
Abstract
Background
Human biomonitoring (HBM) plays a pivotal role in assessing exposure to toxicologically relevant chemicals, with urinary metabolites serving as key indicators. Despite the widespread implementation of HBM programs globally, certain metabolites, such as mercapturic acids (MAs) derived from volatile organic compounds (VOCs), remain understudied in non-occupationally exposed populations.
Objective
To bridge this data gap, we analyzed 18 MAs in 360 24-h urine samples collected over a time span of 21 years from 2000 to 2021 in Germany.
Methods
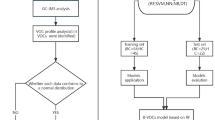
Two LC-MS/MS methods were utilized to quantify MAs in urine samples obtained from the Environmental Specimen Bank. Statistical analyses, including Kruskal-Wallis tests and Spearman correlations, were employed to evaluate temporal trends, sex-specific differences, and correlations between MAs.
Results
Quantification rates between 95 and 100% were obtained for 14 of the 18 MAs, with notable variations in concentrations among different metabolites. The most pronounced decrease in MA levels was observed from 2010/2015 to 2019 with a significant trend for 8 MAs, potentially reflecting changes in environmental exposures and regulations. Moreover, significant differences in urinary excretion per 24 h between males and females were observed for several MAs, highlighting the importance of considering sex in exposure assessments.
Impact Statement
Comprehensive human biomonitoring (HBM) data with regard to the exposure to volatile organic compounds (VOCs) in Europe is lacking. This prompted us to quantify 18 mercapturic acids as urinary VOC metabolites in 360 samples from the Environmental Specimen Bank collected between 2000 and 2021 in Germany. Our study demonstrates the ubiquitous exposure to numerous VOCs of high toxicological relevance, albeit with a decreasing trend over time for most of the metabolites. This emphasizes the need for a broader HBM to better understand the risk of VOC exposure in Germany and more general in Europe.
Similar content being viewed by others


Introduction
Human biomonitoring (HBM) deals with the assessment of internal exposure to toxicologically relevant chemicals by measuring them and/ or their specific metabolites in biospecimens such as blood or urine. The growing importance of HBM in the chemical risk assessment is underscored by its integration into the Green Deal as part of the European chemicals strategy towards a toxic free environment. HBM programs have been launched in several countries for decades inter alia as part of extensive health surveys in population-representative samples, including the National Health and Nutrition Examination Survey in the US (NHANES) [1] as the most comprehensive program worldwide, the German Environmental Survey (GerES) [2], Korea National Health and Nutrition Examination Survey (KNHANES) [3] or the Canadian Health Measures Survey (CHMS) [4]. As a major part of these surveys, several environmental chemicals and their metabolites have been periodically monitored to observe changes in the exposure over time, and to identify causal relationships with the individual behavior, environmental factors, and regional differences. Besides Germany several European countries have established national surveys such as FLEHS in Belgium [5], the Czech Republic’s HBM program (CZ-HBM) [6] and the French national HBM program [7] and biobanks for the analyses of time trends like the German Environmental Specimen Bank [8]. While these HBM programs have a similar scope, there are variations in recruitment, sample collection, analytical measurement, and data evaluation strategies. Recognizing the need for harmonization at the European level and addressing data gaps for previously overlooked toxicologically relevant chemicals, a joint European program co-funded by the European Commission—The European Human Biomonitoring Initiative (HBM4EU)—was launched in 2017. The initiative ran for five and a half years focusing on harmonizing HBM practices [9, 10], collecting new Europewide HBM data, and bridging data gaps for specific toxicants [11, 12].
This paper addresses the limited assessment of mercapturic acids (MAs), which represent the urinary elimination products of volatile organic compounds (VOCs). VOCs (e.g., benzene, toluene, acrylonitrile, acrolein, 1,3-butadiene) are electrophiles themselves or form electrophilic intermediates during metabolism. As a result, they can readily react with nucleophilic sites of physiological macromolecules such as DNA, RNA or proteins, which explains their toxic potential. The main detoxification process encompasses the addition of the electrophiles to glutathione and subsequent excretion as mercapturic acids [13], which can be determined in urine as biomarkers of VOC exposure. While NHANES routinely quantifies 24 MAs covering a broad spectrum of VOCs [14], European, national HBM programs have infrequently examined MAs to date.
In Germany, the Environmental Specimen Bank (ESB) complements GerES by storing, among others, urine samples over liquid nitrogen to retrospectively assess chemical exposures over time [15]. The cryostorage coupled with detailed documentation of sex, age, and 24 h urine volume allows for a comprehensive elucidation of time series and sex-specific differences in exposure assessment [8]. In this study, 18 MAs derived from 14 VOCs were quantified in 360 24-h urine samples from the ESB over a 21-year period from 2000 to 2021. Structures of the MAs along with their corresponding precursor chemicals are summarized in Table 1. The aim was to fill existing data gaps on toxicant exposure in Europe, in accordance with the scope of HBM4EU.
Materials and methods
Analytical method
18 MAs were determined by means of two LC-MS/MS methods as previously described [16]. The abbreviations for the MAs follow the harmonized acronym system introduced by Tevis et al. [17] (Table 1). One method applies a column-switching online extraction for the analysis of ten MAs in a 500 µL aliquot of urine (2-hydroxyethyl mercapturic acid (2HEMA), methyl mercapturic acid (MMA), ethyl mercapturic acid (EMA), 2-cyanoethyl mercapturic acid (2CyEMA), 3-hydroxy-1-methylpropyl mercapturic acid (3HMPMA), 2-carboxy-1-methylethyl mercapturic acid (2CoMEMA), 1-phenylethyl-2-hydroxy mercapturic acid (2H1PhEMA), 2-phenylethyl-2-hydroxy mercapturic acid (2H2PhEMA), phenyl mercapturic acid (PhMA), benzyl mercapturic acid (BzMA)). A second aliquot of 100 µL urine was completely evaporated and reconstituted in 100 µL methanol before analysis. Eight MAs were quantified for aliquot 2 (2-hydroxypropyl mercapturic acid (2HPMA), 3-hydroxypropyl mercapturic acid (3HPMA), 2-carbamoylethyl mercapturic acid (2CaEMA), 2-carbamoyl-2-hydroxy-ethyl mercapturic acid (2CaHEMA), methylcarbamoyl mercapturic acid (MCaMA), 1-hydroxymethyl-2-propenyl mercapturic acid (1HMPeMA), 2-hydroxymethyl-3-buten-1-yl mercapturic acid (2HBeMA), 3,4-dihydroxybutyl mercapturic acid (34HBMA)).
