
Abstract
Given the complex relationship between cardiovascular disease (CVD) and chronic kidney disease (CKD), CVD-related markers may serve as CKD biomarkers. We examined associations of three major CVD-markers [mid-regional pro-adrenomedullin (MR-proADM), MR-pro-atrial natriuretic peptide (MR-proANP), and N-terminal pro-B-type natriuretic peptide (NT-proBNP)] with CKD. Cross-sectional analyses included up to 61,830 participants, and longitudinal analyses (NT-proBNP only) 4205 individuals. Kidney function was assessed by estimated glomerular filtration rate (eGFR) using creatinine, cystatin C, or both (eGFRcr-cys). Markers were categorized into four groups. Cross-sectional analyses found that higher levels of all three markers were consistently associated with lower eGFR and higher CKD prevalence. For example, per 1 standard deviation (SD) increase in log-transformed NT-proBNP, corresponding to a 2.71-fold increase in the original concentration, was associated with -2.35 (-2.49, -2.21) ml/min/1.73m2 lower eGFRcr-cys, and the highest NT-proBNP group had a 5.72-fold higher odds of CKDcr-cys (eGFRcr-cys < 60 ml/min/1.73m2) compared with the lowest. Associations with eGFR were stronger among participants with CVD and diabetes. In longitudinal analyses, participants with higher baseline NT-proBNP had faster declines in eGFR, with a 10-year decline of -1.37 (-1.77, -0.98) ml/min/1.73m2 eGFRcr-cys per 1 SD increase, and higher CKD incidence. These findings suggest MR-proADM, MR-proANP, and NT-proBNP as CKD biomarkers.
Similar content being viewed by others

Introduction
Chronic kidney disease (CKD) is characterized by a gradual kidney function decline, with a median prevalence of 9.5% among adults and children worldwide1. Given the asymptomatic onset, early CKD detection remains challenging. Heart and kidneys interact bidirectionally, and a spectrum of disorders involving both organs is termed cardiorenal syndrome2. CKD and cardiovascular disease (CVD) share common risk factors such as diabetes3, and mechanisms of disease development such as overactivation of the renin–angiotensin–aldosterone system (RAAS)4,5. Given their complex interactions, mid-regional pro-adrenomedullin (MR-proADM), MR-pro-atrial natriuretic peptide (MR-proANP), and N-terminal pro-B-type natriuretic peptide (NT-proBNP), some of the prominent CVD-related markers6,7,8,9, may be useful as CKD biomarkers.
MR-proADM, MR-proANP, and NT-proBNP are stable surrogate markers for ADM, ANP, and BNP, respectively, because the latter three markers have shorter half-lives. ANP, BNP, and ADM are all vasodilators. The elevations of these markers in the circulation usually occur in response to ventricular/atrial wall stretch and volume overload7,8,10, which in turn, are positively associated with impaired kidney function3,11. On the other hand, these markers are partially dependent on kidney clearance for elimination, and thus, the elevations of these markers are related to kidney function decline12,13,14,15. The above evidence suggests that these markers could be biomarkers for kidney function decline.
Epidemiological studies have shown that MR-proADM/ADM16,17,18, MR-proANP/ANP16,19, and NT-proBNP/BNP20,21,22,23,24,25,26,27,28,29,30,31, are positively associated with kidney function decline as well as the development and progression of CKD. Our previous study, including 233 proteomic biomarkers, also found that higher levels of ADM and NT-proBNP were associated with a faster kidney function decline and higher CKD incidence32. However, there are only a few studies regarding MR-proADM/ADM and MR-proANP/ANP, which have mainly focused on end-stage kidney disease (ESKD), the last stage of CKD, among patients with diabetes and CKD16,17,18,33, while studies in the general population are scarce19. Given diabetes is a major cause of CKD, the associations may differ between patients with diabetes and the general population, limiting the generalizability of previous findings. To date, the largest study investigating NT-proBNP with incident ESKD comprised 10,749 white and black participants, but they focused on ESKD and found the association differed by ethnicity23. Thus, large studies based on the general population with diverse genetic backgrounds are needed to further understand the associations of these markers with early stages of CKD, which is a more prevalent condition than ESKD.
We aimed to investigate the longitudinal (NT-proBNP only) and cross-sectional associations of MR-proADM, MR-proANP, and NT-proBNP with kidney function and CKD in a large general population from the Biomarkers for Cardiovascular Risk Assessment in Europe (BiomarCaRE) project34. Given they are CVD-related markers and both CVD and diabetes are major CKD causes, we further aimed to assess if the associations differed by CVD and diabetes.
Methods
Study design and population
BiomarCaRE has relied on the European population of the Monitoring of Trends and Determinants in Cardiovascular Diseases (MONICA), Risk, Genetics, Archiving and Monograph (MORGAM) project35. All studies included in BiomarCaRE were conducted in accordance with relevant guidelines and regulations, including the Declaration of Helsinki, and were approved by their respective local ethical committees. The names of the approving committees and approval numbers for each included study are provided in Table S1. For example, the FINRISK Study was approved by the National Public Health Institute of Finland (approval number 38/96). Written informed consent was obtained from all participants. We included seven studies from BiomarCaRE comprising 61,830 participants with data on both NT-proBNP and kidney function: FINRISK Study, MONICA/Cooperative Health Research in the Region of Augsburg (MONICA/KORA), Moli-sani Study, MONICA Brianza Study, Northern Sweden MONICA Study, Prospective Epidemiological Study of Myocardial Infarction Belfast (PRIME/Belfast), and Scottish Heart Health Extended Cohort (SHHEC). Short descriptions of each study are presented in Table S1. Data on MR-proANP (N = 9499) and MR-proADM (N = 9327) were only available in the FINRISK and PRIME/Belfast studies. Harmonized data on age, sex, body mass index, smoking status (current smoker), alcohol consumption, systolic blood pressure, use of antihypertensive medication, high-density lipoprotein cholesterol, low-density lipoprotein cholesterol, triglycerides, history of diabetes, and history of CVD were included. Diabetes (any type of diabetes) and CVD (myocardial ischemia, stroke, and, for some participants in the MONICA Brianza Study, angina pectoris) were assessed based on documented or self-reported history of these conditions. The categories of categorical variables are presented in Table 1. Missing values of covariates, up to 5.7%, were imputed by multiple imputation. For longitudinal analysis, follow-up measurement of kidney function was available in the MONICA/KORA study. Figure S1 shows that a maximum of 4205 participants with 10,208 observations were included in the longitudinal analysis, with a mean follow-up time of 11.1 ± 2.49 years.
