
Abstract
Cardiovascular disease (CVD) is a major complication in individuals with chronic kidney disease (CKD). In Japan, the incidence of CVD among persons with CKD is lower than that in the United States. Although various classes of antihypertensive agents are prescribed to prevent CVD, the proportion varies between the United States and Japan. Until now, few studies have compared clinical practices and CVD prevalence among patients with CKD in the United States vs. Japan. In this study, we performed a cross-sectional comparison of the prevalence of CVD and the prescription of β-blockers at study entry to the Chronic Kidney Disease Japan Cohort (CKD-JAC) Study and the Chronic Renal Insufficiency Cohort (CRIC) Study. The mean patient age was 58.2 and 60.3 years, the mean estimated glomerular filtration rate (eGFR) was 42.8 and 28.9 (mL/min/1.73 m2), and the median urinary albumin:creatinine ratio was 51.9 and 485.9 (mg/g) among 3939 participants in the CRIC Study and 2966 participants in the CKD-JAC Study, respectively. The prevalence of any CVD according to a self-report (CRIC Study) was 33%, while that according to a medical chart review (CKD-JAC Study) was 24%. These findings were consistent across eGFR levels. Prescriptions for β-blockers differed between the CRIC and CKD-JAC Studies (49% and 20%, respectively). The odds ratios for the association of any history of CVD and β-blocker prescription were 3.0 [2.6–3.5] in the CRIC Study and 2.0 [1.6–2.5] in the CKD-JAC Study (P < 0.001 for the interaction). In conclusion, the prevalence of CVD and treatment with β-blockers were higher in the CRIC Study across eGFR levels.
Similar content being viewed by others
Introduction
Cardiovascular diseases (CVDs) are important outcome events in both patients with chronic kidney disease (CKD) not dependent on dialysis and among those with end-stage kidney disease (ESKD) [1,2,3,4,5,6]. Although CVD is a major cause of death among patients with CKD, with prior studies suggesting that individuals with CKD are more likely to die from CVD than develop ESKD [7], studies have shown that the incidence varies among countries [8].
Antihypertensive medications play a crucial role in CVD prevention among individuals with CKD [9]. Although β-blockers are effective for the management of heart disease in patients with CKD [10,11,12,13], the proportion of participants prescribed β-blockers in the Japanese CKD cohort is lower than that in any other CKD cohort in the world [14, 15]. The prevalence of CVD can partly account for this prescription pattern, but the association between β-blocker prescription and CVD history in patients with CKD has not been directly compared between countries. In addition, these prescription patterns might be influenced by patients’ conditions and epidemiological information in each region where clinicians perform their practice [14].
The Chronic Renal Insufficiency Cohort (CRIC) Study and the Chronic Kidney Disease Japan Cohort (CKD-JAC) Study are well-established, large, and diverse CKD cohort studies conducted in the United States and Japan. There are significant differences in the definition of CVDs, such as coronary artery disease (CAD), congestive heart failure (CHF), stroke, and peripheral artery disease (PAD), and in the manner in data were collected with regard to participants’ history of CVDs. While participants self-reported their history of CVDs at enrollment in the CRIC Study, local investigators or treating physicians collected information about the history of CVDs based on a medical chart review in the CKD-JAC Study. Prior studies have shown incomplete agreement between information derived from medical chart reviews and self-reports for heart failure [16]. Therefore, it is necessary to examine the agreement between self-reports and medical records on participants’ history of CVDs.
The aims of this study were to investigate (1) the baseline prevalence of CVDs in well-characterized CKD cohorts in Japan and the United States, (2) the level of agreement between self-reported and medical chart-reviewed information in a subset of CRIC study participants, and (3) the factors contributing to the differences in the prescription patterns of use of antihypertensive medications in these groups.
Methods
Participants
The CRIC Study is an ongoing multicenter, prospective observational cohort study of participants with CKD recruited in seven clinical centers in the United States. We used data from 3939 participants from the Phase I CRIC Study recruited between 2003 and 2008 [17, 18]. The cohort included a racially and ethnically diverse population where the inclusion criteria were estimated glomerular filtration rate (eGFR) = 20–70 mL/min per 1.73 m2 for persons aged 21–44 years, 20–60 mL/min per 1.73 m2 for persons aged 45–64 years, and 20–50 mL/min per 1.73 m2 persons aged 65–74 years based on the MDRD creatinine-based eGFR. Exclusion criteria included prior transplantation, polycystic kidney disease, multiple myeloma, the use of immunosuppression, and severe comorbid illnesses, such as cirrhosis, HIV disease, and severe (New York Heart Association class III or IV) heart failure. The institutional review boards at all clinical sites approved the study protocol, and all participants provided written informed consent.
