
Abstract
Background
Women conceiving via assisted reproductive technology (ART) may have a higher risk of developing gestational diabetes mellitus (GDM) compared to those who conceive spontaneously. However, the underlying factors associated with this relationship are not fully understood. This study aimed to investigate the association between ART conception and GDM prevalence and to explore related maternal serum biomarkers.
Methods
In an observational cohort of 11,563 singleton pregnancies, GDM was diagnosed at 24–28 weeks. We compared maternal characteristics, GDM prevalence, and late-pregnancy serum levels of folate, vitamin B12, and lipids between ART and spontaneously conceived women. Multivariable logistic regression assessed the independent association between ART and GDM.
Results
Among the participants, 2.3% conceived through ART. The overall GDM prevalence was 8.4%, but significantly higher in the ART group (15.0%). Within the ART group, GDM was more common among women with advanced age (23.2%), obesity (21.8%), or multiparity (25.0%). After adjustment for confounders, ART conception remained independently associated with an increased prevalence of GDM (adjusted OR: 1.49, 95% CI: 1.03–2.15). Furthermore, women in the ART group had significantly higher adjusted serum levels of folate (adjusted β = 3.58, 95% CI: 1.96–5.21) and triglycerides (adjusted β = 0.25, 95% CI: 0.13–0.37) compared to the spontaneous conception group. In the entire cohort, higher levels of both folate (adjusted OR = 2.21, 95% CI: 1.71–2.85) and triglycerides (adjusted OR = 1.70, 95% CI: 1.31–2.22) were independently associated with an increased GDM prevalence.
Conclusions
Our study confirms that ART pregnancies are associated with a higher risk of GDM and with elevated circulating folate and triglyceride concentrations at delivery. These findings highlight the importance of monitoring GDM risk and metabolic profiles in pregnancies achieved through ART. Future studies with biomarker assessments earlier in gestation are needed to clarify whether maternal folate and lipid metabolism contribute causally to the excess risk of GDM in ART pregnancies.
Similar content being viewed by others

Introduction
Hyperglycemia first identified during pregnancy is defined as gestational diabetes mellitus (GDM), an increasingly prevalent challenge in public health and clinical practice that complicates approximately 14% of global pregnancies [1]. GDM can not only lead to adverse pregnancy outcomes, such as caesarean section, preterm birth (PTB), macrosomia, and large-for-gestational-age (LGA) infants, but also increase the incidence of developing type 2 diabetes mellitus, metabolic disorders, and cardiovascular disease (CVD) post-pregnancy. Additionally, it can boost the likelihood of diseases in the offspring’s childhood and adulthood, such as metabolic dysfunction and obesity [2, 3]. Therefore, investigating the etiology and risk factors of GDM, and seeking effective preventive strategies, holds practical and enduring importance for improving maternal and fetal outcomes. Well-established risk factors for GDM include advanced maternal age, maternal obesity, high parity, diabetes family history, and a history of prior GDM. Growing epidemiological studies have observed that pregnant women conceived through assisted reproductive technologies (ART) have a higher prevalence of gestational diabetes mellitus (GDM) compared with those who conceived spontaneously [4].
Over the past two decades, the link between ART and GDM has attracted escalating attention in research. However, whether ART is an independent influencing factor for GDM in individuals with singleton pregnancies remains controversial. A number of studies with sufficient sample sizes have examined the association between ART and GDM risk in singleton pregnancies, yielding inconsistent results. Some studies have demonstrated a significantly increased risk of GDM among women with pregnancies achieved through ART compared to those with spontaneous conceptions [5,6,7,8,9,10,11,12,13,14,15,16,17,18,19,20], while others have failed to find any significant association [21,22,23,24,25,26,27,28]. One plausible explanation for these conflicting findings could be the influence of various maternal factors, including age, BMI, and parity, which may contribute to the occurrence of GDM [28]. Despite adjustments for these maternal factors in most studies, other potential determinants, such as maternal folate status and lipid profiles, have generally not been accounted for in the analyses. Given that cumulative evidence indicates elevated maternal levels of folate and triglycerides are associated with an increased occurrence of GDM [29,30,31,32], no previous studies to date have investigated the differences in these potential determinants between ART and natural conception groups.
Consequently, we utilized the perinatal real-world database of a tertiary (3 A) hospital, which enabled us to elucidate the relationship between ART and GDM prevalence in singleton pregnancies after controlling for these known maternal factors, and to systematically assess the potential role of maternal folate and triglyceride levels within this relationship.
