
Abstract
Pregnancy-related cardiovascular complications cause substantial morbidity and account for a large proportion of maternal deaths. The relationship between maternal age and pregnancy-related cardiovascular complications remains unclear. Most prior studies categorized patients using an age threshold, and previous studies did not delineate patients’ baseline cardiovascular risk versus pregnancy-specific risk. Here we show that pregnancy and the postpartum period are associated with a 7-fold higher risk of major adverse cardiovascular events compared to patients’ baseline risk. This relative risk increase does not vary with maternal age. Absolute risk increases are stable at approximately 3 excess events per 1000 pregnancies until 31 years of age, then steadily increase, reaching 10 excess events per 1000 pregnancies by 44 years of age. These findings suggest that aging does not drive pregnancy-specific mechanisms of cardiovascular events. Rather, our findings suggest that pregnancy uniformly amplifies existing cardiovascular risk, resulting in increasing complications as patients accrue more baseline risk with age.
Similar content being viewed by others


Introduction
Pregnancy-related cardiovascular complications account for approximately 20–30% of maternal deaths based on U.S. and global data from the past decade1,2. Aging increases the risk of major adverse cardiovascular events in the general population, and previous studies have established advanced maternal age, variously defined as greater than 35, 40, or 45 years, as a risk factor for general adverse pregnancy outcomes3. The nature of the relationship between maternal age and pregnancy-related cardiovascular complications remains unclear. Most prior studies have dichotomized patients using an age threshold, leaving it unclear whether the association between age and pregnancy-associated cardiovascular complications is linear or exponential or follows some other form4,5,6,7,8,9,10,11. Previous studies did not delineate patients’ baseline risk of cardiovascular events versus pregnancy-specific risk, so it remains unclear whether aging increases the specific cardiovascular risk from pregnancy itself or whether older patients simply have higher baseline cardiovascular risk4,5,6,7,8,9,10,11. Addressing these knowledge gaps may be helpful given the trend toward older maternal age in developed countries12 and the implications for managing high-risk pregnancies and identifying complications. Here, we show that pregnancy and the postpartum period are associated with a 7-fold higher risk of major adverse cardiovascular events compared to patients’ baseline risk. This relative risk increase does not vary with maternal age. Absolute risk increases are stable at approximately 3 excess events per 1000 pregnancies until 31 years of age, then steadily increase, reaching 10 excess events per 1000 pregnancies by 44 years of age. These findings suggest that aging does not drive pregnancy-specific mechanisms of cardiovascular events. Rather, pregnancy uniformly amplifies existing cardiovascular risk, resulting in an increase in complications as patients accrue more baseline risk with age.
Results
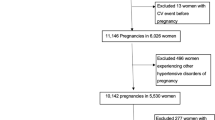
We identified 2,710,983 patients with a first-recorded pregnancy (Fig. 1), of whom 13,744 had a major adverse cardiovascular event during the pregnancy/postpartum period or during the equivalent control period 1 year later. Patients with cardiovascular events were slightly older (mean age, 30.9 ± 6.2 years versus 29.3 ± 5.8 years), more likely to have pre-existing comorbidities such as hypertension, more likely to be Black, and less likely to be privately insured or in the upper half of the household income distribution (Table 1).
Of the 13,744 patients with a major adverse cardiovascular event, 12,059 had an event during pregnancy or the postpartum period (4.45 [95% CI, 4.37–4.53] events per 1000 patients), whereas 1685 had an event during the equivalent control period 1 year later (0.62 [95% CI, 0.59–0.65] events per 1000 patients). Overall, the pregnancy/postpartum period was associated with a substantially higher relative risk of major adverse cardiovascular events compared with the control period (risk ratio, 7.2; 95% CI, 6.9–7.4) (Fig. 1). This relative risk increase did not vary with maternal age (P value for multiplicative interaction, 0.43) (Fig. 2). Absolute risk increases were broadly stable at approximately 3 excess events per 1000 pregnancies until 31 years of age, then steadily increased and reached 10 excess events per 1000 pregnancies by 44 years of age (Table 2, Fig. 3).