The CKD-JAC Study is a multicenter, prospective observational cohort study of 2966 participants enrolled at 17 clinical facilities across Japan between April 2007 and December 2008 [19]. The eligibility criteria were as follows: (1) Japanese or Asian patients living in Japan; (2) age 20–75 years; and (3) an eGFR of 10–59 mL/min/1.73 m2. The exclusion criteria were as follows: (1) patients with polycystic kidney disease, human immunodeficiency virus (HIV) infection, liver cirrhosis, or active cancer, and patients who had received cancer treatment within the past 2 years; and (2) transplant recipients and patients who had previously been on long-term dialysis. The protocol was approved by the ethics committee of each participating medical institution, and the study was conducted in accordance with the Declaration of Helsinki. All patients provided written informed consent.
Measurements
In both studies, clinical data, including medical history and anthropometric measurements, were collected at enrollment, and laboratory parameters of blood and urine samples were measured centrally using standardized assays, as reported previously [18, 20]. The eGFR in the CRIC Study was calculated using an equation derived from CRIC Study participants based on serum creatinine and cystatin C levels, age, sex, and race [21], while the eGFR in the CKD-JAC Study was calculated using the Japanese formula derived in Japanese patients with CKD:
eGFR (mL/min/1.73 m2) = 194 × age−0.287 × [serum Cr (mg/mL)]−1.094 × [0.739 if female] [22].
These two equations used to calculate the eGFR were validated with the measured GFR in each source population.
In the CRIC Study, demographic characteristics, medical history, and lifestyle information were collected directly from the study participants. Medication within the past 30 days of enrollment was determined from the prescribed drugs brought to the clinic. Biometric data, such as height, weight, and blood pressure, were obtained using standardized procedures. Hypertension was defined as having either systolic blood pressure ≥140 mmHg, diastolic blood pressure ≥90 mmHg, or the use of any antihypertensive drugs, including diuretics. Diabetes was defined as either having fasting blood glucose ≥126 mg/dL, blood glucose at any time ≥200 mg/dL, or the use of antidiabetic drugs, including insulin injection. In the CKD-JAC Study, the definitions of hypertension and diabetes were the same; however, the baseline information was collected by the treating physicians as recorded in the medical records. The prevalence of atrial fibrillation (AF) was collected via self-reported information at baseline in the CRIC Study, while AF was defined using medical chart-based information or electrocardiographic findings at baseline in the CKD-JAC Study. Regarding BMI, we set the different classifications for Asians and other ethnic groups to adjust for racial diversity: for Asians, BMI was considered < 18.5 underweight, 18.5–22.9 was considered normal, 23–24.9 was considered overweight, 25–29.9 was considered obese I, and BMI ≥ 30 was considered obese II or more; for individuals belonging to other ethnic groups, BMI < 18.5 was considered underweight, 18.5–24.9 was considered normal, 25–29.9 was considered overweight, 30–34.9 was considered obese I, and BMI ≥ 35 was considered obese II or more. A history of CVDs at baseline was thus differently ascertained in the CRIC and CKD-JAC Studies (Supplementary Tables 1 and 2). CVD consists of four components: CAD, CHF, PAD, and stroke. Each component is not mutually exclusive. Individuals with any CVD have at least one CVD subcategory.
Medical chart review
In the present study, we defined CAD as having at least one of the following items: a history of myocardial infarction, a history of effort or resting pectoris, and a history of coronary artery bypass grafting surgery or percutaneous coronary intervention. We also defined PAD as having at least one of the following items: symptoms due to peripheral ischemia such as claudication, limb pain, skin ulcers, or weak pulse; and a history of extremity amputation, bypass, or percutaneous transcatheter angioplasty. Stroke was defined as either cerebral infarction, nontraumatic cerebral hemorrhage, or subarachnoid hemorrhage, with or without significant neurologic sequelae.
To compare the prevalence of CVDs between the CRIC and CKD-JAC Studies, we measured the agreement between self-reported information and medical chart-based information with regard to the history of CVDs in a randomly selected set of CRIC participants at the University of Pennsylvania CRIC Clinical Center (UPENN). The medical charts of ~30% (N = 156) of all CRIC participants at UPENN (N = 507), which were electronically accessible for at least 5 years prior to enrollment, were reviewed by a researcher blinded to the participant-reported information. Data were collected using the same questionnaire that had been used in the CKD-JAC Study.