Methods
Study design and data source
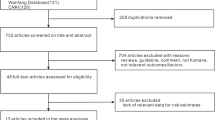
We conducted an observational cohort study using data from a real-world database provided by the Changzhou Maternal and Child Health Care Hospital. This database included 13,275 consecutive women who delivered at the hospital between April 2016 and March 2017 and incorporated their demographic and reproductive characteristics, laboratory measurements upon admission for delivery, and pregnancy outcomes. Participants were eligible for inclusion if they had a single pregnancy leading to a live birth between 28 and 41 weeks of gestation. Participants were disqualified from the final analysis if they fulfilled any of the following criteria: multiple pregnancies; a previous medical history including diabetes (either type 1 or 2), hypertension, cardiovascular, hepatic, and renal disorders, rheumatic autoimmune diseases, or syphilis; use of illegal drugs, alcohol, or tobacco during pregnancy; congenital defects or fetal death in utero; medically induced termination of pregnancy; or missing serum levels of folate, total homocysteine (tHcy), vitamin B12, blood lipids, and liver and kidney function tests. Following the exclusion of 1712 participants for various reasons including 335 cases of plural pregnancies, 488 with pre-existing medical disorders, 96 involving congenital anomalies or non-live births, and 793 lacking related laboratory measurements, a total of 11,563 individuals remained eligible for the final analysis (Fig. 1). Throughout their pregnancies, none of the study participants reported using illegal drugs, smoking, or consuming alcohol. We retrieved data from the clinical medical records, including maternal demographics, reproductive history, disease history, medication use history, admission and discharge diagnoses, mode of delivery, fetal gestational age, sex, birth length, and birth weight.

Participants flow chart.
Ethical approval for this study was granted by the hospital’s institutional review board (IRB; reference number ZD201803). Given that the data were retrospectively collected in an anonymous manner from the hospital’s database, the requirement for informed consent was waived. Due to the retrospective, observational nature of this study using an existing database, the investigators were not involved in patient care or group allocation. However, the primary exposure (ART conception) and outcome (GDM) were defined by objective data extracted from medical records. The laboratory measurements were performed automatically, and the GDM diagnosis was based on standardized, objective OGTT criteria, which minimized the potential for assessment bias.
Biochemical analyses
In this study, all individuals were hospitalized for childbirth either upon reaching their estimated date of confinement or presenting with signs of impending labor. Blood samples were collected from participants upon admission and subsequently sent to the hospital’s laboratory for routine measurements on the respective automated platforms: for hepatorenal function and lipid profiles, the AU5800 (Beckman Coulter, Japan); for tHcy, the BN II System (Siemens Diagnostics, Germany); and for vitamin B12 and folate, the UniCel DxI 800 (Beckman Coulter, USA). The intra-assay and inter-assay coefficients of variation (CVs) for these laboratory measurements were < 5% and < 10%, respectively. We retrieved these laboratory results from the hospital’s information system.
Diagnosis of GDM
GDM was diagnosed following the guidelines suggested by the International Association of Diabetes and Pregnancy Study Groups. All participants were requested to undergo an oral glucose tolerance test (OGTT) administering 75 grams of glucose during the 24th to 28th weeks of gestation. During the OGTT, plasma glucose levels were assessed at 0 (fasting), 1, and 2 h post-glucose intake. Normal glucose values were set as follows: a fasting glucose level below 5.1 mmol/L, a 1 h glucose level below 10.0 mmol/L, and a 2 h glucose level below 8.5 mmol/L. If any of these glucose readings met or exceeded their respective thresholds, the participant would be diagnosed with GDM [33].
Definitions
Maternal age was classified as either advanced (35 years or older) or non-advanced (under 35 years), and prenatal body mass index (BMI) was categorized as obesity (30.0 kg/m² or higher), overweight (25.0 to 29.9 kg/m²), or normal weight (below 25.0 kg/m²) [34]. Diagnosis of maternal comorbidities, including preeclampsia (PE), pregnancy induced hypertension (PIH), and intrahepatic cholestasis of pregnancy (ICP), followed the criteria established in a prior study [35]. Preterm birth (PTB) was defined as birth occurring between the 28th week and the end of the 36th week plus 6 days of gestation [36]. Newborns were classified as small for gestational age (SGA) if their birth weights were below the 10th percentile for their respective gestational age, as appropriate for gestational age (AGA) if their birth weights fell within the 10th to 90th percentiles, and as large for gestational age (LGA) if their birth weights exceeded the 90th percentile [37].