Laboratory measurements
Details are presented in Text S1. Briefly, plasma MR-proADM and MR-proANP were measured using immunoluminometric assays. Serum NT-proBNP was measured using an electrochemiluminescence immunoassay. Plasma/serum creatinine was measured by the kinetic alkaline picrate Jaffe method or the enzymatic method. Serum cystatin C was measured using a Latex immunoassay. Table S2 presents intra- and inter-assay coefficients of variation.
Assessment of kidney function and CKD
Kidney function was assessed by estimated glomerular filtration rate (eGFR), with creatinine-based (eGFRcr), cystatin C-based eGFR (eGFRcys), and combined creatinine and cystatin C-based eGFR (eGFRcr-cys), calculated using the Chronic Kidney Disease Epidemiology Collaboration equations (equations are presented in Text S1)36,37. CKD cases were defined as eGFR < 60 ml/min per 1.73m2,38. Incident CKD cases were defined as participants free of CKD at baseline and identified as CKD cases at any stage of the follow-up.
Statistical analysis
All analyses were conducted by R v. 4.3.2 and RStudio v. 2023.12.1.
Transformation of markers
A log10 transformation was applied to each marker, followed by Z-score standardization for comparability across different markers. The standard deviations (SD) of log-transformed markers were 0.43 for NT-proBNP, 0.22 for MR-proANP, and 0.12 for MR-proADM, corresponding approximately to 2.71-, 1.66-, and 1.32-fold increases in their original scale, respectively. Original levels of NT-proBNP were also categorized into four groups (G1, G2, G3, and G4): < 48, 48–125 (including 48), 125–300 (including 125), and ≥ 300 pg/ml. The value of 48 is the median value of NT-proBNP among the 61,830 participants. The values of 125 and 300 are used as thresholds to rule in heart failure (HF) and acute HF, respectively6. Categories of MR-proANP were: < 40, 40–80, 80–120, and ≥ 120 pmol/l. The value of 40 can be used as a threshold to rule out HF, while 120 is used for ruling in acute HF6. These cut-off values of MR-proANP corresponded to the 37.3th, 84.5th (same as value 125 of NT-proBNP among 61,830 participants), and 95.6th percentiles in the participants from the FINRISK and PRIME/Belfast studies. MR-proADM levels were categorized based on cut-off values corresponding to these percentiles: 0.425, 0.609, and 0.766 nmol/l.
Associations with kidney function and CKD
In cross-sectional analysis, linear regression was used to estimate unstandardized β coefficients and 95% confidence intervals (CIs) of eGFR (ml/min/1.73m2) per 1 SD increase in log-transformed markers. Model 1: adjusted for age, sex, and study cohort. Model 2: model 1 plus body mass index, smoking status, alcohol consumption, systolic blood pressure, use of antihypertensive medication, high-density lipoprotein-cholesterol, log-transformed triglycerides, history of diabetes, and history of CVD. The same linear regression models were applied for grouped markers (G1-4), with G1 serving as the reference group. Logistic regression was used to estimate odds ratios (ORs) and 95% CIs for the association between biomarker levels (both log10-transformed and grouped) and prevalent CKD. In sensitivity analyses, CKD cases were redefined as all three eGFR < 60 ml/min per 1.73m2 and non-cases as all three eGFR ≥ 60 ml/min per 1.73m2.
In longitudinal analysis in the MONICA/KORA study, linear mixed-effects models were used to investigate the associations of NT-proBNP with change in eGFR, using “lme4” package. The follow-up duration was used as the timescale and divided by 10 to give a 10-year change. The fixed effects included standardized log-transformed NT-proBNP, follow-up duration, and their interaction terms, while random effects included random intercept and random slope (i.e., individual differences in eGFR change). The β coefficient of the interaction term is the impact of NT-proBNP on the 10-year change in eGFR. The same models were applied for grouped NT-proBNP (G1-4), with G1 serving as the reference group. Participants with at least one follow-up measurement on eGFR were included. For associations with incident CKD, interval-censored Cox regression models with 1000 bootstrap samples for 95% CIs estimation were performed, using “icenReg” package. The first two models in longitudinal analyses were similar to the cross-sectional analysis, with the exclusion of study cohort, and model 3 further adjusted for baseline eGFR. Since model 3 may be overcorrected39, we used model 2 as our main model. Linear mixed-effects models included time-varying covariates, except for sex. To address bias due to participants lost to follow-up (Figure S1), inverse probability weighting-weights were applied in all longitudinal analyses (details in Text S2).
