
Abstract
To ensure progress towards zero new HIV infections, more detailed information is needed about why certain individuals might not successfully transition through the steps of the HIV care continuum. We used data from 21,788 individuals with HIV who were enrolled in the ATHENA cohort before 31 December 2023, and combined these with registry data from Statistics Netherlands. This allowed modeling socio-demographic, -economic, and health-related determinants of not achieving two milestones of the HIV care continuum, i.e., suppressed viral load and engagement in care. Across all subgroups of men who have sex with men (MSM), cisgender heterosexual men, and women, living in poverty was associated with having detectable viral loads and disengagement from care, and younger age with only detectable viral loads. In MSM, having only primary education, a second-generation migration background, and living in a single-parent, institutionalized, or other household was also associated with having a detectable viral load. The HIV care continuum in the Netherlands is heavily influenced by socio-economic, rather than health-related, determinants. Efforts to optimize HIV care through specialized interventions should consider individual economic vulnerability. Our findings also illustrate the value of using registry data to identify gaps in care.
Similar content being viewed by others
Introduction
Since the introduction of antiretroviral therapy (ART), HIV-related morbidity and mortality have been substantially reduced. Moreover, by suppressing circulating HIV RNA levels to undetectable levels, successful ART has made onward transmission of HIV impossible1,2,3. The HIV care continuum, which is represented by the chain of events from a person’s awareness of HIV status to achieving viral suppression, is an important tool to monitor the epidemic globally and is therefore embedded in the Joint United Nations Program on HIV/AIDS (UNAIDS) testing and treatment targets for 20254.
The Netherlands is on track to achieve these targets5. In 2023, an estimated 25,240 individuals were living with HIV in the Netherlands, of whom 23,770 (94%) were ever linked to HIV care, and 22,649 (95%) were retained in care5. 22,557 individuals with HIV were using ART in 2023, of whom 21,753 (96%) had an HIV-1 RNA < 200 copies/mL at their most recent measurement. Despite this achievement, approximately 3,487 individuals with HIV in the Netherlands are estimated to have a detectable HIV-1 viral load due to being undiagnosed, being disengaged from care, not yet having started ART, or having a detectable HIV RNA despite ART.
To continue on the path towards zero new HIV infections, more detailed information is needed as to why certain individuals have suboptimal progression through the HIV care continuum. Most research has focused on exploring health-related indicators that could influence the continuum of care; however, few studies have clarified the role of socio-economic disparities in this cascade6,7,8. Conversely, there is strong reason to believe that HIV, and infectious diseases more broadly, are subject to strong behavioral and social determinants9,10.
To this end, we assessed socio-demographic and economic determinants of not achieving two major milestones of the HIV care continuum, i.e., having a suppressed viral load (HIV-1 RNA < 200 copies/mL) and engagement in HIV care. To do so, we harnessed the increasing availability of full population registries for research and linked our data with full population data from Statistics Netherlands. Registries are unique in that they provide highly detailed information on socio-demographic and socio-economic data, and do so continuously. This provides unique possibilities to guide efforts to reach zero infections for HIV and other infectious diseases.
Results
On 31 December 2023, there were 30,730 individuals with HIV ever registered in the ATHENA cohort. Of them, data from 28,294 (92%) individuals were linked with data from Statistics Netherlands. Individuals who could not be linked were younger (median = 42 vs. median = 52 years] and more often born outside the Netherlands (77.5% vs. 46.0%) compared to those linked to data from Statistics Netherlands (SI Table 1). They were less often men who have sex with men (MSM) (43.3% vs. 59.2%) and less often had an undetectable viral load (84.7% vs. 93.7%) compared to those linked.
Of the 28,294 individuals who could be linked, 572 individuals had migrated or died by 2023 and were thus excluded from analysis. Additionally, we excluded individuals who were <18 years of age (n = 107), had HIV-2 (n = 164), were transgender (n = 331), had not been in care for over 10 years (n = 23), and had no data in 2023 (n = 5,309). In total, 21,788 individuals with HIV were included in the analysis: 13,688 MSM, 3999 cis-gender heterosexual men, and 4121 women. Median age of included individuals was 52 [interquartile range = 42–60] (Table 1). 9152 (41%) and 1780 (8.2%) had a first or second generation migration background, respectively, and 4920 (23.7%) had an income below the poverty line.