Statistical analysis
Statistical analyses were conducted using EmpowerStats version 4.1 (X&Y Solutions, Boston, MA) and R version 4.2.0 (R Foundation, Vienna, Austria). Data were summarized as frequency (percentage) for categorical variables and as mean ± standard deviation (SD) for continuous variables, stratified by conception method (natural versus ART). The distribution of continuous variables was assessed for normality using the Shapiro-Wilk test. Based on this assessment, variables following normal distributions were compared using one-way ANOVA, with the homogeneity of variances verified by Levene’s Test, while variables exhibiting skewed distributions were compared using the Mann-Whitney U test with visual assessment of distributional similarity. Categorical variables were compared using the chi-square test. Logistic regression models were employed to estimate the odds ratios (ORs) and corresponding 95% confidence intervals (CIs) for GDM in ART compared to natural conception. Model Ⅰ adjusted for maternal age, prenatal BMI, blood pressure (BP), parity, and fetal sex, while Model Ⅱ further incorporated additional laboratory findings alongside these variables. For subgroup analysis, stratified logistic regression models were applied to assess the interactions between ART and GDM within different subgroups defined by maternal age ( < 35 years vs. ≥ 35 years), prenatal BMI ( < 30 kg/m² vs. ≥30 kg/m²), and parity (nulliparous vs. multiparous). Linear regression models were used to calculate the regression coefficients (βs) for folate and triglycerides levels between ART and naturally conceived groups. Logistic regression models were also applied to estimate the ORs and 95% CIs for GDM prevalence, comparing higher quintiles to the lowest quintile of folate and triglycerides levels, as well as assessing the impact of a one-SD increase in these levels in late pregnancy. P-values less than 0.05 were considered to indicate statistical significance, and all statistical tests conducted in this study were two-sided. The sample size was determined by the available data in the real-world database. A post-hoc power analysis confirmed that the study had > 99% power to detect the observed effect size for the primary association (ART and GDM) at a two-sided alpha of 0.05.
Results
Participants’ characteristics
Among the 11,563 eligible participants with singleton pregnancies, 266 (2.3%) received ART to assist conception, whereas 11,297 (97.7%) conceived naturally. The prenatal characteristics and laboratory measurements of all women are described in Table 1. In the ART group, compared with the spontaneous conception group, maternal age, BMI, nulliparity proportion, rates of cesarean section and LGA delivery, GDM prevalence, and levels of vitamin B12, folate, ALT, and triglycerides were significantly higher (all P < 0.05). In contrast, gestational age at delivery, the proportion of SGA births, and tHcy levels were significantly lower in the ART group (all P < 0.01). No significant differences were observed between the two groups in terms of BP, the prevalence of ICP, PE, PIH, and PTB, fetal sex, height, and weight, as well as levels of AST, urea nitrogen, creatinine, total cholesterol, LDL-C, and HDL-C.
Relationship between ART and GDM
GDM prevalence in associations with ART among the participants are shown in Table 2. In the crude model, an increased prevalence of GDM was observed in women who conceived through ART compared with those who conceived spontaneously (15.0% vs. 8.2%), with an OR of 1.98 (95% CI: 1.40–2.78). After sequentially controlling for potential confounders in Model 1 and Model 2, the ART–GDM relationship remained significant, with ORs of 1.72 (95% CI: 1.40–2.78) and 1.49 (95% CI: 1.03–2.15), respectively. Stratified analyses across subgroups of maternal age ( < 35 and ≥35 years), prenatal BMI ( < 30 and ≥30 kg/m²), and parity (no children and ≥ 1 child) revealed no significant interactions (all P-values for interaction > 0.05, Table 3). A higher prevalence of GDM was observed in people who underwent ART and those of advanced maternal age (35 years or older) (23.2%), people with obesity (21.8%), and people with multiparity (25.0%). In contrast, a lower prevalence of GDM was found in people who conceived naturally and were of non-advanced maternal age (under 35 years), without obesity, and nulliparous (each with 7.2%).
Relationships of ART with folate and triglycerides
Compared with women who conceived spontaneously, those who conceived through ART had significantly higher serum folate (33.6 ± 15.3 nmol/L vs. 26.6 ± 14.5 nmol/L) and triglycerides levels (4.5 ± 2.0 mmol/L vs. 3.9 ± 1.8 mmol/L), with all P-values < 0.001 (Fig. 2). In general regression analyses, the β coefficients for serum folate and triglycerides levels were 6.99 and 0.53 in the crude models, 5.55 and 0.44 in Model 1, and 3.58 and 0.25 in Model 2, respectively (Table 4).

Comparison of maternal serum folate and triglyceride levels in ART versus spontaneous conception groups (A folate: 33.6 ± 15.3 nmol/L vs. 26.6 ± 14.5 nmol/L, B triglycerides: 4.5 ± 2.0 mmol/L vs. 3.9 ± 1.8 mmol/L, all P < 0.001).