Sample analysis was conducted in accordance with ICH guideline M10 on bioanalytical method validation and study sample analysis [18]. The analytical runs were accepted based on the criteria for calibration and quality control (QC) samples. QC samples were interspersed throughout the run in three different concentration levels (low, medium, high) with a tolerance range of 85–115% accuracy. LLOQ ranged from 0.02 µg/L (SPMA) to 25 µg/L (3-HPMA).
Study population
The biobanked aliquots of 24-h urine samples from the ESB collected in the years 2000, 2005, 2010, 2015, 2019, and 2021 were provided by the German Environment Agency (Umweltbundesamt, UBA). In total, 360 urine samples (60 per year with a 50/50 sex ratio) from non-occupationally exposed participants between 20 and 29 years of age from Münster (North Rhine-Westphalia, Germany) were analyzed in this study. The sampling location was chosen to facilitate the evaluation of time trends of exposure over more than 20 years and allowing for potential future mixture assessments based on measurements in the same samples. The study protocol of the ESB has been approved by the ethics committee of the Medical Association Westfalen-Lippe, the Medical Faculty of the University of Münster and (since 2012) by the ethical committee of the Medical Association of the Saarland. The study was conducted in compliance with both European and national legal and ethical requirements in accordance with the Declaration of Helsinki. All participants gave informed written consent to participate in the study. Information on total 24-h urine volume, urinary creatinine concentration, BMI, age and sex are summarized in Table 2. More information regarding sampling procedures and storage conditions of the ESB urine samples can be found elsewhere [19].
Statistical analysis
MA concentrations were normalized for 24-h urine volume and expressed as µg excreted in 24 h (µg/24 h). Values below LLOQ were set to LLOQ/2 for further analyses. Mean, geometric mean (GM), standard deviation (SD), median, and 95th percentile (P95) were calculated where appropriate. GM are discussed in the manuscript unless otherwise indicated. The data were tested for normal distribution by means of the D’Agostino-Pearson and Shapiro-Wilk tests showing that the MA concentrations were not normally distributed. Consequently, non-parametric Kruskal-Wallis ANOVA and post-hoc Dunn’s multiple comparisons test were performed to test for statistical significance (α = 0.05) regarding time-specific differences. Mann–Whitney U test was applied to verify sex-specific differences over all years and each specific year of collection (α = 0.05). To determine the effects of sex, smoking-status and BMI on MA levels, a multiple linear regression analysis was performed (p < 0.05; two-tailed). Due to the right-skewed distribution, the excreted amounts were log-transformed as outcome variables for each analyte. All statistical analyses were carried out using Prism 10.4.0 (GraphPad Software, LaJolla, CA, USA).
Results
No significant differences were observed in the study population for age, BMI, urinary creatinine, nor the 24-h urine volume (Table 2). The majority of the 24-h urine samples had quantifiable levels for most of the 18 MA analyzed: 2CoMEMA, 3HMPMA, 2HPMA, MCaMA, 34HBMA, 2CaHEMA (all 100%), PhMA, BzMA, 3HPMA (all 99%), 2CyEMA, 2HEMA, MMA (all 97%), 2CaEMA (95%). EMA, 2HBeMA, 2H1PhEMA, and 2H2PhEMA were found in 55%, 32%, 16%, and 5%, respectively, while 1HMPeMA was not detectable. With regard to the low detection rates, 2H1PhEMA, 2H2PhEMA, and 1HMPeMA were omitted from further analyses. The Spearman correlation matrix is illustrated in Figure S1 (Supplementary Information) for the 13 MAs with high detection rates (97-100%). A strong correlation between 2CaEMA and 2CaHEMA (r = 0.77) as well as between 2CoMEMA and 2HPMA (r = 0.67) was observed. Overall, MMA (0.07–0.59) and MCaMA (0.06–0.29) tended to show poor correlations (average r = 0.25 and 0.17) while the highest correlations were found for 2CyEMA, 2CaEMA, 2CaHEMA, and 2HPMA (average r = 0.42–0.44). Correlations for the 77 smokers (S), as well as for the 283 non-smokers (NS, based on self-report, and verified by urinary cotinine with a cut-off of 50 µg/L [20]), were very similar to the complete set of samples (cf. Supplementary Information Figure S2, S3). 2CyEMA, EMA, PhMA, 2CaEMA, and 2CaHEMA were significantly elevated in smokers (see Fig. 1, and Table 3) with 2CyEMA showing the most pronounced elevation of 2.4-fold, followed by EMA, SMPA and 2CaEMA/2CaHEMA with 1.7-, 1.4-, and 1.2-fold [16, 21]. We tested the time trends for 2CyEMA for all 360 urine samples (NS + S) as well as for the 283 NS and the 77 S separately (data not shown). Since no alterations in time trends and correlations were observed for 2CyEMA which represents the most significant difference between S and NS in these subpopulations compared to the complete study population, the data evaluation was performed for the whole sample set, independent of the smoking status.

