Heart Assoc. 12 (18), e029254 (2023).
Zhang, H. et al. The influence of Life’s essential 8 on the link between socioeconomic status and depression in adults: a mediation analysis. BMC Psychiatry 24 (1), 296 (2024).
Williams, A. et al. Association of socioeconomic status with life’s essential 8 in the National Health and Nutrition Examination Survey: Effect modification by sex. J. Am. Heart Assoc. 13 (4), e030805 (2024).
van der Heide, F. C. T. et al. Role of cardiovascular health factors in mediating social inequalities in the incidence of dementia in the UK: two prospective, population-based cohort studies. EClinicalMedicine 70, 102539 (2024).
Huang, L. et al. Life’s essential 8 and risk of all-cause mortality in individuals with cardiovascular diseases: a prospective community-based study. Clin. Cardiol. 47 (2), e24119 (2024).
Sun, M., Qiu, Y., Zhang, L. & Chen, G. The correlation between life’s essential 8 and cardiovascular disease and mortality in individuals with nonalcoholic fatty liver disease: a cross-sectional study. Sci. Rep. 14 (1), 23999 (2024).
Huang, J. et al. Association between updated cardiovascular health construct and risks of non-alcoholic fatty liver disease. Nutr. Metab. Cardiovasc. Dis. 34 (2), 317–325 (2024).
He, P. et al. A healthy lifestyle, life’s essential 8 scores and new-onset severe NAFLD: a prospective analysis in UK Biobank. Metabolism 146, 155643 (2023).
Sun, J. et al. Association of the American heart association’s new Life’s essential 8 with all-cause and cardiovascular disease-specific mortality: prospective cohort study. BMC Med. 21 (1), 116 (2023).
Xing, A. et al. Life’s essential 8’ cardiovascular health with premature cardiovascular disease and all-cause mortality in young adults: the Kailuan prospective cohort study. Eur. J. Prev. Cardiol. 30 (7), 593–600 (2023).
Zhang, J. et al. Relation of Life’s essential 8 to the genetic predisposition for cardiovascular outcomes and all-cause mortality: results from a national prospective cohort. Eur. J. Prev. Cardiol. 30 (15), 1676–1685 (2023).
Isiozor, N. M., Kunutsor, S. K., Voutilainen, A. & Laukkanen, J. A. Life’s essential 8 and the risk of cardiovascular disease death and all-cause mortality in Finnish men. Eur. J. Prev. Cardiol. 30 (8), 658–667 (2023).
Rempakos, A., Prescott, B., Mitchell, G. F., Vasan, R. S. & Xanthakis, V. Association of life’s essential 8 with cardiovascular disease and mortality: the framingham heart study. J. Am. Heart Assoc. 12 (23), e030764 (2023).
Jiang, J. et al. Association of life’s essential 8 with all-cause mortality and risk of cancer: a prospective cohort study. BMC Public Health 24 (1), 1406 (2024).
Ma, H. et al. Cardiovascular health and life expectancy among adults in the United States. Circulation 147 (15), 1137–1146 (2023).
Wang, X. et al. Association of cardiovascular health with life expectancy free of cardiovascular disease, diabetes, cancer, and dementia in UK adults. JAMA Intern. Med. 183 (4), 340–349 (2023).
Sun, Y. et al. Association between Life’s essential 8 score and risk of premature mortality in people with and without type 2 diabetes: a prospective cohort study. Diabetes Metab. Res. Rev. 39 (5), e3636 (2023).
Chen, H. et al. Life’s essential 8 and mortality in US adults with chronic kidney disease. Am. J. Nephrol. 54 (11–12), 516–527 (2023).
López-Bueno, R., Yang, L., Calatayud, J., Andersen, L. L. & Del Pozo Cruz, B. Dose-response association between cardiovascular health and mortality in cancer survivors. Curr. Probl. Cardiol. 49 (1 Pt C), 102176 (2024).
Romero-Gómez, M., Zelber-Sagi, S. & Trenell, M. Treatment of NAFLD with diet, physical activity and exercise. J. Hepatol. 67 (4), 829–846 (2017).
Ekstedt, M. et al. Fibrosis stage is the strongest predictor for disease-specific mortality in NAFLD after up to 33 years of follow-up. Hepatology 61 (5), 1547–1554 (2015).
Vilar-Gomez, E. et al. Significant dose-response association of physical activity and diet quality with mortality in adults with suspected NAFLD in a population study. Am. J. Gastroenterol. 118 (9), 1576–1591 (2023).
Younossi, Z. M. et al. Clinical profiles and mortality rates are similar for metabolic dysfunction-associated steatotic liver disease and non-alcoholic fatty liver disease. J. Hepatol. 80 (5), 694–701 (2024).
Fan, X., Zhang, B., Shi, Y., Liu, L. & Zhao, J. Systemic metabolic abnormalities: key drivers of complications and mortality in MASLD. J. Hepatol. 80 (6), e246–e248 (2024).
Author information
Authors and Affiliations
Contributions
ZL conceived and designed the experiments; XL performed the experiments; YZ analyzed the data; and XN, JG, and JY wrote the manuscript. All authors reviewed and approved the manuscript prior to submission.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics statement
All NHANES protocols were approved by the NCHS Ethics Review Board, and all participants have provided written informed consent.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Li, X., Zhang, Y., Gong, J. et al. Association of life’s essential 8 with all-cause and cause-specific mortality in metabolic dysfunction-associated steatotic liver disease. Sci Rep 14, 30624 (2024). https://doi.org/10.1038/s41598-024-82875-w
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-024-82875-w
Keywords
This article is cited by
-
Pan-immune-inflammation value and mortality in the US adult MASLD: a nonlinear NHANES analysis
BMC Gastroenterology (2025)