Relationships of GDM with folate and triglycerides
As shown in Table 5 and Table 6, an elevation in folate and triglycerides levels by one SD was significantly related to an increased risk of GDM, with ORs of 1.38 for folate and 1.29 for triglycerides in the crude model, 1.37 for folate and 1.26 for triglycerides in Model 1, and 1.26 for folate and 1.15 for triglycerides in Model 2. For folate, the multivariable-adjusted ORs of GDM for higher quintiles versus the lowest quintile were 1.30 (95% CI: 1.00–1.69), 1.68 (95% CI: 1.31–2.17), 1.69 (95% CI: 1.31–2.18), and 2.21 (95% CI: 1.71–2.85). For triglycerides, the corresponding ORs were 1.14 (95% CI: 0.88–1.46), 1.39 (95% CI: 1.08–1.77), 1.57 (95% CI: 1.23–2.00), and 1.70 (95% CI: 1.31–2.22). Additionally, increased levels of folate and triglycerides displayed a non-linear relationship with an elevated likelihood of GDM, as depicted in Fig. 3.

Smooth curve fitting analysis of GDM prevalence with folate and triglycerides levels (A folate-associated GDM, B triglycerides-associated GDM).
Discussion
This observational cohort study analyzed differences in pregnancy complications between women who conceived via ART and those who conceived naturally at a Grade A tertiary hospital in eastern China. We found that GDM was more prevalent among ART pregnant women, particularly those of advanced age, people with obesity, or those with multiparity. Our results confirmed a significant association between ART conception and GDM prevalence, even after adjusting for potential confounders, whereas no such association was observed for other complications such as ICP, PE, or PIH. Furthermore, ART conception was associated with elevated serum levels of folate and triglycerides, both of which were independently correlated with GDM prevalence. These findings identify folate and triglycerides as important biological correlates in the pathway linking ART to GDM, highlighting the need for further investigation into their potential role.
There has been a steady increase in the number of pregnancies conceived through ART over the past few decades, enabling countless couples with infertility to become parents and accounting for 1–6% of all live births globally [7]. Although the vast majority of children born through ART are healthy, there is growing concern about the incidence of adverse pregnancy outcomes. Epidemiological studies and meta-analyses have accumulated evidence suggesting that singleton pregnancies achieved through ART are associated with a higher risk of adverse pregnancy outcomes compared to those conceived naturally, which mainly included pregnancy complications (GDM/PE/PIH/ICP) and adverse birth outcomes (caesarean section/PTB/low birth weight/SGA/LGA) [38,39,40,41,42,43,44]. In the present real-world study, we observed a higher prevalence of GDM, cesarean sections, and LGA deliveries among ART singleton pregnancies compared to spontaneous singleton pregnancies. However, there was no significant difference in the prevalence of other pregnancy complications, including PE, PIH, ICP, and PTB, or in the fetal birth weight. Some of these research findings are consistent with previous epidemiological studies, while others are contradictory. For instance, an Israeli prospective study comparing 561 ART singleton pregnancies to 600 spontaneous ones found no significant differences in complications like GDM, PIH, and cesarean sections [22]. Conversely, a Chinese retrospective cohort study of 1453 ART and 6667 spontaneous singleton pregnancies showed that ART was linked to higher rates of GDM, ICP, PIH, and mild PE compared to spontaneous conception [15]. Another Chinese retrospective study, involving 5,960 ART and 8,005 spontaneous singleton pregnancies, indicated that ART was associated with higher rates of GDM and cesarean sections but not with PIH [18]. This discrepancy could be attributed to differences in study design (cohort vs. cross-sectional vs. case-control studies), study location (reflecting variations in GDM prevalence and race/ethnicity among populations), causes of infertility, and ART subtypes. Significant differences in GDM prevalence have been reported among different ART subtypes and causes of infertility [42]. This discrepancy might also be due to some studies failing to control for maternal characteristics, whereas the present study adjusted for factors such as age, BMI, and parity.