Box plots for males in grey (N = 180), females in white (N = 180), smokers (S) in blue (N = 77) and non-smokers (NS) in red (N = 283) of 2CyEMA (A), EMA (B), PhMA (C), 2CaEMA (D), and 2CaHEMA (E). Boxes: 75th/25th percentile; whiskers: 90th/10th percentile; horizontal line: median. Significant differences between males / females and between S / NS, respectively, are illustrated by the asterisks (non-parametric Mann–Whitney U test). *: p < 0.05; **: p < 0.01; ***: p < 0.001.
GMs ranged between 1021 µg/24 h (567 µg/L) for 2CoMEMA and 0.0609 µg/24 h (0.0338 µg/L) for EMA in the following order (see Table 3): 2CoMEMA > 34HBMA > 3HPMA > 3HMPMA > MCaMA > 2CaEMA > 2HPMA > MMA > BzMA > 2CaHEMA > 2CyEMA > 2HEMA > PhMA > 2HBeMA > EMA.
Urinary excretions (µg/24 h) were investigated across all years and for each sampling year and sex to determine time trends and sex-specific differences. Urinary concentrations (µg/L) and creatinine-normalized values (µg/g creatinine) are summarized in Table S1 and S2, respectively (Supplementary Information). BzMA was the only analyte with high detection rates (99%) with neither time nor sex-specific alterations. 2HBeMA also showed no differences in the statistical analysis, but with a much lower detection rate of 32%.
11 MAs showed a significant difference between males and females (Table 3). Males had higher levels in 10 of these 11 MAs (2CyEMA (Fig. 1A), 2CoMEMA, 3HMPMA, EMA (Fig. 1B), PhMA (Fig. 1C), 2CaEMA (Fig. 1D), 2CaHEMA (Fig. 1E), 34HPMA, 2HPMA, and 3HPMA), while MMA was the only analyte with a significantly higher excretion in females. This difference was significant across all years and for most of the individual collection years, except for MMA, where the sex-specific difference was only significant when comparing the complete study population (2000–2021, N = 360). The highest sex-specific differences occurred for 2CyEMA (1.7-fold) and 2CaEMA (1.6-fold), while the other MAs were in the range of 1.3 to 1.4-fold higher in males compared to females. A separate evaluation of S and NS revealed the same differences (data not shown).
In addition, we performed multiple linear regression including sex, smoking-status, and BMI to account for the contribution of these covariables. Sex and smoking contribute to statistically significant differences for the same MAs as found in the univariate analysis (Table S3), except for EMA which did not show a sex-specific difference in the multiple linear regression. The most profound increase in men was identified for 3HPMA with an elevation by 40% compared to women, while smoking status and BMI did not affect 3HPMA levels. Moreover, the BMI significantly impacts the MA levels for 14 MAs (2CyEMA, 2CoMEMA, EMA, 2HEMA, 3HMPMA, MMA, BzMA, PhMA, 2CaEMA, 2CaHEMA, MCaMA, 34HBMA, 2HPMA, and 2HBeMA) while no significant difference was obtained for 3HPMA. The overall variance which can be explained by these covariables differs substantially by MA as expressed by R2 in Table S3 (variance in MA level attributable to MA concentrations = R2 x 100 in percent). The investigated covariables contributed to a larger extent to the overall amount of 2CyEMA, 2CoMEMA, 2CaEMA, 2CaHEMA, 34HBMA, and 3HPMA in the range of 24% (2CyEMA) to 15%. The percentage change in MA levels for one covariable can be calculated from the respective regression coefficient (β) [22]. With each unit change in the covariable, the outcome (MA excretion) changes by 100*[exp (β)-1] (%). The smoking status is the most relevant predictor in terms of 2CyEMA, EMA and PhMA with 27 to 56% change. For the other MAs, sex is primarily driving the differences in MA excretion, whereas BMI, while showing a significant correlation, only provides a minor contribution to the changes in MA levels in the range of 2–9% change with increasing BMI.
A significant decrease over time (Kruskal Wallis ANOVA, p < 0.05) was observed for 8 MAs (2CyEMA, EMA, 2HEMA, PhMA, 2CaEMA, 2CaHEMA, MCaMA, 34HBMA) with 18 to 50% reductions from 2000 to 2021 (Fig. 2). Differentiated by sex, the same time trend was obtained for 2CyEMA, PhMA, 2CaEMA, 2CaHEMA for both sexes and additionally for MCaMA and 34HBMA for the male population. The time trend for EMA and 2HEMA was only significant for the complete population under scrutiny. Dunn’s test for multiple comparisons revealed that the decrease was in general most pronounced in 2015 compared to previous collection years, while the downward trend leveled off in the following years 2019 / 2021. For instance, 2CyEMA, showing the strongest overall reduction of 50%, had a steep decline between 2010 and 2015, with no further decrease in 2019. As an exception, MCaMA showed a significant decrease only in 2021 compared to the first collection year in 2000. A few MAs appear to have a higher excretion rate in 2010 for the male samples (2CaEMA, 2CaHEMA, MCaMA, 34HBMA, 3HPMA), which did not reach statistical significance.

Urinary excretions (µg/24 h) depicted as GM ± 95% CI of 2CyEMA (A), EMA (B), 2HEMA (C), PhMA (D), 2CaEMA (E), 2CaHEMA (F), MCaMA (G), 34HBMA (H) in males (N = 30 per year of collection) and females (N = 30 per year of collection). All MAs illustrated here showed statistically significant decrease (Kruskal-Wallis ANOVA; p < 0.05).