This figure demonstrates how the relative risk of major adverse cardiovascular events associated with pregnancy varies for different event types. Source data are provided as a Source Data file. The error bars represent the 95% confidence interval.

This figure demonstrates how the relative risk of major adverse cardiovascular events associated with pregnancy varies across maternal age. Source data are provided as a Source Data file. The error bars represent the 95% confidence interval. The diagonal parallel lines represent error bars that have been truncated for readability.

This figure demonstrates how the relative risk of major adverse cardiovascular events associated with pregnancy varies across maternal age. Source data are provided as a Source Data file. The error bars represent the 95% confidence interval.
The relationship between maternal age and cardiovascular risk was similar for arterial, venous, and other events (Table 2, Figs. S2–S4 in the supplementary appendix); during the antepartum/intrapartum, early postpartum, and late postpartum periods (Figs. S5–S7); and across subgroups defined by race and ethnicity, insurance type, household income, region, and comorbidities (Figs. S8–S17). Our findings were unchanged in sensitivity analyses extending the risk period from 9 months antepartum through 12 months postpartum (Fig. 18), including all pregnancies (Fig. 19), including patients with major adverse cardiovascular events prior to pregnancy (Fig. 20), accounting for potential effects of the COVID-19 pandemic (Fig. 21), counting cardiovascular events during both the pregnancy/postpartum period and during the control period (Fig. 22), comparing the risk of cardiovascular events during pregnancy versus the same time period 12 months before pregnancy (Fig. 23), or comparing pregnant versus non-pregnant women (Fig. 24).
The most common major adverse cardiovascular events were venous thromboembolism, cardiomyopathy, and heart failure (Table 3). Of the 13,744 patients with a major adverse cardiovascular event, 240 (1.7%; 95% CI, 1.5–2.0%) died, representing 49.4% (95% CI, 44.9–53.9%) of all maternal deaths in our study population. Among survivors of a major adverse cardiovascular event, 9.6% (95% CI, 9.1–10.1%) were discharged to a rehabilitation or nursing facility or required home health care.
Discussion
In a large, population-based cohort-crossover study, we found that pregnancy was associated with a 7-fold higher relative risk of major adverse cardiovascular events, resulting in approximately 4 excess events per 1000 pregnancies. The relative risk of cardiovascular events associated with pregnancy did not vary with maternal age. Absolute risk differences approximately doubled at higher maternal ages, starting to increase after age 31 years and exceeding 1% by age 44 years. Cardiovascular events accounted for half of all maternal deaths and approximately 10% of survivors required further institutional or home health care after their acute hospitalization.
Prior studies have established advanced maternal age as a risk factor for general adverse pregnancy outcomes including both fetal and maternal conditions such as preterm labor, low birth weight, and pre-eclampsia4,5,6,7,8,9,10,11. The limited existing data on maternal age as a continuous variable indicate varying patterns of association—linear, curvilinear, or U-shaped—for varying endpoints3. Given the relative rarity of major pregnancy-related cardiovascular events, sparse and conflicting data exist on the risk of such complications across the range of maternal age. Furthermore, prior studies have generally compared pregnant patients to an independent group of non-pregnant patients or compared older pregnant patients to younger pregnant patients13,14, potentially introducing residual confounding and making it difficult to disentangle baseline risk from pregnancy-specific risk. In this context, our study found that the relative risk of pregnancy-related cardiovascular complications did not increase with maternal age, suggesting that aging does not substantially drive pregnancy-specific mechanisms of cardiovascular events. Rather, it appears that pregnancy uniformly heightens patients’ baseline risk, resulting in more cardiovascular complications in older patients who have higher cardiovascular risk to begin with than younger patients.