Statistical analysis
Descriptive data are expressed as the mean ± standard deviation (S.D.) and the median [interquartile range (IQR)] for normally and nonnormally distributed continuous variables, respectively. Between-group differences in categorical, normal, and nonnormally distributed continuous variables were assessed using the chi-squared test, Student’s t-test, and the Wilcoxon rank-sum test, respectively. For the comparison of CVD history, the sensitivity, specificity, positive predictive value, and negative predictive value were calculated. Agreement between self-reports and medical charts was assessed by calculating the Kappa coefficient. Kappa values of <0.40, 0.41 to 0.60, 0.61 to 0.80, and 0.81 to 1.00 were considered poor-to-fair, moderate, substantial, and excellent agreement, respectively [23].
We used multiple imputation to address missing data. To impute missing data, we included variables potentially related to the fact that the data were missing and variables that correlated with outcome [24]. The covariates included in our imputation models were as follows: baseline age; sex, race/ethnicity; income; education attainment; smoking status; eGFR; log-transformed body mass index (BMI); systolic and diastolic blood pressure; log-transformed UACR; history of hypertension, diabetes mellitus, and CVD; and medication information about ACEis/ARBs, CCBs, β-blockers, α-blockers, and diuretics. We conducted chained equations (20 imputations), with logistic regression models for categorical variables and linear regression models for continuous variables and then combined the results across the 20 imputed datasets using Rubin’s formula [25].
Based on findings from prior studies, we explored the association between the eGFR and the prevalence of CVD and whether they differed between the CRIC and CKD-JAC Studies. We modeled the eGFR using an RCS with four knots (at the 20th, 30th, 40th and 50th percentiles of eGFR distribution in the overall cohort) and performed modified Poisson regression analyses with the logarithm link function and robust error variance [26] for each parameter of interest, exploring differences across cohorts (CRIC vs. CKD-JAC) and adjusting for age, sex, albuminuria, and diabetes. The curves were truncated at the limits of the range of eGFR represented in each cohort and the levels where the confidence intervals were 2.5 times wider than the average. We also employed logistic regression to examine the association between the prevalence of CVD and the prescription pattern of β-blockers separately in eGFR categories (<20, 20–30, 30–40, 40–50, 50–60, and >60 mL/min/1.73 m2). Possible interaction by cohort was evaluated with the likelihood ratio test.
We examined the association between β-blocker prescription and the eGFR (the eGFR was modeled using the RCS) across the cohorts adjusting for age, sex, BMI category, albuminuria, diabetes, and history of CVD. We examined whether the association of CVD subcategories and the prescription pattern of β-blockers differed between the two cohorts (CRIC vs. CKD-JAC) using multivariable logistic regression models. In the models, we adjusted for age, sex, race/ethnicity, BMI category, SBP, albuminuria, eGFR, use of ACEis/ARBs, use of Ca channel blockers, use of α-blockers, and use of diuretics. All continuous variables with right-skewed distributions were logarithmically transformed. We also examined the association between AF and β-blocker prescription.
Two-sided p-values less than 0.05 were considered statistically significant. Statistical analyses were performed using Stata/MP 16.0 (Stata Corp., College Station, TX, USA).
Results
Baseline characteristics of the study subjects
The characteristics of the study participants are shown in Table 1. Overall, CRIC participants were younger and more often female than CKD-JAC participants. Due to the different inclusion criteria, the mean estimated glomerular filtration rate (eGFR) levels in the CRIC Study were higher than those in the CKD-JAC Study (42.8 ± 13.5 and 28.9 ± 12.3 mL/min/1.73 m2 in the CRIC and CKD-JAC Studies, respectively). The proportion of participants with diabetes and the average BMI were higher in the CRIC Study, while the urinary albumin:creatinine ratio (UACR) was lower. The proportion of individuals with hypertension in both studies was greater than 90%. The proportions of individuals with AF were 17% and 2% in the CRIC and CKD-JAC Study, respectively. Angiotensin-converting enzyme inhibitors or angiotensin receptor blockers (ACEis/ARBs) and calcium channel blockers (Ca-blockers) were more commonly prescribed to participants in the CKD-JAC Study, while diuretics and β-blockers were more often prescribed to participants in the CRIC Study. The prevalence of any CVD, CAD, CHF, and PAD was higher in the CRIC Study, although the measurement methods were different: self-reported in the CRIC Study and medical chart review in the CKD-JAC Study.
Agreement between self-reported and medical chart-based information in 156 CRIC participants at one CRIC clinical site
Table 2 summarizes the agreement between self-reported CVD history and medical chart-based information in a randomly selected subgroup of CRIC participants at a single site. Medical chart-based reporting was used as the gold standard, and the sensitivity (proportion of participants who were correctly classified as positive based on self-reported information among subjects classified as positive based on medical records) for any CVD, CAD, CHF, stroke, and PAD was substantially high (78.9 to 100%). The specificity (proportion of participants who were correctly classified as negative based on self-reported information among subjects classified as negative based on medical records) for any CVD, CAD, CHF, stroke, and PAD was also high (78.2 to 93.2%). Generally, false positives were more often observed than false negatives. The Kappa statistics were 0.72, 0.78, 0.83, 0.53, and 0.59 for any CVD, CAD, CHF, stoke, and PAD, respectively, which indicated moderate to excellent agreement between the two classification methods.