The mechanisms underlying the increased prevalence of GDM in individuals who achieve singleton pregnancies through ART compared to those who conceive spontaneously remain unclear. One potential explanation for this negative effect of ART-induced pregnancy may be the hormonal therapy employed in ovulation stimulation and luteal phase supplementation [19]. Previous study has suggested that luteal phase support with progesterone until 12 weeks, preterm labor prevention, and the specific mode of progesterone administration may contribute to an increased risk of GDM in women conceiving via ART [45]. Progesterone has been shown to increase insulin resistance by reducing glucose transporter 4 expression, which may contribute to the occurrence of GDM [46]. Due to the lack of relevant data, we were unable to investigate this association. A Chinese cohort study involving 4353 participants demonstrated that high-dose folate supplementation ( ≥ 800 μg/day) from pre-pregnancy to mid-pregnancy is associated with an elevated risk of GDM [47]. Another cohort study of 3252 Chinese women with singletons further observed a higher prevalence of GDM among those who conceived via ART and received high-dose folate supplementation ( > 800 μg/day) compared to those who conceived naturally and received low-dose folate supplementation ( < 400 μg/day) [20]. Our real-world study provided the first evidence that serum folate levels in the third trimester are significantly higher in women who conceived via ART compared to those who conceived naturally. Additionally, our study revealed that maternal serum folate levels in late pregnancy are positively correlated with the prevalence of GDM. This finding aligns with two previous cohort studies conducted in Singapore and China [29, 30], which also noted this correlation. Collectively, these findings suggest that the elevated folate levels commonly observed in ART pregnancies may be one of the factors associated with the increased GDM risk in this population. The mechanisms by which a high folate status can influence the occurrence of GDM include triggering inflammation, interfering with insulin signaling pathways, and indirectly affecting insulin sensitivity and β-cell function through its impact on vitamin B12 metabolism [48]. A similar pattern is observed for serum triglycerides. In spontaneous pregnancies, elevated triglyceride levels have been consistently correlated with an increased risk of GDM [32]. Among ART-conceived pregnancies, individuals who developed GDM have been shown to exhibit significantly higher pre-conception triglyceride levels than those who did not, with an elevated level ( ≥ 1.7 mmol/L) associated with a 1.9-fold increased likelihood of developing GDM [49, 50]. Our study reinforces these observations, confirming a significant association between elevated triglyceride levels in late pregnancy and GDM prevalence. Therefore, both elevated folate and triglycerides represent important biological correlates that may partly explain the link between ART conception and GDM, warranting further investigation into their precise roles.
This study features several notable advantages that are well worth highlighting. Firstly, this study comprehensively analyzed the serum profiles of folate, vitamin B12, tHcy, hepatic and renal function, and lipids in ART women during late pregnancy and, for the first time, examined the differences in these analytes compared to those conceived naturally. Secondly, this study provided initial evidence of significant associations between ART and elevated folate and triglyceride levels during late pregnancy. Thirdly, the data for this study were obtained from a large hospital’s real-world database, ensuring that the findings accurately reflect actual conditions and that the study population is highly diverse and representative.
Inevitably, this study still has some disadvantages. Firstly, as a result of the lack of information on causes of infertility and ART procedures in the database, this study did not account for these factors that have been demonstrated to affect the prevalence of GDM. Secondly, due to the observational nature of this study, it was not possible for us to determine a definitive causal relationship. The fact that serum biomarkers were measured only once in late pregnancy, after GDM had been diagnosed, further complicates temporal interpretation and prevents establishing causality. In addition, uncollected or unmeasured confounding factors, such as the socioeconomic status of participants, history of GDM, and dietary habits including folate supplementation, may still influence the results. Thirdly, there is a potential for selection bias since the study included only participants with recorded measures of hepatic and renal function, blood lipids, and serum levels of folate, vitamin B12, and tHcy from a single institution. The generalizability of these results to broader contexts and populations requires additional validation.
Conclusion
This study confirms that Chinese women who conceive by ART have a significantly higher prevalence of GDM, a risk that is further elevated among those of advanced age, people with obesity, or those with multiparity. Our findings also show that ART pregnancies are associated with altered metabolic profiles, specifically higher serum levels of folate and triglycerides, which are themselves independent correlates of GDM. Future studies measuring these biomarkers earlier in gestation are required to investigate their potential causal contribution to the underlying mechanism linking ART and GDM. If confirmed, these findings highlight the importance of monitoring folate and triglyceride levels during pregnancy, particularly in ART-conceived pregnancies, with attention to folate supplementation dosage and lipid control.
Data availability
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
References
Wang H, Li N, Chivese T, Werfalli M, Sun H, Yuen L, et al. IDF Diabetes Atlas Committee Hyperglycaemia in Pregnancy Special Interest Group. IDF Diabetes Atlas: Estimation of Global and Regional Gestational Diabetes Mellitus Prevalence for 2021 by International Association of Diabetes in Pregnancy Study Group’s Criteria. Diab Res Clin Pract. 2022;183:109050.
Ye W, Luo C, Huang J, Li C, Liu Z, Liu F. Gestational diabetes mellitus and adverse pregnancy outcomes: systematic review and meta-analysis. BMJ. 2022;377:e067946.
Moon JH, Jang HC. Gestational Diabetes Mellitus: Diagnostic Approaches and Maternal-Offspring Complications. Diab Metab J. 2022;46:3–14.
Reddy UM, Wapner RJ, Rebar RW, Tasca RJ. Infertility, assisted reproductive technology, and adverse pregnancy outcomes: executive summary of a National Institute of Child Health and Human Development workshop. Obstet Gynecol. 2007;109:967–77.