Absolute risk increases were particularly notable—reaching 20 excess events per 1000 pregnancies by age 45 years—for the subgroup of patients with comorbidities, the most common of which were hypertension and asthma. The over-representation of patients with asthma among those with major adverse cardiovascular events is striking, and suggests a need for further research on why patients with asthma may be at heightened risk of pregnancy-associated cardiovascular complications. Black patients were disproportionately represented among those with major adverse cardiovascular events, but there was no interaction between pregnancy and maternal age in analyses stratified by race, suggesting that differences in aging-related cardiovascular susceptibility does not explain the racial disparities seen in our data. These disparities likely reflect structural and systemic factors, including differences in access to care and underlying social determinants of health. Further research using more granular data will be required to better understand and design interventions to address Black patients’ over-representation among those with cardiovascular complications of pregnancy.
Our study has several limitations. First, we relied on diagnosis codes to ascertain events, which may have led to misclassification. However, hospital discharge diagnosis codes for major adverse cardiovascular events have previously been shown to be reliable when compared to gold-standard medical record review15,16,17, and the event rates we found during the control period align closely with the reported background incidence of major adverse cardiovascular events in similarly aged patients in prospective cohort and registry studies18,19. Second, we lacked data on medications, particularly regarding aspirin which is often used to prevent pre-eclampsia in high-risk patients such as those with a first pregnancy at 35 years of age or older20. However, we found similar patterns of risk for all phases of pregnancy, including the late postpartum period which would not be affected by aspirin since it is stopped at delivery when used for the prevention of pre-eclampsia20. Third, we were unable to capture events at federal acute care hospitals or at hospitals in neighboring states. This would be expected to involve a very small proportion of events. Fourth, we only had data from a sample of U.S. states. However, these heterogeneous states comprise approximately 80 million people and 25% of the U.S. population, and our results were similar in subgroup analyses stratified by region, providing further confidence that our findings are generalizable to other broadly similar countries and healthcare systems. Lastly, there were relatively fewer patients in older age groups, resulting in less precision, which should be kept in mind when interpreting our results.
Our findings may have several implications. First, our estimates of steadily rising absolute risks starting after the age of 31 years may inform strategies for more closely monitoring high-risk pregnancies to improve maternal outcomes, particularly given that current practices for designating advanced maternal age are associated with better perinatal outcomes but not a reduction in severe maternal morbidity21. The absolute risks in those older than 31 years of age, particularly in those with pre-existing comorbidities, may justify additional screening, close follow-up, and optimization of cardiovascular risk factors throughout pregnancy. Second, our finding of a uniform relative risk increase associated with pregnancy throughout the maternal age span highlights the importance of patients’ baseline, pre-pregnancy health status in determining the risk of pregnancy-related cardiovascular complications, indicating a need for multidisciplinary clinical and public health efforts to ensure that patients’ cardiovascular health is optimized before pregnancy. Lastly, clinicians who care for patients presenting with possible cardiovascular events during pregnancy or the postpartum period should recognize that such complications, while somewhat more common in older patients, are not uncommon even in young patients, affecting approximately 1 in 250 pregnancies and resulting in substantial morbidity and mortality.
Methods
The Weill Cornell Medicine Institutional Review Board certified our analysis of these publicly available, deidentified data as exempt from review and waived the requirement for informed consent. We received and analyzed only completely anonymized data for this study.