Stratified and sensitivity analyses
Interaction terms of standardized log-transformed markers with CVD or diabetes were included in the aforementioned final models in both cross-sectional and longitudinal analyses, and stratified analyses were performed if a significant interaction (p < 0.05) was found. Sensitivity analyses were conducted by further adjusting for low-density lipoprotein cholesterol, and E-values40 were calculated to assess the robustness of observed associations to potential unmeasured or uncontrolled confounders.
Non-linear associations analysis
Restricted cubic spline functions with three knots were used to investigate the non-linear associations of original levels of three markers with prevalent CKDcr-cys in logistic regression models and non-linear associations of NT-proBNP with incident CKD in Cox proportional hazards models, adjusting for the covariates as in the aforementioned final models, using “rms” package. Participants with levels of markers < 2.5th percentile or > 97.5th percentile were excluded. P-values for nonlinearity were calculated using ANOVA tests.
Results
The 61,830 participants included in the cross-sectional analysis had an average age of 51.8 ± 12.5 years (Table 1), and characteristics of participants across study cohorts are presented in Table S3 & S4. The baseline characteristics of participants from the MONICA/KORA study included in the longitudinal analysis are shown in Table S5.
Cross-sectional associations
Higher levels of three myocardial stress markers were associated with lower eGFR across all three eGFR assessments (Table S6 & Fig. 1A). In model 2, the β (95% CIs) of eGFRcr-cys per 1 SD increase in log-transformed markers were −2.35 (−2.49, −2.21) ml/min/1.73m2 for NT-proBNP, −2.93 (−3.30, −2.57) for MR-proANP, and −5.60 (−5.94, −5.26) for MR-proADM, respectively (Table 2). A 1 SD increase on the log₁₀ scale corresponds approximately to 2.71-, 1.66-, and 1.32-fold increases in the original concentrations. Figure S2 shows that compared with G1, G2-G4 with higher levels of markers had significantly lower eGFR. For instance, β (95% CIs) of eGFRcr-cys for G2-G4 compared with G1 of NT-proBNP in model 2 were −1.41 (−1.69, −1.14), −4.10 (−4.52, −3.68), and −11.2 (−11.8, −10.5), respectively (Table 2).

Cross-sectional associations of 3 myocardial stress markers with kidney function and CKD. (A). Linear regression was used to estimate beta coefficients and 95% CI of eGFR per 1 SD increase in log-transformed markers. (B). Logistic regression was used to estimate odds ratios of CKD. Detailed information on adjusted models is described in Table 2 & 3. Data from 61,830 participants for NT-proBNP, 9499 for MR-proANP, and 9327 for MR-proADM were included in these analyses. CI, confidence interval; CKD, chronic kidney disease; cr, creatinine-based; cys, cystatin C-based; cr-cys, combined creatinine and cystatin C-based; eGFR, estimated glomerular filtration rate; MR-proADM, mid-regional pro-adrenomedullin; MR-proANP, mid-regional pro-atrial natriuretic peptide; NT-proBNP, N-terminal pro-B-type natriuretic peptide; SD, standard deviation; * p < 0.05, ** p < 0.01, *** p < 0.001.
Results for CKD showed consistent associations, with higher levels of three markers associated with a higher prevalence of CKD across all three CKD assessments (Table S7 & Fig. 1B). Fully-adjusted ORs (95% CIs) of CKDcr-cys per 1 SD increase in log-transformed markers were, 1.81 (1.72, 1.90) for NT-proBNP, 1.80 (1.58, 2.05) for MR-proANP, and 3.04 (2.65, 3.48) for MR-proADM, respectively (Table 3). Associations with categories of markers also revealed significantly higher CKD prevalence in G2-G4 compared with G1, with G4 demonstrating the strongest associations (Figure S3). For example, Table 3 shows that fully-adjusted ORs (95% CIs) of CKDcr-cys across G2-G4 compared with G1 of NT-proBNP were 1.37 (1.19, 1.58), 2.56 (2.19, 2.99), and 5.72 (4.82, 6.78). In sensitivity analyses using redefined CKD cases, the association with per 1 SD increase in log-transformed markers remained significant with higher ORs but wider 95% CIs (Table S8 & Figure S4).
Longitudinal associations
Participants with higher baseline NT-proBNP levels had faster eGFR declines during follow-up (Table 4 & Fig. 2). In model 2, the β (95% CIs) of a 10-year decline in eGFRcr-cys per 1 SD increase in log-transformed NT-proBNP were −1.37 (−1.77, −0.98) ml/min/1.73m2/10-year, and −1.04 (−1.88, −0.20), −3.37 (−4.66, −2.07), and −7.28 (−9.92, −4.64) for G2-4 compared with G1. Regarding incident CKD, we observed 179 incident CKDcr-cys cases/30,856 person-years during follow-up. Baseline NT-proBNP levels were positively associated with incident CKD across all three incident CKD assessments (Table S9 & Fig. 3). In model 2, hazard ratio (95% CIs) was 1.39 (1.20, 1.62) per 1 SD increase in log-transformed NT-proBNP for incident CKDcr-cys. For categories of NT-proBNP, G4 shows significantly higher risks of incident CKD compared with G1 of NT-proBNP, with hazard ratio of 4.40 (2.63, 7.36) for incident CKDcr-cys. In model 3, further adjusting for baseline eGFR in longitudinal analyses, all significant associations of log-transformed NT-proBNP and G4 compared with G1 remained significant (Table 4 & Table S9).