Discussion
General considerations and detection rates
The MA pathway is an important detoxification mechanism in the body that results in the excretion of the corresponding VOC metabolites in urine [13]. In general, the correlation between the different MAs was moderate to weak with high significance (p < 0.001). This suggests different exposure sources such as diet, tobacco smoke, or ambient air. Comprehensive biomonitoring data related to VOC exposure in larger European cohorts are scarce. PhMA and 2CaEMA/2CaHEMA are the only MAs for which HBM data in a population-representative sample in Germany have been assessed so far in children within GerES V [23]. PhMA averaged 0.097 µg/L (GM) with 95th percentile (P95) of 0.41 µg/L which is slightly below the mean PhMA concentration in our study of 0.124 µg/L with a comparable P95 of 0.42 µg/L, despite the far lower proportion of smokers in GerES V (2%) compared to the current HBM assessment in ESB samples (21%). This indicates the importance of other sources than smoking, like oil heating and air traffic pollution which were positively correlated with PhMA [23]. An HBM study conducted in Italy in 2013–2014 (adults aged 35–69; N = 1076) reported similar PhMA concentrations of 0.139 µg/g creatinine (GM of 0.167 µg/g creatinine in our study) [24]. Acrylamide exposure was around 2.5-times higher in GerES V with 72.6 µg/L 2CaEMA and 15.0 µg/L 2CaHEMA. Consumption of fried food was identified as the major contributor to elevated 2CaEMA concentrations besides smoking. In contrast, comparable levels were found in 20-40 year old adults in Poland (median 2CaEMA: 20.9 µg/L vs 28.5 µg/L; median 2CaHEMA: 8.6 µg/L vs 5.95 µg/L) at a similar proportion of smokers of 16% compared to our study [25].
Given the data gap in Germany and Europe in general related to VOC exposure in adults, the following discussion will refer to data from the NHANES study of the adult (20+ years) U.S. population covering the years 2005 to 2018 [14].
In total, 14 out of 18 MAs were found at very high detection rates of 95% and more, proving their applicability in the HBM of VOCs and providing the first baseline concentration levels for a large number of MAs in non-occupationally exposed young adults in Germany. For BzMA, 3HPMA and 34HBMA, the median concentrations are comparable with NHANES data for the respective time span (Table 4). In contrast, 2CyEMA, 3HMPMA, 2CaEMA, MCaMA, and 2HPMA, appear to be less concentrated in the ESB samples. We confirmed this observation using creatinine-normalized values (data not shown) to rule out dilution effects as a cause for these differences. However, the comparability may be limited owing the difference in the study populations, where NHANES is population-representative in contrast to the 24-h urine samples from 20- to 29-year-old students in the ESB. Some MAs (2HEMA, PhMA, 2CaHEMA) were not detectable in NHANES, which reported LODs above the median concentrations found in the ESB samples. Obviously, a higher sensitivity is required for an HBM in the general population, which may be compromised in the analysis applied by the CDC in favor of a broader range of analytes. For comparison, our analysis comprises 18 MAs measured by two separate methods, while the HBM program for VOCs in NHANES determines 28 urinary VOC metabolites in one run [21].
Focusing on behavioral aspects, smokers had higher levels of 5 MAs compared to non-smokers deriving from acrylonitrile (2CyEMA), ethylating agents (EMA), benzene (PhMA), and acrylamide (2CaEMA/2CaHEMA). These differences have been reported previously by several groups [16, 21, 26,27,28]. In addition, the US Population Assessment of Tobacco and Health (PATH), the most comprehensive population-based longitudinal study of tobacco use worldwide, confirmed our findings for the respective MAs [21, 29]. Yet, several MAs such as 2-HPMA, 3-HPMA, or MCaMA did not show a significant difference in our study, which is in contrast to the findings of the PATH and other studies [21, 29, 30]. The low number of 77 smokers and the concise classification by self-report (yes/no) and cotinine levels without detailed stratification by cigarettes per day or smoking history for the ESB samples may result in the misclassification. This applies in particular to vapers or users of other nicotine products, who have high cotinine levels but no pronounced exposure to the precursors of the respective tobacco smoke constituents propylene oxide, acrolein, or dimethylformamide. In this context it has to be noted that the discrimination between S and NS was not the primary scope in this study.
2H1PhEMA and 2H2PhEMA, both biomarkers of styrene exposure, were rarely detected, which is consistent with NHANES study data in the U.S. population [14]. This indicates the need for alternative biomarkers to monitor styrene exposure. While both MAs are specific to styrene, they lack in sensitivity due to the low excretion rate of only 1% of the styrene dose [31]. Mandelic acid (hydroxy(phenyl)acetic acid) remains the primary choice as a more sensitive biomarker for styrene exposure, although it is less specific [32].
1,3-BD forms at least four MAs [33], with 2HBeMA and 34HBMA being most frequently applied in biomonitoring studies [34]. In contrast, 1HMPeMA is a minor metabolite not detectable in the general population as shown in the present study and in NHANES [14]. Only one study has measured 1,3-BD exposure on a population-representative scale in 5897 subjects for NHANES cycles between 2011 and 2016 and reported 34HBMA (25th to 75th percentile (P25-P75): 211–465 µg/g creatinine) in more than 96% and 2HBeMA in 9.8% of the samples, respectively [35]. Our study had somewhat higher detection rates for 34HBMA (100%) and 2HBeMA (32%) with a comparable concentration range of 380-564 µg/g creatinine for 34HBMA (P25-P75).
Sex-specific differences in MA excretion
The main aim of the study was to decipher potential differences between sexes and the overall exposure over time. Males had higher urinary excretions for 10 of the 18 MAs which are related to the exposure to acrylonitrile (2CyEMA), crotonaldehyde (2CoMEMA/3HMPMA), ethylating agents (EMA), benzene (PhMA), acrylamide (2CaEMA/2CaHEMA), 1,3-BD (34HBMA), propylene oxide (2HPMA), and acrolein (3HPMA). Interestingly, MMA was the only analyte with significantly higher levels in females while EMA follows the trend found for the 9 MAs listed above. The assessment of MMA and EMA has not been reported in large scale studies so far. MMA and EMA are indicative of the exposure to toxic methylating and ethylating agents such as N-nitrosodimethylamine, N-nitrosodiethylamine, methyl chloride or ethyl chloride [36].