A comparison of CRIC participants whose medical chart was reviewed (N = 156) and not reviewed (N = 351) in one clinical center (UPENN) is shown in Supplementary Table 3. Although the participants whose medical chart was reviewed were more often female and had a higher prevalence of CVD history, there were no significant differences in other important parameters, such as the eGFR, UACR, systolic or diastolic blood pressure, socioeconomic status, or use of antihypertensive agents.
Restricted cubic splines of CVD prevalence
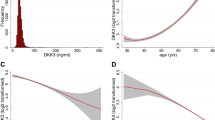
We estimated the predicted probabilities of CVD and its subtypes in both cohorts after adjusting for age, sex, diabetes, and UACR (Fig. 1). The prevalence of any CVD, CAD, and CHF was higher in the CRIC Study than in the CKD-JAC Study at any level of eGFR, while the prevalence of stroke was not different between the two cohorts. Similar results were obtained with the multivariable logistic regression analyses in separate eGFR categories (Supplementary Fig. 1).

RCS for the baseline prevalence of cardiovascular diseases. RCSs show the baseline prevalence of all cardiovascular diseases (a), coronary artery disease (b), congestive heart failure (c), stroke (d), and peripheral artery disease (e) after adjusting for age, sex, diabetes, and log(UACR). RCSs with 95% confidence intervals were truncated at the 1st and 99th percentiles in the CRIC Study and at the 0th and 97th percentiles in the CKD-JAC Study (a); at the 1st and 98th percentiles in the CRIC Study and at the 0th and 98th percentiles in the CKD-JAC Study (b); at the 2nd and 99th percentiles in the CRIC Study and at the 1st and 98th percentiles in the CKD-JAC Study (c); at the 0th and 99th percentiles in the CRIC Study and at the 0th and 97th percentiles in the CKD-JAC Study (d); and at the 1st and 98th percentiles in the CRIC Study and at the 0th and 96th percentiles in the CKD-JAC Study (e). RCS restricted cubic spline, UACR urinary albumin:creatinine ratio
Prescription patterns of antihypertensive agents
Figure 2 shows the patterns of antihypertensive agents (α-blockers, β-blockers, Ca-blockers, and diuretics) and ACEis/ARBs across eGFR categories in each cohort. Diuretics and ACEis/ARBs were commonly prescribed across eGFR categories in both cohorts. However, β-blockers were more often prescribed for participants in the CRIC Study than in the CKD-JAC Study across eGFR categories. ARBs were more commonly prescribed than ACE inhibitors in the CKD-JAC Study, a pattern opposite to that observed in the CRIC Study. In addition, prescriptions for the combination of ACE inhibitors and ARBs were more common for participants in the CKD-JAC Study than in the CRIC Study. Ca blockers and diuretics were more likely to be prescribed as the eGFR decreased.

Medication patterns of antihypertensive drugs (α-blockers, β-blockers, Ca-blockers, and diuretics) (a) and ACEis/ARBs (b) across eGFR categories in each cohort. Combined represents being prescribed both an ACE inhibitor and an ARB. Ca-blocker calcium channel blocker, ACEi angiotensin-converting enzyme inhibitor, ARB angiotensin receptor blocker
Association between β-blocker prescription and CVD history
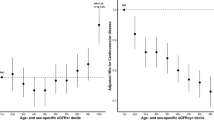
Regarding CVD, all the participants were classified into the following categories: CAD, heart failure (HF) without CAD, CVD without heart disease, and no CVD. Here, heart disease means either CAD or CHF; thus, CVD without heart disease represents either stroke or PAD but not CAD or CHF. We described the association of CVD with AF (Supplementary Table 4). We observed differences in the relative association of β-blocker prescription with CVD and AF (Fig. 3). In the CRIC Study, the OR for β-blocker prescription was 3.0 [2.6–3.5] in the patients with a positive history of any baseline CVD compared to those with no history, whereas in the CKD-JAC Study, the OR was 2.0 [1.6–2.5]. These associations were significantly different across studies (P < 0.001 for interaction). Among the subtypes of CVD, we observed a significant interaction only for CAD. In the CRIC Study, the OR of β-blocker prescription was 4.0 [3.3–4.8] in the patients with a baseline history of CAD to those with no baseline history, whereas in the CKD-JAC Study, the OR was only 2.6 [1.9–3.4] (P < 0.001 for interaction). In the CRIC Study, the OR for β-blocker prescription was 1.9 [1.6–2.3] in patients with AF compared to those with no AF, whereas in the CKD-JAC Study, the OR was 2.8 [1.6–5.0], with no significant interaction (P = 0.41 for interaction).