Ashrafi M, Gosili R, Hosseini R, Arabipoor A, Ahmadi J, Chehrazi M. Risk of gestational diabetes mellitus in patients undergoing assisted reproductive techniques. Eur J Obstet Gynecol Reprod Biol. 2014;176:149–52.
Silberstein T, Levy A, Harlev A, Saphier O, Sheiner E. Perinatal outcome of pregnancies following in vitro fertilization and ovulation induction. J Matern Fetal Neonatal Med. 2014;27:1316–9.
Yang X, Li Y, Li C, Zhang W. Current overview of pregnancy complications and live-birth outcome of assisted reproductive technology in mainland China. Fertil Steril. 2014;101:385–91.
Zhu L, Zhang Y, Liu Y, Zhang R, Wu Y, Huang Y, et al. Maternal and Live-birth Outcomes of Pregnancies following Assisted Reproductive Technology: A Retrospective Cohort Study. Sci Rep. 2016;6:35141.
Qin J, Sheng X, Wu D, Gao S, You Y, Yang T, et al. Adverse Obstetric Outcomes Associated With In Vitro Fertilization in Singleton Pregnancies. Reprod Sci. 2017;24:595–608.
Cai S, Natarajan P, Chan JKY, Wong PC, Tan KH, Godfrey KM, et al. Maternal hyperglycemia in singleton pregnancies conceived by IVF may be modified by first-trimester BMI. Hum Reprod. 2017;32:1941–7.
Dayan N, Fell DB, Guo Y, Wang H, Velez MP, Spitzer K, et al. Severe maternal morbidity in women with high BMI in IVF and unassisted singleton pregnancies. Hum Reprod. 2018;33:1548–56.
Harlev A, Walfisch A, Oran E, Har-Vardi I, Friger M, Lunenfeld E, et al. The effect of fertility treatment on adverse perinatal outcomes in women aged at least 40 years. Int J Gynaecol Obstet. 2018;140:98–104.
Lee B, Koeppel AF, Wang ET, Gonzalez TL, Sun T, Kroener L, et al. Differential gene expression during placentation in pregnancies conceived with different fertility treatments compared with spontaneous pregnancies. Fertil Steril. 2019;111:535–46.
Yang P, Kang H, Ma C, Wei Y, Tao L, Wu Z. Risk of preterm delivery in singletons conceived by in vitro fertilization. Gynecol Endocrinol. 2019;35:661–4.
Lei LL, Lan YL, Wang SY, Feng W, Zhai ZJ. Perinatal complications and live-birth outcomes following assisted reproductive technology: a retrospective cohort study. Chin Med J (Engl). 2019;132:2408–16.
Wang J, Liu Q, Deng B, Chen F, Liu X, Cheng J. Pregnancy outcomes of Chinese women undergoing IVF with embryonic cryopreservation as compared to natural conception. BMC Pregnancy Childbirth. 2021;21:39.
Stern JE, Liu CL, Cui X, Cabral HJ, Farland LV, Coddington C, et al. Assisted reproductive technology treatment increases obstetric and neonatal risks over that of the underlying infertility diagnosis. Fertil Steril. 2022;117:1223–34.
He M, Sun X, Wang C, Sui Y. Analysis of the risk of complications during pregnancy in pregnant women with assisted reproductive technology: a retrospective study using registry linkage from 2013 to 2018 in Shanghai, China. BMC Pregnancy Childbirth. 2022;22:526.
Bianchi C, Brocchi A, Baronti W, Nicolì F, Citro F, Aragona M, et al. Assisted reproductive technology, risk of gestational diabetes, and perinatal outcomes in singleton pregnancies. Diab Metab Res Rev. 2023;39:e3625.
Li M, Chen Y, Wang Y, Wang H, Ding X, Li G. Maternal gestational diabetes in singleton pregnancies conceived by ART may be modified by periconceptional B vitamins. Front Nutr. 2023;9:1069911.
Kuivasaari-Pirinen P, Raatikainen K, Hippeläinen M, Heinonen S. Adverse Outcomes of IVF/ICSI Pregnancies Vary Depending on Aetiology of Infertility. ISRN Obstet Gynecol. 2012;2012:451915.
Farhi A, Reichman B, Boyko V, Hourvitz A, Ron-El R, Lerner-Geva L. Maternal and neonatal health outcomes following assisted reproduction. Reprod Biomed Online. 2013;26:454–61.
Luke B, Gopal D, Cabral H, Stern JE, Diop H. Pregnancy, birth, and infant outcomes by maternal fertility status: the Massachusetts Outcomes Study of Assisted Reproductive Technology. Am J Obstet Gynecol. 2017;217:327.e1–327.e14.