The comparison of urinary VOC metabolites between males and females has been previously reported in only two larger studies, both evaluating the data from the US NHANES 2011/2012 cycle, albeit in different subpopulations [37, 38]. Jain (2015) compared the adjusted GMs separated by sex and smoking status [37] while Mendy et al. (2022) used the creatinine-normalized values in a subset for which spirometry data were available [38]. Mendy et al. (2022) reported elevated levels of 3HMPMA and 2HPMA in females, which contradicts to our findings. In contrast, Jain (2015) found higher 3HPMA concentrations in female non-smokers in agreement with our results. However, the evaluation by Jain did not observe any sex-specific differences in non-smokers for 1,3-BD and crotonaldehyde. Hartmann et al. (2008) identified differences in 2CaEMA and 2CaHEMA with 1.5-fold higher urinary concentrations in men, similar to our study (1.6-fold elevation in men), while this sex difference disappeared for the creatinine-based concentrations [39]. It is important to note that women generally have lower creatinine concentrations due to differences in physiology and metabolism [40]. This would suggest that the concentration in females may be higher after normalization, even if there is no actual difference in exposure or a similar exposure, although men could be more exposed. In our study, concentrations were adjusted for the 24-h urine volume, which should not be influenced by additional factors like body weight, age, or muscle mass [41]. It is noteworthy that sex-specific differences were observed in both the complete study population as well as for the smokers and non-smokers individually. Variations in VOC exposures have been discussed in relation to the physiological differences between sexes in terms of absorption, deposition, and metabolism (ADME) of environmental chemicals [42]. For instance, sex hormones can influence GI tract motility, potentially leading to the accumulation of the ingested chemicals before excretion, which is especially pertinent for VOCs absorbed through dietary intake [43]. Regarding inhalation, which is the primary route of exposure for most VOCs, differences in ventilation capacity, tidal volumes, and lung size may result in varying uptakes between sexes [42]. However, it is likely that other exogenous sources, in addition to active smoking of combustible cigarettes and/or differences in the ADME of VOCs, likely contribute to the observed differences. For instance, diet significantly contributes to acrylamide exposure as reflected by higher CaEMA/CaHEMA levels after consumption of fried potatoes [44]. Moreover, various fruits contain crotonaldehyde and their consumption was linked to elevated 3HMPMA levels [45]. For most VOCs, their primary source can be attributed to the ubiquitous presence in ambient air, stemming from industrial and traffic emissions. Disparities in exposure may be linked to differences in occupational settings or residence. However, most studies have not found a causal relationship between sex and exposure levels [23, 44]. The observed sex- and smoking-specific differences illustrate the potential of HBM data to improve our understanding of the main sources of exposure to this highly toxic class of chemicals.
Influence of different covariables on MA levels
Our multiple linear regression model included three covariables: sex, smoking status and BMI. As discussed in the previous section 4.2, sex-specific differences may be attributed to differences in the ADME of VOCs as well as lifestyle and use behavior. However, the manifold environmental sources of exposure are too heterogenous to provide a simple answer for the observed variance. One significant contributor is the BMI, which correlates with dietary habits [46]. Our study suggests that BMI is positively correlated with the excreted amounts of MA coming from acrylonitrile, crotonaldehyde, ethylene oxide, toluene, benzene, acrylamide, dimethylformamide, 1,3-butadiene, propylene oxide, and alkylating agents, in agreement with previous reports [47, 48]. A more detailed investigation regarding dietary effects in a European cohort, similar to Lei et al [47], requires a comprehensive questionnaire, as available for instance in the GerES. In general, smoking contributes to a much higher extent to the exposure to several VOCs like acrylonitrile, benzene or acrylamide with an increase in MA levels of 56%, 27%, and 17% for 2CyEMA, PhMA, and 2CaEMA, respectively.
Time trends in VOC exposure from 2000 to 2021
In the present study, a notable reduction in MA concentrations was observed from 2000 to 2021, with significant decreases for 2CyEMA (50%), EMA (50%), 2HEMA (31%), PhMA (41%), 2CaEMA (24%), 2CaHEMA (29%), MCaMA (39%), and 34HBMA (18%), irrespective of sex and smoking status. We want to draw attention to the fact that while several classes of environmental chemicals, such as metals, PFAS, phthalates and PAHs have been extensively studied in terms of changes in exposure over time [15, 49,50,51,52], the assessment of MA VOC metabolites in HBM studies in this context is still limited. Poteser et al. performed a comprehensive analysis of acrylamide HBM data across ten European countries revealing an overall increase from 2001 to 2017 followed by a decline starting in 2018 in adults [53]. Notably, benchmark levels in food were adopted in 2017 which came into effect early 2018 in Europe may have influenced this trend [53]. In contrast, our data for 2CaEMA/2CaHEMA show a different time trend with the lowest value and most significant drop in 2015 and no significant increase in the years before.
In the population-representative Canadian study (CHMS) within 6 years from 2009-2015 [54], a significant decline in PhMA (18%) was observed, similar to our findings. Moreover, a substantial decline in acrylonitrile (2CyEMA) and N,N-dimethylformamide (MCaMA) exposure was observed in an extensive evaluation of NHANES data from 2012 onwards (Table 4), which falls within the time frame of the most pronounced decline in our study [55]. With regard to the major sources and given the fact that the decrease is independent of the smoking status, a reduction in secondhand smoke exposure seems a probable cause for the observed trends. Secondhand smoke exposure has steadily decreased in Germany since 2002 as a result of smoking bans and regulations limiting secondhand smoke exposure [20]. Moreover, the exposure to polycyclic aromatic hydrocarbons showed a similar time trend, which was attributed to reduced secondhand smoke exposure and legislation that has been implemented in the EU over the past 20 years to minimize chemical emissions into the air and improve air quality [20]. Hence, besides secondhand smoke exposure, environmental air and diet may contribute to the reduced exposure to these VOCs. Yet, closing data gaps and establishing a causal relationship requires comprehensive and regular monitoring of VOCs. This emphasizes the importance of national representative surveys such as GerES to facilitate the correlation of MA levels with the participants’ habits, diet, and socioeconomic status.