Detectable viral load
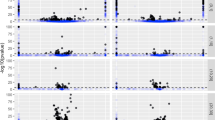
892 MSM, 449 cis-gender heterosexual men, and 442 women had a detectable viral load in 2023. Results from the univariable Heckman probit regression model can be found in SI Table 2 and 3. For all three populations, individuals with a household income below the poverty line or from a low-middle income household had a higher probability of having a detectable viral load in multivariable Heckman regression (Fig. 1A–C). The effect of lower income on viral suppression was more pronounced among MSM and cis-gender heterosexual men (Fig. 1B, C). Having a second-generation migration background (i.e., an individual born in the Netherlands who has at least one parent born abroad) or living in a single-parent, institutionalized, or other type of household was associated with a higher probability of a detectable viral load in only MSM. Having a college or university degree was associated with a lower probability of a detectable viral load in MSM only. Younger age was associated with a higher probability of having a detectable viral load in cisgender heterosexual men and women only.

For MSM, age, education level, migration background, type of household, income, receival of social welfare, year of HIV diagnosis, stage at HIV diagnosis, use of antidepressants, and use of anti-psychotic medication were included in the initial multivariable model. For cisgender heterosexual men, age, education level, migration background, type of household, income, year of HIV diagnosis, and use of antidepressants were included in the initial multivariable model. For women, age, migration background, type of household, and income were included in the initial multivariable model. The grey square indicated the probit coefficient; the lines indicate the corresponding 95% confidence interval. Numbers in each category with the outcome can be found in Supplementary Table 2. All coefficients from the univariable and multivariable Heckman probit regression models can also be found in Supplementary Table 3. CI confidence interval, REF reference category. A Men who have sex with men. B Cis-gender heterosexual men. C Women.
When increasing the threshold for viral suppression to HIV-1 RNA < 1000 copies/mL, 833 MSM, 413 cisgender heterosexual men, and 398 women had a detectable viral load. Increasing the threshold slightly changed the results from the main analysis for MSM and cis-gender heterosexual men. For MSM, age and use of antidepressants were no longer associated with an increased probability of a detectable viral load in MSM (SI Table 4). For cis-gender heterosexual men, having only primary education and no migration background were associated with increased probability of a detectable viral load.
Disengagement from care
333 MSM, 215 cis-gender heterosexual men, and 157 women disengaged from care before 31 December 2023. A lower income was associated with disengagement from care only in MSM and cisgender heterosexual men (Table 2, SI Table 5). For women, being diagnosed in or after 2015 decreased the probability of disengagement from care. We found no association between age and disengagement from care for all three populations.
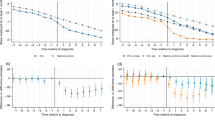
In the sensitivity analysis assessing the time to disengagement from care among individuals diagnosed with HIV after 2012, the piecewise exponential survival model identified a broader set of significant exposures associated with disengagement from care (SI Table 6). For all three populations, increased years since HIV diagnosis, younger age, and a low-middle income or income below the poverty line were associated with a higher rate of disengagement from care. For MSM and cisgender heterosexual men, only having a primary education, a first or second generation migration background, or being a single parent or living institutionalized or in another type of household were associated with a higher rate of disengagement from care. For MSM, receiving social welfare and using antidepressants were associated with a lower rate of disengagement from care.
Discussion
Efforts to minimize the number of new HIV infections have historically been guided by health-related determinants. This has led to great strides in reaching the UNAIDS targets in the Netherlands. However, closing the final gap to no new infections will require appreciating and understanding the social and behavioral dimensions of infectious diseases. In the past, these types of determinants were difficult to study due to a lack of data availability, but the emergence of full population registries has changed this. To illustrate, we identified that even though the HIV care continuum in the Netherlands almost reaches the UNAIDS targets nationally5, these targets are clearly not being met among younger individuals and individuals with lower incomes. Furthermore, these at-risk individuals seem to experience additional difficulties in remaining engaged in care. These findings highlight that the HIV care continuum is heavily influenced by specific socio-economic, rather than solely health-related, determinants. Efforts to optimize HIV care, through specialized interventions, should consider individual economic vulnerability to improve HIV care outcomes.