Frankenthal D, Hirsh-Yechezkel G, Boyko V, Orvieto R, Ron-El R, Lerner-Geva L, et al. The effect of body mass index (BMI) and gestational weight gain on adverse obstetrical outcomes in pregnancies following assisted reproductive technology as compared to spontaneously conceived pregnancies. Obes Res Clin Pract. 2019;13:150–5.
Nagata C, Yang L, Yamamoto-Hanada K, Mezawa H, Ayabe T, Ishizuka K, et al. Japan Environment & Children’s Study Group. Complications and adverse outcomes in pregnancy and childbirth among women who conceived by assisted reproductive technologies: a nationwide birth cohort study of Japan environment and children’s study. BMC Pregnancy Childbirth. 2019;19:77.
Szymusik I, Kosinska-Kaczynska K, Krowicka M, Sep M, Marianowski P, Wielgos M. Perinatal outcome of in vitro fertilization singletons - 10 years’ experience of one center. Arch Med Sci. 2019;15:666–72.
Lavie I, Lavie M, Doyev R, Fouks Y, Azem F, Yogev Y. Pregnancy outcomes in women with inflammatory bowel disease who successfully conceived via assisted reproduction technique. Arch Gynecol Obstet. 2020;302:611–8.
Sesmilo G, Prats P, Álvarez M, Romero I, Guerrero M, Rodríguez I, et al. Gestational diabetes prevalence and outcomes in women undergoing assisted reproductive techniques (ART). Endocrinol Diab Nutr (Engl Ed). 2022;69:837–43.
Lai JS, Pang WW, Cai S, Lee YS, Chan JKY, Shek LPC, et al. High folate and low vitamin B12 status during pregnancy is associated with gestational diabetes mellitus. Clin Nutr. 2018;37:940–7.
Li S, Hou Y, Yan X, Wang Y, Shi C, Wu X, et al. Joint effects of folate and vitamin B12 imbalance with maternal characteristics on gestational diabetes mellitus. J Diab. 2019;11:744–51.
Saravanan P, Sukumar N, Adaikalakoteswari A, Goljan I, Venkataraman H, Gopinath A, et al. Association of maternal vitamin B12 and folate levels in early pregnancy with gestational diabetes: a prospective UK cohort study (PRiDE study). Diabetologia. 2021;64:2170–82.
Ryckman KK, Spracklen CN, Smith CJ, Robinson JG, Saftlas AF. Maternal lipid levels during pregnancy and gestational diabetes: a systematic review and meta-analysis. BJOG. 2015;122:643–51.
Yuan XS, Shi H, Wang HY, Yu B, Jiang J. Ficolin-3/adiponectin ratio for the prediction of gestational diabetes mellitus in pregnant women. J Diab Investig. 2018;9:403–10.
Yuan X, Gao Y, Zhang M, Long W, Liu J, Wang H, et al. Fibrin/fibrinogen degradation products in late pregnancy promote macrosomia prediction in normal uncomplicated pregnancy. Placenta. 2020;96:27–33.
Yuan X, Gao Y, Zhang M, Long W, Liu J, Wang H, et al. Association of maternal D-dimer level in late pregnancy with birth outcomes in a Chinese cohort. Clin Chim Acta. 2020;501:258–63.
Yuan X, Han X, Jia C, Zhou W, Yu B. Low Fetal Fraction of Cell Free DNA at Non-Invasive Prenatal Screening Increases the Subsequent Risk of Preterm Birth in Uncomplicated Singleton Pregnancy. Int J Women’s Health. 2022;14:889–97.
Yuan X, Hu H, Zhang M, Long W, Liu J, Jiang J, et al. Iron deficiency in late pregnancy and its associations with birth outcomes in Chinese pregnant women: a retrospective cohort study. Nutr Metab (Lond). 2019;16:30.
Pandey S, Shetty A, Hamilton M, Bhattacharya S, Maheshwari A. Obstetric and perinatal outcomes in singleton pregnancies resulting from IVF/ICSI: a systematic review and meta-analysis. Hum Reprod Update. 2012;18:485–503.
Qin J, Liu X, Sheng X, Wang H, Gao S. Assisted reproductive technology and the risk of pregnancy-related complications and adverse pregnancy outcomes in singleton pregnancies: a meta-analysis of cohort studies. Fertil Steril. 2016;105:73–85. e1-6.
Palomba S, Homburg R, Santagni S, La Sala GB, Orvieto R. Risk of adverse pregnancy and perinatal outcomes after high technology infertility treatment: a comprehensive systematic review. Reprod Biol Endocrinol. 2016;14:76.