Exposure assessment
Since many of the analyzed VOC metabolites have parent compounds which are carcinogens, mutagens or toxic for reproduction (see Table 1) deriving a safe level of exposure is difficult and only few health-based guidance values are available.
All urine samples in this study showed MCaMA concentrations below the HBM guidance value (HBM-GV) of 1000 µg/g creatinine [56], indicating a low health-risk from N,N-dimethylformamide exposure. For non-cancer toxicity, Hays and Aylward derived a Biomonitoring Equivalent (BE) value consistent with a health protective guidance value for the general population for 2CaEMA of 13 μg/L urine [57]. For cancer risk, they calculated a BE value for urinary 2CaEMA concentrations of 1 μg/L (for a risk of 1 × 10–4) and of 0.01 μg/L (for a risk of 1 × 10–6). Most urinary 2CaEMA concentrations found in this study (with an LLOQ of 10 µg/L for 2CaEMA; 95% > LLOQ) were higher than the BE values. Therefore, individual avoidance as well as further regulation are necessary to reduce hazardous exposure, which holds true for all VOCs.
Conclusion
This is the first comprehensive HBM of a large number of VOCs in a non-occupationally exposed population based on the respective MA metabolites in a European country. The analysis of 360 24-h urine samples from the ESB spanning 21 years showed widespread detection of 14 MAs, indicative of their applicability in HBM. The multivariate analysis identified BMI and smoking-status as confounders for several MA metabolites. Moreover, significant differences between males and females underscore the importance of considering sex-specific exposure patterns. The high detection rates, sex-specific differences and time trends emphasize the need for a closely meshed HBM, preferably in the German Environmental Survey, in order to fill existing data gaps, establish reference values, and further elucidate the sources and health implications of VOC exposure. HBM derived reference values will improve our understanding of the health consequences from the exposure of the general population to VOCs, as exemplified for the guidance-value based exposure assessment of DMF and acrylamide.
Data availability
Additional data are available from the corresponding author on reasonable request.
References
Calafat AM. The U.S. National Health and Nutrition Examination Survey and human exposure to environmental chemicals. Int J Hyg Environ Health. 2012;215:99–101.
Umweltbundesamt (UBA). German Environmental Survey, GerES. https://www.umweltbundesamtde/en/topics/health/assessing-environmentally-related-health-risks/german-environmental-survey-geres last accessed 2024-01-17.
Park C, Yu SD. Status and prospects of the Korean National Environmental Health Survey (KoNEHS). J Environ Health Sci. 2014;40:1–9.
Statistics Canada. Canadian Health Measures Survey (CHMS). https://www.statcangcca/en/survey/household/5071 last accessed 2023-06-28.
Reynders H, Colles A, Morrens B, Mampaey M, Coertjens D, Koppen G, et al. The added value of a surveillance human biomonitoring program: The case of FLEHS in Flanders (Belgium). Int J Hyg Environ Health. 2017;220:46–54.
Czech National Institute of Public Health. Environmental Health Monitoring System. https://www.szu.gov.cz/wp-content/uploads/2024/01/Summary_report_2022.pdf last accessed 2024-01-17.
Sante publique France. Pollution et santé. https://www.santepubliquefrancefr/determinants-de-sante/pollution-et-sante last accessed 2024-01-16.
Kolossa-Gehring M, Becker K, Conrad A, Schroter-Kermani C, Schulz C, Seiwert M. Environmental surveys, specimen bank and health related environmental monitoring in Germany. Int J Hyg Environ Health. 2012;215:120–6.
Esteban López M, Göen T, Mol H, Nübler S, Haji-Abbas-Zarrabi K, Koch HM, et al. The European human biomonitoring platform - Design and implementation of a laboratory quality assurance/quality control (QA/QC) programme for selected priority chemicals. Int J Hyg Environ Health. 2021;234:113740.
Pack LK, Gilles L, Cops J, Tolonen H, van Kamp I, Esteban-Lopez M, et al. A step towards harmonising human biomonitoring study setup on European level: Materials provided and lessons learnt in HBM4EU. Int J Hyg Environ Health. 2023;249:114118.
Ganzleben C, Antignac JP, Barouki R, Castano A, Fiddicke U, Klanova J, et al. Human biomonitoring as a tool to support chemicals regulation in the European Union. Int J Hyg Environ Health. 2017;220:94–97.
Govarts E, Gilles L, Rodriguez Martin L, Santonen T, Apel P, Alvito P, et al. Harmonized human biomonitoring in European children, teenagers and adults: EU-wide exposure data of 11 chemical substance groups from the HBM4EU Aligned Studies (2014-2021). Int J Hyg Environ Health. 2023;249:114119.
Hanna PE, Anders MW. The mercapturic acid pathway. Crit Rev Toxicol. 2019;49:819–929.
Center for Disease Control and Prevention (CDC). Biomonitoring Data Tables for Environmental Chemicals. https://www.cdcgov/exposurereport/data_tableshtml last accessed 2024-01-17.
Goen T, Lermen D, Hildebrand J, Bartel-Steinbach M, Weber T, Kolossa-Gehring M. Discovering time-trends of the German populations exposure to contaminants by analysis of human samples of the German Environmental Specimen Bank (ESB). Toxicol Lett. 2018;298:194–200.
Pluym N, Gilch G, Scherer G, Scherer M. Analysis of 18 urinary mercapturic acids by two high-throughput multiplex-LC-MS/MS methods. Anal Bioanal Chem. 2015;407:5463–76.