Notwithstanding mandated health insurance, which is the case in the Netherlands, lower socio-economic status still negatively impacted viral suppression and retention in care. Similar effects have been observed in other settings, such as the United States of America and the United Kingdom6,7,8. Importantly, the association between socio-economic status and viral suppression was found to be significant across all populations. Women, particularly those with a lower socio-economic status, may face specific challenges to HIV care and treatment adherence, such as caregiving responsibilities, intimate partner violence, lack of social support, and financial dependence7,11. Moreover, HIV-related stigma may influence prioritization of HIV care and treatment adherence12. Cis-gender heterosexual men have been historically less engaged in HIV care than MSM in the Netherlands5, which may be due to e.g. HIV-related stigma or the fact that most HIV programs might not be tailored to heterosexual cis-gender men.
We found that younger age was inversely associated with detectable viral load for cisgender heterosexual men and women, consistent with previous studies13. Younger individuals with HIV may face their own unique barriers to HIV care, such as lower knowledge or awareness of HIV and greater stigma14. Surprisingly, we also found that MSM with a second-generation migration background more often had a detectable viral load, but migration background had no effect on retention in HIV care. In the Netherlands, many individuals with a first migration background were already diagnosed with HIV in their country of origin and had commenced ART before their arrival in the Netherlands, possibly explaining why these individuals were not at increased risk of an unsuppressed viral load5. Why MSM with a second-generation migration background specifically are at increased risk of an unsuppressed viral load, despite being born in the Netherlands, remains to be studied. It is however, likely that migration background intersects with barriers related to socio-economic status, and that community- or culture-related stigma or self-stigma may play an important role15.
Interventions providing financial or structural support to people vulnerable to disengagement from care and suboptimal treatment due to financial constraints could be considered. Microfinance interventions have, for instance, been associated with improved adherence to ART and treatment outcomes in mostly low-middle income settings16,17,18, but are currently not available in the Netherlands. Peer support has also been effective in helping people obtain access to care and adhere to medication19,20, and when implemented as an e-health intervention, could offer support to individuals who prefer digital interventions21. Long-acting ART options, administered over longer periods of time or through health care providers closer to the individual, may also offer alternatives for those struggling to refill prescriptions or attend HIV care visits22,23,24.
A major strength of our study is the use of a comprehensive prospective cohort consisting of over 97% of all individuals receiving HIV care in the Netherlands. This provides a unique surveillance tool for the HIV epidemic in the Netherlands. Nevertheless, this study is not without limitations. First, 8% of the population with HIV could not be combined with data from Statistics Netherlands. Individuals who could not be combined were younger and more often born outside the Netherlands. They were also less often MSM and more often had a detectable viral load. As people are only represented in Statistics Netherlands if they have a postal code by the end of the calendar year, this may mean that the individuals who could not be combined represent a group of people with more intersecting vulnerabilities (e.g., undocumented migrants or homeless individuals). Second, we had no data on reasons for low income or actual mental health disorders, so the underlying issues cannot be examined further than what the data allows. Third, we cannot regroup individuals to specific key subpopulations (e.g., MSM who inject drugs), hence these results only represent the overall key populations and may not be generalizable to specific subpopulations. Furthermore, these groupings could conflate gender identity, sexual orientation, and sexual behavior. Future research could incorporate more inclusive and nuanced measures of gender identity and sexuality to more specifically reflect the experiences of all individuals. Fourth, our main analysis used cross-sectional data from 2023. If, for example, there were declines in income or changes in employment status after HIV diagnosis, which then contributed to an increased risk of disengagement from care, the temporality of exposure on outcome would be unclear in a cross-sectional analysis. In a sensitivity analysis using longitudinal data on time from HIV diagnosis to disengagement from care and time-updated variables, a broader set of determinants was identified, but these associations (particularly the key associations age and income) were consistent among MSM and cisgender heterosexual men. Notably, income was not associated with disengagement from care among women in the cross-sectional analysis, but it was in the longitudinal analysis. Fifth, there could have been insufficient statistical power to identify determinants in some subgroups, namely, women.