Design
We performed a cohort-crossover study using comprehensive all-payer claims data on hospitalizations across 11 U.S. states during 2016-2021. We compared each patient’s likelihood of a major adverse cardiovascular event during pregnancy or the postpartum period with the likelihood of such an event during an equivalent nonpregnant control period. Since exposure to pregnancy varies transiently over time, this design allowed patients to serve as their own controls during a nonpregnant time period that reflected their baseline risk, reducing unmeasured confounding from fixed factors22. Given that cardiovascular risk rises during the second trimester23 and lasts through the 3-month postpartum period, we defined the risk period for pregnancy-related cardiovascular events as 6 months before through 3 months after labor and delivery24, as done in previously published papers24,25. The control period was the equivalent of a 9-month period 1 year later. In a sensitivity analysis designed to reflect a commonly used period for tracking and reporting maternal outcomes1, we extended the risk period from 9 months before through 12 months after labor and delivery, and compared it to the equivalent 21-month period 2 years later. The 11 states included in this analysis were chosen because they provide comprehensive hospital discharge data with unique anonymous patient identifiers linking multiple hospitalizations over time26. These geographically dispersed states—AR, FL, GA, IA, MA, MD, NE, NY, VT, WI, and UT—have a combined population of approximately 80 million residents, comprising 25% of the U.S. population27. Trained analysts at all nonfederal acute care facilities in these states use automated online reporting software to provide standardized data on all hospitalizations to their respective state health department, which then performs a multistep quality assurance check to identify invalid or inconsistent records before making the data publicly available via the Healthcare Cost and Utilization Project26. We followed the terms of our data use agreement with the Healthcare Cost and Utilization Project and the Reporting of Studies Conducted Using Observational Routinely-Collected Data guidelines28.
Patients
We used standard International Classification of Disease, 10th Edition (ICD-10) codes to identify hospitalizations for labor and delivery. We included female patients 12 through 55 years of age at the time of delivery, based on the infrequency of births outside this population (<0.01% of all births)12. Sex was determined from a sex variable in the administrative source data. Our sex classification was based on administrative data and our sample included only individuals recorded as female in the administrative source data. Our use of terminology such as ‘maternal’ and ‘pregnant women’ reflects this classification. For patients with multiple labor-related hospitalizations during a single 40-week period, we excluded cases of false labor by identifying delivery as the latest hospitalization during that time. Since patients with a cardiovascular event may be less likely to subsequently become pregnant, we included only the first pregnancy captured in our data for each patient; in a sensitivity analysis, we included all pregnancies. To focus on incident outcomes, we excluded patients who had any major adverse cardiovascular events diagnosed before their first recorded pregnancy; in a sensitivity analysis, we included those patients. To compare the risk of cardiovascular events during pregnancy with the risk during nonpregnant periods, we excluded patients with a subsequent delivery during the control period, 1 year after the first pregnancy. The start date of 2016 reflected the earliest available data and allowed for the transition to ICD-10 codes in late 2015, and the latest data were available through 2021. To accommodate analyses of the 180 days before delivery through the end of the control period 3 months plus 1 year after delivery, we included patients with a hospitalization for a delivery from July 1, 2016 through September 30, 2020. Data from GA, MA, and UT were only available through 2020, so our cut-off date for labor and delivery in those states was September 30, 2019. In a sensitivity analysis to assess potential effects from the COVID-19 pandemic, we excluded patients whose control period ended after December 31, 2019. Cut-off dates were adjusted as necessary in all secondary and sensitivity analyses that used risk periods different from those in our primary analysis.
Measurements
Our primary outcome was a composite of major adverse cardiovascular events, defined as hospitalization for heart failure, cardiomyopathy, myocardial infarction, stroke, systemic embolism, venous thromboembolism, arterial dissection, aortic dissection or rupture, or cardiac arrest. This outcome included both fatal and non-fatal events and was chosen to represent both the major adverse cardiovascular events traditionally used in epidemiological studies and clinical trials as well as additional highly morbid events that have previously been associated with pregnancy. We used the Clinical Classification System from the Healthcare Cost and Utilization Project26 to identify and categorize specific ICD-10 codes for these major adverse cardiovascular events (see Table S1 in the supplementary appendix for a list of ICD-10 codes). In secondary analyses, we separately examined the following categories of outcomes: (a) arterial events, (b) venous events, and (c) other cardiovascular events (see Table S2 in the supplementary appendix for specific events included within each category). In further secondary analyses, we separately examined outcomes occurring during the antepartum/intrapartum period, defined as 6 months before labor and delivery through the duration of the labor and delivery hospitalization, the early postpartum period, defined as after discharge from the labor and delivery hospitalization through 6 weeks after labor and delivery, and the late postpartum period, defined as 6 through 12 weeks after labor and delivery; all periods were compared with their equivalent periods 1 year later.