Longitudinal associations of NT-proBNP with 10-year change in kidney function. Linear mixed-effects model was used to estimate beta coefficients and 95% CI of the change in eGFR for G2-4 compared with G1 of NT-proBNP, as well as for per 1 SD increase in log-transformed NT-proBNP. The follow-up duration was used as a timescale and divided by 10 to give a 10-year change. Detailed information on adjusted models is described in Table 4. A maximum of 4205 participants with 10,208 observations were included in these analyses. Categories of NT-proBNP: G1: < 48; G2: 48–125; G3: 125–300; G4: ≥ 300 pg/ml. CI, confidence interval; G, group; eGFR, estimated glomerular filtration rate; eGFRcr, creatinine-based eGFR; eGFRcys, cystatin C-based eGFR; eGFRcr-cys, creatinine and cystatin C-based eGFR; NT-proBNP, N-terminal pro-B-type natriuretic peptide; SD, standard deviation; * p < 0.05, ** p < 0.01, *** p < 0.001.

Longitudinal associations of NT-proBNP with incident CKD. Interval-censored Cox regression was used to estimate HR and 95% CI (1000 bootstrap samples for 95% CI estimation) of incident CKD for G2-4 compared with G1 of NT-proBNP, as well as for per 1 SD increase in log-transformed NT-proBNP. A total of 4167 participants free of CKDcr, 2557 free of CKDcys, and 2621 free of CKDcr-cys at baseline were included in these analyses. Detailed results are presented in Table S9. Categories of NT-proBNP: G1: < 48; G2: 48–125; G3: 125–300; G4: ≥ 300 pg/ml. CI, confidence interval; CKD, chronic kidney disease; CKDcr, creatinine-based CKD; CKDcys, cystatin C-based CKD; CKDcr-cys, creatinine and cystatin C-based CKD; G, group; HR, hazard ratio; NT-proBNP, N-terminal pro-B-type natriuretic peptide; SD, standard deviation; * p < 0.05, ** p < 0.01, *** p < 0.001.
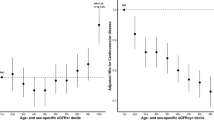
Stratified analysis by CVD/diabetes
Significant interactions with both CVD and diabetes were mainly found in the cross-sectional analyses with eGFR (P-interaction < 0.05, Fig. 4). In stratified analyses, significant inverse associations of three markers with eGFR were observed in both participants with and without CVD or diabetes, while the associations were stronger among participants with diabetes or CVD (Table S10-S12). For example, the β (95% CIs) of eGFRcr-cys per 1 SD increase in log-transformed NT-proBNP were −2.13 (−2.27, −1.98) ml/min/1.73m2 among participants without CVD and −4.76 (−5.32, −4.20) among participants with CVD, respectively. Similar results were observed for MR-proANP and MR-proADM. For interaction analysis for prevalent CKD, only a few significant interactions were observed (Figure S5). For instance, interaction with diabetes among associations of MR-proADM with CKDcr-cys, and the associations were stronger among participants with diabetes. In longitudinal analysis, although significant interactions of NT-proBNP with CVD were observed among associations with incident CKDcr-cys (P-interaction < 0.05, Figure S6), there was no significant difference in associations among participants with and without CVD, probably due to small sample size in participants with CVD.

Cross-sectional associations of 3 myocardial stress markers with kidney function stratified by CVD and diabetes. Interaction terms of standardized log-transformed markers with CVD or diabetes were included in linear regression, applying model 2 described in Table 2, to test the significance of interaction. Data from 61,830 participants for NT-proBNP, 9499 for MR-proANP, and 9327 for MR-proADM were included in these analyses. Please refer to Table S10-12 for detailed results. CVD, cardiovascular disease; eGFR, estimated glomerular filtration rate; eGFRcr, creatinine-based eGFR; eGFRcys, cystatin C-based eGFR; eGFRcr-cys, creatinine and cystatin C-based eGFR; MR-proADM, mid-regional pro-adrenomedullin; MR-proANP, mid-regional pro-atrial natriuretic peptide; NT-proBNP, N-terminal pro-B-type natriuretic peptide; SD, standard deviation; * p < 0.05, ** p < 0.01, *** p < 0.001.
Non-linear associations
A modest non-linear association of NT-proBNP with the prevalence of CKDcr-cys in cross-sectional analysis was observed (Figure S7, P-nonlinear = 0.012). The shape of the associations tended to be steeper after reaching an NT-proBNP level of around 200 pg/ml. For MR-proADM and MR-proANP, the shape of the associations also tended to be steeper for marker levels above G3, but with P-nonlinear > 0.05. Investigating NT-proBNP and incident CKD in the longitudinal analyses found no evidence of nonlinearity (Figure S8, P-nonlinear > 0.05).
Discussion
In the present study, we investigated the associations of MR-proADM, MR-proANP, and NT-proBNP with kidney function and CKD in the general population based on pooled individual-level data from several large population-based studies. Cross-sectional analysis found that higher levels of these markers were associated with lower kidney function and a higher prevalence of CKD. Similarly, longitudinal analysis based on the MONICA/KORA study found that higher baseline NT-proBNP levels were associated with faster kidney function decline and a higher incidence of CKD. We observed significant interaction effects with CVD and diabetes mainly in the cross-sectional analyses of kidney function, with the associations being more pronounced among participants with CVD or diabetes. To the best of our knowledge, the present study has the largest sample size among cross-sectional studies in the field.
Our findings for NT-proBNP are consistent with most previous studies. A European general population-based study consisting of 8121 participants found an inverse cross-sectional association between serum NT-proBNP and kidney function41. Similar associations have also been observed in a cross-sectional study based on the Northern Sweden MONICA Study (N = 10,185)42, and two small cross-sectional studies among patients with hypertension (N = 207)43 or acute HF (N = 138)44. Several community-based cohort studies, including two Japanese20,21 and one American studies22, have also reported positive associations of serum/plasma NT-proBNP with faster kidney function decline and CKD incidence. Another cohort study reported a positive association of baseline plasma NT-proBNP with incident ESKD23. Various cohort studies among CKD patients have reported positive associations of circulating NT-proBNP with incident ESKD and other adverse CKD outcomes24,25,26,27,28,29,30. Collectively, circulating NT-proBNP exhibits strong associations with kidney function and kidney diseases.