In conclusion, these results not only quantify but emphasize the role of socio-economic status in HIV care progression and engagement, and suggest a need for specialized interventions to reduce these barriers to care, such as peer- or community-led support systems. Efforts to optimize HIV care should consider economic vulnerability to improve outcomes. More broadly, our findings illustrate the value of full population registry data in identifying gaps in care and guiding efforts to minimize the spread of infectious diseases.
Methods
Study design and data sources
We conducted a secondary analysis leveraging individual data from the ATHENA cohort and non-public microdata from Statistics Netherlands.
Briefly, HIV care in the Netherlands is provided by 23 designated treatment centres. The HIV Monitoring Foundation [Stichting hiv monitoring (SHM)] is tasked by the Dutch Ministry of Healthcare, Welfare and Sports to monitor and report on all aspects of HIV care for people with HIV in the Netherlands. Data collection was initiated in 1998, and data are prospectively collected in the ATHENA (AIDS Therapy Evaluation in the Netherlands) cohort, which represents over 97% of all people with HIV in care in the Netherlands5,25.
People entering HIV care receive written material about participation in the ATHENA cohort, after which they are asked to consent verbally to the use of their routinely collected medical data for research and monitoring (i.e., an “opt-in” procedure). Participants can withdraw their consent at any time. Data collection was approved by the boards of all participating centers. Only routinely collected data were used for this analysis, and therefore, no additional review or consent was required.
Statistics Netherlands (Centraal Bureau voor de Statistiek, CBS) is an independent organization that collects, processes, and publishes reliable statistical data on residents of the Netherlands. The Statistics Netherlands Act constitutes the legal basis for Statistics Netherlands, and Statistics Netherlands is adherent to the European Union’s General Data Protection Regulation.
Data from the ATHENA cohort were uploaded to the secure Remote Access environment hosted by Statistics Netherlands. Data linkage between data from ATHENA and microdata from Statistics Netherlands was facilitated by Statistics Netherlands using a probabilistic approach based on individual's date of birth, the first four digits of the postal code of the last known residence, and sex at birth. Statistics Netherlands performed exact matching. Any linkage error would be the result of measurement error (e.g., mis-registered data in one of the data registries) or the inability to perform exact matching (e.g., two people with the exact same date of birth and sex registered at a single postal code). Any data with a linkage error was discarded.
Participants from the ATHENA cohort provided consent for use of their data for data linkage purposes, and information about active data linkages is available on the SHM website. The Remote Access environment is only available for researchers authorized by SHM and Statistics Netherlands. All output from the Remote Access environment is independently verified by Statistics Netherlands to ensure data cannot be traced back to individuals. The combined dataset was used in accordance with Dutch Statistics Netherlands (CBS) law, which permits secure data linkage for scientific research26.
Study population
We selected all individuals aged 18 years or older in the ATHENA cohort who had been registered with SHM and were still in care in 2023. We included all those who belonged to key populations with sufficient numbers of individuals for which the risk of identification was minimal (i.e., n ≥ 10). This criterion resulted in the inclusion of men who have sex with men (MSM), other men, and women, while those who were transgender could not be included. Individuals who were diagnosed with HIV-2, migrated outside of the Netherlands, or were deceased before 31 December 2023 were also excluded from analysis.
Study variables
At enrollment into the ATHENA cohort, the following demographic information was collected: year of birth, country of birth, sex assigned at birth, gender identity (if different from sex at birth), and most likely transmission route of HIV. Information about the date of HIV diagnosis was retrieved from the referral letter provided by the general practitioner or Centre for Sexual Health, from health records in the HIV treatment center, or self-reported if no documentation was available.