Forest plot of the ORs for β-blocker prescription in each cohort and the interactions between CVDs and the cohorts. Multivariable logistic regression models were adjusted for age, sex, BMI category, log(UACR), eGFR, diabetes mellitus, ACEis/ARBs, α-blockers, Ca-blockers, and diuretics. *Heart disease represents either CAD or CHF. OR odds ratio, CVD cardiovascular disease, UACR urinary albumin:creatinine ratio, ACEi angiotensin-converting enzyme inhibitor, ARB angiotensin receptor blocker, Ca-blocker calcium channel blocker
We also performed RCS analyses to characterize the prescription patterns of β-blockers across eGFR levels and history of any CVD in both cohorts, as shown in Fig. 4. β-Blockers were more commonly prescribed in the CRIC Study than in the CKD-JAC Study, and the difference was more prominent when stratified by history of any CVD. Similar results were obtained from the multivariable logistic regression analyses in separate eGFR categories (Supplementary Fig. 2).

RCS for the baseline prescriptions of β-blockers. RCSs show the baseline prescription of β-blockers after adjusting for age, sex, BMI category, systolic blood pressure, diabetes mellitus, log(UACR), and atrial fibrillation (a) and stratified by the presence of any CVD history—those with any CVD history (b) and those without CVD history (c). RCSs with 95% confidence intervals were truncated at the 1st and 99th percentiles in the CRIC Study and at the 0th and 97th percentiles in the CKD-JAC Study (a); at the 1st and 97th percentiles in the CRIC Study and at the 0th and 96th percentiles in the CKD-JAC Study (b); and at the 1st and 99th percentiles in the CRIC Study and at the 0th and 98th percentiles in the CKD-JAC Study (c). The interaction represents eGFR × cohorts (CKD-JAC vs. CRIC). RCS restricted cubic spline, CVD cardiovascular disease, CHF congestive heart failure, UACR urinary albumin:creatinine ratio
Discussion
In the present cross-sectional study, we demonstrated that the prevalence of CVD was higher in the CRIC Study than in the CKD-JAC study both overall and across eGFR levels. In addition, β-blocker use was lower in CKD-JAC Study than in CRIC Study, even among individuals with CVD. This finding suggests that the use of β-blockers might be less influenced by the presence of CVD in Japan than in the United States.
The present study showed that the association between β-blocker use and CVD history was particularly stronger among individuals with a history of CAD, which showed a lower prevalence in Japan than in the United States. This result suggests that Japanese physicians are less likely to prescribe β-blockers to patients with a history of CAD. β-Blockers are commonly prescribed for those who are at high risk for CAD within the CKD population [11, 12, 27, 28]. Nevertheless, the frequency of β-blocker prescriptions within this population has been low in Japan [15, 19]. Potential reasons for such a difference in clinical practice include (1) a lower prevalence of CAD in Japan than in other Western countries [29] and (2) differences in healthcare systems between countries expressed as a discrepancy in coronary interventions, especially for patients in nonacute settings [30, 31]. In Japan, patients who are suspected of having CAD may be more likely to receive coronary interventions than in the United States, which may have led to a differential ascertainment of CAD between the two countries. Finally, diagnosing or even holding concerns about coronary vasospasm can have a significant impact on decision making. Prior studies have shown that β-blockers can induce coronary vasospasm, and its frequency is much higher in Japan than in other countries [32, 33]. Since coronary vasospasm can cause myocardial infarction and sudden cardiac death, some physicians may avoid the proactive prescription of β-blockers. Another study showed that the incidence of vasospastic angina in White patients may be as frequent as that in Asian patients, which implies that vasospasm of the coronary arteries may actually occur more frequently than previously considered [34]. Given the growing awareness of vasospasm among Western doctors [35], the practice of β-blocker treatment may change in the future in the United States as well. Another reason for the differences in antihypertensive medication may also be related to the differences in health care and insurance systems between Japan and the United States. For example, the use of ARBs differed among insurance providers in the United States [36], while in Japan, universal health care did not hinder physicians from prescribing such relatively expensive agents.