Findings for MR-proANP and MR-proADM are also consistent with previous studies. A cohort study comprising 294 Japanese residents reported a positive association of plasma ANP with incident CKD19. Another cohort found that plasma MR-proANP and MR-proADM were positively associated with the progression of CKD among 177 CKD patients from three European countries16. Positive associations of MR-proADM with severe kidney outcomes such as incident ESKD have also been reported in cohort studies conducted among patients with diabetes17,18. Two clinical trials have reported that starting human ANP infusion at the beginning of heart bypass surgery improves postoperative kidney function in patients, regardless of their CKD status45,46. In another clinical trial, HF patients treated with the angiotensin-neprilysin inhibition LCZ696, a drug that suppresses the RAAS and increases natriuretic peptides levels, had a significantly lower mortality rate and a non-significantly lower kidney dysfunction incidence, compared to those treated with enalaprilin47. The above findings indicate the potential of MR-proANP and MR-proADM as biomarkers of kidney function decline.
In the present study, in extension to previous work, significant interactions of MR-proADM, MR-proANP, and NT-proBNP with CVD and diabetes on the cross-sectional associations with kidney function were observed, with the associations being more pronounced among participants with CVD and diabetes. This could be partially explained by the fact that both CVD and diabetes are important risk factors for the development of CKD, and thus, these individuals may be more susceptible to the impact of these markers on kidney function38,48. Results of non-linear associations could also support CVD-stratified results. Although no convincing non-linear associations were confirmed, the shapes of associations tended to become steeper with increasing marker levels. Since higher levels of these markers are strongly associated with CVD, the observed steeper associations with higher marker levels were similar to CVD-stratified results. Our findings suggest the importance of monitoring these markers, particularly in individuals with CVD or diabetes.
The precise mechanisms remain elusive. The elevation of these markers, as well as their active forms ADM, ANP, and BNP in the circulation, can be attributed to conditions such as ventricular/atrial wall stretch and volume overload. ADM, ANP, and BNP counteract these conditions through multiple effects, including vasodilatory, natriuretic, and diuretic effects, partially by inhibiting the actions of RAAS7,8,12. Chronic and excessive presence of these conditions can result in impaired cardiac function, such as cardiac output decrease, thereby contributing to an overactivation of RAAS, a key player in CKD development11. On the other hand, kidney function decline can lead to an accumulation of these markers in the circulation12,13,14,15. Nonetheless, compelling evidence has suggested that cardiac pathology remains the primary determinant for elevation of these markers8,49. Given the intricate interplay between the heart and kidneys, these markers may serve as valuable biomarkers for disorders involving both organs, such as the cardiorenal syndrome.
Key strengths of our study include the largest sample size derived from the general population in the cross-sectional analysis, and the estimation of kidney function using creatinine and/or cystatin C. Several limitations should also be acknowledged. First, in longitudinal analysis, data were only available in a restricted dataset and only baseline NT-proBNP was considered, and thus, we were unable to explore the impact of dynamic changes in NT-proBNP over time. Second, the counterintuitively inverse associations between obesity and levels of natriuretic peptides (e.g., MR-proANP and NT-proBNP), as reported in previous studies50, may have had impacts on our observed associations, despite our adjustment for body mass index. Third, the definition of CKD cases using a single creatinine and/or cystatin C measurement, and different assays across surveys, as well as the lack of follow-up confirmatory tests after a certain period such as three months, could potentially result in misclassification. However, sensitivity analysis of redefined CKD showed robust results. In addition, this study was conducted in a general population, and consequently, our data are not well-suited to establish clinically applicable cut-off values for these markers in relation to CKD. Fourth, analyses of MR-proADM and MR-proANP were only based on cross-sectional data, but our study contributes significantly to the existing literature due to its large general population-based sample size. Finally, data on albuminuria, hemoglobin A1c, specific classes of antihypertensive or antidiabetic medications, and inflammatory markers were not uniformly available across cohorts, and thus, residual confounding by these factors can not be excluded. In addition, unmeasured or uncontrolled confounders (e.g., medications that affect both the levels of these makers and kidney function) may have had impacts on the observed associations, but our sensitivity analyses and E-values suggested that our results were robust to potential unmeasured or uncontrolled confounders (Table S13-15).
In conclusion, our study found cross-sectional associations of higher levels of MR-proADM, MR-proANP, and NT-proBNP with lower kidney function and a higher prevalence of CKD, with the associations being more pronounced among individuals with CVD and diabetes. Moreover, higher NT-proBNP levels were also associated with faster kidney function decline and a higher incidence of CKD. Our findings indicate the potential utility of these myocardial stress markers as valuable biomarkers of kidney health, particularly in the context of comorbidities such as CVD and diabetes. Further research is warranted to include additional unmeasured or uncontrolled confounders and understand the underlying mechanisms driving these associations. Moreover, future studies with standardized CKD measurements in clinical settings are needed to establish clinically applicable cut-off values for these myocardial stress markers.