Statistics Netherlands provided detailed individual-based socio-demographic and socio-economic information, including education level, migration background, employment status, household composition, household income, and use of social welfare (SI A). Household income was defined according to the social minimum (the minimal amount of financial resources required to achieve a minimally acceptable lifestyle). The social minimum is determined and adjusted bi-annually by the Ministry of Social Affairs and Employment27. An individual’s income was categorized as below the poverty line if their household income was <120% of the social minimum (which determines if an individual gets benefits in the Netherlands), as middle income is the household income was between 120–299% of the social minimum, and as high in the household income was ≥300% of the social minimum. Additionally, information on health expenditure paid through the universal health insurance program in the Netherlands was obtained. All health expenditures are assigned a Diagnostic-Treatment-Classification (DTC), which reflects a diagnosis or treatment. Data on care related to the Long-term Care Act (defined as declared costs >0€ associated with this Act)28, mental health care (defined as declared costs >0€ for basic or specialized mental health care), use of antipsychotics (ATC code N05A), and use of antidepressants (ATC code N06A) were also included. The Long-term Care Act involves care with stay and care at home, elderly care, psychiatric care, care during chronic illness, and care for individuals with a disability.
For data from Statistics Netherlands, we used socio-demographic, socio-economic, and health-related information from the most recent data as registered by the end of the previous calendar year (i.e., 31 December 2022).
Statistical analysis
We described socio-demographic, socio-economic, and health-related determinants for all individuals with HIV registered in 2023. To minimize the risk of personal data inadvertently leading to the identification of an individual, data involving fewer than ten people was not reported.
We assessed socio-demographic, -economic, and health-related determinants of not achieving two major milestones of the HIV care continuum, i.e., suppressed viral load (HIV-1 RNA < 200 copies/mL) and engagement in care (at least one HIV care visit in 2023), using multivariable Heckman probit regression. This model jointly estimates the probability of being successfully linked to the registry data from Statistics Netherlands (in a “selection” equation) and the outcomes (in an “outcome” equation), and hence reduces selection bias from individuals who were not linked to data from Statistics Netherlands. Age, being born in the Netherlands, and the level of urbanization of residence were included in the selection equation. We added individual covariates to the outcome equation to obtain univariable coefficients and 95% confidence intervals (CI) comparing the probability of having the outcome across levels of covariates. Missing values were included in the models as a separate category. Determinants with p < 0.2 in univariable analysis were included in a full multivariable model. Variables that did not significantly improve the model fit based on the likelihood ratio test (p > 0.05) were removed sequentially from the model in a backwards, stepwise fashion. Age was included a priori in both the selection and outcome equations in the multivariable model. We stratified analyses by key population based on sex assigned at birth and probable mode of HIV acquisition, as the epidemiology, prevention, and care of HIV has been known to differ between these key populations5. Specifically, we categorized individuals as men who have sex with men (MSM, assigned male at birth, not transgender, and likely acquired HIV through sex with another man), cisgender women (assigned woman at birth, not transgender), or heterosexual cisgender men (assigned male at birth, not transgender, acquired HIV through sex with a woman).
To assess the robustness of our results, we conducted two sensitivity analyses. In the first sensitivity analysis, we increased the threshold of viral suppression to HIV-1 RNA < 1000 copies/mL29. In the second sensitivity analysis, we modeled the time from HIV diagnosis to disengagement from care with time-updated covariates. The hazard ratio (HR) comparing the hazards across levels of determinants was obtained along with its 95% CI using a piecewise exponential survival model. Due to data availability, only individuals diagnosed with HIV after 2012 could be included in this analysis.
The results presented are based on calculations carried out by Stichting HIV Monitoring (SHM) in project number 8944 using non-public microdata from Statistics Netherlands (CBS) and Vektis C.V. Analyses were carried out using STATA (v16.0, StataCorp, College Station, TX, USA).
Reporting summary
Further information on research design is available in the Nature Portfolio Reporting Summary linked to this article.