Tevis DS, Flores SR, Kenwood BM, Bhandari D, Jacob P 3rd, et al. Harmonization of acronyms for volatile organic compound metabolites using a standardized naming system. Int J Hyg Environ Health. 2021;235:113749.
International Council for Harmonisation of Technical Requirements for Pharmaceuticals for Human Use (ICH). Bioanalytical Method Validation and Study Sample Analysis M10. (2022).
Lermen D, Bartel-Steinbach M, Jost N German environmental Specimen Bank (ESB) - guideline for sampling and sample processing 24h-sampling urine. In, (2015).
Burkhardt T, Scherer M, Scherer G, Pluym N, Weber T, Kolossa-Gehring M. Time trend of exposure to secondhand tobacco smoke and polycyclic aromatic hydrocarbons between 1995 and 2019 in Germany–Showcases for successful European legislation. Environ Res. 2022;114638:1–11.
Alwis KU, Blount BC, Britt AS, Patel D, Ashley DL. Simultaneous analysis of 28 urinary VOC metabolites using ultra high performance liquid chromatography coupled with electrospray ionization tandem mass spectrometry (UPLC-ESI/MSMS). Anal Chim Acta. 2012;750:152–60.
Wooldridge JM. Introductory Econometrics: A Modern Approach. South-Western Cengage Learning, (2013).
Schwedler G, Murawski A, Schmied-Tobies MIH, Rucic E, Scherer M, Pluym N, et al. Benzene metabolite SPMA and acrylamide metabolites AAMA and GAMA in urine of children and adolescents in Germany – human biomonitoring results of the German Environmental Survey 2014–2017 (GerES V). Environ Res. 2021;192:110295.
Tranfo G, Pigini D, Paci E, Bauleo L, Forastiere F, Ancona C. Biomonitoring of urinary benzene metabolite SPMA in the general population in central Italy. Toxics. 2018;6:37.
Mojska H, Gielecinska I, Cendrowski A. Acrylamide content in cigarette mainstream smoke and estimation of exposure to acrylamide from tobacco smoke in Poland. Ann Agric Environ Med : AAEM. 2016;23:456–61.
De Jesus VR, Zhang L, Bhandari D, Zhu W, Chang JT, Blount BC. Characterization of acrylonitrile exposure in the United States based on urinary n-acetyl-S-(2-cyanoethyl)-L-cysteine (2CYEMA): NHANES 2011-2016. J Expo Sci Environ Epidemiol. 2021;31:377–85.
Frigerio G, Mercadante R, Campo L, Polledri E, Boniardi L, Olgiati L, et al. Urinary biomonitoring of subjects with different smoking habits. Part I: Profiling mercapturic acids. Toxicol Lett. 2020;327:48–57.
Scherer G, Pluym N, Scherer M. Comparison of urinary mercapturic acid excretions in users of various tobacco/nicotine products. Drug Test Anal. 2023;15:1107–26.
Anic GM, Rostron BL, Hammad HT, van Bemmel DM, Del Valle-Pinero AY, Christensen CH et al. Changes in biomarkers of tobacco exposure among cigarette smokers transitioning to ENDS use: the population assessment of tobacco and health study, 2013–2015. Int J Environ Res Public Health 2022;19:1–13.
Eckert E, Schmid K, Schaller B, Hiddemann-Koca K, Drexler H, Goen T. Mercapturic acids as metabolites of alkylating substances in urine samples of German inhabitants. Int J Hyg Environ Health. 2011;214:196–204.
Seutter-Berlage F, Delbressine LP, Smeets FL, Ketelaars HC. Identification of three sulphur-containing urinary metabolites of styrene in the rat. Xenobiotica. 1978;8:413–8.
Capella KM, Roland K, Geldner N, Rey deCastro B, De Jesus VR, van Bemmel D, et al. Ethylbenzene and styrene exposure in the United States based on urinary mandelic acid and phenylglyoxylic acid: NHANES 2005-2006 and 2011-2012. Environ Res. 2019;171:101–10.
Sterz K, Scherer G, Krumsiek J, Theis FJ, Ecker J. Identification and quantification of 1-hydroxybutene-2-yl mercapturic acid in human urine by UPLC- HILIC-MS/MS as a novel biomarker for 1,3-butadiene exposure. Chem Res Toxicol. 2012;25:1565–7.
Osterman-Golkar S, Bond JA. Biomonitoring of 1,3-butadiene and related compounds. Environ health Perspect. 1996;104:907–15.
Nieto A, Zhang L, Bhandari D, Zhu W, Blount BC, De Jesus VR. Exposure to 1,3-Butadiene in the U.S. Population: National Health and Nutrition Examination Survey 2011-2016. Biomarkers. 2021;26:371–83.
Eckert E, Goen T. Rapid determination of four short-chain alkyl mercapturic acids in human urine by column-switching liquid chromatography-tandem mass spectrometry. J Chromatogr B. 2014;965:54–60.
Jain RB. Distributions of selected urinary metabolites of volatile organic compounds by age, gender, race/ethnicity, and smoking status in a representative sample of U.S. adults. Environ Toxicol Pharm. 2015;40:471–9.
Mendy A, Burcham S, Merianos AL, Mersha TB, Mahabee-Gittens EM, Chen A, et al. Urinary volatile organic compound metabolites and reduced lung function in U.S. adults. Respir Med. 2022;205:107053.
Hartmann EC, Boettcher MI, Schettgen T, Fromme H, Drexler H, Angerer J. Hemoglobin adducts and mercapturic acid excretion of acrylamide and glycidamide in one study population. J Agric Food Chem. 2008;56:6061–8.
Barr DB, Wilder LC, Caudill SP, Gonzalez AJ, Needham LL, Pirkle JL Urinary creatinine concentrations in the US population: implications for urinary biologic monitoring measurements. Environ Health Perspectives 2005;113:192–200.