Data and materials availability
The MORGAM/BiomarCaRE data are not available in a public repository. Access to the data is restricted by the ethical approvals and the legislation of the European Union and the countries of each study. Approval by the Principal Investigator of each cohort study and the MORGAM/BiomarCaRE Steering Group will be required for release of the data. The MORGAM Manual at https://www.thl.fi/publications/morgam/manual/contents.htm gives more information on access to the data. The informed consent given by MONICA/KORA study participants does not cover data posting in public databases. Cooperation partners can obtain permission to use MONICA/KORA data under the terms of a project agreement (https://helmholtz-muenchen.managed-otrs.com/external).
Abbreviations
- BiomarCaRE:
-
Biomarkers for Cardiovascular Risk Assessment in Europe
- CI:
-
Confidence interval
- CKD:
-
Chronic kidney disease
- CKD-EPI:
-
Chronic kidney disease epidemiology collaboration
- cr:
-
Creatinine-based
- cr-cys:
-
Combined creatinine and cystatin C-based
- CVD:
-
Cardiovascular disease
- cys:
-
Cystatin C-based
- eGFR:
-
Estimated glomerular filtration rate
- ESKD:
-
End-stage kidney disease
- G:
-
Group
- HF:
-
Heart failure
- KORA:
-
Cooperative Health Research in the Region of Augsburg
- MONICA:
-
Monitoring of Trends and Determinants in Cardiovascular Diseases
- MORGAM:
-
Monitoring of Trends and Determinants in Cardiovascular Diseases Risk, Genetics, Archiving and Monograph
- MR-proADM:
-
Mid-regional pro-adrenomedullin
- MR-proANP:
-
Mid-regional pro-atrial natriuretic peptide
- NT-proBNP:
-
N-terminal pro-B-type natriuretic peptide
- OR:
-
Odds ratio
- RAAS:
-
Renin–angiotensin–aldosterone system
- SD:
-
Standard deviation
References
Bello, A. K. et al. An update on the global disparities in kidney disease burden and care across world countries and regions. Lancet Glob Health 12, e382–e395. https://doi.org/10.1016/S2214-109X(23)00570-3 (2024).
Rangaswami, J. et al. Cardiorenal Syndrome: Classification, Pathophysiology, Diagnosis, and Treatment Strategies: A Scientific Statement From the American Heart Association. Circulation 139, e840–e878. https://doi.org/10.1161/CIR.0000000000000664 (2019).
Laffin, L. J. & Bakris, G. L. Intersection Between Chronic Kidney Disease and Cardiovascular Disease. Curr Cardiol Rep 23, 117. https://doi.org/10.1007/s11886-021-01546-8 (2021).
Ravarotto, V., Simioni, F., Pagnin, E., Davis, P. A. & Calo, L. A. Oxidative stress - chronic kidney disease - cardiovascular disease: A vicious circle. Life Sci 210, 125–131. https://doi.org/10.1016/j.lfs.2018.08.067 (2018).
Gargiulo, R., Suhail, F. & Lerma, E. V. Cardiovascular disease and chronic kidney disease. Dis. Mon. 61, 403–413. https://doi.org/10.1016/j.disamonth.2015.07.005 (2015).
McDonagh, T. A. et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur. Heart. J. 42, 3599–3726. https://doi.org/10.1093/eurheartj/ehab368 (2021).
Czajkowska, K. et al. Mid-Regional Proadrenomedullin as a New Biomarker of Kidney and Cardiovascular Diseases-Is It the Future?. J. Clin. Med. https://doi.org/10.3390/jcm10030524 (2021).
Voors, A. A. et al. Adrenomedullin in heart failure: pathophysiology and therapeutic application. Eur. J. Heart Fail 21, 163–171. https://doi.org/10.1002/ejhf.1366 (2019).
Neumann, J. T. et al. Prognostic Value of Cardiovascular Biomarkers in the Population. JAMA 331, 1898–1909. https://doi.org/10.1001/jama.2024.5596 (2024).
Kuwahara, K. The natriuretic peptide system in heart failure: Diagnostic and therapeutic implications. Pharmacol Ther 227, 107863. https://doi.org/10.1016/j.pharmthera.2021.107863 (2021).
Patel, N., Yaqoob, M. M. & Aksentijevic, D. Cardiac metabolic remodelling in chronic kidney disease. Nat Rev Nephrol 18, 524–537. https://doi.org/10.1038/s41581-022-00576-x (2022).
Nishikimi, T. Adrenomedullin in the kidney-renal physiological and pathophysiological roles. Curr Med Chem 14, 1689–1699. https://doi.org/10.2174/092986707780830943 (2007).
Volpe, M. Natriuretic peptides and cardio-renal disease. Int J Cardiol 176, 630–639. https://doi.org/10.1016/j.ijcard.2014.08.032 (2014).
van Kimmenade, R. R. et al. Renal clearance of B-type natriuretic peptide and amino terminal pro-B-type natriuretic peptide a mechanistic study in hypertensive subjects. J Am Coll Cardiol 53, 884–890. https://doi.org/10.1016/j.jacc.2008.11.032 (2009).
Tsutamoto, T., Sakai, H., Yamamoto, T. & Nakagawa, Y. Renal Clearance of N-Terminal pro-Brain Natriuretic Peptide Is Markedly Decreased in Chronic Kidney Disease. Circ Rep 1, 326–332. https://doi.org/10.1253/circrep.CR-19-0063 (2019).
Dieplinger, B. et al. Pro-A-type natriuretic peptide and pro-adrenomedullin predict progression of chronic kidney disease: the MMKD Study. Kidney Int 75, 408–414. https://doi.org/10.1038/ki.2008.560 (2009).
Saulnier, P. J. et al. Association of Circulating Biomarkers (Adrenomedullin, TNFR1, and NT-proBNP) With Renal Function Decline in Patients With Type 2 Diabetes: A French Prospective Cohort. Diabetes Care 40, 367–374. https://doi.org/10.2337/dc16-1571 (2017).