Data availability
All results presented here are calculated from non-public registry data from Centraal Bureau voor de Statistiek (CBS), accessed through the Remote Access environment. CBS was not involved in the calculation of any of the results presented. While the data are not publicly available, academic institutions can apply for access to the Remote Access environment through the CBS (for additional information, see https://www.cbs.nl/en-gb/our-services/customised-services-microdata/microdata-conducting-your-own-research. ATHENA cohort data (without CBS data) used in this study are available upon request. Requests for data access can be made to: hiv.monitoring@amsterdamumc.nl. Requests will be reviewed on a case-by-case basis based on scientific value and overlap with existing projects. Statistical information or data for separate research purposes from the ATHENA cohort can be requested by submitting a research proposal to SHM (https://www.hiv-monitoring.nl/english/research/research-projects/). The proposal will undergo review by representatives of SHM for evaluation of scientific value, relevance of the study, design, and feasibility, statistical power, and overlap with existing projects.
Code availability
All code underlying our analyses are available from: https://github.com/vitajongen/HIVcarecontinuum_NatureCommunications.git.
References
Cohen, M. S. et al. Antiretroviral Therapy for the Prevention of HIV-1 Transmission. N. Engl. J. Med. 375, 830–839 (2016).
Rodger, A. J. et al. Risk of HIV transmission through condomless sex in serodifferent gay couples with the HIV-positive partner taking suppressive antiretroviral therapy (PARTNER): final results of a multicentre, prospective, observational study. Lancet 393, 2428–2438 (2019).
Bavinton, B. R. et al. Viral suppression and HIV transmission in serodiscordant male couples: an international, prospective, observational, cohort study. Lancet HIV 5, e438–e447 (2018).
UNAIDS. 2025 AIDS Targets, <https://www.unaids.org/en/topics/2025_target_setting>
van Sighem A. I. et al. Monitoring Report 2024. Human Immunodeficiency Virus (HIV) Infection in the Netherlands., (https://www.hiv-monitoring.nl/nl/resources/monitoring-report-2024, 2024).
Menza, T. W., Hixson, L. K., Lipira, L. & Drach, L. Social Determinants of Health and Care Outcomes Among People With HIV in the United States. Open Forum Infect. Dis. 8, https://doi.org/10.1093/ofid/ofab330 (2021).
Ojukwu, E., Cianelli, R., Villegas Rodriguez, N., De Oliveira, G. & Kalu, V. A qualitative study on the social determinants of hiv treatment engagement among black older women living with HIV in the Southeastern United States. J. Assoc. Nurses AIDS Care 33, 211–223 (2022).
Burch, L. S. et al. Socioeconomic status and treatment outcomes for individuals with HIV on antiretroviral treatment in the UK: cross-sectional and longitudinal analyses. Lancet Public Health 1, e26–e36 (2016).
Frey, A., Tilstra, A. M. & Verhagen, M. D. Inequalities in healthcare use during the COVID-19 pandemic. Nat. Commun. 15, 1894 (2024).
Buckee, C., Noor, A. & Sattenspiel, L. Thinking clearly about social aspects of infectious disease transmission. Nature 595, 205–213 (2021).
Mukerji, R., Osrin, D. & Mannell, J. Mixed studies review of domestic violence in the lives of women affected by HIV stigma. AIDS Care 35, 678–695 (2023).
Nawfal, E. S., Gray, A., Sheehan, D. M., Ibañez, G. E. & Trepka, M. J. A systematic review of the impact of HIV-related stigma and serostatus disclosure on retention in care and antiretroviral therapy adherence among women with HIV in the United States/Canada. AIDS Patient Care STDs 38, 23–49 (2024).
Anderson, A. N. et al. Disparities in retention in care among adults living with HIV/AIDS: A systematic review. AIDS Behav. 24, 985–997 (2020).
Chem, E. D., Ferry, A., Seeley, J., Weiss, H. A. & Simms, V. Health-related needs reported by adolescents living with HIV and receiving antiretroviral therapy in sub-Saharan Africa: a systematic literature review. J. Int. AIDS Soc. 25, e25921 (2022).
Nöstlinger, C. et al. HIV among migrants in precarious circumstances in the EU and European Economic Area. Lancet HIV 9, e428–e437 (2022).
Bosma, C. B. et al. Effects of economic interventions on pediatric and adolescent HIV care outcomes: a systematic review. AIDS Care 36, 1–16 (2024).