The present study had three major methodological advantages over past research. First, we were able to compare the baseline demographics, disease prevalence, and prescription patterns of antihypertensive medications using individual data from well-established CKD cohorts in the United States and Japan. Second, we investigated the agreement of two different methods to assess CVD prevalence using data from one clinical facility in the CRIC Study, which showed a high level of consistency. A prior study showed that the agreement between self-assessed and professional-assessed medical history was not good, especially regarding CHF [16]. In contrast, the present study showed substantial to excellent agreement regarding CAD and CHF. These findings suggest that self-reported medical information is a reliable alternative to medical record review for detecting a history of CVD (as in the CRIC Study), thereby facilitating comparisons between the CRIC and CKD-JAC Studies. Third, we investigated the adjusted probability of β-blocker prescriptions between the two cohorts across eGFR levels. We also performed the analysis stratified by CVD history, which we hypothesized would be associated with the prescription patterns of antihypertensive medications.
There were several limitations to the present study. First, the manner in which medical information was collected was different, especially concerning the history of CVD. Despite the high concordance rate between the two cohorts, self-reported information may have overestimated the prevalence of CVD in the CRIC Study. Since this bias was towards the null hypothesis, there should have been a larger difference in the association between CVD history and β-blocker prescriptions across studies. Second, since this was a cross-sectional study, we do not know whether β-blocker prescription patterns affect prognosis. However, despite the infrequent use of β-blockers among CKD-JAC participants, these individuals showed a better cardiovascular prognosis than those in the United States [37]. Different characteristics in terms of CAD and AF between Western and Japanese people likely determine the prescription of β-blockers. We believe that the use of β-blockers does not explain the difference in prognosis between countries, but this is beyond the scope of the current study. Further research is needed to elucidate the pathophysiological differences in CKD patients in Japan and those in the United States.
In conclusion, we demonstrated that the prevalence of CVD was higher in the CRIC Study across a broad range of kidney functions despite CRIC Study participants being younger and having better baseline kidney function. The association between CVD history and β-blocker prescription was stronger in the CRIC Study. The prescription pattern of β-blockers based on CVD history may have been influenced by the pathophysiological differences in CAD between the two countries as well as the difference in clinical practices.
References
de Jager DJ, Grootendorst DC, Jager KJ, van Dijk PC, Tomas LMJ, Ansell D, et al. Cardiovascular and noncardiovascular mortality among patients starting dialysis. JAMA. 2009;302:1782–9.
Ninomiya T, Kiyohara Y, Kubo M, Tanizaki Y, Doi Y, Okubo KEN, et al. Chronic kidney disease and cardiovascular disease in a general Japanese population: the Hisayama Study. Kidney Int. 2005;68:228–36.
Keith DS, Nichols GA, Gullion CM, Brown JB, Smith DH. Longitudinal follow-up and outcomes among a population with chronic kidney disease in a large managed care organization. Arch Intern Med. 2004;164:659–63.
Manjunath G, Tighiouart H, Ibrahim H, MacLeod B, Salem DN, Griffith JL, et al. Level of kidney function as a risk factor for atherosclerotic cardiovascular outcomes in the community. J Am Coll Cardiol. 2003;41:47–55.
Muntner P, He J, Hamm L, Loria C, Whelton PK. Renal insufficiency and subsequent death resulting from cardiovascular disease in the United States. J Am Soc Nephrol. 2002;13:745–53.
Foley RN, Parfrey PS, Sarnak MJ. Clinical epidemiology of cardiovascular disease in chronic renal disease. Am J Kidney Dis. 1998;32:S112–119.
Go AS, Chertow GM, Fan D, McCulloch CE, Hsu C. Chronic kidney disease and the risks of death, cardiovascular events, and hospitalization. N Engl J Med. 2004;351:1296–305.
Grams ME, Sang Y, Ballew SH, Carrero JJ, Djurdjev O, Heerspink HJL, et al. Predicting timing of clinical outcomes in patients with chronic kidney disease and severely decreased glomerular filtration rate. Kidney Int. 2018;93:1442–51.
Eckardt KU, Bansal N, Coresh J, Evans M, Grams ME, Herzog CA, et al. Improving the prognosis of patients with severely decreased glomerular filtration rate (CKD G4+): conclusions from a Kidney Disease: Improving Global Outcomes (KDIGO) Controversies Conference. Kidney Int. 2018;93:1281–92.
Segall L, Nistor I, Covic A. Heart failure in patients with chronic kidney disease: a systematic integrative review. Biomed Res Int. 2014;2014:937398.
Badve SV, Roberts MA, Hawley CM, Cass A, Garg AX, Krum H, et al. Effects of beta-adrenergic antagonists in patients with chronic kidney disease: a systematic review and meta-analysis. J Am Coll Cardiol. 2011;58:1152–61.
Wali RK, Iyengar M, Beck GJ, Chartyan DM, Chonchol M, Ann Lukas M, et al. Efficacy and safety of carvedilol in treatment of heart failure with chronic kidney disease: a meta-analysis of randomized trials. Circ Hear Fail. 2011;4:18–26.