Velho, G. et al. Plasma Adrenomedullin and Allelic Variation in the ADM Gene and Kidney Disease in People With Type 2 Diabetes. Diabetes 64, 3262–3272. https://doi.org/10.2337/db14-1852 (2015).
Ogawa, N., Komura, H., Kuwasako, K., Kitamura, K. & Kato, J. Plasma levels of natriuretic peptides and development of chronic kidney disease. BMC Nephrol 16, 171. https://doi.org/10.1186/s12882-015-0163-9 (2015).
Sasaki, T. et al. N-Terminal Pro-B-Type Natriuretic Peptide and Incident CKD. Kidney Int Rep 6, 976–985. https://doi.org/10.1016/j.ekir.2021.01.006 (2021).
Nakayama, S. et al. N-Terminal Pro-B-Type Natriuretic Peptide Is a Predictor of Chronic Kidney Disease in an Asian General Population-The Ohasama Study. Circ Rep 2, 24–32. https://doi.org/10.1253/circrep.CR-19-0044 (2019).
Bansal, N. et al. NT-proBNP and troponin T and risk of rapid kidney function decline and incident CKD in elderly adults. Clin J Am Soc Nephrol 10, 205–214. https://doi.org/10.2215/CJN.04910514 (2015).
Kim, Y. et al. Association of high-sensitivity cardiac troponin T and natriuretic peptide with incident ESRD: the Atherosclerosis Risk in Communities (ARIC) study. Am J Kidney Dis 65, 550–558. https://doi.org/10.1053/j.ajkd.2014.08.021 (2015).
Zhao, Y. et al. The association of plasma NT-proBNP level and progression of diabetic kidney disease. Ren Fail 45, 2158102. https://doi.org/10.1080/0886022X.2022.2158102 (2023).
Anderson, A. H. et al. Novel Risk Factors for Progression of Diabetic and Nondiabetic CKD: Findings From the Chronic Renal Insufficiency Cohort (CRIC) Study. Am. J. Kidney Dis. 77(56–73), e51 (2021).
Bansal, N. et al. Cardiac and Stress Biomarkers and Chronic Kidney Disease Progression: The CRIC Study. Clin Chem 65, 1448–1457. https://doi.org/10.1373/clinchem.2019.305797 (2019).
Yoshitomi, R. et al. Plasma B-type natriuretic peptide concentration is independently associated with kidney function decline in Japanese patients with chronic kidney disease. J Hypertens 34, 753–761. https://doi.org/10.1097/HJH.0000000000000847 (2016).
Sundqvist, S. et al. Clinical Value of Natriuretic Peptides in Predicting Time to Dialysis in Stage 4 and 5 Chronic Kidney Disease Patients. PLoS ONE 11, e0159914. https://doi.org/10.1371/journal.pone.0159914 (2016).
Desai, A. S. et al. Association between cardiac biomarkers and the development of ESRD in patients with type 2 diabetes mellitus, anemia, and CKD. Am J Kidney Dis 58, 717–728. https://doi.org/10.1053/j.ajkd.2011.05.020 (2011).
Spanaus, K. S. et al. B-type natriuretic peptide concentrations predict the progression of nondiabetic chronic kidney disease: the Mild-to-Moderate Kidney Disease Study. Clin. Chem. 53, 1264–1272. https://doi.org/10.1373/clinchem.2006.083170 (2007).
Ascher, S. B. et al. Changes in Natriuretic Peptide Levels and Subsequent Kidney Function Decline in the SPRINT Trial. Am J Kidney Dis 83, 615-623.e611. https://doi.org/10.1053/j.ajkd.2023.09.018 (2023).
Lin, J. S. et al. Proteomic profiling of longitudinal changes in kidney function among middle-aged and older men and women: the KORA S4/F4/FF4 study. BMC Med. 21, 245. https://doi.org/10.1186/s12916-023-02962-z (2023).
Landman, G. W. et al. Midregional fragment of proadrenomedullin, new-onset albuminuria, and cardiovascular and all-cause mortality in patients with type 2 diabetes (ZODIAC-30). Diabetes Care 37, 839–845. https://doi.org/10.2337/dc13-1852 (2014).
Zeller, T. et al. BiomarCaRE: rationale and design of the European BiomarCaRE project including 300,000 participants from 13 European countries. Eur. J. Epidemiol. 29, 777–790. https://doi.org/10.1007/s10654-014-9952-x (2014).
Evans, A. et al. MORGAM (an international pooling of cardiovascular cohorts). Int. J. Epidemiol. 34, 21–27. https://doi.org/10.1093/ije/dyh327 (2005).
Inker, L. A. et al. New Creatinine- and Cystatin C-Based Equations to Estimate GFR without Race. N. Engl J. Med. 385, 1737–1749. https://doi.org/10.1056/NEJMoa2102953 (2021).
Inker, L. A. et al. Estimating glomerular filtration rate from serum creatinine and cystatin C. N. Engl. J. Med. 367, 20–29. https://doi.org/10.1056/NEJMoa1114248 (2012).
Webster, A. C., Nagler, E. V., Morton, R. L. & Masson, P. Chronic Kidney Disease. Lancet 389, 1238–1252. https://doi.org/10.1016/S0140-6736(16)32064-5 (2017).
Glymour, M. M., Weuve, J., Berkman, L. F., Kawachi, I. & Robins, J. M. When is baseline adjustment useful in analyses of change? An example with education and cognitive change. Am. J. Epidemiol. 162, 267–278. https://doi.org/10.1093/aje/kwi187 (2005).