Storgaard M, Loft A, Bergh C, Wennerholm UB, Söderström-Anttila V, Romundstad LB, et al. Obstetric and neonatal complications in pregnancies conceived after oocyte donation: a systematic review and meta-analysis. BJOG. 2017;124:561–72.
Bosdou JK, Anagnostis P, Goulis DG, Lainas GT, Tarlatzis BC, Grimbizis GF, et al. Risk of gestational diabetes mellitus in women achieving singleton pregnancy spontaneously or after ART: a systematic review and meta-analysis. Hum Reprod Update. 2020;26:514–44.
Maroufizadeh S, Navid B, Alizadeh A, Amini P, Almasi-Hashiani A, Mohammadi M, et al. Risk of gestational diabetes mellitus following assisted reproductive technology: systematic review and meta-analysis of 59 cohort studies. J Matern Fetal Neonatal Med. 2021;34:2731–40.
Ban M, Sun Y, Chen X, Zhou X, Zhang Y, Cui L. Association between maternal polycystic ovarian syndrome undergoing assisted reproductive technology and pregnancy complications and neonatal outcomes: a systematic review and meta-analysis. J Ovarian Res. 2024;17:6.
Kouhkan A, Khamseh ME, Moini A, Pirjani R, Valojerdi AE, Arabipoor A, et al. Predictive factors of gestational diabetes in pregnancies following assisted reproductive technology: a nested case-control study. Arch Gynecol Obstet. 2018;298:199–206.
Sferruzzi-Perri AN, Lopez-Tello J, Napso T, Yong HEJ. Exploring the causes and consequences of maternal metabolic maladaptations during pregnancy: Lessons from animal models. Placenta. 2020;98:43–51.
Li Q, Zhang Y, Huang L, Zhong C, Chen R, Zhou X, et al. High-Dose Folic Acid Supplement Use From Prepregnancy Through Midpregnancy Is Associated With Increased Risk of Gestational Diabetes Mellitus: A Prospective Cohort Study. Diab Care. 2019;42:e113–e115.
Xu R, Liu S, Zhong Z, Guo Y, Xia T, Chen Y, et al. The Influence of Maternal Folate Status on Gestational Diabetes Mellitus: A Systematic Review and Meta-Analysis. Nutrients. 2023;15:2766.
Ashrafi M, Sheikhan F, Arabipoor A, Hosseini R, Nourbakhsh F, Zolfaghari Z. Gestational diabetes mellitus risk factors in women with polycystic ovary syndrome (PCOS). Eur J Obstet Gynecol Reprod Biol. 2014;181:195–9.
Liu Y, Hocher JG, Ma S, Hu L, Chen H, Zhang X, et al. Pre-pregnancy LDL/HDL and total Cholesterol/HDL ratios are strong predictors of gestational diabetes mellitus in women undergoing assisted reproductive technologies. Reprod Biol Endocrinol. 2024;22:155.
Acknowledgements
We thank all participants of this study and the staff of the laboratory and medical record sections from Changzhou Maternal and Child Health Care Hospital for their technical assistance and information service.
Funding
This research received grants from Noncommunicable Chronic Diseases-National Science and Technology Major Project (2024ZD0532100, 2024ZD0532103), National Natural Science Foundation of China (82371697, 81971410), Top Talent of Changzhou “The 14th Five-Year Plan” High-Level Health Talents Training Project, General project of Jiangsu Provincial Health Commission (H2023131), Key Project of Changzhou Medical Center of Nanjing Medical University (CMCM202312), Changzhou Key Laboratory of Maternal and Child Health Medicine (Grant No. CM20240013), Graduate Research and Practice Innovation Plan of Jiangsu Province (SJCX24_0749).
Author information
Authors and Affiliations
Contributions
Xiaosong Yuan: Writing–original draft, Conceptualization. Bin Zhang: Investigation, Data curation. Sijie Xi: Methodology, Investigation. Runrun Hao: Formal analysis, Conceptualization. Zhaolong Zhan: Resources. Zhonghua Shi: Writing–review & editing, Supervision, Conceptualization.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval
The study protocol was approved by the Ethics Committee of Changzhou Maternal and Child Health Care Hospital (ZD201803). Owing to the anonymous data recorded in the present study, the requirement for written informed consent was waived by the Ethics Committee of Changzhou Maternal and Child Health Care Hospital. All methods were performed in accordance with the relevant guidelines and regulations.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Zhang, B., Xi, S., Hao, R. et al. Association between assisted reproductive technology and gestational diabetes mellitus: the role of serum folate and triglycerides. Nutr. Diabetes 16, 7 (2026). https://doi.org/10.1038/s41387-026-00414-0
Received:
Revised:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41387-026-00414-0