Matsushita K, Minamishima T, Sakata K, Satoh T, Yoshino H. Prognostic factors for one-year mortality in patients with acute heart failure with and without chronic kidney disease: differential impact of beta-blocker and diuretic treatments. Hypertens Res. 2019;42:1011–8.
Alencar de Pinho N, Levin A, Fukagawa M, Hoy WE, Pecoits-Filho R, Reichel H, et al. Considerable international variation exists in blood pressure control and antihypertensive prescription patterns in chronic kidney disease. Kidney Int. 2019;96:983–94.
Drawz PE, Brown R, De Nicola L, Fujii N, Gabbai FB, Gassman J, et al. Variations in 24-hour BP profiles in cohorts of patients with kidney disease around the world: the I-DARE study. Clin J Am Soc Nephrol. 2018;13:1348–57.
Okura Y, Urban LH, Mahoney DW, Jacobsen SJ, Rodeheffer RJ. Agreement between self-report questionnaires and medical record data was substantial for diabetes, hypertension, myocardial infarction and stroke but not for heart failure. J Clin Epidemiol. 2004;57:1096–103.
Lash JP, Go AS, Appel LJ, He J, Ojo A, Rahman M, et al. Chronic renal insufficiency cohort (CRIC) study: Baseline characteristics and associations with kidney function. Clin J Am Soc Nephrol. 2009;4:1302–11.
Feldman HI. The chronic renal insufficiency cohort (CRIC) study: design and methods. J Am Soc Nephrol. 2003;14:148S–153.
Imai E, Matsuo S, Makino H, Watanabe T, Akizawa T, Nitta K, et al. Chronic Kidney Disease Japan cohort study: baseline characteristics and factors associated with causative diseases and renal function. Clin Exp Nephrol. 2010;14:558–70.
Imai E, Matsuo S, Makino H, Watanabe T, Akizawa T, Nitta K, et al. Chronic Kidney Disease Japan Cohort (CKD-JAC) study: design and methods. Hypertens Res. 2008;31:1101–7.
Anderson AH, Yang W, Hsu C, Joffe MM, Leonard MB, Xie D, et al. Estimating GFR among participants in the chronic renal insufficiency cohort (CRIC) study. Am J Kidney Dis. 2012;60:250–61.
Matsuo S, Imai E, Horio M, Yasuda Y, Tomita K, Nitta K, et al. Revised equations for estimated GFR from serum creatinine in Japan. Am J Kidney Dis. 2009;53:982–92.
Landis JR, Koch GG. The measurement of observer agreement for categorical data. Biometrics. 2016;33:159–74.
van Buuren S, Boshuizen HC, Knook DL. Multiple imputation of missing blood pressure covariates in survival analysis. Stat Med. 1999;18:681–94.
Graham JW, Olchowski AE, Gilreath TD. How many imputations are really needed? Some practical clarifications of multiple imputation theory. Prev Sci. 2007;8:206–13.
Zou G. Modified poisson regression approach to prospective studies with binary data. Am J Epidemiol. 2004;159:702–6.
Chang TI, Yang J, Freeman JV, Hlatky MA, Go AS. Effectiveness of β-blockers in heart failure with left ventricular systolic dysfunction and chronic kidney disease. J Card Fail. 2013;19:176–82.
Gurwitz JH, Magid DJ, Smith DH, Tabada GH, Sung SH, Allen LA, et al. Treatment effectiveness in heart failure with comorbidity: lung disease and kidney disease. J Am Geriatr Soc. 2017;65:2610–8.
Ueshima H, Sekikawa A, Miura K, Turin TC, Takashima N, Kita Y, et al. Cardiovascular disease and risk factors in Asia. Circulation. 2008;118:2702–9.
Inohara T, Kohsaka S, Miyata H, Ueda I, Noma S, Suzuki M, et al. Appropriateness of coronary interventions in Japan by the US and Japanese standards. Am Heart J. 2014;168:854.e11
Maekawa Y, Fukuda K, Inohara T, Kohsaka S, Ueda I, Yagi T, et al. Application of appropriate use criteria for percutaneous coronary intervention in Japan. World J Cardiol. 2016;8:456–63.
Yasue H, Nakagawa H, Itoh T, Harada E, Mizuno Y. Coronary artery spasm - clinical features, diagnosis, pathogenesis, and treatment. J Cardiol. 2008;51:2–17.
Pristipino C, Beltrame JF, Finocchiaro ML, Hattori R, Fujita M, Mongiardo R, et al. Major racial differences in coronary constrictor response between Japanese and Caucasians with recent myocardial infarction. Circulation. 2000;101:1102–8.