Nadkarni, S., Genberg, B. & Galarraga, O. Microfinance interventions and HIV treatment outcomes: a synthesizing conceptual framework and systematic review. AIDS Behav. 23, 2238–2252 (2019).
Silva, A. F. et al. Income determines the impact of cash transfers on HIV/AIDS: cohort study of 22.7 million Brazilians. Nat. Commun. 15, 1307 (2024).
Berg, R. C., Page, S. & Øgård-Repål, A. The effectiveness of peer-support for people living with HIV: A systematic review and meta-analysis. PLOS ONE 16, e0252623 (2021).
Ayala, G. et al. Peer- and community-led responses to HIV: A scoping review. PLOS ONE 16, e0260555 (2021).
Dos Santos, F. C. et al. The effect of a combined mHealth and community health worker intervention on HIV self-management. J. Am. Med. Inform. Assoc. 32, 510–517 (2025).
Gutner, C. A. et al. Patient participant perspectives on implementation of long-acting Cabotegravir and Rilpivirine: results from the Cabotegravir and Rilpivirine Implementation Study in European Locations (CARISEL) Study. J. Int Assoc. Provid AIDS Care 23, 23259582241269837 (2024).
Kerrigan, D. et al. Experiences with long acting injectable ART: A qualitative study among PLHIV participating in a Phase II study of cabotegravir + rilpivirine (LATTE-2) in the United States and Spain. PLOS ONE 13, e0190487 (2018).
Jongen, V. W. et al. Effectiveness of bi-monthly long-acting injectable cabotegravir and rilpivirine as maintenance treatment for HIV-1 in the Netherlands: results from the Dutch ATHENA national observational cohort. Lancet HIV 12, e40–e50 (2025).
Boender, T. S. et al. AIDS Therapy Evaluation in the Netherlands (ATHENA) national observational HIV cohort: cohort profile. BMJ Open 8, e022516 (2018).
Wet op het Centraal bureau voor de statistiek, https://wetten.overheid.nl/BWBR0015926/2022-03-02/#Hoofdstuk5_Paragraaf1_Artikel33.
Uitvoeringsinstituut Werknemersverzekeringen (UWV). Sociaal Minimum, https://www.uwv.nl/nl/toeslag/sociaal-minimum (2024).
Overheid.nl. Wet langdurige zorg, https://wetten.overheid.nl/BWBR0035917/2025-01-01.
Broyles, L. N., Luo, R., Boeras, D. & Vojnov, L. The risk of sexual transmission of HIV in individuals with low-level HIV viraemia: a systematic review. Lancet 402, 464–471 (2023).
Acknowledgements
The ATHENA Cohort (SI B) is managed by Stichting hiv monitoring and supported by a grant from the Dutch Ministry of Health, Welfare, and Sport through the Centre for Infectious Disease Control of the National Institute for Public Health and the Environment. The collaboration project [LSHM23014-SGF] is co-funded by the PPP Allowance made available by Health~Holland, Top Sector Life Sciences & Health, to stimulate public-private partnerships. We further acknowledge funding from the Amsterdam Diner Foundation.
Author information
Authors and Affiliations
Contributions
V.J., A.B and Mvd.V conceptualized and designed this study. V.J., Av.S, and A.B. were involved in the data management and analysis. V.J, A.B, T.A., N.S., M.V., Rv.Z., Mvd.B., C.N., V.C.H., W.B., Av.S., and Mvd.V. were involved with the interpretation of the data. V.J. drafted the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
AB received speaker’s fees from Gilead Sciences. MvdV received unrestricted research grants and fees for participation in advisory boards from Gilead Sciences, MSD and ViiV, all paid to his institution. AvS received grants, paid to his institution, from the European Centre for Disease Prevention and Control (ECDC). All other authors declare no competing interest.
Peer review
Peer review information
Nature Communications thanks the anonymous reviewer(s) for their contribution to the peer review of this work. A peer review file is available.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Jongen, V.W., Boyd, A., Albers, T. et al. Harnessing registry data to identify socio-demographic and socio-economic gaps in HIV care in the Netherlands. Nat Commun 16, 10517 (2025). https://doi.org/10.1038/s41467-025-65512-6
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41467-025-65512-6