Lermen D, Bartel-Steinbach M, Gwinner F, Conrad A, Weber T, von Briesen H, et al. Trends in characteristics of 24-h urine samples and their relevance for human biomonitoring studies – 20 years of experience in the German Environmental Specimen Bank. Int J Hyg Environ Health. 2019;222:831–39.
Arbuckle TE. Are there sex and gender differences in acute exposure to chemicals in the same setting?. Environ Res. 2006;101:195–204.
Soldin OP, Mattison DR. Sex differences in pharmacokinetics and pharmacodynamics. Clin Pharmacokinet. 2009;48:143–57.
Fernandez SF, Poteser M, Govarts E, Pardo O, Coscolla C, Schettgen T, et al. Determinants of exposure to acrylamide in European children and adults based on urinary biomarkers: results from the “European Human Biomonitoring Initiative” HBM4EU participating studies. Sci Rep. 2023;13:21291.
Bagchi P, Geldner N, deCastro BR, De Jesus VR, Park SK, Blount BC. Crotonaldehyde exposure in U.S. tobacco smokers and nonsmokers: NHANES 2005-2006 and 2011-2012. Environ Res. 2018;163:1–9.
Kennedy ET, Bowman SA, Spence JT, Freedman M, King J. Popular diets: correlation to health, nutrition, and obesity. J Am Diet Assoc. 2001;101:411–20.
Lei T, Qian H, Yang J, Hu Y. The association analysis between exposure to volatile organic chemicals and obesity in the general USA population: A cross-sectional study from NHANES program. Chemosphere. 2023;315:137738.
Lee I, Park H, Kim MJ, Kim S, Choi S, Park J, et al. Exposure to polycyclic aromatic hydrocarbons and volatile organic compounds is associated with a risk of obesity and diabetes mellitus among Korean adults: Korean National Environmental Health Survey (KoNEHS) 2015-2017. Int J Hyg Environ Health. 2022;240:113886.
Choi W, Kim S, Baek YW, Choi K, Lee K, Kim S, et al. Exposure to environmental chemicals among Korean adults-updates from the second Korean National Environmental Health Survey (2012-2014). Int J Hyg Environ Health. 2017;220:29–35.
Lermen D, Weber T, Goen T, Bartel-Steinbach M, Gwinner F, Mueller SC, et al. Long-term time trend of lead exposure in young German adults - Evaluation of more than 35 Years of data of the German Environmental Specimen Bank. Int J Hyg Environ Health. 2021;231:113665.
Stajnko A, Lundh T, Assarson E, Akerberg Krook E, Broberg K. Lead, cadmium, and mercury blood levels in schoolchildren in southern Sweden: Time trends over the last decades. Chemosphere. 2024;346:140562.
Zhang X, Li Z. Developing a profile of urinary PAH metabolites among Chinese populations in the 2010s. Sci Total Environ. 2023;857:159449.
Poteser M, Laguzzi F, Schettgen T, Vogel N, Weber T, Zimmermann P, et al. Time Trends of Acrylamide Exposure in Europe: Combined Analysis of Published Reports and Current HBM4EU Studies. Toxics. 2022;10:481.
Pollock T, Karthikeyan S, Walker M, Werry K, St-Amand A. Trends in environmental chemical concentrations in the Canadian population: biomonitoring data from the Canadian Health Measures Survey 2007-2017. Environ Int. 2021;155:106678.
Stanfield Z, Setzer RW, Hull V, Sayre RR, Isaacs KK, Wambaugh JF. Characterizing chemical exposure trends from NHANES urinary biomonitoring data. Environ health Perspect. 2024;132:17009.
Apel P, Lamkarkach F, Lange R, Sissoko F, David M, Rousselle C, et al. Human biomonitoring guidance values (HBM-GVs) for priority substances under the HBM4EU initiative - New values derivation for deltamethrin and cyfluthrin and overall results. Int J Hyg Environ Health. 2023;248:114097.
Hays SM, Aylward LL. Biomonitoring equivalents (BE) dossier for acrylamide (AA) (CAS No. 79-06-1). Regulatory Toxicol Pharm. 2008;51:S57–67.
Acknowledgements
We thank the ESB teams of Fraunhofer IBMT and the University Hospital of Münster for their excellent work in sampling, handling and storing the human samples, and measuring of anthropometric data, urine volumes, and urinary creatinine concentrations for the German ESB.
Funding
This study was funded by the Federal Ministry for the Environment, Nature Conservation, Nuclear Safety and Consumer Protection (BMUV).
Author information
Authors and Affiliations
Contributions
NP: Data curation, Formal analysis, Project Administration, Supervision, Writing—original draft, Writing—review & editing; TB: Investigation, Formal analysis, Writing—review & editing; TW: Conceptualization, Data curation, Project administration, Writing—review & editing; GS: Writing—Reviewing & Editing; MS: Funding acquisition; Project Administration; Supervision; Writing—Reviewing & Editing; MK-G: Funding acquisition; Conceptualization; Writing—Reviewing & Editing.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethical approval
The study protocol for collection of the ESB samples has been approved by the ethics committee of the Medical Association Westfalen-Lippe, the Medical Faculty of the University of Münster and (since 2012) by the ethical committee of the Medical Association of the Saarland (Reg. No.: HA02/12). The study was conducted in compliance with both European and national legal and ethical requirements in accordance with the Declaration of Helsinki in its version of Fortaleza, 2013. All participants provided written, informed consent prior to participating.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Pluym, N., Burkhardt, T., Weber, T. et al. Analysis of 18 mercapturic acids in urine samples from the German Environmental Specimen Bank—tackling the data gap in the human biomonitoring of VOCs in Europe. J Expo Sci Environ Epidemiol (2026). https://doi.org/10.1038/s41370-026-00838-x
Received:
Revised:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41370-026-00838-x