Ong P, Athanasiadis A, Borgulya G, Vokshi I, Bastiaenen R, Kubik S, et al. Clinical usefulness, angiographic characteristics, and safety evaluation of intracoronary acetylcholine provocation testing among 921 consecutive white patients with unobstructed coronary arteries. Circulation. 2014;129:1723–30.
Beltrame JF, Crea F, Kaski JC, Ogawa H, Ong P, Sechtem U, et al. Coronary vasomotion disorders international study group (COVADIS). The Who, what, why, when, how and where of vasospastic angina. Circ J. 2016;80:289–98.
Shah SJ, Stafford RS. Current trends of hypertension treatment in the United States. Am J Hypertens. 2017;30:1008–14.
Tanaka K, Watanabe T, Takeuchi A, Ohashi Y, Nitta K, Akizawa T, et al. Cardiovascular events and death in Japanese patients with chronic kidney disease. Kidney Int. 2017;91:227–34.
Acknowledgements
We thank all the investigators and participants of the CRIC Study and the CKD-JAC Study for their contributions. The CKD-JAC Study was conducted by principal investigators at the following facilities: JCHO Sendai Hospital, JA Toride Medical Center, Jichi Medical University, Tokyo Women’s Medical University Hospital, St. Luke’s International Hospital, Showa University Hospital, Showa University Yokohama Northern Hospital, Showa University Fujigaoka Hospital, Gifu Prefectural General Medical Center, Kasugai Municipal Hospital, Tosei General Hospital, Osaka University Hospital, Osaka General Medical Center, Osaka City General Hospital, Kurashiki Central Hospital, Fukuoka Red Cross Hospital, and Iizuka Hospital.
The CRIC Study Investigators
Lawrence J. Appel12,13, Alan S. Go14, James P. Lash15, Robert G. Nelson16, Mahboob Rahman17, Panduranga S. Rao18, Vallabh O. Shah19, Raymond R. Townsend20, Mark L. Unruh21
Funding
The CRIC Study was obtained under a cooperative agreement from the National Institute of Diabetes and Digestive and Kidney Diseases (U01DK060990, U01DK060984, U01DK061022, U01DK061021, U01DK061028, U01DK060980, U01DK060963, U01DK060902 and U24DK060990). In addition, this work was supported in part by the Perelman School of Medicine at the University of Pennsylvania Clinical and Translational Science Award (NIH/NCATS UL1TR000003), Johns Hopkins University (UL1 TR-000424), the University of Maryland (GCRC M01 RR-16500), the Clinical and Translational Science Collaborative of Cleveland (UL1TR000439), the National Center for Advancing Translational Sciences (NCATS) component of the National Institutes of Health and the NIH roadmap for Medical Research, Michigan Institute for Clinical and Health Research (MICHR) (UL1TR000433), the University of Illinois at Chicago (CTSA UL1RR029879), Tulane COBRE for Clinical and Translational Research in Cardiometabolic Diseases (P20 GM109036), Kaiser Permanente (NIH/NCRR UCSF-CTSI UL1 RR-024131), and the Department of Internal Medicine, University of New Mexico School of Medicine Albuquerque, NM (R01DK119199).
Author information
Authors and Affiliations
Consortia
Corresponding author
Ethics declarations
Conflict of interest
The CKD-JAC Study was financially supported by Kyowa Kirin Company (KKC). The funding agencies had no role in the study design; collection, analysis, or interpretation of data; or decision to submit the report for publication. Advisory role: HF (Kyowa Kirin Company);Honoraria: TI, TH, LN, and SM (Kyowa Kirin Company), NF (Kyowa Kirin Company, Chugai, Torii Pharmaceutical, Baxter and Ono Pharmaceutical), MF (Kyowa Kirin Company, Ono-Pharmaceutical, Kissei Pharmaceutical, Bayer Yakuhin, Ono Pharmaceutical, and Torii Pharmaceutical), and HF (Kyowa Kirin Company and InMed, Inc.) All remaining authors have nothing to disclose.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Members of the CRIC Study Investigators are listed below Acknowledgements.
Rights and permissions
About this article

Cite this article
Imaizumi, T., Hamano, T., Fujii, N. et al. Cardiovascular disease history and β-blocker prescription patterns among Japanese and American patients with CKD: a cross-sectional study of the CRIC and CKD-JAC studies. Hypertens Res 44, 700–710 (2021). https://doi.org/10.1038/s41440-020-00608-8
Received:
Revised:
Accepted:
Published:
Version of record:
Issue date:
DOI: https://doi.org/10.1038/s41440-020-00608-8
Keywords
This article is cited by
-
Development and validation of an algorithm for identifying patients undergoing dialysis from patients with advanced chronic kidney disease
Clinical and Experimental Nephrology (2025)

{kind=link}
{kind=link}