Ding, P. & VanderWeele, T. J. Sensitivity Analysis Without Assumptions. Epidemiology 27, 368–377. https://doi.org/10.1097/EDE.0000000000000457 (2016).
Scheven, L. et al. High-sensitive troponin T and N-terminal pro-B type natriuretic peptide are associated with cardiovascular events despite the cross-sectional association with albuminuria and glomerular filtration rate. Eur. Heart J. 33, 2272–2281. https://doi.org/10.1093/eurheartj/ehs163 (2012).
de Man Lapidoth, J. et al. Trends in renal function in Northern Sweden 1986–2014: data from the seven cross-sectional surveys within the Northern Sweden MONICA study. BMJ Open 13, e072664. https://doi.org/10.1136/bmjopen-2023-072664 (2023).
Yang, Y., Wang, Y., Shi, Z. W., Zhu, D. L. & Gao, P. J. Association of E/E’ and NT-proBNP with renal function in patients with essential hypertension. PLoS ONE 8, e54513. https://doi.org/10.1371/journal.pone.0054513 (2013).
Manzano-Fernandez, S. et al. Impact of kidney dysfunction on plasma and urinary N-terminal pro-B-type natriuretic peptide in patients with acute heart failure. Congest Heart Fail 16, 214–220. https://doi.org/10.1111/j.1751-7133.2010.00153.x (2010).
Sezai, A. et al. Results of low-dose human atrial natriuretic peptide infusion in nondialysis patients with chronic kidney disease undergoing coronary artery bypass grafting: the NU-HIT (Nihon University working group study of low-dose HANP Infusion Therapy during cardiac surgery) trial for CKD. J Am Coll Cardiol 58, 897–903. https://doi.org/10.1016/j.jacc.2011.03.056 (2011).
Sezai, A. et al. Influence of continuous infusion of low-dose human atrial natriuretic peptide on renal function during cardiac surgery: a randomized controlled study. J Am Coll Cardiol 54, 1058–1064. https://doi.org/10.1016/j.jacc.2009.05.047 (2009).
McMurray, J. J. et al. Angiotensin-neprilysin inhibition versus enalapril in heart failure. N Engl J Med 371, 993–1004. https://doi.org/10.1056/NEJMoa1409077 (2014).
Francis, A. et al. Chronic kidney disease and the global public health agenda: an international consensus. Nat Rev Nephrol 20, 473–485. https://doi.org/10.1038/s41581-024-00820-6 (2024).
Kula, A. & Bansal, N. Applications of cardiac biomarkers in chronic kidney disease. Curr Opin Nephrol Hypertens 31, 534–540. https://doi.org/10.1097/MNH.0000000000000829 (2022).
Madamanchi, C., Alhosaini, H., Sumida, A. & Runge, M. S. Obesity and natriuretic peptides, BNP and NT-proBNP: mechanisms and diagnostic implications for heart failure. Int J Cardiol 176, 611–617. https://doi.org/10.1016/j.ijcard.2014.08.007 (2014).
Acknowledgements
We thank the participants and the staff of the cohorts included in MORGAM/BiomarCaRE for their continuing dedication and efforts. We thank all participants for their long-term commitment to the MONICA/KORA studies, the staff for data collection and research data management and the members of the MONICA/KORA Study Group (https://www.helmholtz-munich.de/en/epi/cohort/kora) who are responsible for the design and conduct of the study. JSL would like to thank the China Scholarship Council (CSC) for the financial support (No. 202008440343).
Funding
Open Access funding enabled and organized by Projekt DEAL. The MORGAM Project has received funding from EU projects MORGAM (Biomed, BMH4-CT98-3183), GenomEUtwin (FP5, QLG2-CT-2002–01254), ENGAGE (FP7, HEALTH-F4-2007–201413), CHANCES (FP7, HEALTH-F3-2010–242244), BiomarCaRE (FP7, HEALTH-F2-2011–278913), euCanSHare (Horizon 2020, No. 825903) and AFFECT-EU (Horizon 2020, No. 847770); and Medical Research Council, London (G0601463, No. 80983: Biomarkers in the MORGAM Populations). This has supported central coordination, workshops and part of the activities of the MORGAM Data Centre, the MORGAM Laboratories and the MORGAM Participating Centres. The MONICA/KORA study was initiated and financed by the Helmholtz Zentrum München – German Research Center for Environmental Health, which is funded by the German Federal Ministry of Education and Research (BMBF) and by the State of Bavaria. Data collection in the MONICA/KORA study is done in cooperation with the University Hospital of Augsburg. Northern Sweden MONICA was funded by the county councils in Norr- and Västerbotten, Umeå University, Swedish Research Council and Swedish Heart and Lung Foundation. The funders had no role in study design, data collection, analysis, decision to publish, or preparation of the manuscript.
Author information
Authors and Affiliations
Contributions
JSL designed the study, drafted the analysis plan, performed the statistical analysis, interpreted the data, and wrote the first draft of the manuscript. TZ, WK, PJ, FK, LI, HTP, SS, GC, LP, VS, RDP, CD, KK, SB, AP, and BT contributed data. TL contributed to data curation. JDML contributed to the conception of the study and revised the manuscript. AP contributed to the analysis plan. BT designed the study and contributed to the analysis plan and data interpretation. All authors read and approved the final manuscript. JSL and BT had primary responsibility for the final content.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Lin, Js., Zeller, T., Koenig, W. et al. Longitudinal and cross-sectional associations of myocardial stress markers with kidney function and chronic kidney disease in the BiomarCaRE project. Sci Rep 16, 7488 (2026). https://doi.org/10.1038/s41598-026-37377-2
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41598-026-37377-2