We analyzed age, race and ethnicity, insurance type, estimated household income, hospital discharge disposition, and mortality using standardized variables provided by the Healthcare Cost and Utilization Project. Race and ethnicity were categorized as white, Black, Hispanic, Asian or Pacific Islander, Native American, Other, or missing. Race and ethnicity were recorded using standardized categories provided in the source data; the category of “Other” race was not further specified in the source data. Insurance type was categorized in the source data as Medicare, Medicaid, private insurance, self-pay, no charge, other, or missing. The estimated median household income of residents in each patient’s ZIP code was categorized in the source data by quartiles. States were assigned in the source data to the following geographic regions: Midwest (IA, NE, WI), Northeast (MA, NY, VT), South (AR, FL, GA, MD), or West (UT). We used ICD-10 codes, the Clinical Classification System, and the Charlson comorbidity index to ascertain comorbidities documented at the time of labor and delivery29.
Statistical analysis
For each patient, we compared the likelihood of an outcome during pregnancy or the postpartum period versus the equivalent period 1 year later. To focus on incident events, we counted only the first documented outcome for each patient, meaning that a patient could have only one outcome, occurring either during the pregnancy/postpartum period or during the control period. In a sensitivity analysis, we counted all events, meaning that a patient could have outcomes occurring during both the pregnancy/postpartum period and during the control period. In a separate sensitivity analysis, we compared the risk of cardiovascular events during pregnancy versus the same time period 12 months before pregnancy.
For each year of maternal age at delivery, we used McNemar’s chi-squared test for matched data to estimate the risk ratio and absolute risk difference for the pregnancy/postpartum period versus the control period, with 95% confidence intervals. We used conditional logistic regression to test the multiplicative interaction between maternal age (continuous) and pregnancy on vascular events, while simultaneously adjusting for interactions between pregnancy and each of the following factors: race, insurance, income, state, and comorbidity burden. In the sensitivity analysis that including all pregnancies for each patient, we used robust standard errors to account for clustering of multiple pregnancies within individual patients. For secondary outcomes, some of which were relatively uncommon, we tabulated rates across grouped age categories. Among patients with a major adverse cardiovascular event, we performed descriptive analyses of the associated mortality and discharge disposition among survivors.
We performed subgroup analyses by race and ethnicity (non-Hispanic white versus Black, Asian or Pacific Islander, Native American, or Other race or Hispanic ethnicity), insurance type (private versus other), estimated household income (above versus below the median), geographic region (the Midwest, Northeast, or West versus the South), and pre-existing comorbidities (zero versus one or more Charlson comorbidities). All analyses were performed by H.K. using Stata/MP version 18. The threshold of statistical significance was set at alpha = 0.05.
Sensitivity analysis with a non-pregnant population control group
In an additional analysis, we compared the risk of MACE during the pregnancy/postpartum period versus the risk among the general population of women in the 11 states used in our analysis. We used data from the U.S. Census and American Community Survey to adjust for age, demographics, and comorbidities27,30. We used Poisson regression to calculate adjusted incidence rate ratios for pregnant versus non-pregnant women overall and for each year of age.
Reporting summary
Further information on research design is available in the Nature Portfolio Reporting Summary linked to this article.
Data availability
All data supporting the findings of this study are available within the paper, in the supplementary information file, and in the source data file. The data used in this study are available under restricted access for patient confidentiality reasons; access can be obtained by application to the Healthcare Cost and Utilization Project (HCUP). Researchers can independently obtain access to the via an online application to the HCUP Central Distributor (https://cdors.ahrq.gov/). The application requires completion of Data Use Agreement training, submission of a signed Data Use Agreement, and payment of the relevant fees. HCUP and the Agency for Healthcare Research and Quality are responsible for granting data access. Source data for Figs. 1–3 are provided with this paper. Source data are provided with this paper.
Code availability
The analytical code used in this study is available as a supplement (Supplementary data 1).
References
Pregnancy Mortality Surveillance System. U.S. Centers for Disease Control and Prevention. https://www.cdc.gov/maternal-mortality/php/pregnancy-mortality-surveillance/index.html. Accessed January 7, 2025.
Kassebaum, N. J. et al. Global, regional, and national levels and causes of maternal mortality during 1990–2013: a systematic analysis for the Global Burden of Disease Study 2013. The Lancet 384, 980–1004 (2014).
Schummers, L. et al. Absolute risks of obstetric outcomes by maternal age at first birth: a population-based cohort. Epidemiology 29, 379–387 (2018).
Ananth, C. V., Keyes, K. M. & Wapner, R. J. Pre-eclampsia rates in the United States, 1980-2010: age-period-cohort analysis. BMJ 347, f6564 (2013).
Chen, J. et al. Assessment of Incidence and Factors Associated With Severe Maternal Morbidity After Delivery Discharge Among Women in the US. JAMA Netw Open 4, e2036148 (2021).
Lisonkova, S. et al. Maternal age and severe maternal morbidity: A population-based retrospective cohort study. PLoS Med. 14, e1002307 (2017).
Kenny, L. C. et al. Advanced Maternal Age and Adverse Pregnancy Outcome: Evidence from a Large Contemporary Cohort. PloS one 8, e56583 (2013).
Khalil, A., Syngelaki, A., Maiz, N., Zinevich, Y. & Nicolaides, K. H. Maternal age and adverse pregnancy outcome: a cohort study. Ultrasound Obstet. Gynecol. 42, 634–643 (2013).
Lean, S. C., Derricott, H., Jones, R. L. & Heazell, A. E. P. Advanced maternal age and adverse pregnancy outcomes: A systematic review and meta-analysis. PloS one 12, e0186287 (2017).
Cameron, N. A. et al. Association of Birth Year of Pregnant Individuals With Trends in Hypertensive Disorders of Pregnancy in the United States, 1995-2019. JAMA Network Open 5, e2228093 (2022).
De Viti, D. et al. Cardiovascular Outcomes in Advanced Maternal Age Delivering Women. Clinical Review and Medico-Legal Issues. Medicina (Kaunas) 55, (2019).
Birth Data. National Vital Statistics System. National Center for Health Statistics. https://www.cdc.gov/nchs/nvss/births.htm. Accessed January 16, 2025.
Bush, N. et al. Myocardial infarction in pregnancy and postpartum in the UK. European Journal of Preventive Cardiology 20, 12–20 (2013).
Abdul Sultan, A. et al. Impact of risk factors on the timing of first postpartum venous thromboembolism: a population-based cohort study from England. Blood 124, 2872–2880 (2014).
Columbo, J. A. et al. Derivation and validation of ICD-10 Codes for Identifying Incident Stroke. JAMA Neurol 81, 875–881 (2024).
Metcalfe, A. et al. Case definitions for acute myocardial infarction in administrative databases and their impact on in-hospital mortality rates. Health Serv. Res. 48, 290–318 (2013).
So, L., Evans, D. & Quan, H. ICD-10 coding algorithms for defining comorbidities of acute myocardial infarction. BMC Health Serv. Res. 6, 161 (2006).
Shah, R. V. et al. Association of fitness in young adulthood with survival and cardiovascular risk: the coronary artery risk development in young adults (CARDIA) study. JAMA Intern. Med. 176, 87–95 (2016).
Riise, H. K. R. et al. Association Between Gestational Hypertension and Risk of Cardiovascular Disease Among 617 589 Norwegian Women. Journal of the American Heart Association 7, (2018).
ACOG Committee Opinion No 743: low-dose aspirin use during pregnancy. Obstet. Gynecol. 132, e44–e52 (2018).
Geiger, C. K., Clapp, M. A. & Cohen, J. L. Association of prenatal care services, maternal morbidity, and perinatal mortality with the advanced maternal age cutoff of 35 Years. JAMA Health Forum 2, e214044 (2021).
Maclure, M. & Mittleman, M. A. Should we use a case-crossover design? Annu. Rev. Public Health 21, 193–221 (2000).
Mehta, L. S. et al. Cardiovascular considerations in caring for pregnant patients: a scientific statement from the american heart association. Circulation 141, e884–e903 (2020).
Kamel, H. et al. Risk of a thrombotic event after the 6-week postpartum period. N Engl. J. Med. 370, 1307–1315 (2014).
Kamel, H., Roman, M. J., Pitcher, A. & Devereux, R. B. Pregnancy and the risk of aortic dissection or rupture: a cohort-crossover analysis. Circulation 134, 527–533 (2016).
Healthcare Cost and Utilization Project. Agency for Healthcare Research and Quality. https://www.hcup-us.ahrq.gov. Accessed February 13, 2025.
Census QuickFacts. U.S. Census Bureau. https://www.census.gov/quickfacts/fact/table/US/PST045219. Accessed March 29, 2025.
Benchimol, E. I. et al. The reporting of studies conducted using observational routinely-collected health data (RECORD) statement. PLoS medicine 12, e1001885 (2015).
Quan, H. et al. Coding algorithms for defining comorbidities in ICD-9-CM and ICD-10 administrative data. Med. Care 43, 1130–1139 (2005).
U.S. Census Bureau. American Community Survey, ACS 5-Year Estimates Subject Tables, Table S0101, https://data.census.gov/table/ACSST5Y2018.S0101?g=040XX00US05,12,13,19,24,25,31,36,49,50,55. Accessed on 15 Dec 2025.
Acknowledgements
None. There was no specific external funding for this project.
Author information
Authors and Affiliations
Contributions
H.K., L.E.R., M.S., M.G.K., M.J.R., M.T.D.S., M.E.F., A.L.L. and B.B.N. made substantial contributions to the conception or design of the work, and the interpretation of data for the work. HK acquired and analyzed the data, and drafted the work. H.K., L.E.R., M.S., M.G.K., M.J.R., M.T.D.S., M.E.F., A.L.L. and B.B.N. reviewed it critically for important intellectual content. H.K., L.E.R., M.S., M.G.K., M.J.R., M.T.D.S., M.E.F., A.L.L. and B.B.N. gave final approval of the version to be published. H.K., L.E.R., M.S., M.G.K., M.J.R., M.T.D.S., M.E.F., A.L.L. and B.B.N. agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Corresponding author
Ethics declarations
Competing interests
Hooman Kamel reports a Deputy Editor role for JAMA Neurology; clinical trial steering/executive committee roles for the LIBREXIA-AF (Janssen) trial, INTERCEPT (World Health Research Institute and Javelin) trial, and LAAOS-4 (Population Health Research Institute and Boston Scientific) trial; consulting or endpoint adjudication committee roles for AbbVie, Alnylam, Arthrosi, AstraZeneca, Bayer, Boehringer Ingelheim, Eli Lilly, GlaxoSmithKline, Medtronic, Novartis, and Novo Nordisk; and ownership interests in Ascential Technologies, Doug Labs, and TETmedical. Mary J. Roman reports research funding from the Vital Projects Fund. Maria T. De Sancho reports honoraria from Pharmacosmos. Matthew E. Fink reports an Editor role for Neurology Alert. Ava L. Liberman reports a role on the data and safety monitoring board for Shionogi. The remaining authors declare no competing interests.
Peer review
Peer review information
Nature Communications thanks David Williams, and the other, anonymous, reviewer(s) for their contribution to the peer review of this work. A peer review file is available.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Source data
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Kamel, H., Riley, L.E., Son, M. et al. Maternal age and pregnancy-related cardiovascular complications. Nat Commun 17, 4066 (2026). https://doi.org/10.1038/s41467-026-72580-9
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41467-026-72580-9
